")
Back to Journals » Journal of Pain Research » Volume 18
Clinical Effectiveness of Perineural Liposomal Bupivacaine is Not Superior to Bupivacaine Hydrochloride for the Prevention of Postoperative Pain in Orthopedic Surgery: A Systematic Review and Meta-Analysis with Trial Sequential Analysis
Authors Wan M, Liang X, Meng J, Wu H, Xi C
Received 26 March 2025
Accepted for publication 1 July 2025
Published 16 July 2025 Volume 2025:18 Pages 3627—3642
DOI https://doi.org/10.2147/JPR.S525231
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jinlei Li
Meixuan Wan,1 Xuan Liang,1 Jingwen Meng,2 Haiyao Wu,1 Chunhua Xi1
1Department of Anesthesiology, Beijing Tongren Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Operation Center, Beijing Tongren Hospital, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Chunhua Xi, Department of Anesthesiology, Beijing Tongren Hospital, Capital Medical University, 1 Dongjiaominxiang Road, Dongcheng District, Beijing, 100730, People’s Republic of China, Tel +86-10-58268101, Email [email protected]
Background: As a long-lasting local anesthetic, liposomal bupivacaine has become a part of certain multimodal analgesic regimens for acute postoperative pain. The objective of the present meta-analysis was to investigate the efficacy of liposomal bupivacaine in acute pain management after orthopedic surgery through peripheral nerve blocks and compare it with plain bupivacaine.
Methods: The EMBASE, PubMed, Web of Science, Scopus databases, the Cochrane Central Register of Controlled Trials, and the Cochrane Database of Systematic Reviews were searched for randomized controlled trials (RCTs) published in print or online up to 11 October 2024. The primary outcomes were NRS scores and opioid consumption at postoperative 24– 72 hours. A minimum difference of 2.0 points on NRS scores or 30-mg in OME consumption was considered clinically relevant.
Results: A total of 10 RCTs (782 patients) were finally included in the meta-analysis. There were significant differences in the mean NRS scores at postoperative 48 hours (MD = − 0.86, 95% CI: [− 1.19, − 0.45], P < 0.001) and 72 hours (MD = − 0.38, 95% CI: [− 0.54, − 0.21], P < 0.001). As regard to opioid consumption, there were statistical differences at postoperative 48 hours (MD = − 5.51, 95% CI: [− 9.97, − 1.06], P = 0.020) and 72 hours (MD = − 3.62, 95% CI: [− 6.04, − 1.21], P = 0.003). But none of the differences, including NRS scores and opioid consumption, met the prespecified thresholds for clinical relevance. Additional benefits of liposomal bupivacaine over plain bupivacaine were observed only in the nerve block duration (RR = 3.35, 95% CI: [1.92, 5.84], P < 0.001).
Conclusion: The advantages of perineural liposomal bupivacaine over plain bupivacaine in providing analgesia after orthopedic surgery were statistically significant but not clinically relevant. Current evidence suggests that the existing RCTs are insufficient to support the idea that the perineural use of liposomal bupivacaine is clinically worthwhile in pain management after orthopedic surgery compared with plain bupivacaine.
Keywords: orthopedic surgery, liposomal bupivacaine, postoperative pain, peripheral nerve block, systematic review, meta-analysis
Introduction
Orthopedic procedures have increased globally due to several factors, including an aging population, advances in surgical techniques and the introduction of new technologies. For instance, the absolute number of hip fracture surgery increased rapidly between 2012 and 2016,1 and a previous study has indicated that the incidence of hip fractures is expected to increase to more than 1 million annually by 2050 in the USA.2 Meanwhile, the number of knee arthroplasty procedures increased by 32.2% between 2012 and 2018 in France.3 Orthopedic procedures are strongly associated with severe postoperative pain and subsequently significant opioid consumption.4,5 Even arthroscopic rotator cuff repair could give rise to pain that persists from 8 to 16 hours.6 Moderate-to-severe pain has been reported even in foot and ankle surgery, the most severe of which occurring up to 3 days postoperatively.7 Inadequate analgesia would be even expected to develop chronic postsurgical pain lasting up to a year and increase the rate of occurrence of chronic postoperative pain after a year.8 Thus, multimodal analgesia has become one of the effective alternative methods of pain management.9 Peripheral nerve blocks (PNBs) are an important component of multimodal analgesia regimens, especially in orthopedic surgery,10 as regional anesthesia block the nociceptive signal transmission in sensory neurons prior to its start.11 PNBs are commonly used to decrease total and rescue opioid consumption, offer comfortable postoperative care settings, improve analgesic outcomes and shortens hospital length of stay.10,12,13 Both single-shot PNBs and continuous PNBs are effective for postoperative pain. Although continuous PNBs are increasingly used, there are some limitations including infectious risk, local anesthetic systemic toxicity and the requirement for precise catheter placement.14–16 As for the length of duration, single-shot PNBs are shorter than continuous PNBs, which is the main limitation of single-shot approach.17 Researchers found adjuvants, such as dexamethasone, could be added to the local anesthetic to prolong the duration of sense block by 6 to 8 h.18 However, when the analgesic effect of single-shot blocks wears off, it often leads to a phenomenon of rebound pain, which could increase in opioid consumption, hamper patient satisfaction and rehabilitation.19 Chan et al reported that conventional bupivacaine carried a high risk of rebound pain upon discontinuation.20 To address these limitations, extended-release local anesthetics such as liposomal bupivacaine (LB) have emerged as a promising alternative in single-shot PNBs.
