")
Back to Journals » Clinical Ophthalmology » Volume 18
Climate and Rhegmatogenous Retinal Detachment: A Comprehensive Review and Future Research Guidelines
Authors Aharonian K, Krasner H , Martin J , Batra K , Yepremyan M
Received 27 June 2024
Accepted for publication 16 September 2024
Published 29 October 2024 Volume 2024:18 Pages 3083—3095
DOI https://doi.org/10.2147/OPTH.S476142
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr John Miller
Karl Aharonian,1 Henry Krasner,1 Jeffrey Martin,1 Kavita Batra,1,2 Meher Yepremyan1
1Department of Medical Education, Kirk Kerkorian School of Medicine at UNLV, Las Vegas, NV, USA; 2Office of Research, Kirk Kerkorian School of Medicine at UNLV, Las Vegas, NV, USA
Correspondence: Karl Aharonian, Email [email protected]
Purpose: Does weather affect the rate of developing rhegmatogenous retinal detachment (RRD)? This comprehensive review investigates the findings of the most recent studies on the relationship between RRD and climatic or seasonal factors.
Methods: An extensive search across PubMed, Embase, and Google Scholar databases resulted in 112 initial results, from which 18 studies published between 1980 and 2024 were selected. The selection criteria were based on the studies’ relevance to our topic. We analyzed their methodology, geographic scope, and key findings. Data extraction encompassed study design, sample size, sex ratio, incidence rates, results, and identified limitations.
Results: Eight studies found no statistically significant relationship between seasonal variations and the incidence of RRD. Conversely, seven studies reported an increased incidence of RRD during the summer months. Additionally, secondary analyses of factors, such as ambient temperature, atmospheric pressure, and daylight hours, showed varied and sometimes conflicting results. A summary of common limitations and biases was synthesized into a table, providing guidelines for future research exploring this topic.
Conclusion: This comprehensive review highlights the complex interaction between environmental factors and RRD incidence. The conflicting results across different studies suggest a need for further research in this area. Future studies should address the identified limitations and biases to provide a clearer understanding of the relationship between climate and RRD. By utilizing the guidelines from our review, future research could aim to minimize confounding factors and improve the robustness of their findings. Understanding these interactions can be used to develop preventive strategies and enhance clinical practices to reduce the burden of RRD.
Keywords: rhegmatogenous retinal detachment (RRD), climate, seasonality, temperature
Introduction
Rhegmatogenous retinal detachment (RRD) represents one of the most common yet critical emergencies in ophthalmology, posing a significant threat to vision if not promptly and effectively treated. Historically, the prevalence of RRD in the United States (US) is estimated to range from 8.0 to 18 cases per 100,000 individuals.1–3 RRD is characterized by the detachment of the neurosensory layer from the underlying retinal pigment epithelium (RPE). This detachment occurs due to the presence of one or more retinal breaks or tears, through which vitreous fluid passes and accumulates in the subretinal space, leading to the physical separation of the neurosensory retina from the RPE. This separation disrupts the metabolic exchange between these two layers, essential for retinal photoreceptor function, leading to visual impairment.4,5 The urgency of addressing RRD lies in its potential to cause irreversible blindness in the affected eye if left untreated.5 Due to its potentially insidious yet severe damage to vision, the risks factors, and correlations of RRD have been meticulously explored. Clinicians and scientists have been making ongoing efforts to improve clinical outcomes and, more importantly, to prevent such cases from occurring in the first place.
However, the multifactorial nature of RRD complicates these efforts significantly. It encompasses several well-established risk factors that contribute to its development. These include ocular trauma, often resulting from sports activities, and complications following cataract surgery.6–8 Other significant risk factors extend to myopia, age, genetic predispositions, and previous ocular conditions, which can all weaken the retinal structure and predispose individuals to retinal tears and detachment.9–13 Despite the known risk factors, the influence of ambient temperature on RRD incidence has emerged as a subject of scientific inquiry.
There are several hypotheses describing the plausible biological mechanisms of seasonal variations influencing the occurrence of RRD14–19 (See Figure 1). One such hypothesis is temperature fluctuations affecting the vitreous body’s consistency, potentially leading to increased vitreous liquefaction during warmer periods. This process can accelerate posterior vitreous detachment (PVD), a primary precursor to RRD.14,15 Another hypothesis is that UV light induced free radical injury to the vitreous as a cause of cascade downstream effect. Furthermore, seasonal changes in intraocular pressure, influenced by eye temperature variations, could contribute.16 Additionally, a decrease in sub-retinal cortisol levels has been proposed as another mechanism increasing the risk of retinal tears.17
 |
Figure 1 Plausible Mechanisms of Seasonal Influence on Rhegmatogenous Retinal Detachment (RRD) Risk. |
Although there is no clear consensus on the mechanism of the meteorological impact on RRD, in recent decades, this relationship has been explored across various geographic regions. As a result, there is a plethora of studies with varying methodologies and conclusions. A notable attempt to synthesize these findings was made by Qassim et al in 2016, reviewing some of the existing literature up to that point.20 Their work summarized key findings and highlighted the impact of ambient temperature on RRD, yet acknowledged the conflicting conclusions of these studies. To the authors’ best knowledge, there has not been a recent comprehensive review since their study.
