")
Back to Journals » Clinical Ophthalmology » Volume 18
Can the Location of the Iris Claw Lens Influence the Development and Timing of Pseudophakic Macular Edema?
Authors Tourino-Peralba R , Lamas-Francis D, Freijeiro-Gonzalez L, Martínez-Pérez L, Rodríguez-Ares T
Received 29 April 2024
Accepted for publication 6 September 2024
Published 20 September 2024 Volume 2024:18 Pages 2637—2644
DOI https://doi.org/10.2147/OPTH.S476047
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Rosario Tourino-Peralba,1,2,* David Lamas-Francis,1,* Laura Freijeiro-Gonzalez,3 Laura Martínez-Pérez,1 Teresa Rodríguez-Ares1
1Department of Ophthalmology, University Hospital of Santiago de Compostela, Santiago, Spain; 2Department of Surgery and Medical-Surgical Specialities, Faculty of Medicine, University of Santiago de Compostela, Santiago, Spain; 3Department of Statistics, Faculty of Mathematics, University of Santiago de Compostela, Santiago, Spain
*These authors contributed equally to this work
Correspondence: Rosario Tourino-Peralba, Department of Ophthalmology, University Hospital of Santiago de Compostela, Ramón Baltar s/n, 15706, Santiago de Compostela, Spain, Tel +34 981 951 749, Email [email protected]; [email protected]
Purpose: This study aims to analyze the incidence of pseudophakic macular edema (PME) and the role of contributing risk factors following prepupillary or retropupillary implantation of iris-claw lenses.
Methods: This retrospective cohort study included patients who underwent iris-claw intraocular lens implantation over a 16-year period at the University Hospital of Santiago de Compostela, Spain. The presence of risk factors for PME was recorded, and surgical outcomes included visual acuity, macular OCT scans, and description of complications.
Results: A total of 148 eyes from 147 patients were included. Seventy-nine eyes (54.4%) underwent prepupillary iris-claw lens implantation and 69 eyes (46.6%) underwent retropupillary implantation. The mean age of the patients was 68.9 ± 17.2 years. The incidence of PME post-surgery was 23.0% (26.6% prepupillary and 18.8% retropupillary), and the mean time between surgery and diagnosis was similar for both locations (4.8 and 4.7 months, respectively). PME recurred in 33% of the patients, reaching a high rate of 72.7% when the lens location was prepupillary. The mean best-corrected visual acuity was 0.66± 0.55 logMAR preoperatively and 0.38± 0.50 logMAR postoperatively. Postoperative complications occurred in 29 patients (19.6%).
Conclusion: PME following iris-claw lens implantation tends to be more frequent and recurrent when the location is prepupillary. Planning for iris-claw lens surgery should consider the risk factors for the development of PME.
Keywords: macular edema, aphakia, pseudophakia, iris-anchored intraocular lenses
Introduction
Iris-claw intraocular lenses are used for treating aphakia in cases of poor capsular support. This situation may be present in cases of complications following posterior capsule rupture during cataract surgery or due to weak zonular fibers, in cases of trauma, pseudoexfoliation syndrome, high myopia, uveitis, Marfan or Weill-Marchesani syndromes. There are different surgical approaches for correcting aphakia. The intraocular lens (IOL) can be placed in the anterior chamber (angle support IOL or prepupillary iris-claw IOL) or in the posterior chamber (scleral fixated or retropupillary iris-claw IOLs). These IOLs can also lead to complications and their implantation requires a learning curve.1 Iris-claw lenses represent a safe and widely available therapeutic option for aphakia.
Pseudophakic macular edema (PME) or pseudophakic cystic macular edema is a common complication which has been described following cataract surgery (uncomplicated and complicated),2 as well as other intraocular procedures. Its incidence is variable, and several risk factors have been linked to its development, including older age, posterior capsule rupture, diabetes, previous retinal detachment repair, retinal vein occlusion, uveitis or epiretinal membrane.3–5 Iris-claw lenses have been associated with higher rates of PME, as they are usually implanted in complex cases and they are in constant contact with iris tissue.6 The present study aimed to analyze the incidence of PME, to establish the timing of its onset and to indicate which risk factors contribute to its development after prepupillary or retropupillary implantation of claw iris lenses.