Liposomal bupivacaine (LB), encapsulated by lipid-based particle layers and slowly released into the surrounding tissue,21 can provide analgesia lasting up to over 72 h, longer than the duration of the analgesic effect of plain bupivacaine hydrochloride (PB) (<24 hours).22,23 Liposomal bupivacaine was first approved by the Food and Drug Administration (FDA) in 2011 for postoperative pain management in surgical infiltration and transversus abdominis plane block (TAP) at doses up to 266 mg. In 2018, the FDA Anesthetic and Drug Products Advisory Committee authorized the requisition of liposomal bupivacaine for a new indication for interscalene brachial plexus block regimens.24,25 Since then, liposomal bupivacaine has been approved for even more indications, such as field block infiltration, brachial plexus block and femoral nerve block, adductor canal block and sciatic nerve block in the popliteal fossa.26,27 Consequently, the number of published trials focused on perineural liposomal bupivacaine in orthopedic surgery is substantially increasing.
Although previous meta-analyses have concluded that liposomal bupivacaine is not clinically superior to bupivacaine hydrochloride regardless of the regional anesthesia technique used,26,28 no published data are available on the effective of perineural liposomal bupivacaine in orthopedic surgery. Since this meta-analysis exclusively focuses on RCTs evaluating perineural LB in orthopedic procedures to minimize heterogeneity.
The aim of our meta-analysis is to evaluate whether liposomal bupivacaine for peripheral nerve block provides superior efficacy compared to bupivacaine hydrochloride in orthopedic procedures, as demonstrated by high-quality randomized controlled trials (RCTs). We assessed postoperative pain scores and opioid consumption as the primary outcomes and importantly focused on the potential clinical efficacy of liposomal bupivacaine. Our findings may guide clinicians in selecting optimal nerve block agents to balance analgesia efficacy and opioid-sparing effects.
Material and Methods
Study Design and Registration
We searched for RCTs involving orthopedic surgery to evaluate the analgesic effect of liposomal bupivacaine and compare it with standard bupivacaine after a nerve block. This study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist.29 The meta-analysis protocol was registered on 27 October 2024 on the International Prospective Register of Systematic Reviews (PROSPERO; CRD42024600643).
Search Strategy
A detailed literature search was performed on EMBASE, PubMed, Web of Science, Scopus, the Cochrane Central Register of Controlled Trials, and the Cochrane Database of Systematic Reviews to identify eligible studies published in print or online. The search strategy included MeSH and exploded terms related to liposomal bupivacaine, nerve block and postoperative analgesia; the last search was conducted on 11 October 2024. We also searched the reference lists of all the retrieved articles and reviewed them as supplemental trials. We employed the PICOS strategy as follows: P (patients) were defined as adult patients who underwent orthopedic surgery; I (intervention) was defined as peripheral nerve block with LB. C (comparison/control) was defined as peripheral nerve block with PB. O (outcome) was defined as pain reduction, opioid consumption, duration of analgesia, patient satisfaction and adverse events. S (study design) was the only RCTs that satisfied our inclusion criteria. During the actual search, we ignored the specificity of P, C and O to avoid missing relevant studies.
Eligibility Criteria
The inclusion criteria were as follows: 1) adult patients (≥18 years of age); 2) orthopedic surgery; 3) single-injection peripheral nerve block with liposomal bupivacaine and/or plain bupivacaine; 4) a control group consisting of patients treated only with bupivacaine hydrochloride; and 5) a study type of RCT.
The exclusion criteria were as follows: 1) unavailable full text; 2) non-orthopedic surgery; 3) perineural adjuvants other than epinephrine; 4) infiltration techniques and/or field block with liposomal bupivacaine; and 5) continuous nerve block. No limitations on publication language were set.
