")
Back to Journals » Clinical Ophthalmology » Volume 18
Changes in Ocular Blood Flow After Intravitreal Injection for Diabetic Macular Edema Between Aflibercept and Faricimab
Authors Mizukami T , Mizumoto S, Ishibashi T, Ueno S, Toyonishi T, Tachibana K, Mishima S, Shimomura Y
Received 30 April 2024
Accepted for publication 26 July 2024
Published 27 August 2024 Volume 2024:18 Pages 2407—2416
DOI https://doi.org/10.2147/OPTH.S476307
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Takahiro Mizukami,1 Saya Mizumoto,1 Takuya Ishibashi,1 Satoru Ueno,2 Takayo Toyonishi,1 Kuniko Tachibana,1 Soichiro Mishima,1 Yoshikazu Shimomura1
1Department of Ophthalmology, Fuchu Hospital, Izumi, Osaka, Japan; 2Department of Ophthalmology, PL Byoin, Tondabashi, Osaka, Japan
Correspondence: Takahiro Mizukami, Department of Ophthalmology Fuchu Hospital, Higocho1-10-17, Izumi, Osaka, 594-0076, Japan, Tel +81-725-90-5123, Email [email protected]
Purpose: In this study, we aimed to evaluate and compare the effects of intravitreal aflibercept (IVA) and intravitreal faricimab (IVF) injections on the blood flow of retinal vessels in the peripapillary region and optic nerve head (ONH) in eyes with diabetic macular edema (DME) using laser speckle flowgraphy (LSFG).
Patients and Methods: This study included 20 eyes of 18 patients treated with IVA and 15 eyes of 11 patients treated with IVF for DME. The mean blur rate (MBR) of the ONH and retinal artery and vein of the peripapillary region were measured using LSFG at baseline and 1 month after injection. Central retinal thickness (CRT) and best-corrected visual acuity (BCVA) were measured for all patients.
Results: CRT decreased significantly in both IVA-treated (p = 0.0003) and IVF-treated groups (p = 0.0004). Some of the MBR-related parameters of the ONH, such as MBR of all areas (MA), MBR of vascular areas (MV), and MBR of tissue areas (MT), decreased significantly 1 month after IVA and IVF compared to baseline values (MA of IVA, p < 0.0001; MT of IVA, p = 0.0220; MA of IVF, p = 0.0002; MT of IVF, p = 0.0461). MBR of the retinal artery (MBR-A) and vein (MBR-V) also decreased significantly 1 month after IVA and IVF compared with baseline values (MBR-A of IVA, p = 0.0002; MBR-V of IVA, p = 0.0010; MBR-A of IVF, p = 0.0368). No significant difference in ocular perfusion was observed between the IVA-treated and IVF-treated groups.
Conclusion: Intravitreal injection led to a reduction in ocular blood flow in both retinal peripapillary vessels and the ONH in both IVA-treated and IVF-treated groups. No significant difference was observed in MBR reduction between the IVA-treated and IVF-treated groups. Our findings warrant further long-term investigations to reveal differences between aflibercept and faricimab.
Keywords: diabetic macular edema, diabetic retinopathy, laser speckle flowgraphy, vascular endothelial growth factor, observational study
Introduction
Diabetic retinopathy (DR) is the primary cause of visual impairment among working-age populations in industrialized nations. Vision loss may result from various mechanisms, but the most prevalent cause is diabetic macular edema (DME).1
The treatment landscape for DME has advanced significantly over the past decade. Previously, focal or grid macular argon laser photocoagulation was the standard treatment.2 However, its use is now primarily limited to cases of non-center-involved DME.3 Currently, the most frequently employed therapeutic approach involves intravitreal administration of anti-vascular endothelial growth factor (VEGF) agents, and the prognosis of patients with DME has markedly improved.4
There are various commercially available anti-VEGF agents. Older options include monoclonal antibodies such as ranibizumab and bevacizumab. While ranibizumab and bevacizumab alone inhibit VEGF-A,5,6 aflibercept, a recombinant fusion protein, inhibits VEGF-A, VEGF-B, and placental growth factor (Plgf),7 and faricimab, a bispecific antibody, inhibits both VEGF-A and angiopoietin-2 (Ang-2).8
Angiopoietin (Ang) and tyrosine kinase with immunoglobulin-like and epidermal growth factor homology domain (Tie) signaling pathways play crucial roles in regulating vascular stability within the retinal vasculature.9 Under normal physiological conditions, Ang-1 facilitates endothelial cell survival and maintains cell junction integrity by interacting with the Tie2 receptors. However, in retinal vascular diseases, upregulation of Ang-2 competitively inhibits Ang-1 binding to Tie2 receptors, thus diminishing the protective effects of the Ang-1 and Tie2 signaling pathways. Additionally, Ang-2 binding to Tie2 stimulates pericyte apoptosis and enhances leukocyte adhesion and transmigration, both of which render the endothelium more susceptible to other pro-inflammatory and angiogenic cytokines, including VEGF-A.10 Consequently, the combined action of Ang-2 and VEGF-A exacerbates vascular leakage and inflammation in DME.11 In this context, simultaneous inhibition of both pathways may enhance vascular stability and improve outcomes beyond the effects of current anti-VEGF therapies, potentially extending the duration of therapeutic efficacy.