Since the publication of Qassim et al’s review, numerous new studies incorporating data from previously unassessed geographic areas have emerged, warranting a new evidence synthesis using the most recent findings.20 This study aims to bridge the gap by including the latest research and exploring key findings of studies conducted in the interim. This involves examining whether certain times of the year are associated with higher rates of RRD due to factors, such as changes in ambient temperature, variations in outdoor activity levels, or other seasonal behaviors that may affect the risk of ocular traumas. The analysis will also consider how these seasonal patterns might vary across different climates and geographical regions, reflecting the complex interplay between environmental factors and the pathophysiology of RRD. Furthermore, this study will discuss the broader implications of understanding seasonal variations in RRD occurrence and provide suggestions for future research to fill in the gap of data yet to be explored.
Understanding the seasonal patterns of RRD can offer valuable insights into preventive strategies and inform clinical practice, potentially reducing the incidence of this vision-threatening condition. By advancing knowledge in this area, physicians can better educate patients at risk and develop targeted preventive measures, ultimately aiming to reduce the burden of RRD on individuals and healthcare systems. The comprehensive literature search proposed above is a timely and essential update for advancing our understanding of RRD. By reviewing and synthesizing the latest findings, this study will contribute significantly to this evolving topic of scientific inquiry.
Methods
Search Strategy
The electronic databases PubMed, Embase, and Google Scholar were searched in April 2024 to identify potentially relevant articles. The main search terms used were “Rhegmatogenous Retinal Detachment” and “Climate.” Related terms for “Rhegmatogenous Retinal Detachment” included “Retinal Detachment”, while “Climate” was associated with related terms, such as “Meteorological”, “Occurrence”, “Seasonal”, “Seasonality”, “Temperature”, and “Variation.” The main search terms were combined using the Boolean operator “AND”, and the related search terms were combined using “OR.”
Inclusion and Exclusion Criteria
The inclusion criteria of this study were the following: (1) articles written in English or translated in English, (2) articles published in peer-reviewed journals, (3) articles related to the relationship between rhegmatogenous retinal detachment and climate, (4) articles published between 1980 and 2024. Studies that did not meet these criteria were excluded. In addition, reviews, meta-analyses, abstracts-only studies, animal studies and those conducted in-vitro were excluded from this review.
Study Selection
Upon identifying the articles that met these criteria, publication abstracts were screened for relevance to our study aim.
Data Abstraction
Sample size, geographic locations, study duration, and key findings were considered when screening abstracts. If found to be relevant, researchers read the full texts thoroughly and collected relevant data points in a data extraction matrix created by the research team. A graphic depicting this literature search and article selection process is outlined in Figure 2 and flow chart diagram (Figure 3).
 |
Figure 2 Flow diagram of the publication search and selection process. |
 |
Figure 3 Flow diagram of the screening and selection process. |
Results
Results of Study Selection
Eighteen articles were ultimately included in this study. Studies were ultimately selected for inclusion based on their relevance, study design, and specific geographic locations. The data points collected for the data extraction matrix consisted of year of publication, data collection window, location (country/city), sample size, sex ratio (M:F), defined incidence rate, and key findings, specifically seasonal incidence rate and found association, if any. This data can be visualized in Table 1.9,21–33
 |
Table 1 Table Summarizing Data Extraction & Key Findings |
Characteristics of Included Studies
Geographic Scope
This review analyzed 18 studies, revealing a predominant focus on the regional or city-level impact of RD and its seasonal variations. Notably, only four studies—by Ghezala et al, Saraf et al, Choo et al, and Lin et al—expanded their scope to encompass entire countries.19,30,32,33
Geographic distribution of the included studies spans several continents: Asia (5, 28%), Europe (4, 22%), and Scandinavia & Northern Europe (3, 17%); the remaining 33% consist of North America (2), the Middle East (2), Eurasia (1), and Australia (1), showcasing a diverse range of environmental contexts.
Study Design
Among the included studies, nine were retrospective chart reviews, the most common design. Paavola et al and Törnquist et al, respectively, identified their studies as a comparative study and a population-based series.15,22 Recent trends show a preference for nationwide models, as demonstrated by Ghezala et al, Lin et al, and Saraf et al, all utilizing some sort of nationwide database designs.19,32,33 Auger et al introduced a multicenter case-crossover study, while Manners et al performed a whole-population retrospective observational study.26,27 Notably, only one study, by Li et al, employed a prospective approach, conducting a population-based incidence study to assess incidence rates and associations.9
Patient Demographic
The analysis of patient demographics revealed a general trend in age distribution, with most studies reporting a mean age between 50 and 60 years, which is expected considering the pathophysiology of RD. An outlier was noted in the study by Al Samarrai, which reported a mean age of 41.1 years in Kuwait—the lowest among the studies reviewed.23 Regarding gender distribution, males were more frequently associated with RD in 11 studies. This male predominance contrasts with findings from the 1980s, where every study, except for the one conducted in the Novosibirsk region by Paavola et al identified females as the demographic more likely to develop RD.15 The remaining three studies did not report sex ratios in their results.
