")
Back to Journals » Infection and Drug Resistance » Volume 18
Clinical Characteristics and Mortality Risk Factors in Patients with Tuberculosis and Coincident Pneumocystis jirovecii Pneumonia: A Retrospective Single-Center Study
Authors Pan X, Zheng J, Xu J, Pan L, Wang C, Huang X , Qiu J, Yan C, Mao M
Received 24 March 2025
Accepted for publication 18 June 2025
Published 17 July 2025 Volume 2025:18 Pages 3535—3542
DOI https://doi.org/10.2147/IDR.S530186
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor M. Mora-Montes
Xiaohong Pan,1 Jun Zheng,2 Jiekun Xu,1 Lei Pan,1 Caihong Wang,1 Xiaoqing Huang,1 Junke Qiu,1 Chenxi Yan,1 Minjie Mao1
1Department of Intensive Care Unit for Tuberculosis, Zhejiang Tuberculosis Diagnosis and Treatment Center, Zhejiang Hospital of Integrated Traditional Chinese and Western Medicine, Hangzhou, Zhejiang, 310013, People’s Republic of China; 2Department of Rehabilitation, Health Service Center of Nanxing Subdistrict, Hangzhou, Zhejiang, 310000, People’s Republic of China
Correspondence: Minjie Mao, Department of Intensive Care Unit for Tuberculosis, Zhejiang Tuberculosis Diagnosis and Treatment Center, Zhejiang Hospital of Integrated Traditional Chinese and Western Medicine, No. 208 huancheng Road, Hangzhou, Zhejiang, 310013, People’s Republic of China, Tel +8615825500408, Email [email protected]
Introduction: HIV infection and immunosuppressive therapy are major risk factors for tuberculosis (TB) or Pneumocystis jirovecii pneumonia (PJP). The joint presence of these diseases is not rare, posing substantial challenges in diagnosis and treatment. This study examined the clinical characteristics of patients with coincident TB and PJP and identified the associated mortality risk factors.
Methods: Patients diagnosed with TB and PJP at our center between January 2018 and December 2023 were retrospectively investigated. Data on demographics, diagnostic methods, clinical symptoms, imaging findings, laboratory examinations, treatment regimens, and clinical outcomes were collected from electronic medical records and summarized. The risk factors for mortality were then explored by logistic regression analysis, and the corresponding odds ratios (ORs) and 95% confidence intervals (CIs) were calculated.
Results: In total, 26 patients were included (mean age, 61.6 ± 16.6 years; illness duration, 39.8 ± 53.1 days). All cases of PJP were diagnosed by next-generation sequencing. The most common symptoms were cough (88.5%), fever (84.6%), and shortness of breath (69.2%). Chest imaging predominantly revealed ground-glass opacities (57.7%). Six patients (23.1%) died during hospitalization. Multivariate analysis identified the oxygenation index (OR = 0.979, 95% CI = 0.976– 0.982) and lymphocyte count (OR = 0.006, 95% CI = 0.002– 0.017) as independent risk factors for mortality.
Conclusion: Favorable clinical outcomes can be expected in most cases of coincident TB and PJP. However, decreases in the oxygenation index and lymphocyte count increase the risk of mortality.