In recent years, retinal imaging techniques have undergone significant advancements that have enabled the evaluation of retinal morphology, including visualization of the capillary network and assessment of retinal thickness.12
Laser speckle flowgraphy (LSFG) facilitates two-dimensional, non-invasive measurements of perfusion at the optic nerve head (ONH), retina, and choroid by utilizing the laser speckle phenomenon and has proven instrumental in quantifying ocular blood flow in patients with DR, retinal vein occlusion, age-related macular degeneration, or central serous chorioretinopathy.13–18
In this study, we aimed to evaluate and compare the effects of intravitreal aflibercept (IVA) versus intravitreal faricimab (IVF) on blood flow in the optic nerve head and retinal vessels of the peripapillary region using LSFG in patients with DME. To the best of our knowledge, this is the first study to investigate the effect of intravitreal faricimab on ocular perfusion and compare the effects of different anti-VEGF agents on ocular blood flow one month after injection.
Material and Methods
Setting and Design
This was a retrospective observational clinical study and data were obtained between December 2022 and February 2024. Subjects were Asian individuals treated at Fuchu Hospital, Izumi, Osaka, Japan.
Patients
This study included 20 eyes of 18 patients (33.3% female; mean age 68.7 ± 10.8 years) treated with IVA and 15 eyes of 11 patients (63.6% female; mean age 69.7 ± 12.3 years) treated with IVF for DME. The mean blur rate (MBR) of the ONH and retinal artery and vein of the peripapillary region were measured using LSFG at baseline and 1 month after injection. Central retinal thickness (CRT) and best-corrected visual acuity (BCVA) were measured for all patients. The study protocol adhered to the guidelines of the Declaration of Helsinki and was approved by the ethical committee of Fuchu Hospital (No. 2023007). Given the retrospective nature of this study, the requirement for informed consent was waived and this was approved by ethic committee. The inclusion criteria were (1) age > 18 years, (2) best-corrected visual acuity (BCVA) greater than 0.7 logMAR (logarithm of the minimum angle of resolution) in the study eye at baseline examination, (3) presence of DME, and (4) central macular thickness (CMT) > 280μm as measured using swept-source optical coherence tomography (SS-OCT) at the baseline examination. The exclusion criteria were as follows: (1) any previous ocular surgery in the last 3 months, (2) history of glaucoma, (3) vascular retinal diseases, and (4) medium lens opacities (according to the Lens Opacities Classification System). Pretreatment with intravitreal anti-VEGF was not an exclusion criterion, but the last treatment had to have been received at least three months prior to study inclusion.
Study Protocol
At baseline, all subjects underwent comprehensive ophthalmic evaluation including BCVA, tonometry, slit-lamp biomicroscopy, and indirect fundus ophthalmoscopy. Visual acuity data were obtained in decimal BCVA using Landolt C charts and converted to logarithm of the minimum angle of resolution (logMAR) units for analysis. An SS-OCT device (DRI OCT Triton; Topcon Inc., Tokyo, Japan) was used to measure CRT, which was obtained from the central subfield of the macular thickness map.
The systolic blood pressure (SBP) and diastolic blood pressure (DBP) in the upper arm were assessed using a manometer while the subject was seated. The mean arterial pressure (MAP) was determined using the formula MAP = DBP + 1/3 (SBP − DBP), and the ocular perfusion pressure (OPP) was calculated as OPP = 2/3 MAP − IOP, where IOP represents the intraocular pressure.19
Laser Speckle Flowgraphy
Laser speckle flowgraphy is a noninvasive technique based on the laser speckle phenomenon induced by an 830-nm near-infrared laser, enabling the simultaneous assessment of blood flow in the vessels of the optic nerve head, choroid, and retina.13 The technical principles of LSFG have been explained in detail elsewhere.20
LSFG measurements were performed using an LSFG (LAFG-NAVI, Softcare Co. Ltd., Fukutsu, Japan) with dilated pupils (0.5% tropicamide and 0.5% phenylephrine hydrochloride; Mydrin-P™; SantenPharmaceutical Co. Ltd., Osaka, Japan).
