")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Chronic Marijuana Use and Chronic Obstructive Pulmonary Disease: A Case Report
Authors Ostertag BS , Hendrickson KW
Received 25 February 2025
Accepted for publication 24 June 2025
Published 7 July 2025 Volume 2025:20 Pages 2305—2309
DOI https://doi.org/10.2147/COPD.S520875
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jill Ohar
Brenna S Ostertag,1 Kathryn W Hendrickson2
1Internal Medicine Department, Providence Portland Medical Center, Portland, OR, USA; 2Division of Pulmonary, Critical Care & Sleep Medicine, The Oregon Clinic, Portland, OR, USA
Correspondence: Kathryn W Hendrickson, Division of Pulmonary, Critical Care & Sleep Medicine, The Oregon Clinic, 1111 NE 99th Ave #100, Portland, OR, 97220, USA, Email [email protected]
Abstract: Marijuana smoking has become increasingly common in the United States and the world as more states and countries have legalized it for medical and recreational use. There are a number of carcinogens in marijuana smoke similar to those in tobacco smoke, and yet it has been difficult in the literature to find a causal relationship between marijuana smoking and chronic obstructive pulmonary disease (COPD). We present a patient whose main risk factor for emphysema is daily marijuana smoking for upwards of 35 years with no personal history of smoking tobacco, and no other obvious risk factors. Current studies have shown association with chronic marijuana smoking and various lung complaints, forced expiratory volume in 1 second (FEV1) to forced vital capacity (FVC) ratio, and inconsistently with chronic bronchitis. With this case, we add to the current body of literature that suggests a possible relationship between long-term, heavy marijuana use and COPD.
Keywords: carcinogens, chronic obstructive pulmonary disease, emphysema, marijuana, smoking
Introduction
The use of marijuana has increased in prevalence in the United States (US), with 24 states making it legal for recreational use and another 12 states making it legal for medical use as of 2024.1 Marijuana is now the second-most smoked substance in the US, second to tobacco.2 Worldwide, there are an estimated 192 million users of cannabis as of 2018, with highest use among the US, European countries, and less so across Asia where use remains lower.3 Additionally, in the United States, between 2008 and 2022 the per capita rate of reported past-year use increased by 120% and the per capita days of use increased by 210%. Between 1992 and 2022 there was a 15-fold increase in the per capita rate of reported daily or near daily use of marijuana.4 We are encountering a growing population of patients impacted by marijuana and its health effects.
Smoke from marijuana contains many pulmonary carcinogens including phenols, aldehydes, acrolein, benzpyrene, and benzanthracene. These chemicals are also found in tobacco cigarettes and are known to cause lung disease.2 Histologically, chronic marijuana smokers have been shown to have increased number and size of submucosal blood vessels corresponding with submucosal edema, and hyperplasia of goblet cells, as well as an increased number of alveolar macrophages with altered structure and function indicating response to increased airway inflammation, which is also seen in tobacco smokers.5
Despite increasing numbers of marijuana users being exposed on a regular basis to these chemicals, data and opinions are mixed in regard to the link between marijuana and chronic lung disease.6 We present a case of a heavy marijuana smoker with severe obstructive lung disease to add to the literature and encourage ongoing discussions and research into this important topic.
Case Report
A 64-year-old man who worked as a liquor store clerk presented to pulmonary clinic for evaluation of dyspnea on exertion (DOE). He reported progressive DOE for the prior 10 years. This progressed from dyspnea when carrying heavy objects to not being able to walk up a flight of stairs at the time of initial presentation to pulmonary clinic. He reported no significant cough but did hear wheezing at night. Physical exam revealed decreased air movement throughout both lung fields with no wheezes. Chest X-ray revealed hyperinflation of the lungs (Figure 1). Spirometry revealed a forced expiratory volume in 1 second (FEV1) to forced vital capacity (FVC) ratio of 38, an FEV1 of 1.18 L (33%), and an FVC of 3.12 L (65%). He had a normal DLCO on full pulmonary function testing (see Figure 2 for complete details). There was no significant response to inhaled bronchodilators. Computed tomography of the chest revealed mild-moderate emphysema with slight upper lobe predominance (Figure 3). Alpha-1-Antitrypsin level was within normal limits. Past medical history included psoriasis and psoriatic arthritis previously treated with prednisone and methotrexate, which were stopped due to fatigue. Etanercept was started for one month which was also stopped due to fatigue. He had started and continued ustekinumab with good control of his symptoms. Social history revealed a minimal history of secondhand tobacco smoke exposure as a child with his father smoking around him, although not regularly in the home. He moved out of the house as a teenager and the patient himself had no personal history of tobacco smoking. He worked various jobs throughout his life including as a painter, and most recently as a clerk at a liquor store. He never served in the military. He reported 35 years of near-daily marijuana use. A water pipe was used to smoke the marijuana 3–5 times daily during this time. He stopped smoking as his respiratory symptoms worsened.
