")
Back to Journals » Clinical Ophthalmology » Volume 18
Clinical Characteristics and Prognostic Factors of Patients with Intraocular Foreign Bodies from a Tertiary Eye Center in North China
Authors Xing X, Liu F, Qi Y, Li J , Yu B, Wan L
Received 9 October 2024
Accepted for publication 28 November 2024
Published 7 December 2024 Volume 2024:18 Pages 3635—3643
DOI https://doi.org/10.2147/OPTH.S492986
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Xiaoli Xing,1– 3 Fang Liu,1– 3 Yan Qi,1– 3 Jun Li,1– 3 Bin Yu,1– 3 Lei Wan1– 3
1Eye Institute of Shandong First Medical University, Qingdao Eye Hospital of Shandong First Medical University, QingDao, People’s Republic of China; 2State Key Laboratory Cultivation Base, Shandong Provincial Laboratory of Eye Diseases, QingDao, People’s Republic of China; 3School of Ophthalmology, Shandong First Medical University, QingDao, People’s Republic of China
Correspondence: Lei Wan, Qingdao Eye Hospital of Shandong First Medical University, 5 Yanerdao Road, QingDao, 266000, People’s Republic of China, Email [email protected]
Background: This study aims to describe the epidemiology and clinical features of patients with intraocular foreign bodies (IOFBs) and analyze the prognostic factors influencing final vision.
Methods: We retrospectively reviewed medical records of patients with IOFBs admitted to Qingdao Eye Hospital of Shandong First Medical University between January 1, 2014, and December 31, 2021. Inclusion criteria involved complete clinical data details of patients diagnosed with intraocular foreign bodies in our hospital who were treated with concurrent surgery and based on IOFB position and characteristics, different surgical methods were employed. The minimum follow-up duration was 6 months. Exclusion criteria were foreign bodies retained in the orbit, organ failure, surgical contraindications, coagulation abnormalities, autoimmune diseases, history of ocular surgery, and ocular space-occupying lesions. Based on IOFB position and characteristics, different surgical methods were employed. Multivariate logistic regression analysis was performed to predict independent factors influencing final visual acuity after IOFBs.
Results: This study analyzed 159 patients (159 eyes) with IOFBs. Based on discharge and follow-up results, IOFB removal was performed through pars plana incision in 105 (67.9%) eyes, corneoscleral limbus incision in 24 (15.1%) eyes, and original wound in 27 (17.0%) eyes. Of these, 44 eyes underwent IOFB removal without vitrectomy, while 55 (34.6%) eyes were treated with silicone oil. Post-vitrectomy, three cases showed secondary macular membrane, five cases exhibited retinal detachment, and enucleation was necessary in three cases. The final best corrected visual acuity (BCVA, logMAR) was 1.06 ± 0.88, significantly better than preoperative visual acuity of 1.65 ± 0.87 (t = 8.21, p < 0.01). Multi-factor logistic regression analysis revealed that the length of corneal/scleral wound (OR=0.6 P < 0.05), maximum size of IOFB (OR=0.585 P < 0.05), initial presenting VA (OR=0.900 P < 0.05), and macular lesions(OR=0.400 P < 0.05) were risk factors for postoperative vision prognosis after intraocular foreign body surgery.
Conclusion: In a tertiary eye center in northern China, IOFBs predominantly affected the working-age group, particularly males. Factors such as wound length, IOFB size, initial presenting VA, and macular lesions might impact the final visual outcome.
Keywords: intraocular foreign bodies, prognostic factors
Background
Intraocular foreign body (IOFB) injuries constitute a frequent and severe form of eye trauma, accounting for 18%–41% of all open-globe injuries.1–3 Ocular trauma involving IOFBs is a significant cause of visual morbidity and working-age blindness.2,4,5 The causes of IOFBs include a range of incidents, including splashing, stabbing, explosive materials, and fireworks.Common work activities such as hammering, polishing, welding, and drilling often lead to splashing. Various materials such as metal, plastic, stone, and debris entering the eye not only cause mechanical damage but also exhibit toxic effects on ocular tissues. These injuries elevate the risk of intraocular infection, retinal necrosis, and sympathetic ophthalmitis, and in severe instances, can result in blindness.