The main output parameter of the LSFG is the mean blur rate (MBR), which represents ocular blood flow and is expressed in arbitrary units (AU). This measurement was derived from the scattering pattern generated when the ocular fundus was exposed to the laser light. MBR represents the velocity of blurring in the speckle pattern caused by the blood flow.21
Analysis of the ONH provides additional capabilities for analyzing data within the rubber band. This software can differentiate between vessels and tissues, enabling the display of mean bloodstream values separately within the elliptical rubber band surrounding the optic nerve head. Using on-board software, the MBR in each composite map was calculated as follows:
MV: mean of vascular area (higher MBR area).
MT: mean of tissue area (lower MBR area).
MA: mean of all areas.
All selected images were meticulously examined by two retinal specialists (T.I. and T.M). To accurately identify arteries and veins by comparing the LSFG image with a color fundus image. As shown in Figure 1, we measured three regions: the optic nerve head (ONH) (1), a selected retinal artery (2), and a selected retinal vein (3). Arteries and veins were selected from locations near the ONH (within 1.5 cm). A rectangular rubber band was used to analyze the blood flow along a single vessel, whereas an elliptical rubber band was placed on the outline around the ONH to assess the flow around the optic nerve head. In this study, we measured the MA, MV, and MT of the ONH: MBR of the retinal artery (MBR-A) and retinal vein (MBR-V) before and 1 month after each injection, as shown in Figure 1. The measurement conditions were kept constant as follows: angle of view, 21°; number of pixels measured, 750×360 pixels. The MBR was calculated automatically using LSFG Analyzer software (version 3.3.30 Softcare Co. Ltd., Fukutsu, Japan). A single measurement is performed for each region.
 |
Figure 1 Representative composite color maps of the MBR measured using LSFG. In these maps, red indicates a high MBR and blue indicates a low MBR. A circle was set around the ONH to measure the MBR of the blood flow in the ONH. Measurements of the retinal artery and vein were taken from sites within 1.5 papilla diameters. LSFG images (a) before and (b) after intravitreal injection. In the color LSFG maps, number 1 indicates the circular scanning area for the optic nerve head, while numbers 2 and 3 indicate the rectangular scanning areas for the retinal artery and vein, respectively. Characteristics of the IVA-treated and IVF-treated groups before and after injection. Abbreviations: S, superior; N, nasal; T, temporal; I, inferior. |
Intervention
Aflibercept 2.0 mg/0.05 mL (Eyler™, Bayer HealthCare) or faricimab 6.0 mg/0.05 mL (Vabysmo™; Roche/Genentech, Basel, Switzerland) was injected into the vitreous cavity of all patients. After instillation of the topical anesthetic (0.4% oxybuprocaine hydrochloride; Benoxil™), all injections were conducted in a procedure room following the standard aseptic intravitreal technique. Aflibercept or faricimab was injected into the vitreous cavity using the standard pars plana approach (3.5 mm posterior to the limbus) with a 30-gauge needle under sterile conditions. Following the treatment, patients were prescribed 0.5% moxifloxacin ophthalmic solution (Vigamox™; Alcon Japan Ltd., Tokyo, Japan) for 3 days.
Follow-Up
Baseline measurements were performed immediately before initial aflibercept or faricimab injections. The patients underwent re-evaluation one month after the first injection. At each follow-up visit, the patients underwent evaluation with LSFG and simultaneous measurement of blood pressure along with IOP measurement, best-corrected visual acuity, and SS-OCT acquisition. Outcome measures included perfusion of the retinal vessels, ONH, and CRT changes. A representative eye with DME is shown in Figure 2.
 |
Figure 2 Swept-source optical coherence tomography (SS-OCT) images (horizontal scan, vertical scan, and thickness map) showing diabetic macular edema (a) before and (b) after intravitreal injection. Abbreviations: N, nasal; T, temporal. |
Statistical Analysis
Descriptive statistics were used to describe the sample in terms of mean and standard deviation (SD). Within-group comparisons were performed using the Wilcoxon signed-rank test and between-group comparisons were performed using the Mann–Whitney U-test. Sex, stage, and phakic eyes were compared using the Fisher’s exact test.
