")
Back to Journals » Clinical Ophthalmology » Volume 19
Climate and Rhegmatogenous Retinal Detachment: A Retrospective and Multi-Site Study in the High Desert of the United States
Authors Aharonian K, Martin J , Krasner H , Batra K , Yepremyan M
Received 19 January 2025
Accepted for publication 23 May 2025
Published 22 June 2025 Volume 2025:19 Pages 1919—1930
DOI https://doi.org/10.2147/OPTH.S518396
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Scott Fraser
Karl Aharonian,1 Jeffrey Martin,1 Henry Krasner,1 Kavita Batra,1,2 Meher Yepremyan1,3
1Department of Medical Education, Kirk Kerkorian School of Medicine at UNLV, Las Vegas, NV, USA; 2Office of Research, Kirk Kerkorian School of Medicine at UNLV, Las Vegas, NV, USA; 3Retina Consultants of Nevada, Las Vegas, Nevada, USA
Correspondence: Karl Aharonian, Email [email protected]
Purpose: While numerous studies have investigated associations between meteorological factors and the incidence of rhegmatogenous retinal detachment (RRD), findings remain inconclusive. We have identified key limitations in establishing this relationship due to confounding bias in prior research. This retrospective, observational study aims to address these gaps by minimizing residual confounding bias, focusing exclusively on patients aged ≥ 65 to limit seasonal recreational activity as a risk factor, and using incidence ratio calculations to account for patient intake fluctuations. This study explores these dynamics within the distinct climatic conditions of Las Vegas, Nevada, characterized by intense summer heat, cold winters, and low humidity.
Methods: A retrospective chart review was performed across four Retina Consultants of Nevada locations from December 2020 to November 2023. The study included patients aged ≥ 65 diagnosed with a primary RRD. Exclusion criteria were non-residency, recurrent RRD, and comorbid retinal conditions. Monthly RRD incidence ratios were calculated relative to all new patients seen for retinal conditions in the same age group. Environmental data (temperature, atmospheric pressure, humidity, UV index) were obtained from national meteorological databases. Correlations between meteorological factors and RRD incidence were assessed using Pearson correlation coefficients.
Results: Among 308 patients (mean age 72.4 years (SD=5.93), 59.7% male, p=0.0006), no significant correlations were found between RRD incidence and average monthly temperature (r=0.004, p=0.982), barometric pressure (r=− 0.047, p=0.786), humidity (r=0.15, p=0.368), or UV index (r=0.072, p=0.68). Seasonal analysis showed a non-significant trend of higher RRD incidence during colder months (r=− 0.70, p=0.30). Laterality (right eye: 53.2%) was also not statistically significant (p=0.254).
Conclusion: This study’s strength lies in addressing confounding factors by focusing on an older, less active population and using incidence ratios to adjust for patient intake fluctuations. The findings challenge prior reports by showing no significant association between meteorological factors and RRD incidence, suggesting a limited role for environmental variables in older subjects.
Keywords: rhegmatogenous retinal detachment, rrd, retinal detachment, retrospective multi-site study, incidence ratios in retinal detachment, meteorological factors
Introduction
Retinal detachment is an ophthalmologic emergency that can lead to acute vision loss if not treated promptly. Rhegmatogenous retinal detachment (RRD) is the most common form, with an annual incidence of approximately 1 per 10,000 individuals and an overall increasing temporal trend.1–3 Retinal detachment occurs when the neurosensory retina (NSR) separates from the retinal pigment epithelium (RPE).3–6 This separation results from a disruption in the passive and active forces that normally hold these two layers together, leading to the pathologic accumulation of vitreous fluid in the subretinal space.4,5 RRD specifically develops when liquefaction of the vitreous body and a physical retinal defect, such as tear or round hole allow liquified vitreous fluid to pass through the break into the subretinal space.3–6 As vitreous fluid enters, it causes the NSR to detach from the RPE, leading to vision loss.4–6 It is critical to treat RRD in a timely manner due to its potential to cause irreversible vision loss in the affected eye. Given the severe consequences of RRD, identifying potential risk factors is critical in preventing this sight-threatening emergency.