Swift foreign body removal is therefore imperative. Given the complexity of IOFBs, the nature, size, shape, location, and patient condition must be considered when choosing removal methods and timing. Previous studies have identified characteristics of IOFBs as predictive factors, indicating their correlation with visual outcomes and management. However, most of these studies were conducted among Western populations and in South China. However, different regions and countries in the world have different economic and medical development levels, and the epidemiology, clinical characteristics, and treatment prognosis of patients with intraocular foreign bodies may also be different. Therefore, it is imperative to present a study about the current IOFB situation in northern China. The results of this study may serve as guidance for IOFB effective treatment plans and visual outcome comprehensive evaluation in the clinical setting in order to save patients’ vision.
Materials and Methods
Population
We retrospectively reviewed consecutive medical records of all IOFB patients admitted to Qingdao Eye Hospital of Shandong First Medical University between January 1, 2014, and December 31, 2021. Each case was documented using a standardized preformulated datasheet. Inclusion criteria involved complete clinical data details of patients diagnosed with intraocular foreign bodies in our hospital who were treated with concurrent surgery and based on IOFB position and characteristics, different surgical methods were employed. The minimum follow-up duration was 6 months. Exclusion criteria were foreign bodies retained in the orbit, surgical contraindications such as organ dysfunction, coagulation abnormalities, autoimmune diseases, history of fundus or ocular trauma or glaucoma surgery, and ocular space-occupying lesions. The study was approved by the hospital’s ethics committee and adhered to the Declaration of Helsinki.
Procedures
A detailed trauma history was collected for all patients, followed by a comprehensive ophthalmological examination, including best corrected visual acuity (BCVA), intraocular pressure, slit-lamp biomicroscopy, color fundus photography, indirect ophthalmoscopy, ocular ultrasound, and computed tomography (CT) scans. We defined characteristic IOFBs as metal with the help of CT performed for determining the type of IOFBs. On CT, wood density was the lowest, followed by plastic and then glass. Specific details about retained IOFBs, including age, sex, cause of trauma, wound site, and length, were recorded using a standardized data sheet. The zone of open globe injury is based on the standard Birmingham Eye Trauma Terminology as described by F Kuhn et al, and wound entry sites were categorized as zone I (limited to corneal area, including corneoscleral limbus), zone II (5 mm posterior to corneoscleral limbus), and zone III (posterior to anterior 5 mm of sclera).6 Additional details regarding IOFB injury, such as material, longest diameter, location, and timing of removal, were documented. Additionally, the presence of uveal tissue prolapse, hyphema, traumatic lens rupture, vitreous hemorrhage, retinal damage, retinal detachment, endophthalmitis, and siderosis bulbi were noted.
Based on IOFB position and characteristics, different surgical methods were employed: (1) Anterior chamber foreign bodies were extracted using a relay magnet or tweezers, with viscoelastic agent to protect the cornea. (2) Intraocular lens foreign bodies warranted corneoscleral wound repair, limbal incision, and lens removal via phacoemulsification, with consideration for one-stage intraocular lens implantation or anterior vitrectomy based on eye condition. (3) Posterior eye foreign bodies were removed using magnets and intraocular micro-forceps without pars plana vitrectomy (PPV) if certain conditions were met: intact lens, no vitreous hemorrhage or retinal complications in the vitreous cavity, and absence of significant retinal complications or hemorrhage in the eyeball wall and retina embedding. Otherwise, standard 3-port 25-gauge PPV was performed.
The Ocular Trauma Classification Group’s classification system was widely employed in our clinic. VA acuity was categorized into five groups based on the OTS classification: 1). no light perception; 2). light perception/hand motions; 3). 1/200 to–19/200; 4). 20/200 to < 20/50; or 5). ≥ 20/40.