Keywords: tuberculosis, Pneumocystis jirovecii pneumonia, prognosis, risk factors
Introduction
Tuberculosis (TB) remains a major public health challenge, and it has re-emerged as the world’s leading cause of death from a single infectious agent (replacing COVID-19).1 China, one of the 30 high TB burden countries, accounted for 6.8% of the global TB burden in 2023.2 Several factors, including HIV infection, the use of immunosuppressive drugs, smoking, and diabetes, have contributed to the increasing prevalence of TB, complicating TB control and treatment efforts.3–5
Similar to TB, Pneumocystis jirovecii pneumonia (PJP) is a common opportunistic infection, particularly in individuals with HIV. In regions with high HIV prevalence, the co-occurrence of pulmonary TB (PTB) and PJP is not uncommon. However, the diagnosis of PJP is complicated by the non-specific nature of its clinical symptoms and routine laboratory or radiological findings. Because Pneumocystis spp. cannot be cultured, diagnosis typically relies on invasive procedures or specialized staining techniques, which may not be available in all healthcare settings.6,7
Furthermore, diagnosing concurrent PJP and PTB presents significant challenges because of their overlapping clinical features, complicating differential diagnosis and increasing the risk of adverse clinical outcomes, including morbidity and mortality. The need for multiple treatments also raises concerns about drug intolerance and potential liver or kidney toxicity attributable to polypharmacy.8–10
Although coincident PTB and PJP have been documented in the literature and China ranks third in TB burden, the relatively low prevalence of HIV in the region has resulted in limited data on concurrent PTB and PJP. In general, reports of PTB and PJP co-infection are scarce in HIV-positive individuals, and to date, only a few cases have been documented in HIV-negative patients.11 Therefore, in this study, we examined the clinical characteristics of coincident PTB and PJP and assessed the associated mortality risk factors at a referral center in Eastern China.
Methods
Ethics
This study protocol was approved by the Ethics Committee of Zhejiang Hospital of Integrated Traditional Chinese and Western Medicine (approval number: 2024–096-001). As the study was retrospective in nature, the requirement for written informed consent was waived by the committee.
Subjects
Between December 2018 and December 2023, patients diagnosed with PTB and PJP were identified through a review of electronic medical records. PTB was diagnosed using a combination of microbiological, molecular, and clinical criteria.12 Mycobacterial culture, PCR, and Xpert MTB/RIF assays were performed on sputum samples when PTB was clinically suspected on the basis of symptoms and chest imaging. Targeted next-generation sequencing (tNGS) was employed for patients with inconclusive or discordant results from conventional tests or when drug-resistant TB was suspected on the basis of clinical history or epidemiological risk factors. Acid-fast bacillus (AFB) smear microscopy was also used to aid in the diagnostic workflow. PJP was diagnosed using two key criteria: the presence of symptoms, including fever, dry cough, and shortness of breath, along with chest imaging findings; and laboratory examination, including Gomori′s methenamine silver stain or immunofluorescence staining, PCR, or tNGS (≥8 copies/5 µL).13
Data Collection
We collected the following data for the included patients: age, sex, symptoms, underlying diseases, laboratory examinations, radiological findings, treatment regimens, and clinical outcomes.
For patients with suspected PTB, sputum, induced sputum, or bronchoalveolar lavage fluid samples were collected and sent for AFB smear, PCR, Xpert, and mycobacterial culture. For patients with suspected PJP, respiratory samples were tested using Gomori′s methenamine silver stain, immunofluorescence staining, PCR, and next-generation sequencing (NGS).
Statistical Analysis
All statistical analyses were performed using SPSS version 26.0 software. Continuous variables were expressed as the mean ± standard deviation (SD) and compared using the t-test or Mann–Whitney U-test depending on the data distribution. Categorical variables were analyzed using the χ2 test for proportions, and Fisher’s exact test was applied when the sample size was <40. Logistic regression analysis was conducted to identify factors associated with mortality. P < 0.05 denoted statistical significance.
Results
Basic Characteristics
The study included 26 patients diagnosed with both PTB and PJP. The average age of the cohort, which had a male predominance (20 men, 6 women), was 61.1 ± 16.6 years. The duration of illness was highly variable, with a mean of 39.8 ± 53.1 days (Table 1). Regarding diagnostic methods, most patients were diagnosed through a combination of mycobacterial culture (n = 10), Xpert MTB/RIF (n = 13), and tNGS for both TB (n = 21) and PJP (n = 26). Common symptoms included cough (n = 23), fever (n = 22), sputum production (n = 19), and dyspnea (n = 18), whereas weight loss and chest pain were reported in eight and five patients, respectively. Comorbidities were frequent, with two, three, four and three patients having chronic kidney disease, diabetes, HIV, and histories of cytomegalovirus infection, respectively. The notable laboratory findings included C-reactive protein elevation (65.6 ± 50.8 mg/L). Radiological findings revealed bilateral lung involvement in 17 patients, with common CT features including ground-glass opacities (n = 15), patchy shadows (n = 16), and pleural effusion (n = 10). The treatment regimens were diverse, with some patients receiving the standard anti-tuberculosis regimen (n = 5), along with trimethoprim–sulfamethoxazole (n = 21) therapy for PJP. Additionally, some patients received antibiotics, such as meropenem (n = 8), or antifungal agents such as voriconazole (n = 6). Six patients died, and in all cases, severe pneumonia attributable to PJP and leading to multiple-organ dysfunction syndrome was the immediate cause of death.