Previous literature has identified several well-known risk factors for RRD, including trauma, lattice degeneration, myopia, old age, previous cataract surgery, and genetic predisposition.6–9 Many of these etiologic factors predispose individuals to RRD due to retinal degeneration and weakening, which facilitate retinal tears.6–9 In addition to these established risk factors, various meteorological parameters, including ambient temperature, have emerged as intriguing potential contributors. Several studies worldwide have reported higher RRD incidence rates during the summer months.10–15 Furthermore, previous research has noted significant regional discrepancies in RRD incidence, with Europe exhibiting the highest rates and the Americas having the lowest, suggesting a possible meteorological influence.2 While the cause of these regional discrepancies is likely multifactorial, geographic and climatic factors such as average UV index, temperature, and sunshine hours may play a role.
These findings prompted our team to publish a comprehensive literature review examining the relationship between climate and retinal detachment.16 Our review included 10 studies that found correlation between weather patterns and RRD, with seven studies specifically associating summer with increased RRD incidence.10–12,14,17–22 Conversely, eight studies did not find a significant association.23–30 Since the publication of our review, an additional study by Barioulet et al has investigated these relationships. The study found no statistically significant association between the incidence of idiopathic RRD incidence across metropolitan France and various meteorological parameters. Specifically, the study examined factors such as mean temperature over the preceding 10 days, rainfall, atmospheric pressure, radiation, sunshine duration, relative humidity, and wind speed.
Several mechanisms have been proposed to explain the seasonal variation in RRD observed in these published studies. First, it is suggested that warmer temperatures may lead to dehydration, which could cause the vitreous to contract.14 Vitreous contraction, in turn, can create traction forces that pull on the retinal surface, potentially leading to RRD.14,15 Other possible confounding factors that may contribute to the seasonal variation include increased physical activity and potential trauma during the summer months, as well as increased eye rubbing due to allergens.14 However, the inconsistency in prior findings suggests that additional environmental or methodological variables may be at play. For instance, differences in how RRD onset is defined, variability in geographic data granularity, or the possible role of barometric pressure changes and cumulative sun exposure could contribute to mixed results across studies.
Despite the published studies on the relationship between climate and retinal detachment, there are no studies specifically focused on locations with unique temperature extremes, such as in Las Vegas. Las Vegas is characterized by extreme weather and dry climate, with daily temperatures reaching up to 120°F in the summer, relatively cold winters, with temperatures dropping to the 40s°F. The only similar climate that has been explored in the literature is that of Kuwait, as studied by Al Samarrai et al. However, Kuwait’s climate is much more humid, which could serve as a confounding factor. Therefore, Las Vegas serves as an advantageous setting for studying the influence of environmental variables on retinal detachment, as the combination of extreme heat, low humidity, and seasonal variability allows for isolation of climatic factors without the confounding influence of moisture or tropical weather patterns.
Our retrospective review builds on the suggestions from the review published by our team, which summarized potential confounding factors from earlier studies. Specifically, to minimize confounding bias, we focused the study on patients aged 65 and older, a group with lower levels of physical and recreational activity. According to the Centers for Disease Control and Prevention (CDC) data, fewer than 43% of adults over 65 engage in leisure-time aerobic activity at recommended levels, and this proportion is likely even lower in regions like Las Vegas, where summer temperatures can exceed 120°F.31 We also calculated the monthly incidence ratio to account for potential month-to-month fluctuations in patient intake numbers, thus reducing confounding bias. Finally, only RRD-specific codes were utilized, which helped limit the possibility of including traumatic or tractional retinal detachments in the analysis.
Using data from the largest retina practice in Las Vegas alongside local weather data, we examined several potential meteorological risk factors for RRD, including average monthly temperature, UV index, humidity, and atmospheric pressure.
The primary aim of this study is to provide evidence to strengthen the understanding of the relationship between RRD and climate. Additionally, we seek to contribute to the development of preventative health resources aimed at improving outcomes for vulnerable patient populations. By identifying and establishing risk factors for RRD, we hope to reduce its incidence and improve clinical outcomes for retinal detachment, particularly in geographic locations with harsh climates.
Methods
Study Design and Setting
This retrospective, multi-site study was conducted between December 1, 2020, and November 30, 2023, across four offices of Retina Consultants of Nevada, located in Las Vegas Metropolitan Area.
IRB Approval, Financial Disclosures and Ethical Considerations
Institutional Review Board (IRB) Approval
This study was conducted in compliance with the guidelines and regulations set forth by the Institutional Review Board (IRB) and was approved under protocol number 20235190. On November 14, 2023, WCG IRB granted approval via an expedited review, including a waiver of authorization for the use and disclosure of protected health information (PHI) for this research. The study adhered to all applicable ethical standards to protect patient privacy and confidentiality, with all data de-identified prior to analysis to ensure anonymity.