Statistical analysis: Statistical analyses were conducted using SPSS V.22.0. Categorical variables were assessed using the Chi-square test. Furthermore, multivariate logistic regression analysis was performed to predict independent factors influencing final visual acuity after IOFBs.Visual acuity prognosis was used as the dependent variable (assigned as 1 = visual acuity < 20/200, 2 = visual acuity ≥ 20/200). The factors with statistical significance in the Chi-square test were used as independent variables for multivariate logistic regression analysis. A P value of less than 0.05 was considered statistically significant for all tests.
Results
This study included 159 patients (159 eyes) with IOFBs. The patients’ ages ranged from 10 to 67 years (mean, 41.58 ±11.97 years). There were 151 (95%) male and 8 (5%) female patients. The most common age group was 40–49 years (32.7%, n = 52), followed by those aged 50–59 years (25.8%, n = 41) and 30–39 years (19.6%, n = 31). All IOFBs in this study were observed to occur during work. Our study identifies splashing as the leading cause of IOFBs.
Characteristics of IOFBs
The characteristics of IOFBs are outlined in Table 1. Zone I comprised 110 eyes (73.0%), zone II had 40 eyes (22.0%), and zone III consisted of 8 eyes (5.0%). IOFBs were located on the sclera in 13 eyes (8.2%), in the anterior chamber in 6 eyes (3.8%), in the lens in 13 eyes (8.2%), in the vitreous cavity in 96 eyes (60.4%), and embedded in the retina in 27 eyes (17.0%). The properties of IOFBs varied based on their source, with 90.6% being metal and the rest nonmetal. The foreign bodies exhibited a wide range of sizes, with the largest foreign body having a diameter of 28 mm. The interval between injury and surgical intervention spanned from 1 h to 20 years, and 34% of the patients underwent surgery 24 h after injury. The characteristics of corneal or scleral wounds and IOFBs are presented in Table 1.
 |
Table 1 Clinical Characteristics of Patients with IOFBs |
Ocular Findings of Patients with IOFBs
The ocular findings of patients with IOFBs are detailed in Table 1. Further analysis revealed hyphema in 16 cases (10.0%), traumatic cataract in 90 eyes (56.6%), vitreous hemorrhage in 38 eyes (23.9%), retinal detachment in 58 eyes (22.0%), macular lesions in 26 eyes (16.4%), siderosis in 8 eyes (5.0%), choroid detachment in 9 eyes (5.7%), and endophthalmitis in 25 eyes (15.7%). The most common ocular finding was traumatic cataract (56.6% of cases), followed by vitreous hemorrhage (23.9%).
Treatment
Based on discharge and follow-up outcomes, IOFB removal was performed through a pars plana incision in 108 eyes (67.9%), incision of the keratoscleral margin in 24 eyes (15.1%), and the original wound in 27 eyes (17.0%). A total of 44 eyes underwent IOFB removal without vitrectomy, while 55 eyes were treated with silicone oil. After vitrectomy, a secondary macular membrane was observed in three cases, retinal detachment was noted in five cases, and enucleation was necessary in three cases. And pathological examination of the removed eyeballs indicated suppurative endophthalmitis.
Outcomes and Factors Affecting Final VA
The final visual acuity (BCVA, logMAR) was 1.06 ±0.88, significantly better than the preoperative visual acuity of 1.65 ±0.87 (t = 8.21, p < 0.01). Factors influencing final visual acuity are presented in Table 2. The key factors significantly affecting final VA were the length of corneal/scleral wound, maximum size of IOFB, initial presenting VA, macular lesions, choroid detachment, and the difference was statistically significant (P < 0.05). However, factors like gender, timing of IOFB removal, site of laceration, IOFB location, material of IOFB, and endophthalmitis did not affect the final VA (P > 0.05). The length of corneal/scleral wound, maximum size of IOFB, initial presenting VA, and macular lesions were used as independent variables in logistic analysis in Table 3. Multi-factor logistic regression analysis revealed that the length of corneal/scleral wound (OR=0.6 P < 0.05), maximum size of IOFB (OR=0.585 P < 0.05), initial presenting VA (OR=0.900 P < 0.05), and macular lesions(OR=0.400 P < 0.05) were risk factors for postoperative vision prognosis after intraocular foreign body surgery.