Methods
This retrospective cohort study included patients who underwent iris-claw IOL (Artisan® aphakia 205, Ophtec. Spain) implantation during a 15-year period at the University Hospital of Santiago de Compostela, Spain. The research was conducted in accordance with the tenets of the Declaration of Helsinki and approved by the local research ethics committee (Comité de Ética de la Investigación de Santiago-Lugo) (2017/127). All of the subjects signed an informed consent form before undergoing the procedure.
All iris-claw implantation surgeries performed between 2006 and 2021 were considered for inclusion. Patients were followed for at least 12 months. The inclusion criteria were as follows: IOL subluxation, lens subluxation, traumatic cataract and aphakia without capsular support. Exclusion criteria were severe and proliferative diabetic retinopathy, retinal vein occlusion, posterior uveitis, high myopia and age-related macular degeneration.
Data Collection
Patient demographic data, clinical examinations and intraoperative and postoperative outcomes and complications were obtained from electronic medical records. The demographic data included age, sex, laterality, history of trauma or previous ocular surgeries, as well as the presence of certain conditions (epiretinal membrane, retinal venous obstruction, high myopia, diabetes without retinopathy, uveitis, glaucoma, previous pseudophakic macular edema, postoperative complications).
Distance corrected visual acuity (DCVA) was obtained before the surgery and from record of the last visit, in decimal scale, and then transformed into logMAR for statistical analysis. Slit-lamp examination, intraocular pressure and funduscopy were performed during each visit. Macular OCT scans were obtained prior to surgery and in the postoperative follow-ups, using the Zeiss Cirrus HD-OCT 4000 (macular cube) or Heidelberg Spectralis OCT (fast macula). Scans were reviewed for the study. Pseudophakic macular edema (PME) was diagnosed with macular optical coherence tomography (OCT) and was defined as an increase in central foveal thickness (>300 microns) and the presence of intraretinal cysts.7 Macular changes in the presence of vitreomacular traction were not considered in PME. The general schedule of postoperative visits was one month, three, six and finally every twelve months after surgery.
Surgical Technique
Anaesthesia was peribulbar or topical depending on the patients’ cooperation. The surgical technique was previously described by the authors.7 A superior clear corneal incision was created. Prepupillary IOLs were stabilized with Shepard forceps at the optics and the mid-peripheral iris was fixated to the haptics with a needle inserted through the paracentesis (10 and 2 o’clock) or with the Vacufix enclavation system (Ophtec). Retropupillary IOLs were positioned behind the iris, one haptic after the other, with a reverse Sinskey hook or a 27-gauge needle bent at 45 degrees. Pars plana or anterior vitrectomy was performed when necessary. The corneal incision was sutured with 10–0 nylon and selectively removed after 8 weeks. Steroid and antibiotic eyedrops were prescribed for 1 month. Topical NSAIDs were administered during the first month in all patients in the study, in cases where macular edema was present it was maintained for at least 3 months or when macular edema was resolved. The surgeons (R.T. and L.M.) chose, in each case according to the preoperative characteristics, the most optimal location to implant the claw design intraocular lens (prepupillary or retropupillary). Macular OCT scans were obtained prior to surgery and in the postoperative follow-ups, except in some cases when patients did not cooperate or because visual acuity did not allow fixation (Figure 1). The general scheme for postoperative visits was at one, three, six and twelve months after surgery, and annually thereafter.
 |
Figure 1 OCT scan of pseudophakic macular edema with neurosensorial detachment 2 months after a prepupillary iris-claw lens implantation. |
Statistical Analysis
Data were analyzed using R Core Team (2021). Patient characteristics were reported as mean (SD) and/or median (interquartile range) for continuous variables and as a number (percentage) for categorical variables. Chi-square was used to compare categorical variables. Wilcoxon sign ranked test or Mann–Whitney test was used to compare continuous variables. P-values below 0.05 were considered statistically significant.