Incidence Estimate
In the reviewed studies, the prevalent approach for estimating the incidence of RRD involved quantifying the number of cases within specified time intervals, including months, trimesters, seasons, or other predetermined periods. On the contrary, a minority of studies—namely those conducted by Ghezala et al, Lin et al, and Li et al—adopted a method of calculating incidence rates as the proportion of cases relative to the sample size against a broader population metric.9,19,32
Seasonality Findings of Included Studies
In the evaluation of the 18 selected studies, seven identified a statistically significant correlation of RRD incidence during the summer, with some noting overlapping periods extending into spring and fall, as detailed in Table 1. Remarkably, only one study, by Choo et al, discovered a statistically significant association specifically in spring, in the month of March.30 Similarly, the research conducted by Al Samarrai highlighted a significant association during the winter23 Unique in its approach, the study by Prabhu & Raju designated the summer season as spanning March through May, within which they found a significant association.16 Conversely, eight studies reported no significant association between weather conditions and the incidence of RRD.
Additional Findings of Included Studies
Some of the included studies explored beyond primary objectives and set a range of secondary aims, notably investigating the potential impact of meteorological factors—such as ambient temperature, atmospheric pressure, daylight hours, humidity, and precipitation—on the incidence of RRD. However, these studies presented conflicting results regarding the association between RRD incidence and these environmental variables. For example, Ghisolfi et al identified a positive correlation between light flux and RRD incidence, suggesting that increased exposure to light could elevate the risk of RRD.17 Contrarily, Choo et al observed a bimodal distribution of RRD incidence in relation to daylight hours, indicating peaks during specific times of the year.30 Meanwhile, Al Samarrai reported an inverse relationship, with lower RRD incidence associated with longer daylight hours, highlighting the complex and conflicting nature of these relationships.23 However, one meteorological factor has been observed to have an inverse relationship with RRD incidence: atmospheric pressure. Lin et al and Iida et al have found that low atmospheric pressure was associated with increased cases of RRD.19,31
Despite the varied findings on meteorological influences, several studies affirmed well-established risk factors for RRD. High myopia and advanced age were consistently linked with an increased risk of developing RRD, echoing findings from earlier pathophysiological research (insert citations). An interesting association was reported by Choo et al, who found that patients with atopic dermatitis exhibited the highest prevalence of RRD during the summer and the lowest during the fall—a pattern that diverges from the general population trend reported in their study, which typically peaks in spring.30
This exploration of secondary study objectives underscores the intricate interplay between environmental factors and RRD incidence. As of yet, no single meteorological factor has emerged as a consistently significant predictor across multiple studies, suggesting the need for further research to unravel these complex associations and potentially integrate environmental considerations into RRD risk assessment and prevention strategies.
Discussion
The primary objective of this study was to identify the relationship between RRD and climate or other seasonal factors by performing a comprehensive analysis of relevant literature. This study provides additional insight into the current state of knowledge by including a detailed investigation of more recent studies. By providing this insight into the relationship between RRD and climate, novel and improved interventions may be developed to specifically cater to RRD patients with relevant risk factors.
Seasonality and RRD
The major significant finding of this project relates to the significance of the relationship between climate and RRD incidence. Since the study conducted by Qassim et al, there have been eight additional studies conducted on a global scale regarding the intersection of RRD and climate, which is double the amount of literature included in the previous review.20 While it was previously found that the predominant season associated with RRD was the summer, our analysis found no statistically significant association between season and RRD incidence. Yet, due to the limited studies available for evaluation and the closeness of significant vs non-significant results, it is apparent that more studies must be conducted in order to more accurately assess this relationship.
Another important consideration for the findings is the seasonality of PVD. It could be argued that seasonality of PVD is a major finding as the majority of RRD cases are preceded by PVD.34 Such a study was conducted by Rahman et al based on 567 cases of RRD over a 2 years period. They found a highly significant correlation between weekly average temperatures and the incidence of PVD.35 In the studies included in this review, all of them acknowledged PVD as a risk factor and consideration for development of RRD; however, only Saraf et al looked at PVD cases as a separate variable.33 The findings did not show any significant increase with any season. Future studies could focus on PVD as a separate variable to assess the seasonality of RRD due to the clear temporal and pathophysiological relationship between these two conditions.