 |
Table 2 Factors Influencing Foreign Body Characteristics on Final Visual Prognosis |
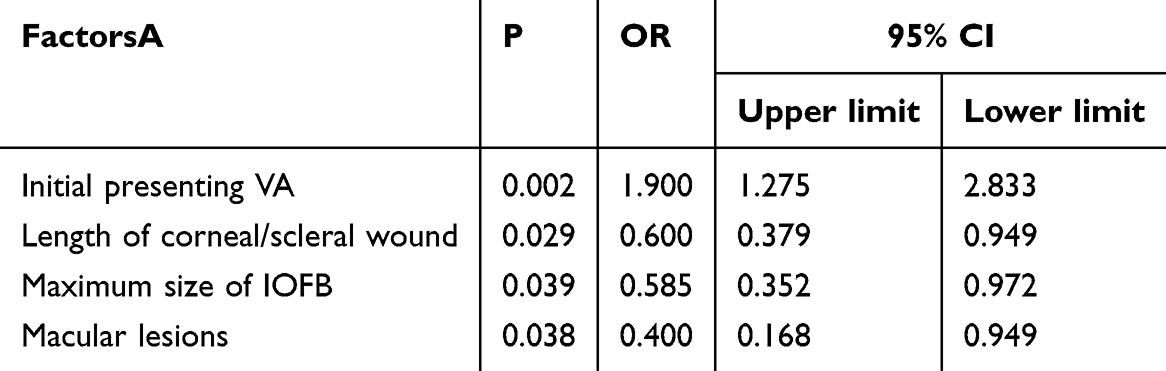 |
Table 3 Multivariate Logistic Regression Analysis of Influencing Factors of Visual Acuity After Intraocular Foreign Body Surgery |
Discussion
Ocular trauma stands as one of the leading causes of visual impairment, with IOFBs representing a significant component of ocular injuries.Work-related open globe injuries are a substantial source of ocular morbidity, as evidenced by our study’s findings indicating that IOFBs predominantly affect a male population aged 40 to 49 years (95.0% of patients). This trend is consistent with earlier research (94.8%).7 Likely, this pattern arises due to individuals in these age groups being more involved in physical labor. In China, a substantial proportion of the population engages in industrial and agricultural professions, with young males constituting the backbone of families and the primary productive workforce of the nation. For patients over 60 years old, the proportion of males was significantly lower than in other age groups. This phenomenon could be attributed to the customary retirement age of 60 for males in China, leading to reduced physical activity after retirement. Nonetheless, the substantial labor force and lack of labor protection contribute to the elevated incidence of IOFB injuries. Such injuries have a significant financial toll on society. Many workplace-related injuries are preventable; thus, emphasizing preventive measures could alleviate the burden on productivity and healthcare expenditures.8 Hence, promoting occupational safety measures is paramount.
IOFBs possess diverse attributes, including metal, glass, eyelashes, stone, plastic, and plants, among others. Our study predominantly found metallic foreign bodies, comprising 90.5% of the IOFB cases. Posterior segment IOFBs are commonly linked with complications like retinal detachment, endophthalmitis, and vitreous hemorrhage.9 Earlier reports documented endophthalmitis incidence in IOFB cases ranging from 0.00% to 16.55% (mean = 6.65%). In our study, endophthalmitis incidence stood at 15.7%, aligning with prior findings. As endophthalmitis can result in diverse ocular injuries, its prognosis tends to be unfavorable. It is essential to further investigate prognostic factors related to endophthalmitis. Zhang et al indicated that scleral wounds posed a lower endophthalmitis risk than corneal wounds.10 However, we did not obtain conclusive results, primarily due to the enhanced sanitary environment, which lowered the bacterial load carried by foreign bodies entering the eye and attenuated their pathogenicity. These perspectives necessitate larger sample sizes for further investigation.