A logistic regression analysis was performed to determine the impact of the previously described risk factors for the development of PME after iris-claw IOL implantation. The logistic model was adjusted with the glm function. A backward selection process (Akaike information criterion, AIC) was carried out to determine whether certain covariables could be eliminated from the analysis, simplifying the model. Non-significant covariables were eliminated using the step function and only those which were relevant were included in the final model.
Results
A total of 148 eyes of 147 patients were included. Seventy-nine eyes (54.4%) underwent prepupillary iris-claw IOL implantation, and 69 eyes (46.6%) underwent retropupillary implantation. Mean age of the patients was 68.9 ± 17.2 years. Eighty eyes (54.1%) were male and 68 were (45.9%) female. Seventy-eight were right eyes (52.7%) and 70 were left eyes (47.3%). Mean follow-up was 3.6 years (range 1–14 years). The preoperative ocular condition (phakic, pseudophakic or aphakic), whether the IOL implantation was primary or secondary and the risk factors for MPE are listed in Table 1. Nine (6.1%) patients had presented PME previously: following routine cataract surgery in the fellow eye (n=3), after cataract surgery in the same eye (n=3), aphakia (n=1), retinal detachment repair (n=1) or trauma (n=1). One hundred and eleven patients had undergone one (87 cataract surgery) or 24 more eye surgeries (15 retinal detachment repair, 4 vitrectomy for other conditions, 3 traumatic corneal laceration repair, 1 trabeculectomy and 1 strabismus). The incidence of PME after surgery was 23.0% (26.6% in the prepupillary group and 18.8% in the retropupillary group). Although there is a higher, non-negligible, percentage of PME in the prepupillary location, this difference was not statistically significant (p=0.33). The mean time between surgery and the diagnosis of PME was 4.7±5.6 months (4.8±6.6 