Other Findings
In addition to the relationship between season and RRD incidence, many of the included studies also reaffirmed known risk factors for RRD, including myopia and advanced age. Such associations are not novel as the pathophysiologic pathway is known to connect the risk factors with RRD development. In particular, myopic eyes, specifically at a high stage, have an increased posterior segment volume, which creates traction of the vitreous gel on the retina.13 Increased axial length of the eye further increases the risk of PVD and subsequent RRD. Aging affects RRD likely via progressive age-related degeneration of vitreous and as a general consequence of PVD. Finally, the male sex appears to be associated with an increased risk of RRD, as seen in all but one study included in this review. One theoretical explanation for this phenomenon is that males typically have longer ocular axial length.36
However, this finding may be due to a physiological or even behavioral pattern as well, requiring additional research.
Other significant findings regarding the relationship between meteorological factors such as light flux and daylight hours and RRD incidence varied among studies. One factor, atmospheric pressure, was found to have a negative correlation with the incidence of RRD.19,31 While several studies found statistically significant associations between meteorological parameters and RRD incidence, conflicting data among the few studies present create a challenge to establishing any clear consensus.
State of Prevention Guidelines and Interventions
Current research has identified that although RRD is unpreventable, there are certain steps that are recommended to lower individuals’ risks. It is advised for individuals to ensure compliance with regular eye exam recommendations, especially in individuals with nearsightedness, as myopia is a major risk factor for RRD.37–40 Furthermore, current recommendations advise that maintenance of overall health and well-being as well as utilization of ocular safety equipment when participating in risky activities.40,41 However, the most important risk factor in developing RRD still appears to be related to age.42 Therefore, the measures mentioned above are even more important to follow for patients over the age of 50 years old.
However, there are minimal preventative interventional strategies currently in place due to the sudden and typically unpreventable nature of RRD, especially in populations where climate may predispose them to RRD. Interventions for RRD are primarily aimed at treating RRD efficiently after the onset, with treatment options including scleral buckle, vitrectomy, or laser photocoagulation.5,43,44 Many studies propose that improving patient education in at-risk individuals, especially children, may be the most valuable intervention in reducing RRD occurrence and burden.45–47 Developing and refining interventions such as improving patient education accessibility on an individualized or community-level basis, as well as continuing research regarding optimal treatment techniques, may improve patient outcomes in RRD, especially in geographic regions that may be exceptionally vulnerable due to climate-based risk factors.
Biases and Limitations
Study Design
The studies conducted so far on this topic have been predominantly of retrospective chart review style. In fact, only one study conducted a prospective study. Although there are disadvantages with retrospective design, it is a common choice due to its relatively inexpensive cost and ease. Regardless of the study design, there are several biases that must be considered by studies to provide stronger correlations. The list of such biases/limitations is presented in Table 2.
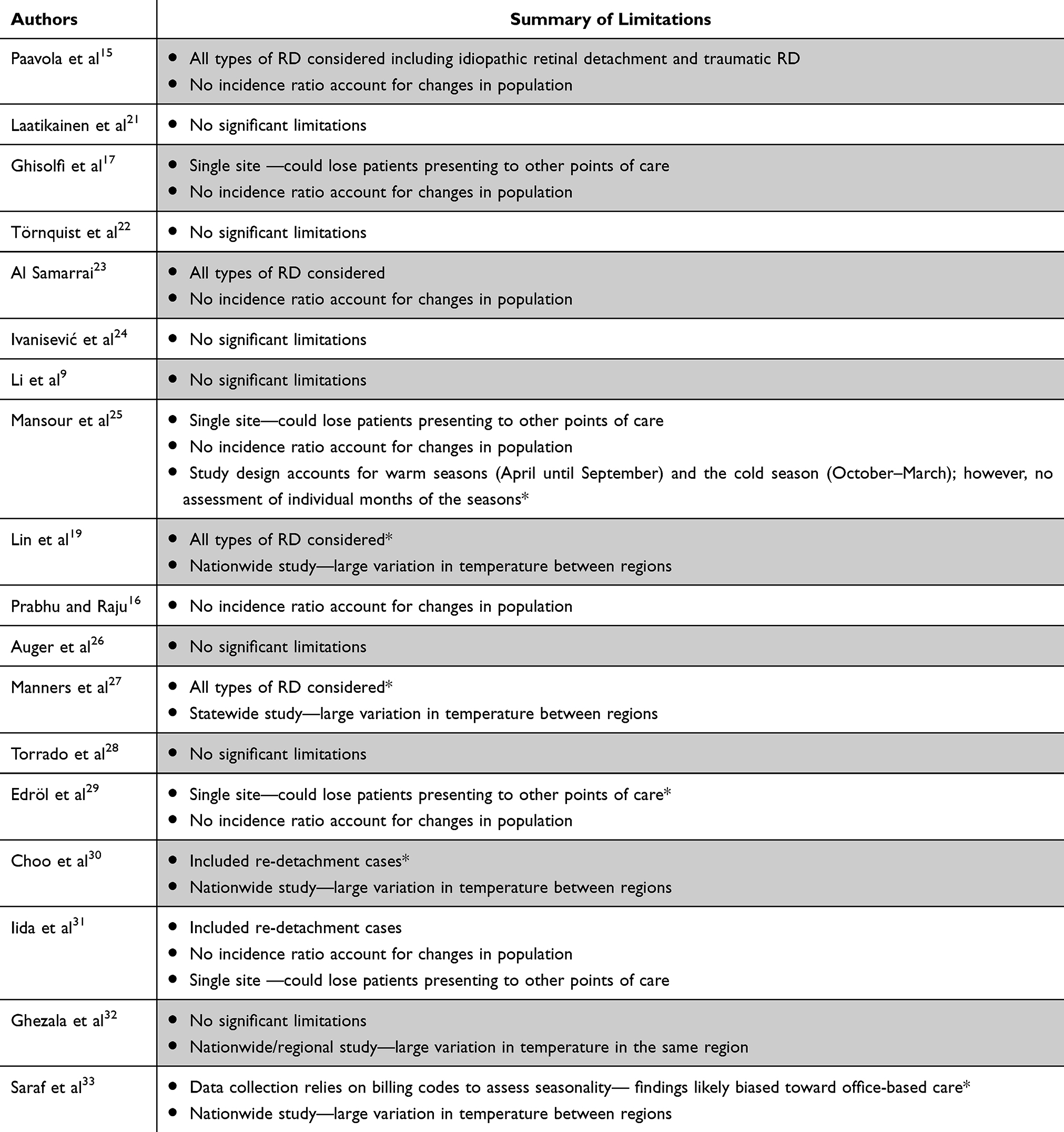 |
Table 2 Table Summarizing Common Limitations |
One particularly common limitation of studies in this review was the insufficient approach to account for population fluctuations and seasonal changes in patient numbers. It is not uncommon for patients to travel more during different months and seasons. Patients can also refer to other sites of care, if the study conducted does not include all of the major points of care in their location. Additionally, variation in physician availability is another factor that may impact the number of patients seen per month. Due to these reasons, studies could account for this significant confounding factor in either of the two ways:
- Conducting a study in a location that is served only by one site or multiple sites that are included in the chart review while also accounting for changes in population number.
- Estimating the number of overall patients seen for ophthalmological issues in the site/multiple sites and calculating corresponding incidence rate of RRD among this population.
Another limitation that was observed in the included studies is the lack of data to exclude non-rhegmatogenous cases of RD. This serves particular importance as ocular trauma is a risk factor for developing traumatic RD and also RRD.48–53 Considering that any population is more likely to engage in sport activities or other forms of recreation during mild and warm weather, traumatic RD cases could cause a rise in seasonal incidence of RD without clear association with the meteorological factors.
Geographic Area and Weather
An important consideration for limitations is the area where the study aims to find associations. Although it is certainly beneficial to collect data from various geographical locations, one interesting pattern was seen in this review: there are only two studies conducted in extreme weather conditions, Törnquist et al and Al Samarrai. Most studies included in the review report data from locations with mild temperatures. The importance of this observation lies behind the hypothesis of these studies. If seasonal association between ambient temperature and incidence of RRD is present, it must display a stronger association with weather conditions that display extreme temperature. In other words, if a study is done in a hot climate, it would be logical to expect a stronger case for incidence of RRD in summer while if the climate is in extreme cold range, it would be expected that such association would fade. Additionally, such study location would likely limit the impact of recreational changes that occur in warm weather increasing risk of ocular trauma. In our review, only one study, Al Samarrai was conducted in a hot climate that can be considered as extreme weather. However, there were several limitations decreasing the strength of findings of this study. On the other end of the weather spectrum, Törnquist et al considered data from subarctic climate, which found no significant associations with weather and RRD.
Another important consideration is the scope of studies. In this review, there are four studies that consider nationwide data and one study that considers Western Australia as a state. The limitation of such study lies in the significance of the climatic range seen in these countries. Ghezala et al did include a regional breakdown of the incidence of RRD to account for this; however, as an overall design including nationwide data is a potential bias due to unpredicted changes in climate in different regions of the country or even within the regions.
Future Directions
This comprehensive review involved 18 studies ranging from 1975 to 2018. Additional studies are needed to further examine the relationship between season and RRD incidence. An important factor to consider for future research is the climate in their specific geographic area. In this review, there is only one study, Al Samarrai, that collected data from a location with extreme heat and relatively mild winter. More studies could be done in extreme weather conditions to find a stronger association of incidence of RRD with ambient temperature or season. Additionally, more studies should be done in areas with large temperature fluctuations between seasons in order to explore the impact of weather variations on incidence of RRD.
In addition to season, future studies can also investigate the relationship between RRD incidence and other specific variables such as light flux, temperature, atmospheric pressure, humidity, precipitation, and other weather conditions. It is possible that these variables have varying effects on the incidence of RRD. These are potential confounding variables when analyzing the impact of climate and RRD, thus it is essential to investigate these factors separately to determine the most accurate assessment of risk factors for RRD.