 |
Table 1 Clinicopathological Characteristics of Patients with Coincident Pulmonary Tuberculosis and PJP (n = 26) |
Comparison Between the Survival and Death Groups
A comparison of the survival and death groups revealed several important differences. Although those who survived had a lower mean age (59.0 ± 18.1 years) than those who died (68.3 ± 7.1 years), the difference was not statistically significant (P = 0.34). The duration of illness was shorter in the death group (13.5 ± 5.8 days) than in the survival group (47.7 ± 58.4 days), but this also did not reach statistical significance (P = 0.4). The presence of diabetes was significantly higher in the death group (P = 0.008), suggesting its role as a potential risk factor for mortality. Laboratory data illustrated that the lymphocyte count was significantly lower in the death group (0.2 ± 0.1 × 109/L) than in the survival group (0.5 ± 0.3 × 109/L, P = 0.0001). Radiologically, ground-glass opacities and patchy shadows were more prevalent in the death group (P = 0.022 and P = 0.035, respectively). Regarding treatment, no significant differences were observed in the use of anti-TB regimens or treatments for PJP between the two groups, indicating that the treatment approaches were similar (Table 1).
Logistic Regression Analysis
Variables included in the logistic regression analysis were selected according to clinical or statistical significance. Diabetes and the lymphocyte count were included because of their significance in univariate analysis, whereas lung involvement and the oxygenation index (PaO2/FiO2) ratio were selected because of their clinical relevance. Multivariate logistic regression analysis identified two independent risk factors for mortality among patients with PTB and PJP: PaO2/FiO2 (odds ratio [OR] = 0.979, 95% confidence interval [CI] = 0.976–0.982) and the lymphocyte count (OR = 0.006, 95% CI = 0.002–0.017, Table 2).
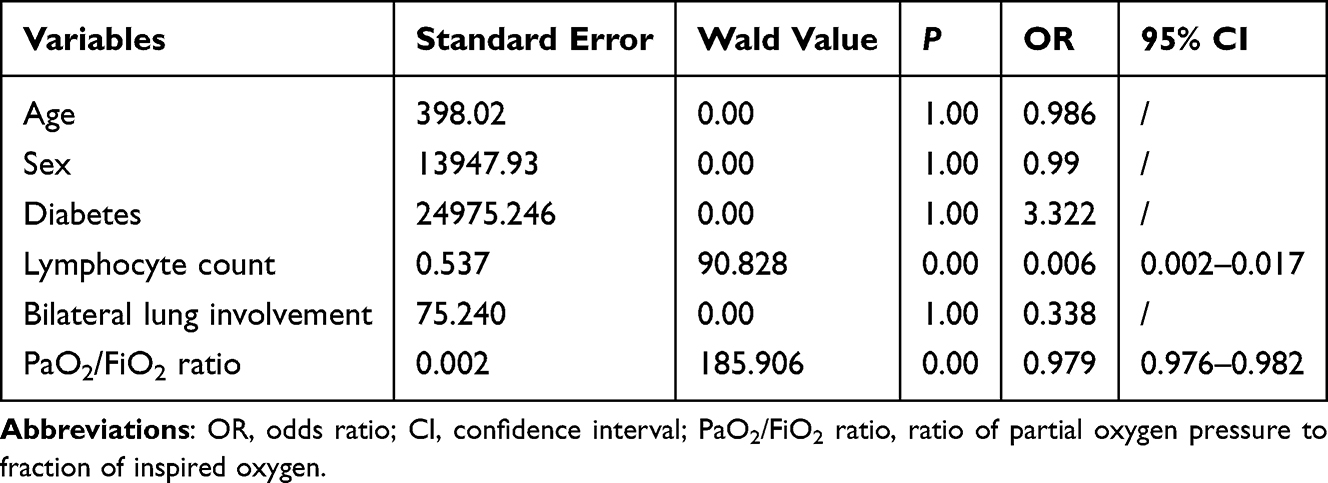 |
Table 2 Multivariate Logistic Regression Analysis of Mortality in Patients with Coincident Pulmonary Tuberculosis and PJP |
Discussion
Both TB and PJP are opportunistic diseases, and co-infection by their causative pathogens is not rare, particularly in patients with AIDS. Previous studies reported a co-infection rate of approximately 5% in HIV-infected individuals.14 However, the coexistence of TB and PJP in non-HIV–infected patients with immune deficiencies remains underexplored, with only isolated case reports available.10,15,16 This study investigated clinical characteristics and identified mortality risk factors in patients with coincident PTB and PJP, a cohort that presents significant diagnostic and therapeutic challenges. Our findings provide valuable insights into the complexities of diagnosing and managing these diseases, particularly in settings with a high TB burden and relatively low HIV prevalence, such as China.
In our cohort, the diagnosis of coincident PTB and PJP presented significant challenges. The clinical presentation was dominated by common respiratory symptoms, including cough, fever, and dyspnea, which are characteristic of both PTB and PJP. Radiologically, ground-glass opacities (57.7%), which are typically associated with PJB but also encountered in PTB, represented the most frequent finding. Additionally, bilateral lung involvement (65.4%) and patchy shadows (61.5%) were prevalent, indicating substantial lung damage in these patients. A key strength of this study was the use of NGS to confirm the diagnosis of both PTB and PJP, overcoming the limitations of traditional diagnostic methods. This approach enabled the detection of PJP in all cases, demonstrating the value of molecular techniques in diagnosing complex infections, particularly in patients with atypical presentations or when conventional tools, such as sputum culture, are ineffective.