Ethical Considerations
This study utilized a retrospective chart review methodology, collecting data that had already been documented in patient records. All data were anonymized to protect patient identities, and only aggregated, de-identified information was used in the analysis and reporting. No informed consent was required due to the retrospective nature of the study and the lack of direct patient interaction, as permitted by the IRB approval.
Financial Disclosures
The authors declare no financial disclosures or conflicts of interest related to this study. This research was conducted independently, without any financial support or funding from external organizations.
Inclusion and Exclusion Criteria
A total of 492 patients were initially admitted during the data collection period. Patients were excluded if they were not residents of Las Vegas Metropolitan Area, younger than 65 years of age, had recurrent retinal detachment or RRD in the fellow eye, or had other significant retinal conditions and intravitreal injections for retinal pathologies such as diabetic retinopathy and macular degeneration. Ultimately, 184 patients did not meet inclusion criteria and were excluded from final data analysis. A total of 308 patients met our inclusion criteria of a confirmed diagnosis of first-episode RRD (Figure 1).
 |
Figure 1 Selection Criteria Flowchart. |
Chart Review Process and Data Mining
The patient charts were reviewed following identification using the relevant ICD-10 codes. These codes included H33.011 (retinal detachment with a single break, right eye), H33.012 (retinal detachment with a single break, left eye), H33.021 (retinal detachment with multiple breaks, right eye), H33.022 (retinal detachment with multiple breaks, left eye), H33.051 (total retinal detachment, right eye), and H33.052 (total retinal detachment, left eye). For each patient, the chart was manually reviewed to extract relevant clinical data, including sex-identify as marked in the chart, date of visit, age, and the associated diagnosis codes. This information was recorded on an encrypted Excel sheet for further analysis. The patient data were retrieved from the electronic health record (EHR) system, NextGen.
For the purposes of calculating the incidence ratio of RRD, the total number of new patients seen in the same age group (65 and above) for any retinal issue during the same month was also collected.
Meteorological Data
Environmental data, including daily average temperatures (°F) and barometric pressure (mmHg), were obtained from the National Weather Service and the National Centers for Environmental Information respectively.32,33 The daily averages were used to calculate monthly and seasonal averages for further analysis.
Outcome Measures
The primary outcome of interest was the incidence ratio of first-episode RRD cases by month, calculated as the number of new RRD cases per month divided by the total number of new patients seen at the same clinical sites in the same age group for any reason during the same period. Secondary outcomes included seasonal and monthly variations in the incidence of RRD, and the potential influence of environmental factors such as temperature and barometric pressure on these variations.
Statistical Analysis
Descriptive statistics, including means and proportions, were used to summarize demographic data such as age, sex-identity as marked in the chart, and laterality of the affected eye.
For the environmental variables, Pearson correlation coefficients were calculated to evaluate the relationship between monthly RRD incidence and average temperature, atmospheric pressure, humidity, and UV index. These correlations were computed using the monthly and seasonal data, and p-values were reported to assess statistical significance (with significance set at p<0.05).
Specifically, the measurements are described below:
- Temperature: Monthly, quarterly, and seasonal average temperatures in Fahrenheit were compared to RRD incidence rates.
- Pressure: Average monthly sea level pressure in mmHg was analyzed to determine whether fluctuations in pressure correlated with RRD incidence.
- Humidity: Average monthly humidity was assessed to evaluate its relationship with RRD incidence.
- UV Index: The UV index for each month was compared with RRD incidence to examine any potential impact of UV radiation on RRD rates.
For demographic analysis, proportions were calculated for sex-identify as marked in the chart (male vs female) and laterality (right eye vs left eye) among the RRD patients.
All statistical analyses were performed using Excel software, and results were visualized using scatter plots to highlight trends and relationships. Pearson correlation coefficients and their corresponding p-values were used to determine the strength and significance of associations between environmental factors and RRD incidence.
Results
Demographic Description
The mean age of the patients diagnosed with RRD was 72.4 years (SD=5.93).
Among the patients diagnosed with Rhegmatogenous Retinal Detachment (RRD), 184 were self-identified male and 124 were self-identified female, indicating that males made up approximately 60% of the RRD cases.
A detailed analysis of the monthly percentage of the new patients of age 65 and above in the same time period showed that male patients made up the percentage fluctuating between a low of 41.83% in March 2023 and a high of 51.17% in June 2022. On an average, the proportion of male patients remained relatively consistent, with males representing nearly half of the population seen each month. Although relatively small sample size, it appears that RRD cases are more common in male population which is consistent with findings of previous studies.