Finally, future studies should include multi-institutional studies within a specific geographic area in order to limit confounding variables. The studies that were included varied greatly in climate, so it is difficult to pinpoint exactly what weather conditions influence the incidence of RRD. As multi-institutional studies are costly and difficult to conduct, one possible direction employed by studies in our review is incidence estimation to account for possible patient loss to other care points in the geographic area. In our review, the studies that did utilize such methods successfully limited confounding factors associated with such study design. Therefore, more studies could utilize this approach and provide a better estimation of the actual incidence of RRD.
Conclusion
This comprehensive review examines the relationship between seasonality and the incidence of RRD. A total of 18 primary studies were reviewed from a wide variety of geographic regions. While several included studies found a significant correlation between summer and RRD incidence, the results varied and overall there was no significant relationship between seasonality and RRD incidence. This could possibly be due to the lack of studies done in areas with extreme seasonal temperature fluctuations, one of the proposed hypotheses for seasonal RRD. Additionally, individual meteorological parameters such as UV index may play a role in RRD incidence independent from season, so it is critical to control for this as well as other confounding factors when examining the relationship between seasonality and RRD incidence. Since RRD is a critical ophthalmic emergency with detrimental effects if left untreated, it is crucial to continue to investigate and collect data on meteorological risk factors in order to protect patients living in potentially at risk climates.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wilkes SR, Beard CM, Kurland LT, Robertson DM, O’Fallon WM. The incidence of retinal detachment in Rochester, Minnesota, 1970–1978. Am J Ophthalmol. 1982;94(5):670–673. doi:10.1016/0002-9394(82)90013-7
2. Rowe JA, Erie JC, Baratz KH, et al. Retinal detachment in Olmsted County, Minnesota, 1976 through 1995. Ophthalmology. 1999;106(1):154–159. doi:10.1016/S0161-6420(99)90018-0
3. Haimann MH, Burton TC, Brown CK. Epidemiology of retinal detachment. Arch Ophthalmol. 1982;100(2):289–292. doi:10.1001/archopht.1982.01030030291012
4. Blair K, Czyz CN. Retinal detachment. Statpearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 [updated December 2022, 26]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK551502/.
5. Feltgen N, Walter P. Rhegmatogenous retinal detachment—an ophthalmologic emergency. Deutsches Arzteblatt Int. 2014;111(1–2):12–22. doi:10.3238/arztebl.2014.0012
6. Javitt JC, Street DA, Tielsch JM, et al. National outcomes of cataract extraction. retinal detachment and endophthalmitis after outpatient cataract surgery. cataract patient outcomes research team. Ophthalmology. 1994;101:100e5.
7. Norregaard JC, Thoning H, Andersen TF, et al. Risk of retinal detachment following cataract extraction: results from the International Cataract Surgery Outcomes Study. Br J Ophthalmol. 1996;80:689e93. doi:10.1136/bjo.80.8.689
8. Polkinghorne PJ, Craig JP. Northern New Zealand rhegmatogenous retinal detachment study: epidemiology and risk factors. Clin Exp Ophthalmol. 2004;32:159e63. doi:10.3238/arztebl.2014.0012
9. Li X; Beijing Rhegmatogenous Retinal Detachment Study Group. Incidence and epidemiological characteristics of rhegmatogenous retinal detachment in Beijing, China. Ophthalmology. 2003;110(12):2413–2417. doi:10.1016/s0161-6420(03)00867-4
10. Zou H, Zhang X, Xu X, et al. Epidemiology survey of rhegmatogenous retinal detachment in Beixinjing District, Shanghai, China. Retina. 2002;22:294e9. doi:10.1097/00006982-200206000-00007
11. Cambiaggi A. Myopia and retinal. Detachment: statistical study of their relationships. Am J Ophthalmol. 1964;58:642e50. doi:10.1016/0002-9394(64)91383-2
12. Byer NE. Changes in and prognosis of lattice degeneration of the retina. Trans Am Acad Ophthalmol Otolaryngol. 1974;78:OP114e25.