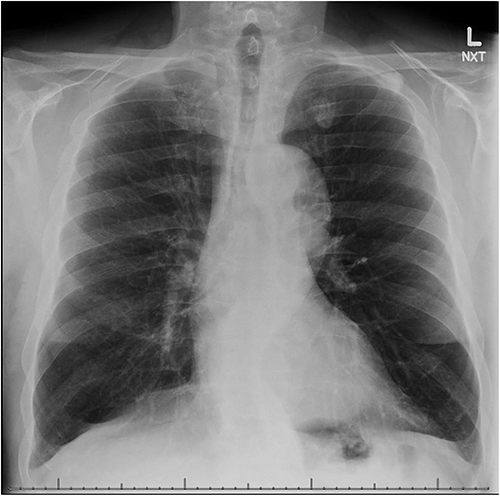 |
Figure 1 Chest X-ray demonstrating hyperinflation of the lungs. |
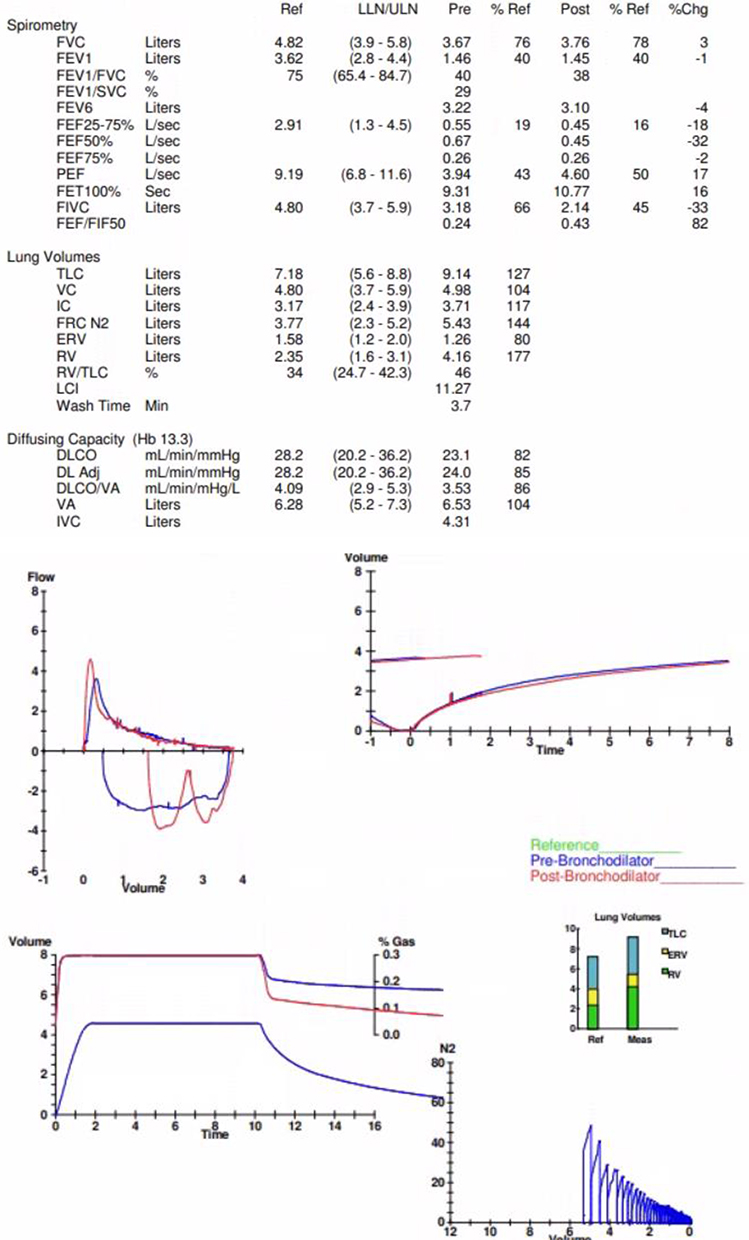 |
Figure 2 Full pulmonary function testing at time of presentation to pulmonary clinic. |
 |
Figure 3 Coronal and axial chest computed tomography imaging demonstrating bullous emphysema. |
Discussion
We present this case of a patient with very severe obstruction due to emphysema without significant personal tobacco history, secondhand tobacco exposure, or Alpha-1-Antitrypsin deficiency. There are no case reports of prednisone or Ustekinumab causing obstructive lung disease. There are case reports of both etanercept7 and methotrexate8 causing asthma; however, for both medications the obstruction reversed with stopping the medication, making these less likely causes of his chronic obstructive pulmonary disease (COPD). This leaves his chronic marijuana use as the most likely cause of his COPD.