Study Selection and Data Extraction
Two reviewers (Dr. Wan and Dr. Meng) independently searched the titles and abstracts on 13 October 2024 in Endnote 21. The full-text versions of eligible studies were then retrieved, and any duplicates were removed. The same reviewers evaluated the studies for potential inclusion, and any discrepancies were settled by a third reviewer (Dr. Xi). A pilot-tested extraction form was created by one of the reviewers (Dr. Wan) in Microsoft Excel for Mac, V.16.9. Data from the included studies were subsequently extracted by two independent reviewers (Dr. Wan and Dr. Xi). Any discrepancies in this process were discussed between the two reviewers or resolved by a third reviewer (Dr. Liang) until a consensus was reached. The collected information included the study authors, publication year, sample size, type of nerve block, type of surgery, surgical anesthetic, time of nerve block, dose and volume administered to the control group and intervention group, postoperative multimodal analgesia, primary outcomes, resting and dynamic pain scores, postoperative opioid consumption, liposomal bupivacaine-related adverse effects, duration of nerve block, patient satisfaction, length of hospital stay, functional recovery and quality of life outcomes. To facilitate the quantitative analyses, any median values and their interquartile ranges (IQRs) from the included studies were converted to means and standard deviations (SDs).
Risk of Bias Assessment and GRADE
The risk of bias (RoB) and the Grading of Recommendations Assessment, Development and Evaluation (GRADE) were independently assessed by two reviewers (Dr. Wan and Dr. Wu). The RoB was assessed with the Cochrane Risk of Bias Tool V.2.030 according to five aspects: 1) bias related to the randomization process; 2) bias due to deviations from the intended interventions; 3) bias due to missing outcome data; 4) bias in the measurement of the outcome; and 5) bias in the selection of the reported result. One of the four options can be selected for each of these aspects: “yes” “probably yes” “probably no” “no” and “no information.” For those studies that did not provide a sufficiently detailed methodology, we considered them to have an “unclear risk of bias”. The overall risk of bias was calculated by the system based on the summary of the five different domains. If the study was judged to have a high risk of bias in at least one of these domains, it was considered to have an overall high risk of bias. Any discrepancies in the quality assessment were ultimately resolved by a third reviewer (Dr. Xi).
GRADE was performed with the online Guideline Development Tool (GRADEpro GDT) to assess the quality of outcomes. According to the GRADE system, the quality of evidence was initially classified as high or low on the basis of whether the outcomes were derived from an experimental or observational trial; subsequently, the level of evidence was classified as high, moderate, low, or very low by considering five different factors.31 In accordance with our prespecified criteria, the initial quality was high, because the included studies were all experimental trials.
As liposomal bupivacaine prolongs the duration of regional analgesia (up to 72 hours) over plain bupivacaine,32 the primary outcomes were the mean pain scores according to a numeric rating scale (NRS) ranging from 0 to 10 (no pain to the worst pain imaginable, respectively) from 24 hours to 72 hours postoperatively. To evaluate the analgesic efficacy of the drugs more comprehensively, we also designated the postoperative oral morphine equivalents (OMEs) consumed each day from 24 hours to 72 hours postoperatively as another primary outcome.
The secondary outcomes included the duration of nerve block, incidence of nerve block-related adverse events, patient satisfaction, length of hospital stay, motor function and postoperative quality of recovery. All data related to time were measured in hours.
Statistical Methods
Continuous data, including pain scores and OMEs, are presented as the means ± SDs. The medians and IQRs or ranges were converted to estimated values of the means and SDs if the latter were unavailable from the original articles.33,34 According to the Cochrane handbook, if the mean and 95% confidence interval (CI) were provided, the data were also converted to the mean and SD. Data from graphs were extracted with GetData Graph Digitizer version 2.24. In some cases, unavailable SDs were estimated as the average SD across similar studies.35 We also contacted the authors of the included studies to obtain as much missing but potentially useful original data as possible.
Heterogeneity was assessed according to the P and I2 values,36 in which I2 > 50% indicated significant heterogeneity. For primary outcomes with high heterogeneity, we performed subgroup analysis or excluded one specific study with confounding factors at a time to determine the source of heterogeneity. As different evaluation systems may be used in individual studies, some heterogeneity is expected. Consequently, a random-effects model was used to eliminate the influence of this heterogeneity. If I2 < 50% with low heterogeneity, a fix-effects model could be used. In addition, we conducted sensitivity analyses for the primary outcomes. Leave-one-study-out analysis and Egger’s regression37 were carried out in StataCorp Stata version 18.0 for Mac.
For continuous outcomes, the weighted mean difference (WMD) was used to weigh the effect size for pain scores and OMEs, and statistical pooling was performed using the inverse variance method due to the presence of experimental heterogeneity. For dichotomous outcomes, the risk ratio (RR) was calculated, and statistical pooling was performed using the Mantel–Haenszel random effects model.38 Forest plots were created to visualize and evaluate the analgesic effects of the different studies. All results were depicted as the 95% CI, and a two-tailed P value of <0.05 was considered to indicate statistical significance. In this meta-analysis, calculations and graphics were generated with Review Manager Software for Mac 5.4 (Nordic Cochrane Centre, The Cochrane Collaboration 2020, Copenhagen, Denmark). The risk of publication bias was assessed by examining the results of Egger’s regression test for the primary endpoints.