Given that IOFBs inflict severe visual impairment, identifying prognostic factors affecting visual outcomes of affected eyes is crucial. Therefore, we analyzed selected variables that could influence final visual outcomes and overall eye survival. A study by Ameer et al (2009),11 demonstrated that final best corrected VA was worse than 6/60 in 48% of patients with eye injuries. In our study, this prevalence was 40.25%, aligning with the previous research. In our analysis, initial VA emerged as a critical factor impacting final vision, consistent with the hypotheses presented by Zhang Y2 and Jonas JB.12 Initial VA post-ocular trauma often reflects the extent of intraocular tissue damage; poorer initial VA translates to poorer final vision. However, final vision proved statistically independent of factors like age, refractive error, surgeon, time between the accident and foreign body removal,12 and duration of follow-up.
Wani VB also reported that timing of IOFB removal did not significantly influence final VA.13 Nevertheless, retaining foreign bodies within the eye can lead to complications such as siderosis bulbi. Siderosis bulbi is a chronic degenerative process stemming from chemical reactions between ocular tissues and iron particles, potentially arising between 18 days and several years post-trauma.14 In our study, siderosis bulbi incidence stood at 5.03%. Thus, prompt IOFB removal remains imperative.
Our study demonstrates that IOFB size significantly predicts final visual outcomes in IOFB patients. Chiquet et al evidenced that IOFBs under 3 mm in length exhibited a better prognosis, suggesting that a 1 mm increase in IOFB diameter raised the risk of poor VA by 1.2118.15 Similarly, Yang CS indicated that every millimeter increase in IOFB diameter corresponded to a 0.8 Snellen line decrease in final VA.16 Woodcock MG found that larger IOFBs causing more tissue damage correlated with poorer visual prognosis.8 It appears that larger foreign bodies, under identical conditions, induce more severe damage due to their higher energy and greater potential for retina injury.17 Zhang Y also proposed that posterior segment IOFBs were more likely to cause mechanical damage to intraocular tissues and generate higher kinetic energy, hence damaging intraocular tissue.2 Furthermore, Zhitao Su suggested that anterior IOFBs generally correlated with better final best-corrected visual acuity compared to posterior IOFBs.18 Yang Liu similarly established a link between IOFB location and poorer visual prognosis.19 In our study, IOFB location also emerged as a factor impacting visual prognosis, with larger foreign bodies being associated with worse vision.
In previous studies, prognosis often hinged on the location of the laceration, with lacerations in zone III resulting in poorer vision. Punnonen and Laatikainen emphasized that blindness could occur in 70% of cases with a zone III laceration, and 20% in cases with a zone I wound.20 However, our research did not yield the same conclusion. This could be due to our perforating wounds being primarily corneal. In our study, visual prognosis was closely tied to wound size. Zhang Y suggested that entry wounds of at least 3 mm significantly contributed to final VA, and wounds larger than 5 mm notably increased the chances of poorer VA.2 Wounds larger than 3 mm constituted 63.5% of our cases.
In our study, RD was observed in 22.01% of eyes with IOFBs. Despite a higher RD incidence post-trauma, our study found no association between RD and visual outcomes. Yaşa21 demonstrated that eyes with RD had lower final VA than those without, although this difference lacked statistical significance. This finding echoed ours. Yang Liu19 suggested that hyphema and vitreous hemorrhage were not significant factors for final VA, as these issues could be effectively treated through surgery. However, macular lesions, which cannot be recovered through surgery, directly impacted visual prognosis in our study, given that the macula is vital for central vision.