To evaluate the relative changes in the MBR, we used the dMBR, expressed as the rate of change from the baseline values; dMBR was defined as follows:

p < 0.05 were considered statistically significant in all analyses. All analyses were performed using JMP Pro 17 software (SAS Institute, Cary, NC, USA).
Results
The demographics at baseline (before the injection) are shown in Table 1. MAP, IOP, and OPP were stable throughout the follow-up period, as shown in Table 2.
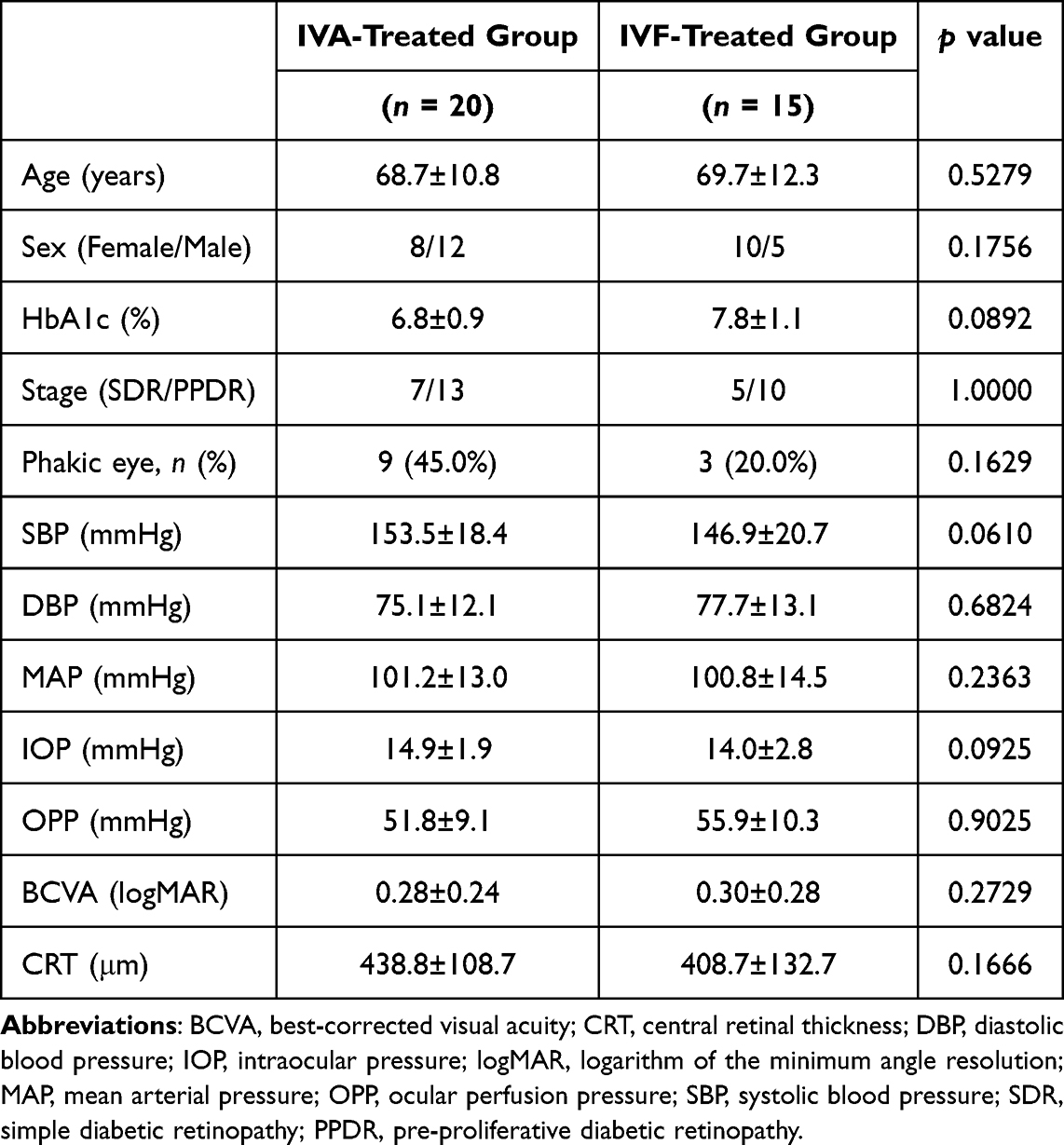 |
Table 1 Comparison of Baseline Demographics of the IVA-Treated and IVF-Treated Groups |
 |
Table 2 Characteristics of the IVA-Treated and IVF-Treated Groups at Before and After Injection |
CRT decreased significantly in the IVA-treated (p = 0.0003) and IVF-treated (p = 0.0004) groups (Table 3). BCVA improved significantly during follow-up (IVA-treated group, p = 0.0178; IVF-treated group, p = 0.0459) (Table 3). Some of the MBR-related parameters of the ONH, such as MBR of all areas (MA), MBR of vascular areas (MV), and MBR of tissue areas (MT), decreased significantly 1 month after IVA and IVF compared to baseline values (MA of IVA, p < 0.0001; MT of IVA, p = 0.0220; MA of IVF, p = 0.0002; MT of IVF, p = 0.0461) (Table 3). MBR of the retinal artery (MBR-A) and vein (MBR-V) decreased significantly 1 month after both IVA and IVF compared to the baseline values (MBR-A of IVA, p = 0.0002; MBR-V of IVA, p = 0.0010; MBR-A of IVF, p = 0.0368) (shown in Table 3). There were no significant differences in dMA, dMV, dMT, dMBR-A, or dMBR-V between the IVA-treated and IVF-treated groups (Figure 3).