In addition, the definition of a minimal clinically meaningful change in the pain score can differ in different studies;39–43 thus, a minimum difference of 2.0 points on a 0–10 scale was considered clinically relevant in this meta-analysis. For postoperative opioid consumption, a minimum 30-mg difference in OME consumption was considered clinically relevant.26,28
Trial Sequential Analysis
Trial sequential analysis (TSA) allows quantification of the statistical reliability of the data in the overall meta-analysis and was used here to assess the reliability of the primary outcomes. The strength of available evidence as assessed by TSA can determine the required information size (RIS) for an expected meta-analysis.
TSA was performed using software developed by the Copenhagen Trial Unit, Center for Clinical Intervention Research, Rigshospitalet, Copenhagen, Denmark.44,45 Because the DerSimonian‒Laird (DL) estimator tends to underestimate between-trial variance, the Biggerstaff and Tweedie (BT) random-effects model was applied.46,47 A two-sided α of 0.05 and β of 0.2 with a power of 80% were used to calculate the RIS, and heterogeneity was corrected for variance-based.
Results
Study Characteristics
We identified 2386 publications through a search of the aforementioned databases and 9 publications through manual searches of the reference lists of related literature reviews, for a total of 2395 studies. After removing duplicates and screening based on the titles and abstracts, 169 reports with available full text were assessed for eligibility. Ultimately, ten RCTs5–7,48–54 were included in this systematic review. The flow diagram for study inclusion is shown in Figure 1. A grid depicting the risk of bias assessment is depicted in Figure 2. Five studies were rated as having low overall risks of bias. In particular, two reports noted that their funding was provided by pharmaceutical companies.7,48
 |
Figure 1 PRISMA 2020 Flow Diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses. PRISMA figure adapted from Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. 2021 Mar 29;10(1):89.55 |
 |
Figure 2 Risk of Bias Assessment for Included Studies.5–7,48–54 |
The baseline characteristics of the patients and the main outcomes of the ten included studies are summarized in Table 1 and Table 2, respectively. A total of 782 patients were enrolled, 60.9% (n = 476) of whom were female, and the average age was 58.75 years. Eight of the ten included studies were from the USA,5–7,49–52,54 one was from China,53 and one was from Belgium.48 The types of orthopedic surgery included total shoulder arthroplasty,48,49,51,52 rotator cuff repair,6,48 total knee arthroplasty,50,54 hip arthroscopy,5 distal metaphyseal osteotomy,7 and distal radial fracture fixation.53 The types of peripheral nerve block used included brachial nerve block,6,48,49,51–53 adductor canal block,50,54 fascia iliaca blockade,5 and sciatic nerve block in the popliteal fossa.7 Owing to different operative sites involved, the volume of perineural liposomal or plain bupivacaine varied from 15 to 40 mL. Two doses of liposomal bupivacaine were used: 133 mg or 266 mg. Except for two studies7,50 in which liposomal bupivacaine alone was used in the experimental groups, a mixture of plain and liposomal bupivacaine was administered to the patients. Regarding basic anesthesia, the majority of the included patients underwent general anesthesia, and some studies were designed with field block7,53 or spinal anesthesia54 as background technologies.
 |
Table 1 Characteristics and Analgesic Regiments of Included Studies |
 |
Table 2 Outcomes of Included Studies |
Primary Outcomes
Mean Pain Score at 24 Hours
All ten studies5–7,48–54 included in this meta-analysis (769 patients) reported pain scores 24 hours after surgery. One trial7 failed to be included in statistics because of a different measuring unit. The liposomal bupivacaine group did not have significantly lower pain scores than the control group from 0 to 24 hours (MD = −0.72, 95% CI: [−1.51, 0.06], P = 0.07; GRADE: moderate; Figure 3). The heterogeneity was high, with an I2 of 91%. As shown in Figure 3, pooled weighted mean differences with 95% CIs; diamonds represent effect estimates and lines indicate the confidence intervals. By the method of leave-one-out analysis, we found the sources of heterogeneity from Chan et al,53 excluding this trial (MD = −0.48, 95% CI: [−1.06, 0.09], P = 0.10; I2 = 62%).
 |
Figure 3 Forest plot of mean pain scores after 24 hours.5–7,48–54 |
Mean Pain Score at 48 Hours
Nine studies5–7,48–51,53,54 included in this meta-analysis (744 patients) reported pain scores 48 hours after surgery. One trial7 failed to be included in statistics because of a different measuring unit. The liposomal bupivacaine group had statistically lower pain scores than the control group from 24 to 48 hours (MD = −0.86, 95% CI: [−1.19, −0.45], P < 0.001; GRADE: moderate; Figure 4). The heterogeneity was low, with an I2 of 44%.