in the prepupillary group and 4.7±3.6 in the retropupillary group). Figure 2 shows the cumulative incidence of PME in the first 12 postoperative months. PME was recurrent in 11 patients (33.3%) (72.7% were prepupillary (n=8) and 27.3% retropupillary (n=3)). Eyes that developed PME were treated with nepafenac 1 mg/mL three times daily until resolution. Eight cases did not resolve with topical treatment: six were treated with periocular steroids, one with periocular steroids and intravitreal ranibizumab, and one of them also required repositioning of the subluxated haptic in the anterior chamber.
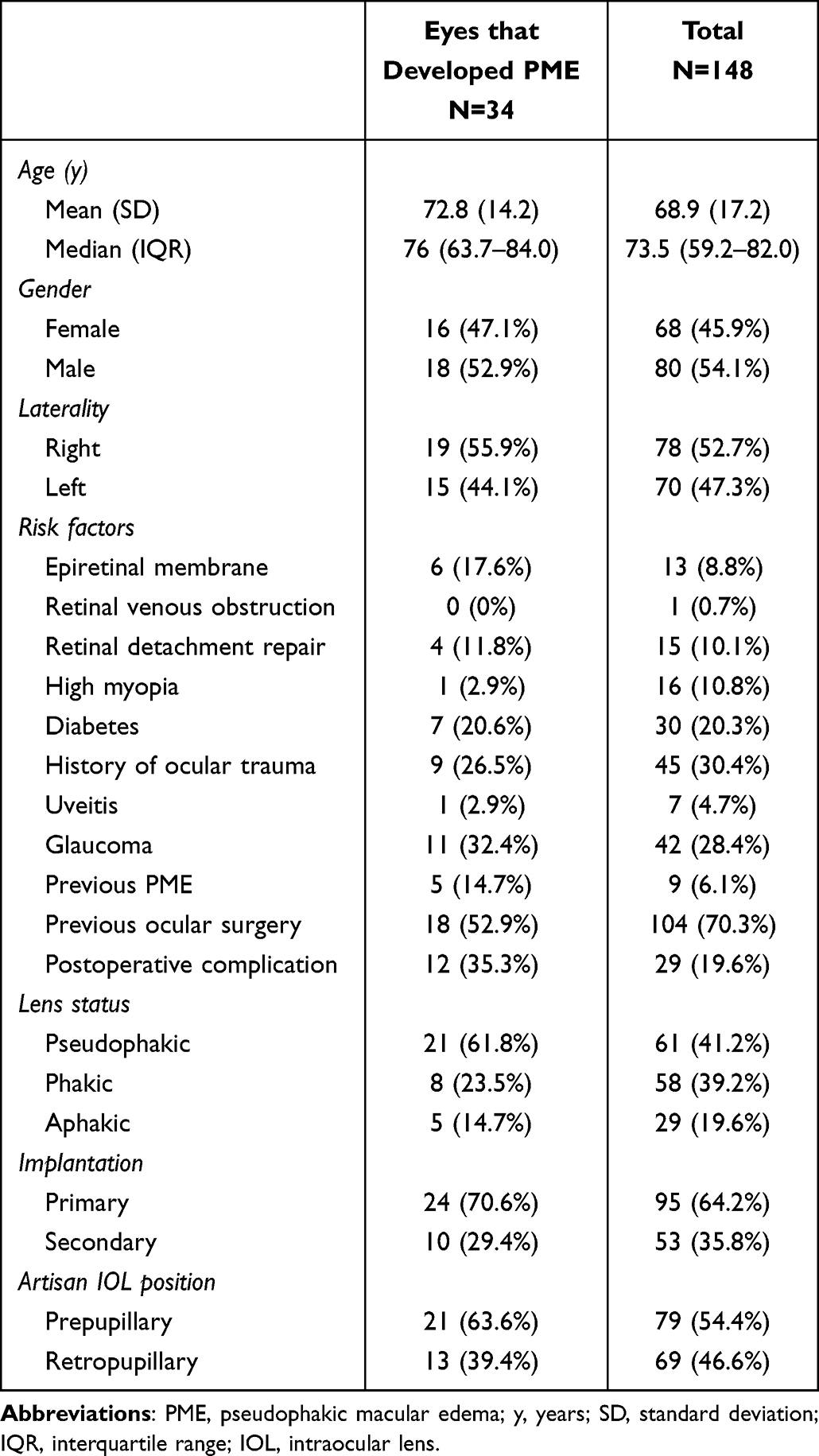 |
Table 1 Comparison of Characteristics Between Patients Who Developed PME and the Overall Study Population |
 |
Figure 2 Cumulative incidence of PME in the first 12 postoperative months following prepupillary vs retropupillary Artisan IOL implantation. |
The mean distance corrected visual acuity (DCVA) was 0.66±0.55 logMAR preoperatively and 0.38±0.50 logMAR after surgery. For prepupillary IOLs, mean BCVA improved from 0.59±0.52 logMAR preoperatively to 0.39±0.57 logMAR after surgery (p=0.00). For retropupillary IOLs, DCVA improved from 0.73±0.57 logMAR preoperatively to 0.35±0.41 logMAR after surgery (p=0.00). Preoperative and postoperative DCVA was not statistically different among prepupillary and retropupillary IOLs (p=0.06; p=0.73). At the final assessment of the study, the DCVA was not significantly different between eyes that developed PME, once resolved (0.35±0.33 logMAR), and eyes that did not develop PME (0.38±0.54 logMAR; p=0.36).
Postoperative complications following iris-claw IOL implantation were present in 29 patients (19.6%) and included ocular hypertension (IOP >30 mmHg) (n=9) or hypotony (IOP < 6 mmHg) (n=2), retinal detachment (n=8), corneal decompensation (n=5), iris-claw lens subluxation (n=3), lens fragment in the anterior chamber (n=1) and acute endophthalmitis (n=1).