13. Mitry D, Charteris DG, Fleck BW, Campbell H, Singh J. The epidemiology of rhegmatogenous retinal detachment: geographical variation and clinical associations. Br J Ophthalmol. 2010;94(6):678–684. doi:10.1136/bjo.2009.157727
14. Thelen U, Gerding H, Clemens S. Rhegmatogene Netzhautablösungen. Saisonale Variation der Häufigkeit [Rhegmatogenous retinal detachments. Seasonal variation and incidence]. Der Ophthalmologe: Zeitschrift der Deutschen Ophthalmologischen Gesellschaft. 1997;94(9):638–641. doi:10.1007/s003470050174
15. Paavola M, Chehova S, Forsius H. Seasonal variations in retinal detachment in Northern Finland and Novosibirsk. Acta Ophthalmol. 1983;61(5):806–812. doi:10.1111/j.1755-3768.1983.tb01461.x
16. Prabhu PB, Raju KV. Seasonal Variation in the Occurrence of Rhegmatogenous Retinal Detachment. Asia Pac J Ophthalmol. 2016;5(2):122–126. doi:10.1097/APO.0000000000000129
17. Ghisolfi A, Vandelli G, Marcoli F. Seasonal variations in rhegmatogenous retinal detachment as related to meteorological factors. Ophthalmologica. 1986;192(2):97–102. doi:10.1159/000309620
18. Kim DY, Hwang H, Kim JH, et al. The Association between the Frequency of Rhegmatogenous Retinal Detachment and Atmospheric Temperature. J Ophthalmol. 2020;2020:2103743. PMID: 32774898; PMCID: PMC7396048. doi:10.1155/2020/2103743
19. Lin HC, Chen CS, Keller JJ, Ho JD, Lin CC, Hu CC. Seasonality of retinal detachment incidence and its associations with climate: an 11-year nationwide population-based study. Chronobiol Int. 2011;28(10):942–948. doi:10.3109/07420528.2011.613324
20. Qassim A, Viki M, Ng SK, Jersmann H, Casson RJ. Climate and season: the effects on ophthalmic diseases. Clin Exp Ophthalmol. 2017;45(4):385–392. doi:10.1111/ceo.12883
21. Laatikainen L, Tolppanen EM, Harju H. Epidemiology of rhegmatogenous retinal detachment in a Finnish population. Acta Ophthalmol. 1985;63(1):59–64. doi:10.1111/j.1755-3768.1985.tb05216.x
22. Törnquist R, Stenkula S, Törnquist P. Retinal detachment. A study of a population-based patient material in Sweden 1971–1981. I. Epidemiology. Acta Ophthalmologica. 1987;65(2):213–222. doi:10.1111/j.1755-3768.1987.tb07003.x
23. Al Samarrai AR. Seasonal variations of retinal detachment among Arabs in Kuwait. Ophthalmic Res. 1990;22(4):220–223. doi:10.1159/000267026
24. Ivanisević M, Erceg M, Eterović D. Rhegmatogenous retinal detachment and seasonal variations. Acta Med Croatica. 2002;56(2):49–51.
25. Mansour AM, Hamam RN, Sibai TA, Farah TI, Mehio-Sibai A, Kanaan M. Seasonal variation of retinal detachment in Lebanon. Ophthalmic Res. 2009;41(3):170–174. doi:10.1159/000210443
26. Auger N, Rhéaume MA, Bilodeau-Bertrand M, Tang T, Kosatsky T. Climate and the eye: case-crossover analysis of retinal detachment after exposure to ambient heat. Environ Res. 2017;157:103–109. doi:10.1016/j.envres.2017.05.017
27. Manners S, Ng JQ, Kemp-Casey A, Chow K, Kang CY, Preen DB. Retinal detachment surgery in Western Australia (2000–2013): a whole-population study. Br J Ophthalmol. 2017;101(12):1679–1682. doi:10.1136/bjophthalmol-2016-310070
28. Sevillano Torrado C, Viso E, Moreira S, Blanco MJ, Gude F. Rhegmatogenous retinal detachment and solar radiation in northwestern Spain. Ophthalmologica. 2020;243(1):51–57. doi:10.1159/000503070
29. Erdöl H, Uzlu D, Kola M. Characteristics and seasonal variations of rhegmatogenous retinal detachment in the eastern black sea region of Turkey: 8-year results. Turk J Ophthalmol. 2020;50(2):94–98. doi:10.4274/tjo.galenos.2019.59140
30. Choo HG, Yu MH, Lee JH, Kim SH. Seasonal variation in the occurrence of rhegmatogenous retinal detachment in Korea: a three-year nationwide study of the Korean population. J Retina. 2021;6(2):84–91. doi:10.21561/jor.2021.6.2.84
31. Iida M, Horiguchi H, Katagiri S, et al. Association of meteorological factors with the frequency of primary rhegmatogenous retinal detachment in Japan. Sci Rep. 2021;11:9559. doi:10.1038/s41598-021-88979-x
32. Ben Ghezala I, Mariet AS, Benzenine E, et al. Incidence of rhegmatogenous retinal detachment in France from 2010 to 2016: seasonal and geographical variations. Br J Ophthalmol. 2022;106(8):1093–1097. doi:10.1136/bjophthalmol-2020-318457