The diagnosis of PTB in our cohort was relatively straightforward, with AFB smear, culture, nucleic acid amplification tests, and the Xpert MTB/RIF assay being routinely used in clinical practice. Notably, the Xpert MTB/RIF assay, which has been endorsed by the World Health Organization, offers a rapid and reliable diagnostic alternative, with sensitivity and specificity approaching 98%. However, the diagnosis of PJP remains more challenging despite the availability of diagnostic tools. Traditional methods, such as Gomori′s methenamine silver stain and direct fluorescent antibody staining, offer limited sensitivity, particularly in immunocompromised patients or those with low organism burdens. Although real-time PCR improves sensitivity and permits earlier detection, challenges persist, including the difficulty in distinguishing between active infection and colonization, as well as the high cost and limited availability of molecular tests in some settings.17,18 NGS, with its superior diagnostic sensitivity, has been increasingly incorporated into clinical practice because of its ability to reduce both diagnostic time and costs.19,20 Compared with traditional methods, NGS offers a significant advantage in diagnosing mixed infections, such as concurrent TB and PJP.21 However, because NGS can detect colonization, results should always be interpreted in conjunction with clinical symptoms and radiological imaging for a comprehensive and accurate diagnosis.22 Additionally, the typical radiological features of PTB include subpleural nodules, cavitary lesions, and mediastinal lymphadenopathy. Conversely, PJP typically presents as widespread ground-glass opacities with or without reticular or cystic lesions, and it might involve interstitial fibrosis in chronic cases.23 In co-infected patients, a combination of classic PTB features and ground-glass opacities revealed by imaging might represent a valuable diagnostic clue.9,13,24
Six patients (23.1%) died during hospitalization, and this relatively high mortality rate highlights the severity of coincident TB and PJP. Mortality risk in these patients might be influenced by a variety of factors, including their immunocompromised status, delayed diagnosis, and complications from polypharmacy. We identified the oxygenation index and lymphocyte count as independent risk factors for mortality. The PaO2/FiO2 ratio is a well-established indicator of respiratory function that is widely used to assess the severity of respiratory failure.25,26 Our findings suggested that a lower PaO2/FiO2 ratio is associated with higher mortality risk, which reflects the severity of respiratory impairment in co-infected patients. Given that both TB and PJP can cause significant lung damage, early detection of hypoxemia and prompt intervention are critical for improving outcomes. It is possible that co-infection by these two pathogens leads to a synergistic effect, overwhelming the respiratory system more rapidly than either infection alone.