The entry of foreign bodies into the eyeball can lead to mechanical damage and toxic effects on eye tissues, raising the likelihood of intraocular infection, retinal necrosis, sympathetic ophthalmitis, and even blindness in severe cases.22 Previous research reported that 26% to 71% of IOFB-affected eyes achieved a final VA of 20/40 or better,23 while our study found such outcomes in 31% of cases. Timely defect repair, IOFB removal, and addressing IOFB complications proved pivotal to prognosis.
Additionally, our study had limitations in terms of a small and retrospective sample size. Therefore, a prospective study aimed at efficient treatment to reduce IOFB incidence and enhance final VA is warranted.
Conclusion
In conclusion, IOFB represents a common and severe ocular injury with the potential for significant visual impairment. In a northern Chinese tertiary eye center, IOFB incidents were most common among the working-age population, especially males. Factors influencing visual prognosis are of utmost importance. Our study highlighted that the length of corneal/scleral wound, maximum IOFB size, initial presenting VA, and macular lesions could impact final visual outcomes. Consequently, there is a need for enhanced education and promotion of eye protection to improve self-awareness of eye health and self-protection. While our study detailed several methods of foreign body removal, IOFB treatment remains complex and challenging, warranting further investigation.
Abbreviations
IOFBs, intraocular foreign bodies; BCVA, best corrected visual acuity; CT, computed tomography; PPV, pars plana vitrectomy; RD, retinal detachment.
Ethics Approval and Consent to Participate
This study was performed in compliance with the principles of Declaration of Helsinki and was approved by the Institutional Ethics Committee of Eye Institute of Shandong First Medical University, Qingdao Eye Hospital of Shandong First Medical University. The informed consent was waived by the Institutional Ethics Committee of Eye Institute of Shandong First Medical University, Qingdao Eye Hospital of Shandong First Medical University considering the retrospective nature of the study. Privacy and data protection: ensure patients’ personal information and data are strictly confidential and will not be abused or leaked.
Acknowledgments
This paper has been uploaded to ResearchSquare as a preprint: https://www.ResearchSquare.com /article/rs-3362708/vl.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Shandong Medical and Health Science and Technology Development Plan Project (202207020553); Natural Science Foundation of Qingdao City (23-2-1-196-zyyd-jch).
Disclosure
The authors declare no competing interests.
References
1. Loporchio D, Mukkamala L, Gorukanti K, et al. Intraocular foreign bodies: a review. Surv Ophthalmol. 2016;61:582–596. doi:10.1016/j.survophthal.2016.03.005
2. Zhang Y, Zhang M, Jiang C, et al. Intraocular Foreign Bodies in China: clinical Characteristics, Prognostic Factors, and Visual Outcomes in 1421 Eyes. Am J Ophthalmol. 2011;152:66–73.e61. doi:10.1016/j.ajo.2011.01.014
3. Duan F, Yuan Z, Liao J, et al. Incidence and Risk Factors of Intraocular Foreign Body-Related Endophthalmitis in Southern China. J Ophthalmol. 2018;2018:1–5. doi:10.1155/2018/8959108
4. Zhang T, Zhuang H, Wang K, et al. Clinical Features and Surgical Outcomes of Posterior Segment Intraocular Foreign Bodies in Children in East China. J Ophthalmol. 2018;2018:5861043. doi:10.1155/2018/5861043
5. Fan Q, Han X, Zhu X, et al. Clinical Characteristics of Intraocular Lens Dislocation in Chinese Han Populations. J Ophthalmol. 2020;2020:1–8. doi:10.1155/2020/8053941
6. Kuhn F, Morris R, Witherspoon CD, et al. The Birmingham Eye Trauma Terminology system(BETT). J Fr Ophthalmol. 2004;27(2):206–210. doi:10.1016/s0181-5512(04)96122-0
7. Li L, Lu H, Ma K, et al. Etiologic Causes and Epidemiological Characteristics of Patients with Intraocular Foreign Bodies: retrospective Analysis of 1340 Cases over Ten Years. J Ophthalmol. 2018;2018:6309638. doi:10.1155/2018/6309638
8. Woodcock MGL, Scott RAH, Huntbach J, et al. Mass and shape as factors in intraocular foreign body injuries. Ophthalmology. 2006;113:2262–2269. doi:10.1016/j.ophtha.2006.06.002
9. Sharma S, Thapa R, Bajimaya S, et al. Clinical characteristics and visual outcome, prognostic factor, visual acuity and globe survival in posterior segment intraocular foreign body at Tilganga Institute of Ophthalmology. Nepal J Ophthalmol. 2018;10:66–72. doi:10.3126/nepjoph.v10i1.21691
10. Zhang Y, Zhang MN, Jiang CH, et al. Endophthalmitis following open globe injury. Br J Ophthalmol. 2010;94:111–114. doi:10.1136/bjo.2009.164913
11. Memon AA, Iqbal MS, Cheema A, et al. Visual outcome and complications after removal of posterior segment intraocular foreign bodies through pars plana approach. J Coll Physicians Surg Pak. 2009;19:436–439.