An analysis of the risk factors for PME was performed. The results of the logistic model considering the effect of prepupillary or retropupillary implantation are shown in Table 2. Risk factors for the development of PME after iris claw IOL implantation include advanced age, previous retinal detachment repair, previous PME, postoperative complications related to iris claw lens implantation, and cases in which a subluxated IOL exchange (grade II and III) was performed. When prepupillary IOLs are analyzed separately, postoperative complications and a history of previous PME are significant risk factors for the development of PME. When only retropupillary IOLs are considered, previous surgery is a risk factor for PME.
 |
Table 2 Analysis of Suspected Risk Factors for PME Following Artisan IOL Implantation. Results of the Logistic Regression Model Showing the Estimation of Each Coefficient (Estimate), Its Standard Deviation (SE), the Value of the Statistic in the Signification Contrast (Z) and the Associated p-value |
Discussion
In this study, the incidence of PME was 23.0% (34 of 148 eyes). Cataract surgery is considered a risk factor for PME, with great variability in the frequency of PME depending on the presence of certain risk factors as well as the complexity of the surgical procedure. The incidence of PME following iris-claw IOL implantation is higher than the frequency reported following uncomplicated cataract surgery (0.1–2.35%).3,5,8
Previous studies have reported variable frequency of PME following iris-claw IOL implantation.7,9–15 As the definition of PME is not consistent among studies, the incidence rates vary significantly. Additionally, the detection of subclinical PME may be overlooked when OCT scans are not routinely performed. In the present study, CME was defined on OCT as macular thickening >300 microns, presence of cystoid changes near the fovea and decreased CVA postoperatively that could not be attributed to other factors. Since subclinical CME does not affect postoperative visual acuity, we did not consider it relevant.
Intraocular lenses can be implanted in very different scenarios. Our study included patients with prepupillary and retropupillary implantation, as well as different preoperative situations (mainly intraocular lens subluxation, subluxated cataract or aphakia) and known risk factors for PME. We did not find a significant difference in the incidence of PME between prepupillary and retropupillary implantation in the 148 cases studied, as our group published in a previous series of 95 eyes.7 However, it is important to note that there does seem to be a higher tendency among patients with prepupillary implants and this could be due to greater manipulation in their implantation and even greater perceived movement in these lenses in this location with the consequent loss of pigment and secondary chronic inflammation. Mora et al15 compared prepupillary and retropupillary implantation, with similar PME rates (33 vs 25%, respectively). Other studies focus on more specific groups of patients. Güell et al10 and Jayamadhury et al13 only reviewed the effects of anterior iris claw IOL implantation in aphakic eyes (secondary implantation), and reported an incidence of PME of 3.1% and 11.5%, respectively. Forlini et al11 and Faria et al12 only included patients with retropupillary iris claw IOLs, with low rates of PME (0.9% and 2.9%, respectively). Bernal-Morales et al14 studied 325 eyes undergoing retropupillary iris claw lens implantation combined with pars plana vitrectomy, with an incidence of PME of 20.5% at 12 months. In a comparative study by Al-Dwairi et al16 found that macular edema was more prevalent in prepupillary (12.1%) than in retropupillary (3.3%), prevalence confirmed by a recent meta-analysis.17
The mean time to diagnosis of PME in our study was 4.7 months (range 1 to 11 months). No study to our knowledge has so far determined the time of onset of oedema in this type of patient. In uncomplicated cataract surgery, the onset of PME usually occurs 1 to 3 months after surgery.6 The fact that the iris claw lenses are continuously in contact and cause friction with the iris (especially in atrophic irises and in an anterior position that allows movement of the IOL) could explain its appearance due to the suppression of post-surgical topical treatment. Risk factors also contribute not only to a higher prevalence of macular edema but may also account for greater durability and resistance to treatment.