Lymphopenia was also a significant predictor of mortality in this study. A lower lymphocyte count is a well-documented marker of poor prognosis in infectious diseases, particularly in patients with HIV or other immunocompromised states.27,28 Lymphocytes play a crucial role in controlling TB and PJP infections, and their depletion might result in an inability to mount an effective immune response.29,30 Notably, several studies demonstrated that low lymphocyte counts predispose HIV-negative individuals to an increased risk of PJP.31 Chronic immunodeficiency with either disease-related or iatrogenic causes compromises the host’s ability to control opportunistic pathogens. Furthermore, lymphopenia is a recognized risk factor for late-onset PJP.32 Lymphocyte subtyping has also proven valuable in predicting PJB and its associated mortality in HIV-negative patients, with low CD8+ T cell counts identified as an independent and strong predictor of mortality.33 In the context of PTB, lymphopenia has similarly deleterious consequences. M. tuberculosis-specific T cell-mediated immunity plays a critical role in bacterial clearance. Consequently, lymphopenia can contribute to persistent bacterial replication and tissue damage. In addition, profound depletion of lymphocytes can lead to broad immunosuppression in patients with TB.34 Collectively, these immunological impairments can result in delayed bacterial clearance, uncontrolled Th1-driven cytokine production, and even cytokine storms, ultimately culminating in multiple-organ dysfunction and death.34 The finding that low lymphocyte counts are associated with increased mortality underscores the importance of monitoring the immune status in these patients and considering immunotherapy or other interventions to bolster immune function.
Although this study included a relatively large sample given the rarity of coincident TB and PJP in areas with a low HIV prevalence, the overall sample size was limited, which might have restricted the statistical power to detect smaller effect sizes. The retrospective design inherently limited causal inferences and introduced potential biases related to data availability and completeness. The single-center setting at a referral hospital might have further contributed to selection bias, as such centers typically manage more complex or severe cases, and they might not fully capture the spectrum of patients with coincident TB and PJP in the broader community. Consequently, the generalizability of our findings might be limited. Furthermore, because the study was conducted in an area with a low HIV prevalence, it remains unclear whether the findings are applicable to regions with a higher HIV burden. Given that HIV is a significant risk factor for both TB and PJP, future prospective, multicenter studies with larger sample sizes, longer follow-up periods, and cohorts from regions with varying HIV prevalence are needed to confirm these findings and better understand the clinical characteristics, outcomes, and long-term management of coincident TB and PJP.
Conclusions
Coincident PTB and PJP is not rare, and it represents a challenging clinical scenario that is associated with a high mortality risk. In this cohort, two independent risk factors for mortality (oxygenation index and lymphocyte count) were identified. Early recognition of these markers, coupled with prompt and aggressive diagnostic and therapeutic interventions, is crucial for improving patient outcomes. Given the diagnostic complexity of these co-infections, especially in settings with limited access to advanced molecular diagnostics, clinicians should maintain a high index of suspicion and consider early initiation of appropriate therapies based on clinical and radiographic findings. Future research should focus on large-scale, prospective, multicenter studies to validate these mortality risk factors and identify additional predictors that might influence clinical outcomes. Operational research is warranted to assess the feasibility and cost-effectiveness of incorporating advanced diagnostic modalities, such as NGS, into routine practice in resource-constrained settings. Finally, investigations into potential interventions, including immunomodulatory therapies and tailored treatment strategies, are essential to improve clinical management and outcomes for patients with coincident TB and PJP.
