")
Back to Journals » Journal of Inflammation Research » Volume 17
Case Series on the Efficacy and Safety of Tocilizumab in IVIG-Resistant Kawasaki Disease: A Retrospective Analysis of Five Patients
Authors Ling J , Xie F, Zhou Q, Ouyang Q, Li L, Zhao W, Liu X
Received 7 September 2024
Accepted for publication 27 November 2024
Published 11 December 2024 Volume 2024:17 Pages 10991—10998
DOI https://doi.org/10.2147/JIR.S479879
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ning Quan
Jiayun Ling,1 Fang Xie,1 Qingfang Zhou,1 Qian Ouyang,1 Lin Li,1 Wei Zhao,2 Xiaohui Liu1
1Department of Rheumatology and Immunology, Jiangxi Children’s Hospital, Jiangxi Medical College, Nanchang, Jiangxi, People’s Republic of China; 2Pediatric Cardiology Treatment Center, Jiangxi Children’s Hospital, Jiangxi Medical College, Nanchang, Jiangxi, People’s Republic of China
Correspondence: Xiaohui Liu, Department of Rheumatology and Immunology, Jiangxi Children’s Hospital, Jiangxi Medical College, Nanchang, Jiangxi, People’s Republic of China, Email [email protected]
Background: Kawasaki disease (KD) is a leading cause of acquired heart disease in children in developed countries. While intravenous immunoglobulin (IVIG) is the standard treatment, 10– 20% of patients do not respond to IVIG. Given the significant role of interleukin-6 (IL-6) in KD pathophysiology, targeting IL-6 may offer a therapeutic option for IVIG-resistant KD.
Objective: This study aims to evaluate the efficacy and safety of tocilizumab (an IL-6 receptor antagonist) in the treatment of IVIG-resistant KD through a retrospective analysis of clinical data.
Methods: Clinical data from five KD patients treated with tocilizumab (TCZ) at Jiangxi Children’s Hospital from January 2023 to February 2024 were retrospectively analyzed. All patients met the 2017 American Heart Association diagnostic criteria for KD and received a single dose of TCZ. Data on clinical manifestations, laboratory indicators, and coronary artery changes before and after TCZ treatment were collected.
Results: Four of the five patients had a KOBAYASHI score > 4, and initial IVIG and glucocorticoid treatments were ineffective. Following TCZ administration, body temperature normalized within 12 hours in three patients, and inflammatory markers, including C-reactive protein and interleukin-6, returned to normal levels. Coronary artery dilation was observed in 75% of patients pre-TCZ; post-TCZ, coronary arteries normalized in three patients, while one patient experienced progressive right coronary artery dilation. No adverse events were reported following TCZ administration.
Conclusion: Tocilizumab effectively controls systemic inflammation and improves coronary artery outcomes in IVIG-resistant KD patients, with no observed adverse events. Larger studies are necessary to confirm these findings and further investigate long-term effects on coronary artery health.
Keywords: Kawasaki disease, tocilizumab, IVIG-resistant, coronary arteries, inflammatory markers
Introduction
Kawasaki disease (KD), also known as mucocutaneous lymph node syndrome, was first identified by Dr. Fujio Kawasaki in Japan in 1967.1 While the etiology and pathogenesis of KD remain unclear, current understanding suggests that acute systemic non-specific vasculitis in genetically susceptible children may be triggered by infectious factors.2 Interleukin-6 (IL-6), a pleiotropic cytokine, plays a significant role in various inflammatory and immune-related disorders, including KD.3 Lymphocyte activation drives vascular inflammation in KD, releasing cytokines such as IL-1, IL-6, and TNF-α intensifying the immune response and leading to systemic vascular inflammation.4,5 Clinical data indicate that IL-6 levels are significantly higher in the IVIG-resistant KD group compared to the IVIG-responsive group, suggesting an association between IL-6 overexpression and IVIG resistance.6,7 Tocilizumab, an IL-6 receptor antagonist and humanized monoclonal antibody, inhibits IL-6 signaling by antagonizing both membrane-bound and soluble IL-6 receptors, delivering targeted anti-inflammatory effects, and is widely used for various autoimmune diseases.8 Current treatments for IVIG-resistant KD include glucocorticoids, secondary IVIG, and infliximab. However, due to a limited early understanding of IL-6’s role in KD pathogenesis, there is minimal clinical experience and research on IL-6 receptor antagonists in KD treatment. This study aims to evaluate the clinical efficacy, safety, and impact on coronary artery damage of tocilizumab for IVIG-resistant KD through a retrospective analysis of clinical data from five cases treated with tocilizumab.