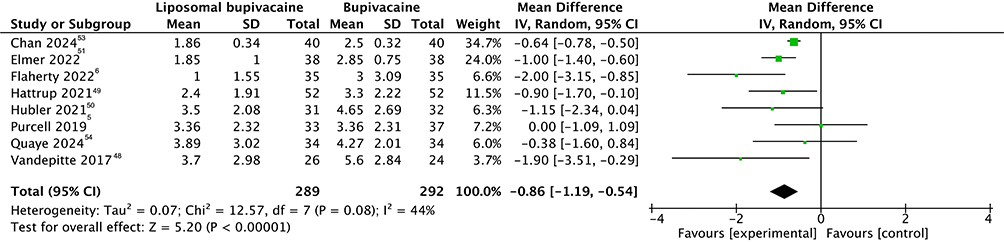 |
Figure 4 Forest plot of mean pain scores after 48 hours.5–7,48–51,53,54 |
Mean Pain Score at 72 Hours
Eight studies5–7,48–51,53 including 676 patients reported pain scores at 72 hours after surgery. One trial7 failed to be included in statistics because of a different measuring unit. Compared with the control group, the liposomal bupivacaine group had statistically lower pain scores from 48 to 72 hours (MD = −0.38, 95% CI: [−0.54, −0.21], P < 0.001; GRADE: moderate; Figure 5). Regrettably, this difference failed to meet the standard of clinical importance. The heterogeneity was low, with an I2 of 4%.
 |
Figure 5 Forest plot of mean pain scores after 72 hours.5–7,48–51,53 |
Opioid Consumption at 24 Hours
Seven trials5–7,48,50,51,54 including 567 patients reported OME consumption from 0 to 24 hours postoperatively. No significant difference was identified between the two groups (MD = −1.50, 95% CI: [−3.65, 0.66], P = 0.17; GRADE: moderate; Figure 6). The heterogeneity was high, with an I2 of 78%. After one study48 that reported industry funding was excluded, statistically significant differences were detected by a fixed-effects model (MD = −2.45, 95% CI: [−3.66, −1.24], P < 0.001, I2 = 46%; GRADE: high). However, this difference was not clinically relevant.
 |
Figure 6 Forest plot of opioid consumption after 24 hours.5–7,48,50,51,54 |
Opioid Consumption at 48 Hours
Seven trials5–7,48,50,51,54 including 566 patients reported OME consumption from 24 to 48 hours postoperatively. The difference between the two groups was significant (MD = −5.51, 95% CI: [−9.97, −1.06], P = 0.02; GRADE: moderate; Figure 7). The heterogeneity was high, with an I2 of 93%. After excluding the study by Vandepitte et al,48 which reported industry funding, patients treated with LB were shown to have consumed significantly less OMEs than those treated with PB according to a fixed-effects model (MD = −5.53, 95% CI: [−6.96, −4.11], P < 0.001, I2 = 50%; GRADE: high). However, this difference was not clinically relevant.
 |
Figure 7 Forest plot of opioid consumption after 48 hours.5–7,48,50,51,54 |
Opioid Consumption at 72 Hours
Seven trials5-7,48–51 including 596 patients reported OME consumption from 48 to 72 hours postoperatively. The difference between the two groups was significant (MD = −3.62, 95% CI: [−6.04, −1.21], P = 0.003; GRADE: moderate; Figure 8). The heterogeneity was high, with an I2 of 78%. After one study that reported industry funding was excluded, notably fewer OMEs were consumed by LB-treated patients than by PB-treated patients when a fixed-effects model was used (MD = −4.16, 95% CI: [−5.39, −2.93], P < 0.001, I2 = 14%; GRADE: high). Regrettably, this difference failed to meet the threshold of clinical importance.
 |
Figure 8 Forest plot of opioid consumption after 72 hours.5–7,48–51 |
Secondary Outcomes
Length of Stay
Four trials5,49,50,54 including 305 patients reported the length of stay, one of which49 was excluded due to missing detailed data. No significant difference was found between the two groups according to a fixed-effects model (MD = −0.32, 95% CI: [−1.51, 0.86], P = 0.59, I2 = 31%; GRADE: moderate).
Patient Satisfaction
Six studies7,48–51,53 (532 patients) involving different reporting tools provided data on patient satisfaction with analgesia. Vandepitte et al48 reported the Overall Benefit of Analgesia Score (OBAS) to assess satisfaction with pain treatment. Patients given liposome bupivacaine reported lower total scores than those given plain bupivacaine, indicating greater benefits from the former (difference, 1.4 ± 0.5; 95% CI, 0.5–2.4). A 10-point scale, with 10 being the highest level of comfort, was used to measure patient satisfaction in three included studies,7,49,50 all of which reported similar scores between the two groups. Chan et al53 also evaluated patient satisfaction with the OBAS and reported that patients given liposomal bupivacaine had significantly lower scores than patients given plain bupivacaine in the first 48 hours.