Abbreviations
AFB, acid-fast bacillus; CIs, confidence intervals; TB, tuberculosis; ORs, odds ratios; NGS, next-generation sequencing; PJP, Pneumocystis jirovecii pneumonia; TB PTB, pulmonary; SD, standard deviation; tNGS, targeted next-generation sequencing.
Data Sharing Statement
The datasets generated and analyzed during the present study are available from the corresponding author on reasonable request.
Human Ethics and Consent to Participate
This study protocol was approved by the Ethics Committee of Zhejiang Hospital of Integrated Traditional Chinese and Western Medicine (approval number: 2024-096-001). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 helsinki declaration and its later amendments or comparable ethical standards. As the study was retrospective in nature, the requirement for written informed consent was waived by the Ethics Committee of Zhejiang Hospital of Integrated Traditional Chinese and Western Medicine. All data were fully anonymized and handled with strict confidentiality.
Funding
This research was supported by grants from the Hangzhou Biomedicine and Health Industry Development Project (2023WJC118) and Hangzhou Municipal Science and Technology Bureau’s Guided Project (20220919Y034).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Wise J. Tuberculosis: health chiefs issue warning over rise in cases. BMJ. 2024;387:q2758. doi:10.1136/bmj.q2758
2. Organization WH. Global tuberculosis report 2024; 2024.
3. Sadeghi K, Poorolajal J, Doosti-Irani A. Prevalence of modifiable risk factors of tuberculosis and their population attributable fraction in Iran: a cross-sectional study. PLoS One. 2022;17(8):e0271511. doi:10.1371/journal.pone.0271511
4. Adhikari N, Bhattarai RB, Basnet R, et al. Prevalence and associated risk factors for tuberculosis among people living with HIV in Nepal. PLoS One. 2022;17(1):e0262720. doi:10.1371/journal.pone.0262720
5. Liu X, Zhang L, Zhang F, et al. Prevalence and risk factors of active tuberculosis in patients with rheumatic diseases: a multi-center, cross-sectional study in China. Emerg Microbes Infect. 2021;10(1):2303–2312. doi:10.1080/22221751.2021.2004864
6. Choe PG, Kang YM, Kim G, et al. Diagnostic value of direct fluorescence antibody staining for detecting Pneumocystis jirovecii in expectorated sputum from patients with HIV infection. Med Mycol. 2014;52(3):326–330. doi:10.1093/mmy/myu002
7. Kaur R, Wadhwa A, Bhalla P, Dhakad MS. Pneumocystis pneumonia in HIV patients: a diagnostic challenge till date. Med Mycol. 2015;53(6):587–592. doi:10.1093/mmy/myv023
8. Sheikholeslami MF, Sadraei J, Farnia P, Forozandeh Moghadam M, Emadi Kochak H. Co-infection of Mycobacterium tuberculosis and Pneumocystis jirovecii in the Iranian patients with human immunodeficiency virus. Jundishapur J Microbiol. 2015;8(2):e17254. doi:10.5812/jjm.17254
9. Wei S, Lin L. Pneumocystis jirovecii and Mycobacterium tuberculosis pulmonary coinfection in an HIV-Seronegative patient: a case report and literature review. Infect Drug Resist. 2022;15:4149–4154. doi:10.2147/IDR.S370023
10. Suk CW, Bai KJ, Yu MC, Hu TY. Coinfection of Pneumocystis jiroveci pneumonia and pulmonary tuberculosis in a non-HIV-infected patient. J Microbiol Immunol Infect. 2015;48(6):711–712. doi:10.1016/j.jmii.2014.07.001
11. Mongardon N, Bruneel F, Henry-Lagarrigue M, Legriel S, Azarian R, Bedos JP. Pneumonia involving Mycobacterium tuberculosis and Pneumocystis jiroveci in HIV-seronegative patients. Eur J Intern Med. 2008;19(7):e70–72. doi:10.1016/j.ejim.2008.04.004
12. Lin Z, Er-yong L, Qing-lin M, et al. Evaluation of the quality of pulmonary tuberculosis diagnosis after the implementation of the newly revised WS 288-2017 Diagnosis for pulmonary tuberculosis standards; 2020.