Iris claw IOLs represent a safe option for IOL implantation in cases of poor or absent capsular support. The incidence of PME reported in the literature with alternative IOL positioning is variable, and iris claw lenses appear to be associated with the highest risk.6 Reported PME with sclerally sutured posterior chamber IOLs is 5.7–10.4%,18,19 with sclerally fixed posterior chamber IOLs is 1–21.3%20,21 and with anterior chamber IOLs is 15%.22 More recent techniques, such as Carlevale lenses fixed with an intrascleral plug (Soleko), represent a promising alternative for the treatment of aphakia, with excellent visual and anatomical results. The incidence of PME with the Soleko lenses ranges from 3.1% to 7.4%,20,23 although the studies have small sample sizes and short follow-up periods.
The presence of certain risk factors should be taken into account when determining the prevalence of PME after IOL implantation. In our series, advanced age, previous retinal detachment, history of previous PME, postoperative complications related to iris claw IOL implantation and IOL exchange surgery in eyes with IOL subluxation were associated with a higher frequency of postoperative PME. Something new, and not described so far, is that some risk factors are associated with a higher frequency of occurrence of PME depending on the localization of this type of IOL. The only study to date that relates risk factors to the development of macular oedema is a recent multicentre study24 conducted only in patients with retropupillary IOL implantation and pars plana vitrectomy simultaneous, and suggests that complicated cataract surgery is associated with an increased risk of developing PME in these cases, but they only analyzed patients with aphakia and IOL subluxation. In our study, in contrast, we included more risk groups. Thus, those patients who had suffered from post-surgical complications or had previously developed PME had an increased risk of PME after prepupillary IOL placement; while those who had a history of previous surgeries, especially retinal detachment, were more likely to suffer PME after retropupillary IOL implantation.
We believe these findings are important and should be considered because they allow us to schedule our surgery by choosing the most appropriate location for this type of lens based on the risk factors from which they start, as well as to personalize the risks in our informed consents. It is evident that the prepupillary location in inexperienced hands will be associated with greater manipulation and therefore a greater probability of developing edema, so it should be avoided in eyes with complex anatomies. Diabetes or a history of previous eye trauma 3 were not associated with PME in our study, perhaps due to the relatively small sample size and the fact that patients with diabetic retinopathy were excluded.
Older age was found to be a risk factor for PME. The mean age in our study was 68.9±17.2 (72.8+-14.2 in the MPE group). A study of a database of 8984 cataract surgery patients in the UK showed a similar trend.3 Other authors evaluating the iris claw lens outcomes have substantially lower mean ages (54.6, Güell et al10 66.3, Faria et al12 59.7–60.1, Forlini et al11 65, Jayamadhury et al13), which could explain the lower PME rates.
In our series, 15 patients underwent previous retinal detachment repair with pars plana vitrectomy. This is a known risk factor for PME following cataract surgery3 and was associated with a higher risk for PME in our study. McCafferty et al22 did not find any cases of PME in patients with previous retinal detachment, although they do not disclose the number of patients who presented this risk factor. An observational study of 99 patients who underwent pars plana vitrectomy and/or scleral buckling for retinal detachment showed 25.3% of cystoid macular edema in the postoperative period.4
In our study, eyes with subluxated IOL (pseudophakic) had a significantly higher incidence of PME (34.4%) than those who were aphakic (17.2%) or had a subluxated cataract (13.7%). A finding that could be due to the greater surgical manipulation required for subluxated IOL replacement, which leads to greater inflammation and vitreomacular traction during surgery; which, together with the manipulation of the iris during anchoring of the claw lens, favors intraocular inflammation and consequently the development of PME. Furthermore, manipulation of the iris associated with the use of pupillary expansion devices also contributes to the risk of PME,25 which will be increased if we opt for a pre-pupillary claw IOL placement.
Most cases of PME are transient, and long-term visual outcomes are generally good and only slightly worse than in eyes which did not develop this complication.5 In our series visual acuity improved after surgery regardless of claw lens location, however the prepupillary location showed greater visual relapses during the study caused by recurrent macular edema. The final visual acuity was not affected, although recuperation was later by the development of PME.