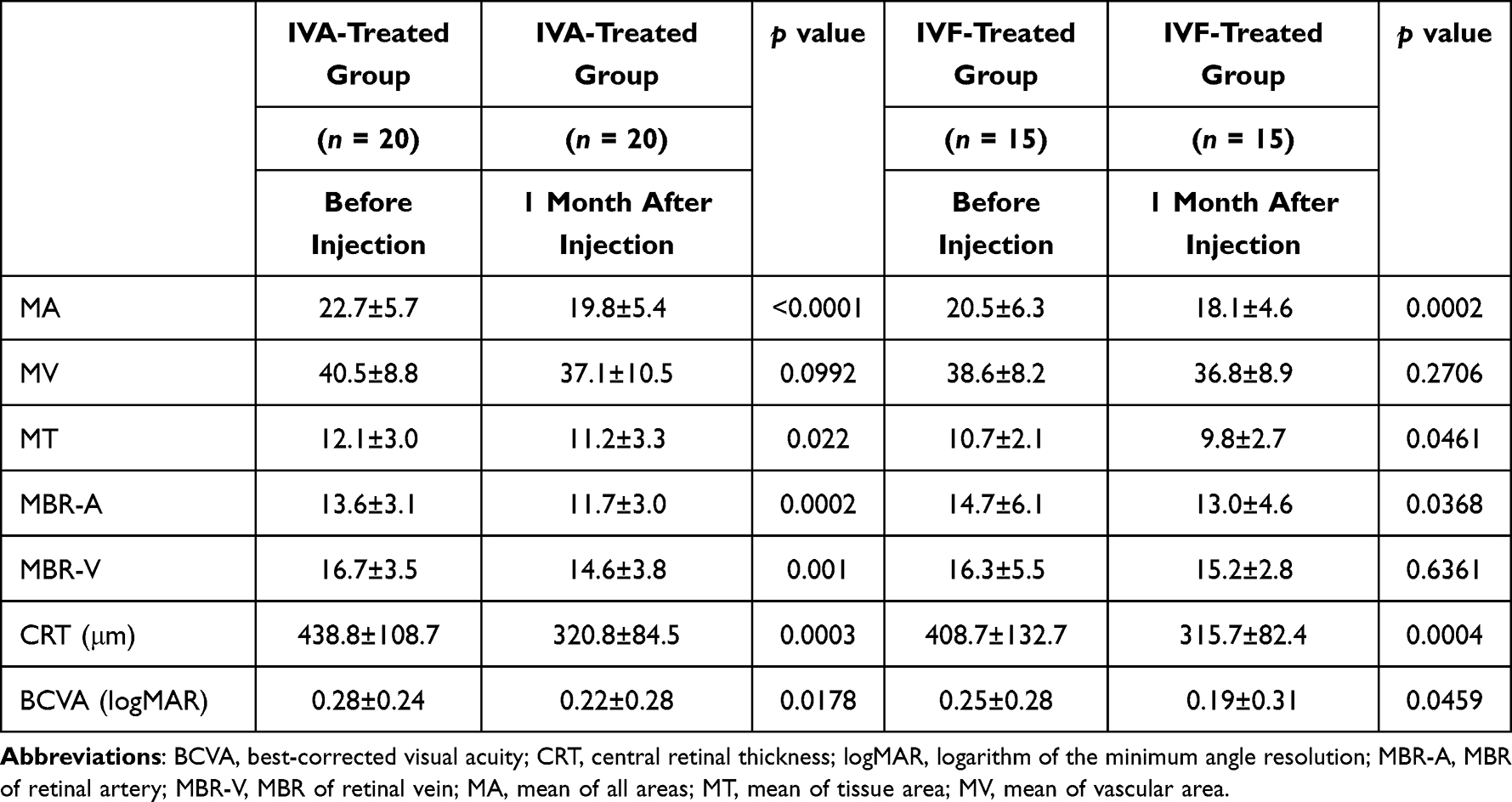 |
Table 3 Baseline characteristics of LSFG and OCT measurements in IVA-treated and IVF-treated groups before and after Injection |
 |
Figure 3 Changes in (a)MA, (b)MV, (c)MT, (d) MBR-A, (e)MBR-V and (f)CRT from baseline to 1 month after injection. Mann–Whitney U-test. * p <0.05. |
No complications stemming from intravitreal injections, such as endophthalmitis, ocular hypertension, retinal detachment, or vitreous hemorrhage, were observed in any of the patients included in this study.