A systemic review and meta-analysis of studies linking secondhand smoke exposure and COPD by Chen et al in 2023 determined an increased risk for COPD with even <5-year duration of secondhand smoke exposure, particularly among women. There was significant heterogeneity amongst these studies in amount of exposure, age of exposure, and length of exposure, making it difficult to know if our patient fits this group. After leaving his home as a teenager, he went on to become a competitive multi-sport athlete, including in running. He had a long and successful athletic career and did not develop respiratory issues until later in life following years of marijuana use and zero secondhand cigarette exposure as an adult, making us believe that secondhand smoke exposure as a child may have put him at greater risk of developing COPD but was not the main cause of his disease.9
Due to the many confounding variables in this population, including concomitant tobacco use, differences in methods of use, and differences in frequency and length of use, studies are inconsistent in linking marijuana use and lung disease. Although some studies seem to show symptoms of chronic bronchitis in heavy users, this is not consistent across studies.10 Polen et al looked at a cohort of 452 marijuana smokers who never smoked tobacco and compared them to 450 demographically similar never smokers of either substance. They noted an increase in outpatient encounters for respiratory complaints among the marijuana users, although did not define these further.11 Like many other cohorts, these patients tended to be younger (<35 years of age) resulting in far less years of use than our patient.
In their Subpopulations and Intermediate Outcome Measures in COPD Study (SPIROMICS), Morris et al found an increase in FEV1 and FVC among current and former marijuana users; however, they note that their study could not comment on lung function changes among long-term, heavy marijuana only smokers.12 Bullous lung disease has been reported in several case reports and thought to be related to the large volume breath holds smokers employ.13 Proving a causal relationship is difficult; however, with our patient’s use of a water pipe we postulate his years of marijuana use and breath holds may have contributed to his emphysema.
Conclusion
The current literature is incomplete and inconclusive on the relationship between marijuana and lung disease, though there is more and more evidence to suggest an association. Additionally, there has been an increase in potency of marijuana over the years, which may be contributing to an increase in demonstration of lung disease in heavy use individuals, and even in those with lighter use. A US study reviewed changes in potency of marijuana from 1995 to 2014 and found that overall potency has increased in cannabis plant material from 4% in 1995 to around 12% in 2014.14 Additional studies should determine if there is a method of use, amount, or number of years that puts our patients at risk for COPD due to marijuana smoking so that we can better counsel them on their use of this common substance.
Abbreviations
COPD, Chronic obstructive pulmonary disease; DOE, Dyspnea on exertion; FEV1, Forced expiratory volume in 1 second; FVC, Forced vital capacity.
Consent for Publication
The patient described in this manuscript has reviewed and consented to publication of its contents. Institutional approval was not required to publish this case.
Acknowledgments
This case report has not been published and is not under consideration for publication elsewhere. We have no conflicts of interest to disclose. All authors have a) contributed substantively to the content of this report, b) contributed substantively to the drafting of the report or critical revision for important intellectual contact, c) given final approval of the version to be published.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Johnston M. U.S. Marijuana Laws by State. Available from: https://www.britannica.com/topic/US-marijuana-laws-by-state.