Patients and Methods
This study retrospectively analyzed KD patients admitted to the Rheumatology and Immunology Department of Jiangxi Children’s Hospital from January 2023 to February 2024. The inclusion criteria were as follows: (1) diagnosis of Kawasaki disease, with both typical and incomplete forms meeting the 2017 American Heart Association diagnostic criteria;9 IVIG-resistant KD, defined as persistent fever 36 hours post-IVIG treatment or recurrence of typical KD symptoms during a previously afebrile phase, met specific diagnostic criteria.9 (2) Single-dose tocilizumab treatment, following the dose recommendations for systemic juvenile idiopathic arthritis: 12 mg/kg per dose for children weighing under 30 kg and 8 mg/kg per dose for children over 30 kg.10 Exclusion criteria included: (1) KD patients previously treated with IVIG before admission; (2) KD patients who received immunosuppressants or other biological agents; (3) KD patients with other rheumatic or immune diseases.
We analyzed the clinical manifestations, laboratory indicators, and imaging results of five KD patients before and after tocilizumab administration. Data collection included temperature measurements on the day before administration, the day of administration, and on days one, two, three, and seven post-administration, as well as laboratory indicators recorded at admission and five days after tocilizumab treatment. A descriptive analysis, including statistical summaries and graphical representations, was conducted on the data collected.
Coronary artery damage was assessed using echocardiogram results. The coronary artery Z-score was calculated based on each child’s gender, age, weight, and echocardiogram data.9 The classification was as follows: no coronary artery dilation (Z-score < 2.0), coronary artery dilation (2.0 < Z-score < 2.5), small aneurysm (2.5 < Z-score < 5.0), medium aneurysm (5.0 ≤ Z-score < 10.0), and giant aneurysm (Z-score ≥ 10.0).
Results
The specific clinical characteristics of these five patients are detailed in Table 1. Eighty percent of the patients presented with typical KD manifestations. Four patients exhibited prominent joint symptoms, mainly swelling or pain in the lower limb joints. One patient experienced convulsions during fever, and three exhibited gastrointestinal symptoms, including skin jaundice, diarrhea, and abdominal distension. One patient had complications of macrophage activation syndrome and severe pneumonia, while none had Kawasaki disease shock syndrome. All patients tested negative for COVID-19 nucleic acid or antigen, and 75% had a KOBAYASHI score above 4. Initial IVIG treatment failed to control clinical symptoms.
 |
Table 1 Characteristics of Tocilizumab-Treated Kawasaki Disease Patients |
Three patients (patients 2, 3, and 4) received 2–6 mg/kg/day intravenous methylprednisolone before TCZ administration, with no improvement in symptoms. Patient 2 developed hyperferritinemia following methylprednisolone shock therapy. Patients 1 and 5 received a second IVIG combined with 2–4 mg/kg/day intravenous methylprednisolone before TCZ treatment. Patient 1 continued to experience recurrent fever, while Patient 5 showed slight temperature improvement but a progressive increase in inflammatory markers. Four patients had coronary artery dilation before tocilizumab, including two with small aneurysms.