Duration of Nerve Block
We extracted the duration of sensory block data from three studies5,7,51 involving 309 patients. We defined the outcome as the ratio of thigh numbness reported at postoperative 72 hours. The results of the meta-analysis revealed significant differences between the two groups both when the nerve block duration was treated as a dichotomous5,7 (RR = 3.35, 95% CI: [1.92, 5.84], P < 0.001 I2 = 0; GRADE: moderate) and a continuous variable51 (geometric mean 24.3 ± 0.9 hours vs 39.9 ± 0.6 hours, P < 0.001).
Motor Function
Four studies7,48,50,53 involving 356 patients reported the outcome. Hubler et al50 reported gait velocity through a 10-meter walk test on postoperative day 1 as the primary outcome of the efficacy of LB (0.46 ± 0.32 m/s) versus PB (0.52 ± 0.26 m/s) and found no significant difference between the two groups (P = 0.271). Vandepitte et al,48 Hubler et al50 and Chan et al,53 meanwhile, reported muscle power according to extension strength, but none reported a significant difference between the two groups. Schwartz et al7 assessed the duration of motor block prior to restoration of complete foot movement and similarly did not report significant differences between the groups. Because different assessments were performed for motor function in these studies, these data failed to be analyzed.
Quality of Life Outcomes
Only two studies6,53 reported the results of the quality of recovery (QoR) test. Chan et al53 found no statistically significant difference between the two groups after the first 48 hours postoperatively. However, an improved QoR was reported after 72 hours (114.3 ± 19.0 vs 125.8 ± 15.9) for patients given liposome bupivacaine over plain bupivacaine by Flaherty et al.6
Nerve Block-Related Adverse Effects
Eight studies5–7,48,50–53 with 594 patients reported complications of the nerve block. No significant difference was identified between the two groups (RR = 1.15, 95% CI: [0.82 1.62], P = 0.41, I2 = 29%). Some common adverse effects included nausea and vomiting (LB 16.0% vs PB 20.6%), shortness of breath (LB 6.2% vs PB 3.0%), falling while standing unassisted (LB 5.1% vs PB 1.9%), and dizziness (LB 4.1% vs PB 4.8%). In addition, three studies6,7,48 reported serious adverse events, including symptoms of systemic toxicity and neurological complications. Berg et al52 did not report any adverse events in their trials. No deaths occurred in all included trials.
Sensitivity Analysis and Publication Bias
A sensitivity analysis regarding all primary endpoints was performed. The results, shown in online Supplemental Content 1, indicated robustness to the exclusion of any single study at a time. The risk of publication bias was low for any point-in-time we included (P = 1.00).
TSA
The results of the TSA for the mean pain score at postoperative 24 hours are presented in online supplemental content 2. In this meta-analysis, the 606 included patients did not meet the requisite sample size of 890 patients at postoperative 24 hours. The cumulative Z curve crossed the conventional boundary (Z = 1.96; P = 0.05) but failed to cross the O’Brien–Fleming boundary. The power of the present meta-analysis therefore indicated that more trials are needed to make valid conclusions.
Discussion
This systematic review and meta-analysis of RCTs demonstrated that the efficacy of liposomal bupivacaine significantly differed from that of plain bupivacaine, especially in the first 72 hours postoperatively. However, no clinically relevant differences were found, which aligns with the findings of previous meta-analyses.26,28 The lack of standardization in experimental designs and outcome measurement as well as the exclusion of studies funded by industries or institutions may have contributed to the reported lack of clinical effectiveness for liposomal bupivacaine. Therefore, further large-scale clinical trials are needed to evaluate the effectiveness of liposomal bupivacaine and form the standardized rating indicators including pain scores, patient satisfaction scores and motor function.