Regarding the laterality of the affected eye, 164 cases involved the right eye (53.2%), and 144 cases involved the left eye (46.8%) This statistically insignificant predominance of the right eye. Table 1 displays the data in a table format.
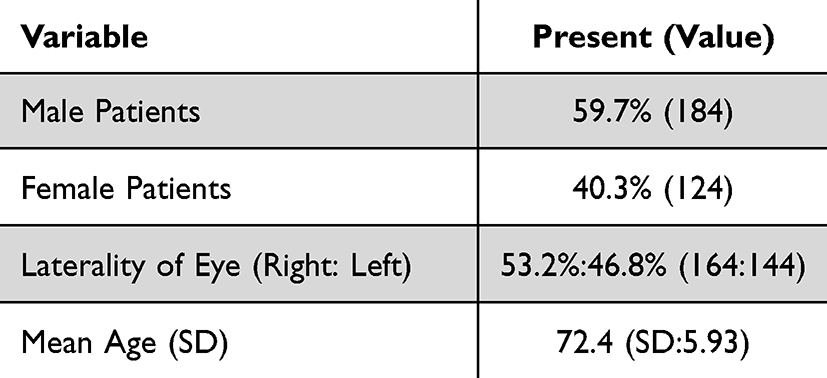 |
Table 1 Characteristics of the Sample (N=308) |
Monthly Temperature and RRD Incidence
The relationship between average monthly temperature and the incidence of Rhegmatogenous Retinal Detachment (RRD) was analyzed using data spanning from December 2020 to November 2023. A Pearson correlation coefficient of r=0.004 (p = 0.982) was observed, indicating no meaningful correlation between temperature and the incidence of RRD. Monthly temperature and incidence are provided in Table 2. Figures 2 and 3 illustrate monthly incidence ratio with meteorological factors and scatter plots with best trend lines.
 |
Table 2 Monthly Incidence Ratio, Average Temperature (Fahrenheit), Average Pressure (hPa), UV Index, and Average Humidity |
 |
Figure 2 Monthly Incidence Ratio and Meteorological Factors (Averaged Data) Aggregated data over a three-year period was utilized by calculating the monthly averages for each variable. Note: The atmospheric pressure values are shown in amplified relative units (scaled deviations from the minimum pressure, multiplied by 10) to better visualize subtle variations over time. |
 |
Figure 3 Correlation of Incidence Ratio with Meteorological Factors. |
Note: The atmospheric pressure values are shown in amplified relative units (scaled deviations from the minimum pressure, multiplied by 10) to better visualize subtle variations over time.
Quarterly/Seasonal Temperature and RRD Incidence
The relationship between both quarterly and seasonal average temperatures and the incidence of Rhegmatogenous Retinal Detachment (RRD) were examined.
The quarterly analysis showed a Pearson correlation coefficient of r=0.030 (p = 0.93), indicating no meaningful relationship between quarterly temperature changes and RRD incidence.
Furthermore, the seasonal analysis revealed a Pearson correlation coefficient of r=−0.70 (p = 0.30), suggesting no statistically significant relationship between seasonal temperature and incidence of RRD. Quarterly and seasonal data is summarized in Table 3.
 |
Table 3 Seasonal and Quarterly Average Temperature and Incidence Ratio |
Pressure and RRD Incidence
We examined the effect of average sea level pressure measured in Hectopascals (hPa) on RRD incidence over the same period. The Pearson correlation coefficient was r=−0.047 (p = 0.786), reflecting a weak negative correlation that was not statistically significant. This finding suggests that variations in atmospheric pressure have no clear impact on the occurrence of RRD. Monthly pressure and incidence are provided in Table 2.
Humidity and RRD Incidence
The average monthly humidity (%) and its potential relationship with RRD incidence were analyzed. The correlation analysis yielded a Pearson correlation coefficient of r=0.15 (p = 0.368), indicating a weak positive correlation. However, this relationship was not statistically significant, suggesting that changes in humidity levels do not meaningfully affect the incidence of RRD. Monthly humidity and incidence are provided in Table 2.
UV Index and RRD Incidence
Lastly, we explored the association between the monthly UV index and the incidence of RRD. The Pearson correlation coefficient was r=0.072 (p = 0.68), indicating almost negligible positive correlation. This relationship was also not statistically significant, suggesting that exposure to varying levels of UV radiation does not play a significant role in the monthly incidence of RRD in this population. Monthly UV index and incidence are provided in Table 2. Summary of correlation and statistical significance values are presented in Table 4.