Discussion
In this study, we explored and compared the short-term effects of IVA and IVF on ocular perfusion in DR patients with DME by using LSFG. Additionally, we evaluated changes in central retinal thickness and visual acuity following treatment. Both IVA and IVF led to a significant reduction in perfusion one month later, as measured by LSFG.
The LSFG has been widely used in several ocular disorders to analyze ocular blood flow. Many studies have analyzed the effects of anti-VEGF agents on ocular perfusion in various retinal vascular diseases. Our results are in accordance with those of other published studies of intravitreally administered anti-VEGF agents. IVA for the treatment of neovascular age-related macular degeneration leads to a reduction in perfusion of the ONH and choroid in the treated eye, with no apparent effect on the fellow eye.18 Intravitreal injection of bevacizumab notably reduced blood flow in the ONH, retinal vessels, and choroid in patients with DME, both one week and one month after injection.21 Intravitreal ranibizumab leads to a decrease in ocular blood flow in the ONH and peripapillary retinal vessels, which is related to a reduction in CRT and an improvement in BCVA.15
A recent study compared the effects of different intravitreal injections on ocular perfusion using an LSFG. A decrease in ocular blood flow at the ONH and choroid was observed 30 min after intravitreal injection of brolucizumab and aflibercept. However, there was no significant difference in the rate of decrease in ocular blood flow between the two treatments.22 However, there is currently no research available that compares the mid-term effects of different agents on ocular perfusion, such as one to several months after injections.
In our study, some MBR-related parameters of the ONH, such as MA, MV, MT, MBR-A, and MBR-V, decreased significantly 1 month after IVA and IVF compared to baseline values. As no significant changes in the OPP were observed before and after the injections, ocular perfusion did not affect our findings regarding retinal circulation. Our study indicates that both IVA and IVF resulted in a reduction in retinal blood flow within the vessels of the optic nerve head and peripapillary artery and vein following anti-VEGF injection and that the reduction in retinal microcirculation led to the improvement of macular edema and vision. VEGF is known to act as a vasodilator by activating endothelial nitric oxide synthase.23 Hence, anti-VEGF injections potentially diminish retinal circulation, resulting in alterations in blood vessel caliber via vasoconstriction. Consequently, this process leads to regression of macular edema.24
The effects of intravitreal injection were sustained for up to 30 days; however, we did not observe significant differences in MBR parameter changes between the IVA-treated and IVF-treated groups. A decrease in ocular perfusion was observed 30 days after the ranibizumab injection. Subsequently, an increase in these parameters was noted at 2 months, indicating the temporary nature of anti-VEGF drug action.25 Faricimab simultaneously binds and neutralizes Ang-2 and VEGF-A. By targeting both Ang-2 and VEGF-A, faricimab displays improved and sustained efficacy over longer treatment intervals.26 By following a longer duration, it was possible to observe differences in the IVF-treated group, such as an extended duration of decreased blood flow.
Our study has some limitations, including its retrospective design, short follow-up time, and small sample size. A longer follow-up with a larger cohort of patients is needed to confirm and elucidate any differences in the effects of aflibercept and faricimab injections on ocular perfusion as well as to understand the underlying mechanisms. Most patients had previously undergone anti-VEGF treatment before being enrolled in the trial, and there is a possibility that previous injections had some influence on the effect. Furthermore, we could not include a control group that received intravitreal injections of buffered saline solution or similar fluids due to ethical considerations. It appears highly improbable that the injection procedure itself has a lasting effect on the ocular perfusion. The study population consisted entirely of Asian individuals, which may limit the generalizability of the results to larger DME populations. In addition, the LSFG itself has a notable limitation in that it cannot provide absolute values.