2. Tashkin DP. Marijuana and Lung Disease. Chest. 2018;154(3):653–663. doi:10.1016/j.chest.2018.05.005
3. Ransing R. Current state of cannabis use, policies, and research across 16 countries: cross-country comparisons and international perspectives. Trends Psychiat Psychother. 2022;24(Suppl 1):1–14.
4. Caulkins JP. Changes in self-reported cannabis use in the United States from 1979 to 2022. Addiction. 2024;119(9):1648–1652. doi:10.1111/add.16519
5. Tashkin DP. Smoked Marijuana as a Cause of Lung Injury. Monaldi Arch Chest Dis. 2005;63(2):93–100. doi:10.4081/monaldi.2005.645
6. Joshi M, Joshi A, Bartter T. Marijuana and the Lung: some Known Knowns. Chest. 2023;163(2):e105. doi:10.1016/j.chest.2022.09.045
7. Torres T, Vilaça S, Velho G, et al. Etanercept-induced asthma in a psoriatic patient resolving with transition to ustekinumab. Eur J Dermatol. 2012;22(5):696–697. doi:10.1684/ejd.2012.1816
8. Jones G, Mierins E, Karsh J. Methotrexate-induced asthma. Am Rev Respir Dis. 1991;143(1):179–181. doi:10.1164/ajrccm/143.1.179
9. Chen P, Li Y, Wu D, et al. Secondhand Smoke Exposure and the Risk of Chronic Obstructive Pulmonary Disease: a Systematic Review and Meta-Analysis. Int J Chron Obstruct Pulmon Dis. 2023;2023(18):1067–1076. doi:10.2147/COPD.S403158
10. Tetrault JM. Effects of marijuana smoking on pulmonary function and respiratory complications: a systematic review. Arch Intern Med. 2007;167(3):221–228. doi:10.1001/archinte.167.3.221
11. Polen MR, Sidney S, Tekawa IS, et al. Health care use by frequent marijuana smokers who do not smoke tobacco. West J Med. 1993;158(6):596–601.
12. Morris MA, Jacobson SR, Kinney GL, et al. Marijuana Use Associations with Pulmonary Symptoms and Function in Tobacco Smokers Enrolled in the Subpopulations and Intermediate Outcome Measures in COPD Study (SPIROMICS). Chronic Obstr Pulm Dis. 2018;5(1):46–56. doi:10.15326/jcopdf.5.1.2017.0141
13. Hii SW, Tam JDC, Thompson BR, et al. Bullous lung disease due to marijuana. Respirology. 2008;3(1):122–127. doi:10.1111/j.1440-1843.2007.01186.x
14. ElSohly MA, Mehmedic Z, Foster S, et al. Changes in Cannabis Potency over the Last Two Decades (1995–2014) - Analysis of Current Data in the United States. Biol Psychiatry. 2016;79(7):613–619. doi:10.1016/j.biopsych.2016.01.004
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Contributions of Emphysema and Functional Small Airway Disease on Intrapulmonary Vascular Volume in COPD
Huang X, Yin W, Shen M, Wang X, Ren T, Wang L, Liu M, Guo Y
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1951-1961
Published Date: 25 August 2022
Phenotyping COPD Patients with Emphysema Distribution Using Quantitative CT Measurement; More Severe Airway Involvement in Lower Dominant Emphysema
Park J, Kim EK, Lee SH, Kim MA, Kim JH, Lee SM, Lee JS, Oh YM, Lee SD, Lee JH
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2013-2025
Published Date: 31 August 2022
Clinical and Radiological Features Between Patients with Stable COPD from Plateau and Flatlands: A Comparative Study
Jiang Z, Wang X, Zhang L, Yangzom D, Ning Y, Su B, Li M, ChuTso M, Chen Y, Liang Y, Sun Y
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:849-858
Published Date: 12 May 2023
COPD Risk Factor Profiles in General Population and Referred Patients: Potential Etiotypes
Lee JH, Kim S, Kim YJ, Lee SW, Lee JS, Oh YM
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2509-2520
Published Date: 9 November 2023
Factors Associated with Chronic Obstructive Pulmonary Disease: A Hospital-Based Case–Control Study
Twinamasiko B, Mutekanga A, Ogueri O, Kisakye NI, North CM, Muzoora C, Muyanja D
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2521-2529
Published Date: 10 November 2023