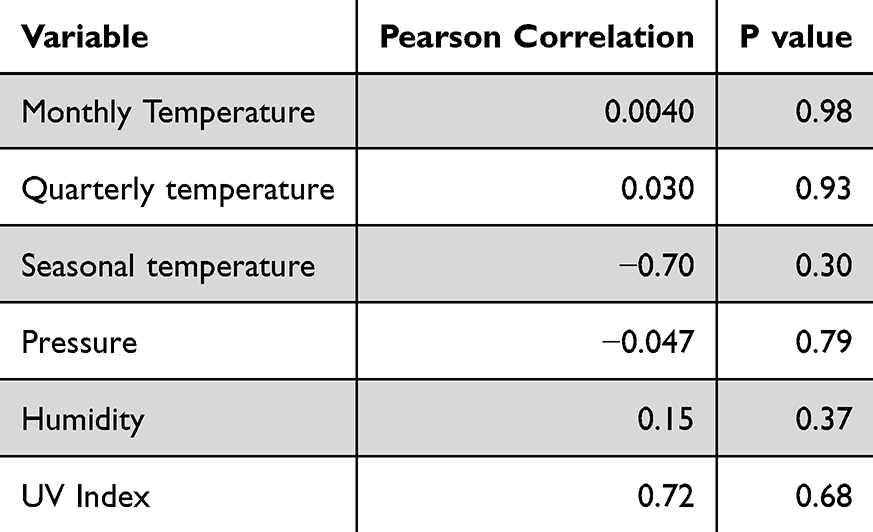 |
Table 4 Summary of Pearson Correlation and P values for Each Meteorological Variable |
Discussion
Seasonality (Temperature and RRD Association)
We conducted the retrospective chart review with the primary objective of exploring association between average monthly temperature in Fahrenheit and incidence of RRD cases. There was no statistically significant correlation between monthly, quarterly, or seasonal temperature averages and the incidence RRD. While previous studies have reported seasonal variations in RRD rates, with higher incidences during warmer months, our data from Las Vegas—a region characterized by extreme heat—did not support these findings. This discrepancy suggests that temperature may not have as strong a role in RRD development as previously hypothesized, especially in populations with unique environmental exposures. The lack of association aligns with majority of studies summarized in the most recent review and other most recent studies on this topic such as the one by Barioulet et al and a regional study in Korea by Kim et al, further reinforcing that meteorological factors like temperature may not be primary contributors to RRD incidence.16,34,35 Additionally, given that most individuals over the age of 65 have already undergone posterior vitreous detachment (PVD), a key precursor event in RRD pathogenesis, the role of external environmental triggers in this age group may be inherently reduced.36
Associations with Other Meteorological Data
We also explored barometric pressure, humidity, and UV index to determine if these factors might influence RRD occurrence. However, similar to temperature, none of these variables demonstrated a significant correlation with RRD incidence. Although there are studies that have shown statistically significant association of one or more of these variables in populations, our findings support literature that suggests these variables are unlikely to have substantial impacts on RRD development. The most notable one of the mentioned is UV index, which reaches extreme levels in summer months in this area. It is also notable that the studies that found correlations between light flux and RD were not done in a climate with such a range of UV index (2–12) as present in this region. Furthermore, elderly individuals are more likely to have limited UV exposure due to institutional living or reduced outdoor activity, potentially minimizing seasonal UV fluctuation effects.37
While some prior studies have examined sunshine hours as a risk factor for RRD, we did not utilize this metric for our analysis given the inclusion of the UV index—which offers a more direct measure of solar radiation exposure (Table 2). Nevertheless, it is notable that sunshine hours in Las Vegas are markedly high year-round, ranging on average from 235 hours in December to 402 hours in June, with consistently high sunlight throughout all seasons. This consistency likely saturates any possible effect of solar exposure and may explain the absence of significant seasonal variation in our results. Furthermore, the elderly population studied is less likely to have variable outdoor exposure patterns due to age-related limitations in mobility and activity, further minimizing the relevance of sunshine hours as an influencing factor.38
Other Findings: Right Vs Left Eye and Sex-Identify Distribution
In the studied sample, self-identified males made up approximately 60% of the RRD cases therefore they were statistically more likely to get RRD in our sample. This finding is consistent with several large sample previous studies.39 The male predisposition could be attributed to factors such as higher rates of myopia, more frequent exposure to physical trauma, or hormonal influences, though further research is needed to confirm these associations.