13. Salzer HJF, Schafer G, Hoenigl M, et al. Clinical, diagnostic, and treatment disparities between HIV-infected and non-HIV-infected immunocompromised patients with Pneumocystis jirovecii Pneumonia. Respiration. 2018;96(1):52–65. doi:10.1159/000487713
14. Rozaliyani A, Wiyono WH, Nawas MA, et al. Laboratory findings and clinical characteristics of Pneumocystis pneumonia and tuberculosis infection among HIV-infected patients with pulmonary infiltrates in Jakarta, Indonesia. Trop Biomed. 2020;37(4):1117–1123.
15. Hou J, Cao J, Tan P, Yu Y. Pneumocystis jiroveci pneumonia, Nocardia brasiliensis, and Mycobacterium tuberculosis co-infection in a myasthenia gravis patient: a case report. Medicine. 2021;100(1):e24245. doi:10.1097/MD.0000000000024245
16. Janmeja AK, Mohapatra PR, Shivaprakash MR, Khurana A, Aggarwal D. Concurrent infection of pneumocystis pneumonia and pulmonary tuberculosis in an HIV-seronegative patient. Indian J Chest Dis Allied Sci. 2008;50(4):369–371.
17. Bateman M, Oladele R, Kolls JK. Diagnosing Pneumocystis jirovecii pneumonia: a review of current methods and novel approaches. Med Mycol. 2020;58(8):1015–1028. doi:10.1093/mmy/myaa024
18. White PL, Backx M, Barnes RA. Diagnosis and management of Pneumocystis jirovecii infection. Expert Rev Anti Infect Ther. 2017;15(5):435–447. doi:10.1080/14787210.2017.1305887
19. Cheng QW, Shen HL, Dong ZH, et al. Pneumocystis jirovecii diagnosed by next-generation sequencing of bronchoscopic alveolar lavage fluid: a case report and review of literature. World J Clin Cases. 2023;11(4):866–873. doi:10.12998/wjcc.v11.i4.866
20. Huang JJ, Zhang SS, Liu ML, Yang EY, Pan Y, Wu J. Next-generation sequencing technology for the diagnosis of Pneumocystis pneumonia in an immunocompetent female: a case report. World J Clin Cases. 2023;11(18):4425–4432. doi:10.12998/wjcc.v11.i18.4425
21. Zhao M, Yue R, Wu X, Gao Z, He M, Pan L. The diagnostic value of metagenomic next-generation sequencing for identifying Pneumocystis jirovecii infection in non-HIV immunocompromised patients. Front Cell Infect Microbiol. 2022;12:1026739. doi:10.3389/fcimb.2022.1026739
22. Vera C, Rueda ZV. Transmission and colonization of Pneumocystis jirovecii. J Fungi. 2021;7(11):979. doi:10.3390/jof7110979
23. Kunihiro Y, Tanaka N, Kawano R, et al. Differential diagnosis of pulmonary infections in immunocompromised patients using high-resolution computed tomography. Eur Radiol. 2019;29(11):6089–6099. doi:10.1007/s00330-019-06235-3
24. Yamao S, Jint T, Nishimura N, Fujiwara M, Suzuki K, Chohnabayashi N. Coinfection with Pneumocystis jirovecii and Mycobacterium tuberculosis in a patient with AIDS: a first report in Japan. Nihon Kokyuki Gakkai Zasshi. 2011;49(3):192–196.