Following TCZ administration, coronary artery diameters returned to normal in three of the four patients with initial dilation. However, as shown in Table 2, one patient (Patient 1) exhibited progressive dilation of the right coronary artery. As illustrated in Figure 1, this dilation peaked eight weeks after onset, reaching a diameter of 7 mm (z-score 13.3). By 37 weeks post-onset, the coronary artery had retracted to a diameter of 3.8 mm, with a z-score of 4.65. Notably, in the third week of illness, when significant coronary dilation was observed in Patient 1, examinations of the aortic branches and peripheral arteries revealed no other arterial involvement.
 |
Table 2 Specific Changes in Coronary Artery of Patient 1 |
 |
Figure 1 Doppler image of right coronary artery dilatation in Patient 1. Abbreviations: RCA, Right Coronary Artery; D, Diameter. |
Clinically, KD-related symptoms gradually subsided in all patients following TCZ treatment. All patients exhibited fingertip desquamation post-treatment, and four patients with joint pain experienced symptom regression. Additionally, liver function returned to normal in three patients. As shown in Figure 2, TCZ had a notable effect on body temperature control. Four patients who had recurrent high fevers before treatment achieved normal body temperatures within one-day post-administration. None of the patients experienced fever following TCZ treatment.
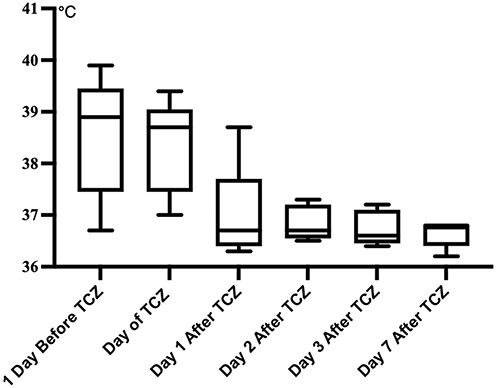 |
Figure 2 Temperature changes of 5 patients. Abbreviation: TCZ, Tocilizumab. |
As shown in Figure 3, laboratory indicators improved significantly following TCZ treatment. Elevated white blood cell counts decreased in three patients (median 9.06×109/L), and lymphocyte counts normalized in all five patients (median 2.75×109/L). C-reactive protein (CRP), initially elevated with a median of 109 mg/L, decreased substantially to a median of 1.02 mg/L post-treatment. Similarly, interleukin-6 levels showed a marked reduction from a median of 461.05 pg/mL pre-treatment to 26.35 pg/mL post-treatment. NT-proBNP levels, tested in three patients, decreased from a median of 1503 pg/mL pre-treatment to 50.8 pg/mL post-treatment, indicating improved cardiac status.
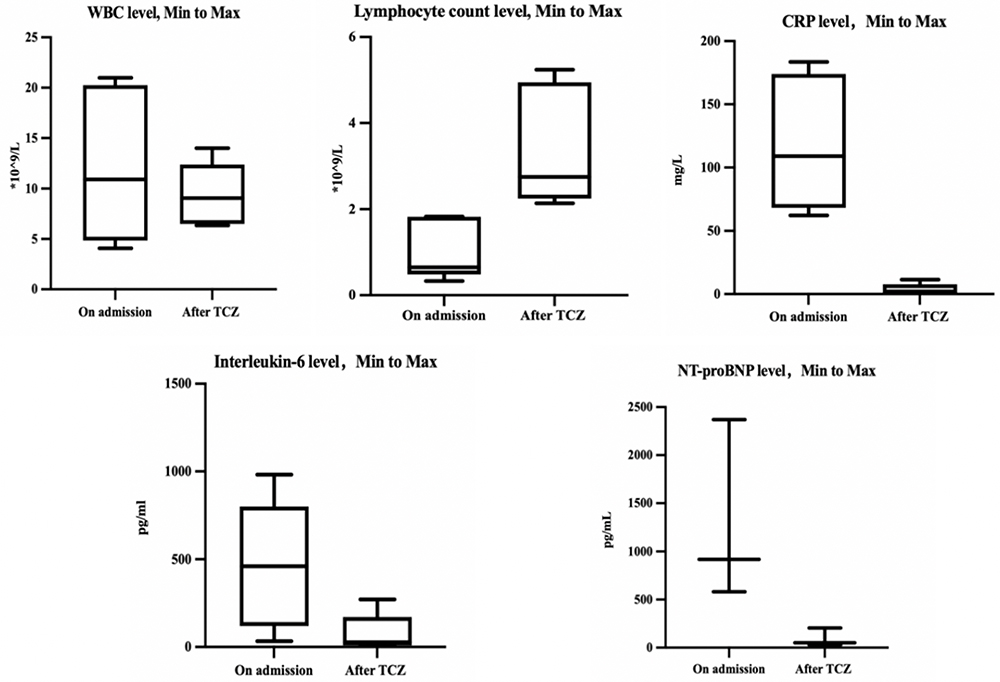 |
Figure 3 Laboratory Parameters of Tocilizumab-treated Kawasaki Disease Patients. Abbreviations: WBC, White blood cell; CRP, C-reactive protein; NT-proBNPcount, N-terminal pro-B-type natriuretic peptide. |
Discussion
With the gradual understanding of the pathogenesis of Kawasaki disease, targeted cytokine therapy has emerged as an effective treatment for treating IVIG-resistant cases. Tumor necrosis factor-α antagonists have proven effective for IVIG-resistant KD,9 and IL-1 antagonists are increasingly used in refractory cases.11 The fundamental pathological feature of Kawasaki disease is systemic vasculitis, with pathological examinations showing local infiltration of inflammatory cells, such as granulocytes and macrophages, alongside tissue necrosis.12 In the LCWE-induced mouse model of Kawasaki disease, increased production of inflammatory cytokines (including IL-1, IL-6, and TNF-α) is associated with heart disease, particularly coronary artery damage.13 Clinical studies further indicate a significant rise in these cytokines during the acute phase of Kawasaki disease, followed by a substantial decrease in the recovery phase.4,14,15 Our analysis of C-reactive protein and interleukin-6 levels, as well as body temperature changes in these five patients, demonstrates that the systemic inflammatory response was effectively controlled post-TCZ treatment.