Postoperative Pain
The primary outcomes of this meta-analysis demonstrate the statistically greater efficacy of perineural liposomal bupivacaine over plain bupivacaine after postoperative 48 hours, but the difference was not clinically relevant. Similarly, an increasing number of randomized controlled trials have reported that liposomal bupivacaine does not seem to present advantages over plain bupivacaine in terms of postoperative analgesia effects. Besides, no significant reduction in pain scores was observed over the first 72 hours after shoulder arthroplasty. Similar results55 were obtained following the injection of periarticular Exparel compared with plain bupivacaine, which did not demonstrate clinically relevant differences in the visual analog scale (VAS) pain scores for the first 96 hours after knee arthroplasty. Moreover, the use of liposomal bupivacaine alone could lead to worse pain scores early in the postoperative period because the local anesthetic exhibits limited activity.56 Although these trials demonstrated that liposomal bupivacaine is not superior to plain bupivacaine in controlling postoperative pain, it should be noted that the drugs were predominantly administered via infiltration techniques or field block instead of nerve block in the strictest sense. Notably, a triple-blinded pharmacodynamic study57 demonstrated that volunteers receiving plain bupivacaine did not consistently perceive residual blockade, whereas those given liposomal bupivacaine experienced intermittent episodes of sensory loss alternating with normal sensation, potentially indicating incomplete or inconsistent sensory and motor blockade. Moreover, among the published studies and indications, most uses of perineural liposomal bupivacaine in orthopedic surgery involved larger nerves rather than smaller nerves. A potential explanation is that the use of liposomal bupivacaine is characterized by an extended duration of loss of sense and motion, leading to aggravated discomfort and delayed convalescence, which is more notable for smaller peripheral nerves. In addition, we noticed one form of postoperative pain following nerve block resolution is rebound pain, described by a delayed increase in patient-reported pain scores, often accompanied by increased analgesic consumption, corresponding to the resolution of the analgesic effect of single-injection blocks.19 The structure of liposomal bupivacaine allows the steady release of anesthetic medication for up to 72 hours. We also hypothesized that according to existing theories on its functioning, the liposomal bupivacaine used in nerve block could reduce the occurrence of postoperative rebound pain in orthopedic surgery by prolonging the duration of the nerve block, helping decrease opioid rescue and achieve satisfactory pain management. Therefore, the optimal nerve block sites for liposomal bupivacaine, which balance postoperative analgesia with motor function, need to be further explored.
Opioid Consumption
To evaluate the analgesic effect, the opioid consumption was another important outcome. For liposomal bupivacaine, the reduction of postoperative narcotic consumption was considered a potential superiority, especially after postoperative 48 hours. Four included studies7,50,51,54 demonstrated the lower total opioid consumption in the early postoperative period, but all of them failed to meet the clinical threshold of difference. However, five included studies5,6,48,49,53 found the total opioid consumption postoperatively did not statistically differ between two groups. Chan et al53 considered that decreasing pain intensity was insufficient to affect outcomes such as postoperative opioid consumption and quality of recovery, chronic pain, upper limb functional scores, and health-related quality of life scores. Namdari et al58 reported that treated with interscalene brachial plexus blockade, patients administered Exparel significantly required more postoperative narcotics. These differences of results among the included studies can be attributed to several factors, including patient demographics, surgical procedures and anesthetic protocols. For instance, age is an important factor leading to clinical differences in the sensation of postoperative pain. A retrospective cohort study43 reported that older patients were insensitive to pain when performing activities in bed, breathing deeply, coughing, sleeping, and experiencing side effects and severe emotions and were unwilling to receive more treatment, including opioids. Furthermore, the type of surgery is a crucial determinant of pain intensity. Major procedures such as hip arthroplasty or spinal surgery were generally associated with high pain scores,59 probably resulting in more opioid consumption. Given these observations, establishing uniform criteria for patient selection, types of surgery, and outcome measures will be critical in reducing heterogeneity and enhancing the comparability of results. Additional RCTs with large sample sizes are essential to better determine whether perineural liposomal bupivacaine has any clinical effects of postoperative pain improvement in orthopedic surgery.
Nerve Block-Related Adverse Effects
As an important part of secondary outcomes in this meta-analysis, there was no statistical difference between two groups. Only one study6 indicated there were more cases of complications in the liposomal bupivacaine group. For upper extremity surgery, Vandepitte et al,48 Elmer et al51 and Flaherty et al6 reported shortness of breath associated with nerve block in both groups. These complications including shortness of breath, numbness in the affected extremity, and Horner’s syndrome are block-related with and without the addition of LB.60 However, two cases of falls in LB group were reported by Flaherty et al,6 for which additional studies are required to determine whether liposomal bupivacaine contributed. For lower extremity surgery, Purcell et al5 and Hubler et al50 reported falls associated with nerve block in both groups. Xing et al61 also found 22% of patients who received femoral nerve block reported falls compared with 0% in placebo in the first postoperative day. This complication may be due to muscle weakness and numbness, in combination with narcotics of a general anesthetic.62 As for liposomal bupivacaine, it may prolong motor and sense blocks resulting to increase the risk of falls. Therefore, nerve block with or without the addition of LB must be used with caution to decrease the incidence of adverse events.