25. Palanidurai S, Phua J, Chan YH, Mukhopadhyay A. P/FP ratio: incorporation of PEEP into the PaO(2)/FiO(2) ratio for prognostication and classification of acute respiratory distress syndrome. Ann Intensive Care. 2021;11(1):124. doi:10.1186/s13613-021-00908-3
26. Sartini S, Massobrio L, Cutuli O, et al. Role of SatO2, PaO2/FiO2 Ratio and PaO2 to predict adverse outcome in COVID-19: a retrospective, cohort study. Int J Environ Res Public Health. 2021;18(21):11534. doi:10.3390/ijerph182111534
27. Vaughan J, Wiggill T, Lawrie D, Machaba M, Patel M. The prognostic impact of monocyte fluorescence, immunosuppressive monocytes and peripheral blood immune cell numbers in HIV-associated diffuse large B-cell Lymphoma. PLoS One. 2023;18(1):e0280044. doi:10.1371/journal.pone.0280044
28. Cai CW, Sereti I. Residual immune dysfunction under antiretroviral therapy. Semin Immunol. 2021;51:101471. doi:10.1016/j.smim.2021.101471
29. Dheda K, Schwander SK, Zhu B, van Zyl-Smit RN, Zhang Y. The immunology of tuberculosis: from bench to bedside. Respirology. 2010;15(3):433–450. doi:10.1111/j.1440-1843.2010.01739.x
30. Deng Z, Zheng Y, Cai P, Zheng Z. The role of B and T lymphocyte attenuator in respiratory system diseases. Front Immunol. 2021;12:635623. doi:10.3389/fimmu.2021.635623
31. Overgaard UM, Helweg-Larsen J. Pneumocystis jiroveci pneumonia (PCP) in HIV-1-negative patients: a retrospective study 2002–2004. Scand J Infect Dis. 2007;39(6–7):589–595. doi:10.1080/00365540601150497
32. Kaminski H, Belliere J, Burguet L, et al. Identification of predictive markers and outcomes of late-onset Pneumocystis jirovecii Pneumonia in kidney transplant recipients. Clin Infect Dis. 2021;73(7):e1456–e1463. doi:10.1093/cid/ciaa1611
33. Li Y, Ghannoum M, Deng C, et al. Pneumocystis pneumonia in patients with inflammatory or autoimmune diseases: usefulness of lymphocyte subtyping. Int J Infect Dis. 2017;57:108–115. doi:10.1016/j.ijid.2017.02.010
34. Li F, Chen D, Zeng Q, Du Y. Possible mechanisms of lymphopenia in severe Tuberculosis. Microorganisms. 2023;11(11):2640. doi:10.3390/microorganisms11112640
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prognostic Factors of Adrenocortical Carcinoma: Experience from a Regional Medical Center in Eastern China
Li P, Su X, Zhang X, Sun L, Zhang G
International Journal of General Medicine 2023, 16:453-465
Published Date: 3 February 2023
Incidence and Risk Factors of Cranial Nerve Palsy in Patients with Tuberculous Meningitis: A Retrospective Evaluation
Wen A, Cao WF, Liu SM, Zhou YL, Xiang ZB, Hu F, Wu LF, Cai W, Leng EL
Infection and Drug Resistance 2023, 16:829-841
Published Date: 14 February 2023
Exploration of the Risk Factors of Anemia in Patients with Tuberculous Meningitis in South China
Wen A, Leng EL, Cao WF, Xiang ZB, Rao W, Cai W, Zhou YL, Hu F, Wu LF, Zhang P, Liu SM
Neuropsychiatric Disease and Treatment 2023, 19:369-377
Published Date: 16 February 2023
External Validation of the Nelson Equation for Kidney Function Decline in Patients with Acute Ischemic Stroke or Transient Ischemic Attack
Zhou H, Chen W, Suo Y, Meng X, Zhao X, Wang M, Liu L, Li H, Pan Y, Wang Y
Clinical Interventions in Aging 2023, 18:901-909
Published Date: 6 June 2023
Predictors of Tuberculosis and Non-Communicable Disease Comorbidities Among Newly Enrolled Tuberculosis Patients, Southern Ethiopia
Nunemo MH, Gidebo KD, Woticha EW, Lemu YK
Integrated Blood Pressure Control 2023, 16:95-109
Published Date: 22 November 2023