Research findings indicate that abnormal immune activation in Kawasaki disease is closely linked to the suppression of regulatory T cells (Tregs) during the acute phase.16 Reduced Treg numbers and impaired function significantly contribute to the onset and progression of Kawasaki disease.17 Studies have shown that IL-6 may downregulate FOXP3+ Tregs, promoting pro-inflammatory Tregs and reducing Treg stability, which exacerbates vasculitis in the acute phase.18 Additionally, IL-6 has been shown to induce thrombocytosis and contribute to vasculitis and endothelial damage by initiating a cascade reaction.19 The relationship between serum IL-6, the IVIG response, and coronary artery aneurysms (CAA) in Kawasaki disease remains largely unexplored. However, overexpression of IL-6-related genes has been linked to IVIG non-responsiveness.20 Clinical data indicate that patients with Kawasaki disease complicated by CAA have IL-6 sub-levels 2.13 times higher than those with normal coronary arteries.21 A 2019 study from Japan suggested that IVIG resistance is associated with inadequate monocyte suppression and increased T lymphocyte activity, particularly activation of the CD8-related immune system.22 The continuous release of inflammatory factors like IL-6 and TNF-α from monocytes and T lymphocytes drives IVIG resistance.23 Further studies on serum cytokines in Kawasaki disease have identified IFN-γ, IL-6, and other cytokines as independent risk factors for IVIG-unresponsive cases.5 Given the critical role of IL-6 in Kawasaki disease pathophysiology, IL-6 antagonism presents a feasible therapeutic approach.
Research on the application of IL-6 receptor antagonists in Kawasaki disease remains limited in both animal models and clinical studies. Porritt et al reported that IL-1 antagonists could control LCWE-induced KD vasculitis, whereas IL-6 receptor antagonists could not.24 However, this study assessed the aorta and abdominal aorta, not the coronary artery. Experimental data indicated that IL-6 receptor antagonists effectively reduced serum SAA levels, suggesting their efficacy in managing systemic inflammation.25 In clinical research, Nozawa et al conducted a prospective small-sample study in 2017,25 demonstrating that IVIG-non-responsive KD patients treated with tocilizumab showed improvement in systemic inflammation. However, 50% (2 out of 4 cases) of these patients developed giant coronary artery aneurysms post-treatment. Based on these findings, Nozawa et al suggested that tocilizumab might contribute to coronary artery aneurysms in KD patients. In our study, one patient developed aneurysm-like dilation after treatment; this patient had extensive systemic involvement, including high inflammation, hypoproteinemia, jaundice, joint effusion, and a Kobayashi score of 6, a known risk factor for coronary dilation. In contrast, 80% of patients in our cohort did not experience progressive coronary artery dilation after tocilizumab, and two patients’ dilated coronary arteries returned to normal following treatment. These findings suggest that the impact of tocilizumab on coronary arteries in KD patients requires further investigation.