12. Jonas JB, Knorr HLJ, Budde WM. Prognostic factors in ocular injuries caused by intraocular or retrobulbar foreign bodies. Ophthalmology. 2000;107:823–828. doi:10.1016/s0161-6420(00)00079-8
13. Wani VB, Al Ajmi M, Thalib L, et al. Vitrectomy for posterior segment intraocular foreign bodies: visual results and prognostic factors. Retina. 2003;23:654–660. doi:10.1097/00006982-200310000-00008
14. Zhu L, Shen P, Lu H, et al. Ocular trauma score in siderosis bulbi with retained intraocular foreign body. Medicine. 2015: 94:e1533. doi:10.1097/md.0000000000001533
15. Chiquet C, Zech JC, Denis P, et al. Intraocular foreign bodies. Factors influencing final visual outcome. Acta Ophthalmol Scand. 1999;77:321–325. doi:10.1034/j.1600-0420.1999.770315.x
16. Yang CS, Hsieh MH, Hou TY. Predictive factors of visual outcome in posterior segment intraocular foreign body. J Chin Med Assoc. 2019;82:239–244. doi:10.1097/jcma.0000000000000021
17. Gao Y, Zhang Y, Zhang M, et al. Clinical characteristics and prognostic factors for visual outcome in 669 patients with intraocular foreign bodies. Int J Ophthalmol. 2021;14:759–765. doi:10.18240/ijo.2021.05.18
18. Su Z, Wang Y, Yi Q, et al. Clinical Characteristics and Visual Outcomes in Patients with Intralenticular Foreign Bodies with Self-Sealing Corneal Penetrating Wounds. J Ophthalmol. 2021;2021:6613205. doi:10.1155/2021/6613205
19. Liu Y, Wang S, Li Y, et al. Intraocular foreign bodies: clinical characteristics and prognostic factors influencing visual outcome and globe survival in 373 eyes. J Ophthalmol. 2019;2019:5208092. doi:10.1155/2019/5208092
20. Punnonen E, Laatikainen L. Prognosis of perforating eye injuries with intraocular foreign bodies. Acta Ophthalmol. 1989;67:483–491. doi:10.1111/j.1755-3768.1989.tb04097.x
21. Yaşa D, Erdem ZG, Demircan A, et al. Prognostic value of ocular trauma score for open globe injuries associated with metallic intraocular foreign bodies. BMC Ophthalmol. 2018;18:1–5. doi:10.1186/s12886-018-0874-3
22. Liang Y, Liang S, Liu X, et al. Intraocular Foreign Bodies: clinical Characteristics and Factors Affecting Visual Outcome. J Ophthalmol. 2021;2021:9933403. doi:10.1155/2021/9933403
23. Greven CM, Engelbrecht NE, Slusher MM, et al. Intraocular foreign bodies: management, prognostic factors, and visual outcomes. Ophthalmology. 2000;107:608–612. doi:10.1016/s0161-6420(99)00134-7
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.