Our study has some limitations that should be taken into consideration. The diverse preoperative characteristics of the patients, as well as the variability in the studied procedure (secondary implantation, IOL exchange, complex cataract surgery, etc)., may have overestimated the incidence of PME attributed to iris-claw lenses. Central foveal thickness measurements, which could have helped in characterizing PME, were not available in all cases. The possibility of mixed-mechanism PME in diabetic patients could not be excluded, as fluorescein angiography was not performed. As iris-claw lenses are generally used in complex cases, it is difficult to design a study which can isolate the effect of these lenses on the development of PME.
In conclusion, PME is a complication to be considered with iris claw lens implantation. Risk factors such as advanced age, previous retinal detachment repair, previous PME, postoperative complications, as well as IOL exchange surgery, should be part of our informed consents as triggers for PME. Although PME usually responds to treatment and does not affect final visual outcomes, there are circumstances such as previous PME and prepupillary IOL location that may delay recovery of final DCVA. These characteristics should be taken into account when planning claw iris lens surgery.
Data Sharing Statement
The authors cannot share their data. The study databases, although anonymised, are not public, but are kept in the clinical-health databases of each hospital, which in turn are protected by each autonomous community of the country in question. However, if it is necessary to share this data, a personalised request can be made to the hospital and autonomous community of the country, indicating the purpose of use and the guarantee of data protection to be used. To do so, please contact the authors of the study to provide the request form.
Disclosure
The authors declare no conflict of interest related to this work.
References
1. Rouhette H, Meyer F, Pommier S, et al. FIL-SSF Carlevale intraocular lens for sutureless scleral fixation: 7 recommendations from a serie of 72 cases. MICA study (Multicentric Study of the Carlevale IOL). J Fr Ophtalmol. 2021;44(7):1038–1046. doi:10.1016/j.jfo.2021.05.002
2. Yonekawa Y, Kim IK. Pseudophakic cystoid macular edema. Curr Opin Ophthalmol. 2012;23(1):26–32. doi:10.1097/ICU.0b013e32834cd5f8
3. Chu CJ, Johnston RL, Buscombe C, et al. Risk factors and incidence of macular edema after cataract surgery. Ophthalmology. 2016;123(2):316–323. doi:10.1016/j.ophtha.2015.10.001
4. Pole C, Chehaibou I, Govetto A, et al. Macular edema after rhegmatogenous retinal detachment repair: risk factors, OCT analysis, and treatment responses. Int J Retin Vitr. 2021;7(1):9. doi:10.1186/s40942-020-00254-9
5. Henderson BA, Kim JY, Ament CS, et al. Clinical pseudophakic cystoid macular edema: risk factors for development and duration after treatment. J Cataract Refract Surg. 2007;33(9):1550–1558. doi:10.1016/j.jcrs.2007.05.013
6. Zur D, Fischer N, Tufail A, Monés J, Loewenstein A. Postsurgical Cystoid Macular Edema. Eur J Ophthalmol. 2011;21:62–68. doi:10.5301/EJO.2010.6058
7. Touriño-Peralba RT, Lamas-Francis D, Sarandeses-Diez T, Martínez-Pérez L, Rodríguez-Ares T. Iris-claw intraocular lens for aphakia: can location influence the final outcomes? J Cataract Refract Surg. 2018;44(7):818–826. doi:10.1016/j.jcrs.2018.05.010