Conclusion
In conclusion, our findings demonstrated that both IVA and IVF resulted in a decrease in ocular blood flow to the optic nerve head and peripapillary retinal vessels, as evaluated using the LSFG. This decrease was associated with a reduction in CRT and improvement in BCVA. No significant difference was observed in MBR reduction between the IVA-treated and IVF-treated groups. Our findings warrant further long-term investigations to reveal differences in ocular circulation modifications between aflibercept and faricimab.
Data Sharing Statement
The data used and analyzed for this study are available from the corresponding author on reasonable request.
Statement of Ethics
This study was conducted in accordance with the principles of the Declaration of Helsinki. The study was approved by the Fuchu Hospital Ethical Committee (Izumi, Osaka, Japan). Institutional Review Board: approval number 2023007. Given the retrospective nature of this study and minimal risks to subjects, the requirement for informed consent was waived and this was approved by ethic committee. The eye center website provided participants with an opportunity to opt out of the study:https://seichokai.jp/fuchu/wp-content/uploads/2023/09/20230928_epi_eye01.pdf. All patient data were handled with strict confidentiality, following ethical standards and institutional guidelines to ensure privacy and data protection.
Acknowledgment
We would like to express our gratitude to the following Certified Orthoptists for their assistance with the examinations: Yuta Sakagawa, Tsubasa Ooishi, Akiko Houkyou, Aya Kotani, Seiya Minai, Kazuho Nagamoto, Hayato Kawano, Shiho Tanabe, Sari Hosomi. This paper was presented at The Association for Research in Vision and Ophthalmology 2024 as a poster presentation. The poster’s abstract was published in ‘Poster Abstracts’ in https://iovs.arvojournals.org/article.aspx?articleid=2793963.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding source to declare.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Romero-Aroca P. Managing diabetic macular edema: the leading cause of diabetes blindness. World J Diabetes. 2011;2(6):98–104. doi:10.4239/wjd.v2.i6.98
2. Photocoagulation for diabetic macular edema. Early treatment diabetic retinopathy study report number 1. early treatment diabetic retinopathy study research group. Arch Ophthalmol. 1985;103(12):1796–1806.
3. Scott IU, Danis RP, Bressler SB, Bressler NM, Browning DJ, Qin H. Effect of focal/grid photocoagulation on visual acuity and retinal thickening in eyes with non-center-involved diabetic macular edema. Retina. 2009;29(5):613–617. doi:10.1097/IAE.0b013e3181a2c07a
4. Schmidt-Erfurth U, Garcia-Arumi J, Gerendas BS, et al. Guidelines for the management of diabetic macular edema by the European society of retina specialists (EURETINA). Ophthalmologica. 2019;242(3):123–162. doi:10.1159/000458539
5. Ferrara N, Damico L, Shams N, Lowman H, Kim R. Development of ranibizumab, an anti-vascular endothelial growth factor antigen binding fragment, as therapy for neovascular age-related macular degeneration. Retina. 2006;26(8):859–870. doi:10.1097/01.iae.0000242842.14624.e7
6. Selid PD, Jundt MC, Fortney AC, Beal JR. Intravitreal bevacizumab and aflibercept for the treatment of exudative age-related macular degeneration. Ophthalmic Surg Lasers Imaging Retina. 2014;45(4):275–281. doi:10.3928/23258160-20140709-03
7. Stewart MW. Aflibercept (VEGF Trap-eye): the newest anti-VEGF drug. Br J Ophthalmol. 2012;96(9):1157–1158. doi:10.1136/bjophthalmol-2011-300654
8. Shirley M. Faricimab: first Approval. Drugs. 2022;82(7):825–830. doi:10.1007/s40265-022-01713-3
9. Saharinen P, Eklund L, Alitalo K. Therapeutic targeting of the angiopoietin-TIE pathway. Nat Rev Drug Discov. 2017;16(9):635–661. doi:10.1038/nrd.2016.278
10. Heier JS, Singh RP, Wykoff CC, et al. THE ANGIOPOIETIN/TIE PATHWAY IN RETINAL VASCULAR DISEASES: a review. Retina. 2021;41(1):1–19. doi:10.1097/IAE.0000000000003003