Conclusion
In summary, this retrospective study highlights the potential efficacy and safety of tocilizumab for treating IVIG-resistant KD. Tocilizumab significantly improved systemic inflammatory markers and coronary artery outcomes in this small cohort, with no adverse events observed. These findings indicate that tocilizumab may offer a viable treatment alternative for refractory KD, introducing a new therapeutic pathway for patients unresponsive to conventional IVIG and glucocorticoid therapies. The limitations of the study, including the small sample size and absence of a control group, particularly the lack of comparison with other biological agents, highlight the need for larger, controlled trials to confirm these findings and clarify tocilizumab’s long-term effects on coronary artery health in Kawasaki disease patients. Future research should target a broader patient population with extended follow-up to better define tocilizumab’s therapeutic role in KD management. Addressing these gaps will enable a more comprehensive treatment strategy for KD, ultimately improving outcomes for patients with this challenging disease.
Ethical Approval
The study was conducted according to the principles of the Declaration of Helsinki. This study was approved by the Ethics Committee of Jiangxi Children’s Hospital affiliated to Nanchang Medical College, which also approved the publication of specific details of the case series. Informed consent from the patient and her legal guardians for publication of identifying information/images in an online open-access publication was obtained. Details of these cases are released as requested by the agency.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no competing interests in this work.
References
1. Kawasaki T. [Acute febrile mucocutaneous syndrome with lymphoid involvement with specific desquamation of the fingers and toes in children]. Arerugi. 1967;16(3):178–222. Maori. doi:10.1126/science.113.2937.418-b
2. Mahajan A, Yadav S, Maheshwari A, et al. Profile of children with Kawasaki disease associated with tropical infections. Indian J Pediatr. 2022;89(8):759–764. doi:10.1007/s12098-021-03953-9
3. Schett G. Physiological effects of modulating the interleukin-6 axis. Rheumatology. 2018;57(suppl_2):ii43–ii50. doi:10.1093/rheumatology/kex513
4. Bordea MA, Costache C, Grama A, et al. Cytokine cascade in Kawasaki disease versus Kawasaki-like syndrome. Physiol Res. 2022;71(1):17–27. doi:10.33549/physiolres.934672
5. Wang Y, Yuan Y, Gao L, et al. Clinical significance of changes of serum cytokines in children with Kawasaki disease. Chin J Appl Clin Pediatr. 2020;35(13):4. doi:10.3760/cma.j.cn101070-20190917-00884
6. Huang XB, Zhao S, Liu ZY, Xu YY, Deng F. Serum amyloid A as a biomarker for immunoglobulin resistance in Kawasaki disease. Ann Med. 2023;55(2):2264315. doi:10.1080/07853890.2023.2264315
7. Wu Y, Liu FF, Xu Y, et al. Interleukin-6 is prone to be a candidate biomarker for predicting incomplete and IVIG nonresponsive Kawasaki disease rather than coronary artery aneurysm. Clin Exp Med. 2019;19(2):173–181. doi:10.1007/s10238-018-00544-5
8. Sheppard M, Laskou F, Stapleton PP, et al. Tocilizumab (Actemra). Hum Vaccin Immunother. 2017;13(9):1972–1988. doi:10.1080/21645515.2017.1316909
9. McCrindle BW, Rowley AH, Newburger JW, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a scientific statement for health professionals from the American Heart Association. Circulation. 2017;135(17):e927–e999. doi:10.1161/CIR.0000000000000484