In terms of laterality, previous studies have reported higher incidence of RRD in the right eye.40 In this study, there was statistically insignificant predominance of the right eye. The reason for statistical insignificance could be sample size. The studies that established the association of right eye and RD did have much higher sample size that potentially affects our data’s significance when it comes to laterality.
However, it could also be that in our geographic area laterality is not a significant risk factor for RRD.
Strengths/Limitations
Our study is the first of its kind to apply rigorous exclusion criteria and calculate incidence ratios for a well-defined population, using multi-year data collected from a single geographic region characterized by hot, dry summers and cold winters. By focusing on patients aged 65 and older, we reduce the impact of seasonal recreational activities as a potential confounding factor in the development of retinal conditions. This unique approach allows for a more accurate assessment of the potential relationship between meteorological factors and retinal detachment in a population that may be more vulnerable to these influences.
While our study offers valuable insights into the connection between climate and retinal detachment, it is not without limitations. First, the cross-sectional nature of this retrospective study limits our ability to draw causal conclusions regarding the impact of meteorological factors on the incidence of RRD. This limitation is inherent in observational studies, where causality cannot be definitively established. Additionally, although our sample size is significant, it may still lack the statistical power necessary to detect smaller, but potentially meaningful, effects—particularly when analyzing complex meteorological data that could involve subtle interactions. Specifically, the observed negative correlation between temperature and RRD incidence (r = –0.70, p = 0.30) suggests a large effect size despite the lack of statistical significance. This raises the possibility that our study may have been underpowered to detect smaller but potentially meaningful associations.
Furthermore, several important variables were not directly measured in this study. For example, individual patient activity levels and a history of myopia—both of which could potentially influence the development of retinal conditions—were not included as part of our analysis. Instead, patients were excluded based on medical coding, which may not fully capture these factors. Physical activity, a potential mediator for trauma or exertion-induced vitreoretinal traction, also declines substantially in elderly populations—by 40% to 80%—further reducing potential exposure to certain activity-related environmental risk factors.41 Moreover, the prevalence of allergic eye conditions—which can lead to eye rubbing and thus vitreoretinal stress—decreases significantly with age, further supporting the idea that older individuals may have diminished sensitivity to environmental RRD triggers.42 Future research would benefit from addressing these gaps by directly measuring relevant variables such as physical activity, myopia, and other ocular risk factors. Additionally, a prospective study design could provide stronger evidence by following patients over time and examining the effects of meteorological variables in real-time.
Future Directions
Looking ahead, our study adds to the growing evidence that temperature may not have a clear association with incidence of RD. A similar study could be conducted in a high-risk patient population, particularly among individuals with myopia, who are known to have a greater predisposition to RRD. Expanding this research to include younger age groups and patients with more specific risk factors could help elucidate the role that meteorological factors play in RRD pathogenesis in combination with other risks such as previous trauma. Prospective studies incorporating additional environmental variables, such as daily activity levels may also yield clearer results.
Conclusion
In conclusion, this study offers novel insights into RRD incidence within the context of unique climate of hot, dry summer climate with cold winters, while addressing and mitigating several common limitations faced by previous studies. No statistically significant associations were found between temperature, humidity, barometric pressure, or UV index and RRD incidence. While environmental factors may influence RRD risk, our results suggest a limited role for environmental variables in older subjects. Future research should focus on higher-risk groups and incorporate additional environmental and patient-level variables to further explore the complex etiology of RRD.
Acknowledgments
Kavita Batra and Meher Yepremyan are co-senior authors for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mitry D, Charteris DG, Yorston D, et al. The epidemiology and socioeconomic associations of retinal detachment in Scotland: a two-year prospective population-based study. Invest Ophthalmol Vis Sci. 2010;51(10):4963–4968. doi:10.1167/iovs.10-5400
2. Ge JY, Teo ZL, Chee ML, et al. International incidence and temporal trends for rhegmatogenous retinal detachment: a systematic review and meta-analysis. Surv Ophthalmol. 2024;69(3):330–336. doi:10.1016/j.survophthal.2023.11.005.
3. Steel D. Retinal detachment. BMJ Clin Evid. 2014;2014:0710.
4. Sultan ZN, Agorogiannis EI, Iannetta D, Steel D, Sandinha T. Rhegmatogenous retinal detachment: a review of current practice in diagnosis and management. BMJ Open Ophthalmol. 2020;5(1):e000474. doi:10.1136/bmjophth-2020-000474 Erratum in: BMJ Open Ophthalmol. 2021 Mar 14;6(1):e000474corr1. doi: 10.1136/bmjophth-2020-000474corr1. PMID: 33083551; PMCID: PMC7549457.