33. Saraf SS, Lacy M, Hunt MS, et al. Demographics and seasonality of retinal detachment, retinal breaks, and posterior vitreous detachment from the intelligent research in sight registry. Ophthalmol Sci. 2022;2(2):100145. doi:10.1016/j.xops.2022.100145
34. Ghazi N, Green W. Pathology and pathogenesis of retinal detachment. Eye. 2002;16:411–421. doi:10.1038/sj.eye.6700197
35. Rahman R, Ikram K, Rosen PH, Cortina-Borja M, Taylor ME. Do climatic variables influence the development of posterior vitreous detachment? Br J Ophthalmol. 2002;86(7):829. PMID: 12084761; PMCID: PMC1771178. doi:10.1136/bjo.86.7.829
36. Mitry D, Tuft S, McLeod D, Charteris DG. Laterality and gender imbalances in retinal detachment. Graefes Arch Clin Exp Ophthalmol. 2011;249(7):1109–1110. doi:10.1007/s00417-010-1529-0
37. Sultan ZN, Agorogiannis EI, Iannetta D, Steel D, Sandinha T. Rhegmatogenous retinal detachment: a review of current practice in diagnosis and management. BMJ Open Ophthalmol. 2020;5(1):e000474. PMID: 33083551; PMCID: PMC7549457. doi:10.1136/bmjophth-2020-000474
38. Flitcroft DI. The complex interactions of retinal, optical and environmental factors in myopia aetiology. Prog Retin Eye Res. 2012;31(6):622–660. doi:10.1016/j.preteyeres.2012.06.004
39. Ludwig CA, Vail D, Al-Moujahed A, et al. Epidemiology of rhegmatogenous retinal detachment in commercially insured myopes in the United States. Sci Rep. 2023;13(1):9430. PMID: 37296124; PMCID: PMC10256775. doi:10.1038/s41598-023-35520-x
40. Hayashi K, Manabe SI, Hirata A, Yoshimura K. Posterior vitreous detachment in highly myopic patients. Invest Ophthalmol Vis Sci. 2020;61(4):33. doi:10.1167/iovs.61.4.33
41. Rodriguez JO, Lavina AM, Agarwal A. Prevention and treatment of common eye injuries in sports. Am Fam Physician. 2003;67(7):1481–1488.
42. Ferrara M, Al-Zubaidy M, Song A, et al. The effect of age on phenotype of primary rhegmatogenous retinal detachment. Eye. 2023;37(6):1114–1122. doi:10.1038/s41433-022-02061-y
43. Morris RE, Kuhn F, Sipos T. Preventing retinal detachment: where are we? Implications from stickler syndrome. Clin Ophthalmol. 2022;16:4315–4321. PMID: 36583093; PMCID: PMC9793794. doi:10.2147/OPTH.S388631
44. Du S, Yang X, Zha Y, Chen X, Zhang J, Kuhn F. Direct laser photocoagulation of the retinal pigment epithelium: a novel method to seal retinal breaks during pars plana vitrectomy for retinal detachment. Discov Med. 2023;35(179):988–994. PMID: 38058064. doi:10.24976/Discov.Med.202335179.95
45. Eijk ES, Busschbach JJ, Timman R, Monteban HC, Vissers JM, van Meurs JC. What made you wait so long? Delays in presentation of retinal detachment: knowledge is related to an attached macula. Acta Ophthalmol. 2016;94(5):434–440. PMID: 27008986. doi:10.1111/aos.13016
46. Arjmand P, Murtaza F, Eshtiaghi A, Popovic MM, Kertes PJ, Eng KT. Impact of the COVID-19 pandemic on characteristics of retinal detachments: the Canadian experience. Can J Ophthalmol. 2021;56(2):88–95. PMID: 33444561; PMCID: PMC7832047. doi:10.1016/j.jcjo.2020.12.008
47. Allbon DS, Avery N, Gray A, Bradshaw H. Retinal detachments in southern New Zealand: do poorer patients have poorer outcomes? N Z Med J. 2015;128(1427):18–24. PMID: 26914000.
48. Hsu HT, Patterson R, Ryan SJ. Traumatic posterior vitreous detachment: scanning electron microscopy of an experimental model in the monkey eye. Scan Electron Microsc. 1984;(Pt 3):1361–1368.
49. Balles MW. Traumatic retinopathy. In: Albert DM, Jakobiec FA, editors. Principles and Practice of Ophthalmology.
50. Lee TH, Chen YH, Kuo HK, et al. Retinal detachment associated with basketball-related eye trauma. Am J Ophthalmol. 2017;180:97–101. doi:10.1016/j.ajo.2017.05.025
51. Baath J, Ells AL, Kherani A, Williams RG. Severe retinal injuries from paintball projectiles. Can J Ophthalmol. 2007;42(4):620–623. doi:10.3129/i07-101
52. Knorr HL, Jonas JB. Retinal detachments by squash ball accidents. Am J Ophthalmol. 1996;122(2):260–261. doi:10.1016/S0002-9394(14)72019-7
53. Qureshi N, Abbas M, Miah MR, Ishaq N, Mumtaz Ch M, Khan WA. Traumatic retinal detachment due to tennis ball injury. Pak J Ophthalmol. 2007;23(3):151–154.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.