10. Ringold S, Weiss PF, Beukelman T, et al. 2013 update of the 2011 American College of Rheumatology Recommendations for the treatment of juvenile idiopathic arthritis recommendations for the medical therapy of children with systemic juvenile idiopathic arthritis and tuberculosis screening among children receiving biologic medications. Arthritis Rheum. 2013;65(10):2499–2512. doi:10.1002/acr.22087
11. Zheng YZ, Hou J, Gui YH. Research progress of interleukin-1 and its receptor antagonist Anakinra in Kawasaki disease. Chin J Appl Clin Pediatr. 2022;37(3):233–237. doi:10.3760/cma.j.cn101070-20210226-00234
12. Amarante-Mendes GP, Adjemian S, Branco LM, et al. Pattern recognition receptors and the host cell death molecular machinery. Front Immunol. 2018;9:2379. doi:10.3389/fimmu.2018.02379
13. Okitsu-Negishi S, Nakano I, Suzuki K, et al. The induction of cardioangitis by Lactobacillus casei cell wall in mice. I. The cytokine production from murine macrophages by Lactobacillus casei cell wall extract. Clin Immunol Immunopathol. 1996;78(1):30–40. doi:10.1006/clin.1996.0005
14. Seo YM, Kang HM, Lee SC, et al. Clinical implications in laboratory parameter values in acute Kawasaki disease for early diagnosis and proper treatment. Korean J Pediatr. 2018;61(5):160–166. doi:10.3345/kjp.2018.61.5.160
15. Li Y, Zheng Q, Zou L, et al. Kawasaki disease shock syndrome: clinical characteristics and possible use of IL-6, IL-10 and IFN-γ as biomarkers for early recognition. Pediatr Rheumatol Online J. 2019;17(1). doi:10.1186/s12969-018-0303-4
16. Olivito B, Taddio A, Simonini G, et al. Defective FOXP3 expression in patients with acute Kawasaki disease and restoration by intravenous immunoglobulin therapy. Clin Exp Rheumatol. 2010;28(1Suppl 57):93–97.
17. Ni FF, Li CR, Li Q, et al. Regulatory T cell microRNA expression changes in children with acute Kawasaki disease. Clin Exp Immunol. 2014;178(2):384–393. doi:10.1111/cei.12418
18. Raugh A, Allard D, Bettini M. Nature vs. nurture: FOXP3, genetics, and tissue environment shape Treg function. Front Immunol. 2022;13:911151. doi:10.3389/fimmu.2022.911151
19. Abrams JY, Weintraub ES, Baggs JM, et al. Childhood vaccines and Kawasaki disease, vaccine safety datalink, 1996–2006. Vaccine. 2015;33(2):382–387. doi:10.1016/j.vaccine.2014.10.044
20. Ikeda K, Mizoro Y, Ameku T, et al. Transcriptional analysis of intravenous immunoglobulin resistance in Kawasaki disease using an induced pluripotent stem cell disease model. Circ J. 2016;81(1):110–118. doi:10.1253/circj.CJ-16-0541
21. Si F, Wu Y, Gao F, et al. Relationship between IL-27 and coronary arterial lesions in children with Kawasaki disease. Clin Exp Med. 2017;17(4):451–457. doi:10.1007/s10238-017-0451-8
22. Matsuguma C, Wakiguchi H, Suzuki Y, et al. Dynamics of immunocyte activation during intravenous immunoglobulin treatment in Kawasaki disease. Scand J Rheumatol. 2019;48(6):491–496. doi:10.1080/03009742.2019.1604992
23. Hu P, Jiang GM, Wu Y, et al. TNF-α is superior to conventional inflammatory mediators in forecasting IVIG nonresponse and coronary arteritis in Chinese children with Kawasaki disease. Clin Chim Acta. 2017;471:76–80. doi:10.1016/j.cca.2017.05.019
24. Porritt RA, Chase Huizar C, Dick EJ, et al. Inhibition of IL-6 in the LCWE mouse model of Kawasaki disease inhibits acute phase reactant serum amyloid A but fails to attenuate vasculitis. Front Immunol. 2021;12:630196. doi:10.3389/fimmu.2021.630196
25. Nozawa T, Imagawa T, Ito S. Coronary-artery aneurysm in tocilizumab-treated children with Kawasaki’s disease. N Engl J Med. 2017;377(19):1894–1896. doi:10.1056/NEJMc1709609
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.