5. Ghazi NG, Green WR. Pathology and pathogenesis of retinal detachment. Eye (Lond). 2002;16(4):411–421. doi:10.1038/sj.eye.6700197.
6. Blair K, Czyz CN. Retinal detachment. In: StatPearls [Internet]. Treasure Island(FL): StatPearls Publishing; 2024. Available from: https://www.ncbi.nlm.nih.gov/books/NBK551502/.
7. Kriebel D, Sama SR, Bradbury M, et al. Risk factors for retinal detachment: a case-control study. J Occup Environ Med. 2020;62(6):445–451. doi:10.1097/JOM.0000000000001867.
8. Williams K, Hammond C.High myopia and its risks. Community Eye Health. 2019;32(105):5–6.
9. Bergstrom R, Czyz CN. Vitreous floaters. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470420/.
10. Paavola M, Chehova S, Forsius H. seasonal variations in retinal detachment in northern Finland and Novosibirsk. Acta Ophthalmol. 2009;61(5):806–812. doi:10.1111/j.1755-3768.1983.tb01461.x
11. Mansour AM, Hamam RN, Sibai TA, et al. Seasonal variation of retinal detachment in Lebanon. Ophthalmic Res. 2009;41(3):170–174. doi:10.1159/000210443
12. Prabhu PB, Raju KV. Seasonal variation in the occurrence of rhegmatogenous retinal detachment. Asia Pac. J. Ophthalmol. (Phila). 2016;5(2):122–126. doi:10.1097/APO.0000000000000129
13. Thelen U, Gerding H, Clemens S. Rhegmatogenous retinal detachments seasonal variation and incidence. Ophthalmologe. 1997;94(9):638–641. doi:10.1007/s003470050174
14. Lin HC, Chen C-S, Keller JJ, et al. Seasonality of retinal detachment incidence and its associations with climate: an 11-year nationwide population-based study. Chronobiol. Int. 2011;28(10):942–948. doi:10.3109/07420528.2011.613324
15. Kim DY, Hwang H, Kim JH, et al. The association between the frequency of rhegmatogenous retinal detachment and atmospheric temperature. J. Ophthalmol. 2020;2103743(2020).
16. Aharonian K, Krasner H, Martin J, Batra K, Yepremyan M. Climate and rhegmatogenous retinal detachment: a comprehensive review and future research guidelines. Clin Ophthalmol. 2024;18:3083–3095. doi:10.2147/OPTH.S476142
17. Ghisolfi A, Vandelli G, Marcoli F. Seasonal variations in rhegmatogenous retinal detachment as related to meteorological factors. Ophthalmologica. 1986;192(2):97–102. doi:10.1159/000309620
18. Laatikainen L, Tolppanen EM, Harju H. Epidemiology of rhegmatogenous retinal detachment in a Finnish population. Acta Ophthalmol. 1985;63(1):59–64. doi:10.1111/j.1755-3768.1985.tb05216.x
19. Al Samarrai AR. Seasonal variations of retinal detachment among Arabs in Kuwait. Ophthalmic Res. 1990;22(4):220–223. doi:10.1159/000267026
20. Sevillano Torrado C, Viso E, Moreira S, Blanco MJ, Gude F. Rhegmatogenous retinal detachment and solar radiation in northwestern Spain. Ophthalmologica. 2020;243(1):51–57. doi:10.1159/000503070
21. Choo HG, Yu MH, Lee JH, Kim SH. Seasonal variation in the occurrence of rhegmatogenous retinal detachment in Korea: a three-year nationwide study of the Korean population. J Retina. 2021;6(2):84–91. doi:10.21561/jor.2021.6.2.84
22. Ben Ghezala I, Mariet AS, Benzenine E, et al. Incidence of rhegmatogenous retinal detachment in France from 2010 to 2016: seasonal and geographical variations. Br J Ophthalmol. 2022;106(8):1093–1097. doi:10.1136/bjophthalmol-2020-318457
23. Erdöl H, Uzlu D, Kola M. Characteristics and seasonal variations of rhegmatogenous retinal detachment in the eastern Black Sea region of Turkey: 8-year results. Turk J Ophthalmol. 2020;50(2):94–98. doi:10.4274/tjo.galenos.2019.59140
24. Auger N, Rhéaume MA, Bilodeau-Bertrand M, Tang T, Kosatsky T. Climate and the eye: case-crossover analysis of retinal detachment after exposure to ambient heat. Environ Res. 2017;157:103–109. doi:10.1016/j.envres.2017.05.017
25. Manners S, Ng JQ, Kemp-Casey A, Chow K, Kang CY, Preen DB. Retinal detachment surgery in Western Australia (2000–2013): a whole-population study. Br J Ophthalmol. 2017;101(12):1679–1682. doi:10.1136/bjophthalmol-2016-310070
26. Iida M, Horiguchi H, Katagiri S, et al. Association of meteorological factors with the frequency of primary rhegmatogenous retinal detachment in Japan. Sci Rep. 2021;11(1):9559. doi:10.1038/s41598-021-88979-x
27. Saraf SS, Lacy M, Hunt MS, et al. Demographics and seasonality of retinal detachment, retinal breaks, and posterior vitreous detachment from the intelligent research in sight registry. Ophthalmol Sci. 2022;2(2):100145. doi:10.1016/j.xops.2022.100145
28. Ivanisević M, Erceg M, Eterović D. Rhegmatogenous retinal detachment and seasonal variations. Acta Med Croatica. 2002;56(2):49–51.