8. Loewenstein A, Zur D. Postsurgical cystoid macular edema. Dev Ophthalmol. 2010;2010:148–159.
9. De Silva SR, Arun K, Anandan M, Glover N, Patel CK, Rosen P. Iris-claw intraocular lenses to correct aphakia in the absence of capsule support. J Cataract Refract Surg. 2011;37(9):1667–1672. doi:10.1016/j.jcrs.2011.03.051
10. Güell JL, Verdaguer P, Elies D, et al. Secondary iris-claw anterior chamber lens implantation in patients with aphakia without capsular support. Br J Ophthalmol. 2014;98(5):658–663. doi:10.1136/bjophthalmol-2013-304035
11. Forlini M, Soliman W, Bratu A, Rossini P, Cavallini GM, Forlini C. Long-term follow-up of retropupillary iris-claw intraocular lens implantation: a retrospective analysis. BMC Ophthalmol. 2015;15:143. doi:10.1186/s12886-015-0146-4
12. Faria MY, Ferreira NP, Pinto JM, et al. Retropupillary iris claw intraocular lens implantation in aphakia for dislocated intraocular lens. Int Med Case Rep J. 2016;9:261–265. doi:10.2147/IMCRJ.S116771
13. Jayamadhury G, Potti S, Kumar KV, et al. Retropupillary fixation of iris-claw lens in visual rehabilitation of aphakic eyes. Indian J Ophthalmol. 2016;64(10):743–746. doi:10.4103/0301-4738.195012
14. Bernal-Morales C, Hernández-Martínez A, Navarro-Angulo MJ, et al. Retropupillary iris-claw intraocular lens and pars plana vitrectomy in aphakia management: a national multicenter audit. Retina. 2021;41(10):2048–2058. doi:10.1097/IAE.0000000000003161
15. Mora P, Calzetti G, Favilla S, et al. Comparative analysis of the safety and functional outcomes of anterior versus retropupillary iris-claw IOL fixation. J Ophthalmol. 2018;4(2018):8463569.
16. Al-Dwairi R, Saleh O, Aleshawi A, et al. Anterior versus retropupillary iris-claw intraocular lens: indications, visual outcome and postoperative complications. Ophthalmol Ther. 2022;11(2):771–784. doi:10.1007/s40123-022-00474-2
17. Liang IC, Chang YH, Hernández Martínez A, Hung CF. Iris-claw intraocular lens: anterior chamber or retropupillary implantation? A systematic review and meta-analysis. Medicina (Kaunas). 2021;57(8):785. doi:10.3390/medicina57080785
18. Mahmood SA, Zafar S, Shakir M, Rizvi SF. Visual acuity after trans-scleral sutured posterior chamber intraocular lens. J Coll Physicians Surg Pak. 2014;24(12):922–926.
19. Long C, Wei Y, Yuan Z, Zhang Z, Lin X, Liu B. Modified technique for transscleral fixation of posterior chamber intraocular lenses. BMC Ophthalmol. 2015;2:15–127.
20. Shekhawat N, Goyal K. Sutureless glueless intrascleral fixation of posterior chamber intraocular lens: boon for aphakic. Indian J Ophthalmol. 2017;65(12):1454–1458. doi:10.4103/ijo.IJO_620_17
21. Todorich B, Stem MS, Kooragayala K, et al. Structural analysis and comprehensive surgical outcomes of the sutureless intrascleral fixation of secondary intraocular lenses in human eyes. Retina. 2018;38(Suppl 1):S31–S40. doi:10.1097/IAE.0000000000001941
22. Donaldson KE, Gorscak JJ, Budenz DL, et al. Anterior chamber and sutured posterior chamber intraocular lenses in eyes with poor capsular support. J Cataract Refract Surg. 2005;31(5):903–909. doi:10.1016/j.jcrs.2004.10.061
23. Vaiano AS, Hoffer KJ, Greco A, et al. Long-term outcomes and complications of the new Carlevale sutureless scleral fixation posterior chamber IOL. J Refract Surg. 2021;37(2):126–132. doi:10.3928/1081597X-20201207-02
24. Bernal-Morales C, Navarro-Angulo MJ, Rodriguez-Maqueda M, et al. Predictive factors and management of macular edema after retropupillary iris-claw intraocular lens implantation in aphakia: national Multicenter Audit-Report 2. J Clin Med. 2023;12(2):436. doi:10.3390/jcm12020436
25. Taipale C, Holmström EJ, Ilveskoski L, Tuuminen R. Incidence of pseudophakic cystoid macular edema in eyes with and without pupil expansion device. Acta Ophthalmol. 2019;97(7):688–694. doi:10.1111/aos.14007
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.