11. Wykoff CC, Abreu F, Adamis AP, et al. Efficacy, durability, and safety of intravitreal faricimab with extended dosing up to every 16 weeks in patients with diabetic macular oedema (YOSEMITE and RHINE): two randomised, double-masked, Phase 3 trials. Lancet. 2022;399(10326):741–755. doi:10.1016/S0140-6736(22)00018-6
12. Choi W, Waheed NK, Moult EM, et al. Ultrahigh speed swept source optical coherence tomography angiography of retinal and choriocapillaries alternations in diabetic patients with and without retinopathy. Retina. 2017;37(1):11–21. doi:10.1097/IAE.0000000000001250
13. Sugiyama T, Araie M, Riva CE, Schmetterer L, Orgul S. Use of laser speckle flowgraphy in ocular blood flow research. Acta Ophthalmol. 2010;88(7):723–729. doi:10.1111/j.1755-3768.2009.01586.x
14. Okamoto M, Yamashita M, Ogata N. Effects of intravitreal injection of ranibizumab on choroidal structure and blood flow in eyes with diabetic macular edema. Graefes Arch Clin Exp Ophthalmol. 2018;256(5):885–892. doi:10.1007/s00417-018-3939-3
15. Toto L, Evangelista F, Viggiano P, et al. Changes in ocular blood flow after ranibizumab intravitreal injection for diabetic macular edema measured using laser speckle flowgraphy. Biomed Res Int. 2020;2020:9496242. doi:10.1155/2020/9496242
16. Okamoto M, Matsuura T, Ogata N. Choroidal thickness and choroidal blood flow after intravitreal bevacizumab injection in eyes with central serous chorioretinopathy. Ophthalmic Surg Lasers Imaging Retina. 2015;46(1):25–32. doi:10.3928/23258160-20150101-04
17. Nagasato D, Mitamura Y, Semba K, et al. Correlation between optic nerve head circulation and visual function before and after anti-VEGF therapy for central retinal vein occlusion: prospective, interventional case series. BMC Ophthalmol. 2016;16(1):36. doi:10.1186/s12886-016-0211-7
18. Mursch-Edlmayr AS, Luft N, Podkowinski D, Ring M, Schmetterer L, Bolz M. Effects of three intravitreal injections of aflibercept on the ocular circulation in eyes with age-related maculopathy. Br J Ophthalmol. 2020;104(1):53–57. doi:10.1136/bjophthalmol-2019-313919
19. Costa VP, Harris A, Anderson D, et al. Ocular perfusion pressure in glaucoma. Acta Ophthalmol. 2014;92(4):e252–e266. doi:10.1111/aos.12298
20. Luft N, Wozniak PA, Aschinger GC, et al. Measurements of retinal perfusion using laser speckle flowgraphy and Doppler optical coherence tomography. Invest Ophthalmol Vis Sci. 2016;57(13):5417–5425. doi:10.1167/iovs.16-19896
21. Nitta F, Kunikata H, Aizawa N, et al. The effect of intravitreal bevacizumab on ocular blood flow in diabetic retinopathy and branch retinal vein occlusion as measured by laser speckle flowgraphy. Clin Ophthalmol. 2014;8:1119–1127. doi:10.2147/OPTH.S62022
22. Kato N, Haruta M, Furushima K, Arai R, Matsuo Y, Yoshida S. Decrease in ocular blood flow thirty minutes after intravitreal injections of brolucizumab and aflibercept for neovascular age-related macular degeneration. Clin Ophthalmol. 2023;17:1187–1192. doi:10.2147/OPTH.S407249
23. Forstermann U, Sessa WC. Nitric oxide synthases: regulation and function. Eur Heart J. 2012;33(7):829–837,837a–837d. doi:10.1093/eurheartj/ehr304
24. Sugimoto M, Nunome T, Sakamoto R, Kobayashi M, Kondo M. Effect of intravitreal ranibizumab on the ocular circulation of the untreated fellow eye. Graefes Arch Clin Exp Ophthalmol. 2017;255(8):1543–1550. doi:10.1007/s00417-017-3692-z
25. Fukami M, Iwase T, Yamamoto K, Kaneko H, Yasuda S, Terasaki H. Changes in retinal microcirculation after intravitreal ranibizumab injection in eyes with macular edema secondary to branch retinal vein occlusion. Invest Ophthalmol Vis Sci. 2017;58(2):1246–1255. doi:10.1167/iovs.16-21115
26. Khan M, Aziz AA, Shafi NA, Abbas T, Khanani AM. Targeting angiopoietin in retinal vascular diseases: a literature review and summary of clinical trials involving faricimab. Cells. 2020;9(8):1869. doi:10.3390/cells9081869
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.