29. Törnquist R, Stenkula S, Törnquist P. Retinal detachment. A study of a population-based patient material in Sweden 1971–1981. I. Epidemiology. Acta Ophthalmologica. 1987;65(2):213–222. doi:10.1111/j.1755-3768.1987.tb07003.x
30. Li X, Beijing Rhegmatogenous Retinal Detachment Study Group. Incidence and epidemiological characteristics of rhegmatogenous retinal detachment in Beijing, China. Ophthalmology. 2003;110(12):2413–2417. doi:10.1016/s0161-6420(03)00867-4
31. QuickStats: percentage* of adults† aged ≥65 years meeting 2008 federal guidelines for leisure-time aerobic§ and muscle-strengthening activities, by age and type of activity — United States, 2000–2002 and 2013–2015. MMWR Morb Mortal Wkly Rep. 2016;65(37):1019. doi:10.15585/mmwr.mm6537a9
32. National Weather Service. Available from: https://www.weather.gov/.
33. National Centers for Environmental Information. Available from: https://www.ncei.noaa.gov/.
34. Barioulet L, Rueter M, Sentis V, et al. Meteorological factors and rhegmatogenous retinal detachment in metropolitan France. Sci Rep. 2024;14(1):18857. doi:10.1038/s41598-024-69591-1
35. Kim DY, Hwang H, Kim JH, et al. The Association between the Frequency of Rhegmatogenous Retinal Detachment and Atmospheric Temperature. J Ophthalmol. 2020;2020:2103743. doi:10.1155/2020/2103743
36. Uchino E, Uemura A, Ohba N, et al. Initial stages of posterior vitreous detachment in healthy eyes of older persons evaluated by optical coherence tomography. Arch Ophthalmol. 2001;119(10):1475–1479. doi:10.1001/archopht.119.10.1475
37. Durvasula S, Kok C, Sambrook PN, et al. Sunlight and health: attitudes of older people living in intermediate care facilities in southern Australia. Arch Gerontol Geriatr. 2010;51(3):e94–9. doi:10.1016/j.archger.2010.01.008
38. https://www.usclimatedata.com/climate/las-vegas/nevada/united-states/usnv0049.
39. Mitry D, Charteris DG, Fleck BW, Campbell H, Singh J. Fleck BW, et alThe epidemiology of rhegmatogenous retinal detachment: geographical variation and clinical associations. British Journal of Ophthalmology. 2010;94(6):678–684. doi:10.1136/bjo.2009.157727
40. Ferrara M, Song A, Al-Zubaidy M, et al. The effect of sex and laterality on the phenotype of primary rhegmatogenous retinal detachment. Eye (Lond). 2023;37(14):2926–2933. doi:10.1038/s41433-023-02443-w
41. Suryadinata RV, Wirjatmadi B, Adriani M, Lorensia A. Effect of age and weight on physical activity. J Public Health Res. 2020;9(2):1840. doi:10.4081/jphr.2020.1840
42. Janson C. Does allergy decrease with age?L’allergie diminue-t-elle avec l’âge? Revue Française d’Allergologie. 2024;64. doi:10.1016/j.reval.2024.103789
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.