Economic Problems
According to the secondary outcomes such as length of hospital stay and the duration of nerve block in this meta-analysis, the total cost of hospitalization could not be ignored between two groups. Evaluating the actual clinical importance of liposomal bupivacaine is challenging because of the significant publication bias and that related to industrial fundings. According to McCann et al,24 Pacira Biosciences developed a massive market for Exparel in 2013. The financial report of this company revealed that sales of liposomal bupivacaine increased by one quarter in 2019 over 2018. Our meta-analysis included two studies sponsored by industrial or departmental funding. After these studies were excluded, the degree of statistical heterogeneity was notably decreased. In addition, for the clinical application of new drugs, expenses such as direct costs and health care costs must be considered. Gailey et al63 considered that liposomal bupivacaine utilization could shorten the length of stay and duration of recovery, thus reducing overall hospital expenditures. Critically, the lack of clinical importance of the outcomes for Exparel was ignored, as were the extremely higher per-dose costs associated with liposomal bupivacaine ($334) than with nonliposomal bupivacaine ($3) in the USA. Consequently, future studies should focus on a comparison of the medical expenditures related to liposomal bupivacaine versus plain bupivacaine.
Strengths and Limitations of the Study
First, this is a comprehensive systematic review and meta-analysis of RCTs evaluating the potential clinical value of perineural liposomal bupivacaine. Our inclusion criteria were strict and precise to ensure that the results were sufficiently convincing. Second, for those outcomes with high levels of heterogeneity, we attempted to eliminate the heterogeneity and identify its sources. Third, to draw valuable conclusions and provide future directions in this field, we performed a TSA. The meta-analysis for pain scores at 24 hours was not conclusive because the required sample size was not reached. Therefore, additional RCTs are required in the future.
Our meta-analysis also has several potential limitations. First, owing to the limited number of studies, we failed to perform subgroup analyses including liposomal bupivacaine alone or in combination with bupivacaine hydrochloride, different surgical type and block site. If more RCTs have been included, the subgroup analyses would be more precise. Second, the dosing regimens (eg, 133 mg vs 266 mg) differed across the ten clinical studies because of the type of operation. However, the relatively low heterogeneity undermined this possibility. Third, the disparate multimodal analgesia regimens used in the included studies may have influenced the outcomes of the nerve blocks. Finally, we only assessed the main outcomes over three days after surgery, and additional, longer-term follow-up studies are needed to better assess motor function recovery, chronic pain status, opioid dependence, and health-related quality of life postoperatively.
Conclusion
Current evidence suggests that existing RCTs in patients undergoing orthopedic surgery are insufficient to support the use of liposomal bupivacaine as a clinically meaningful alternative to bupivacaine hydrochloride for postoperative pain management. Although some statistically significant differences were observed in pain scores and opioid consumption, these differences did not meet the thresholds for clinical importance. Overall, liposomal bupivacaine did not demonstrate clinically relevant advantages over bupivacaine hydrochloride in terms of analgesia. Given the high cost, further studies need to specifically consider which types of orthopedic surgery are more suitable for the use of perineural liposomal bupivacaine.
Data Sharing Statement
All data relevant to the study are included in the article or uploaded as Supplementary Materials.
Acknowledgments
Assistance with the study: We gratefully acknowledge the editors at American Journal Experts for their assistance in improving the English language herein.
Funding
The authors have not declared a specific grant for this research from any funding agency in the public and commercial sectors.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Zhang C, Feng J, Wang S, et al. Incidence of and trends in Hip fracture among adults in urban China: a nationwide retrospective cohort study. PLoS Med. 2020;17(8):e1003180. doi:10.1371/journal
2. Brown CA, Starr AZ, Nunley JA. Analysis of past secular trends of Hip fractures and predicted number in the future 2010-2050. J Orthop Trauma. 2012;26(2):117–122. doi:10.1097/BOT.0b013e318219c61a
3. Erivan R, Tardieu A, Villatte G, et al. Knee surgery trends and projections in France from 2008 to 2070. Orthop Traumatol Surg Res. 2020;106(5):893–902. doi:10.1016/j.otsr.2020.02.018
4. Stessel B, Fiddelers AA, Joosten EA, Hoofwijk DMN, Gramke HF, Buhre W. Prevalence and predictors of quality of recovery at home after day surgery. Medicine. 2015;94(39):e1553. doi:10.1097/MD.0000000000001553
5. Purcell RL, Brooks DI, Steelman TJ, et al. Fascia iliaca blockade with the addition of liposomal bupivacaine versus plain bupivacaine for perioperative pain management during hip arthroscopy: a double-blinded prospective randomized control trial. Arthroscopy. 2019;35(9):2608–2616. doi:10.1016/j.arthro.2019.03.056
6. Flaherty JM, Berg AA, Harrison A, et al. Comparing liposomal bupivacaine plus bupivacaine to bupivacaine alone in interscalene blocks for rotator cuff repair surgery: a randomized clinical trial. Reg Anesth Pain Med. 2022;47(5):309–312. doi:10.1136/rapm-2021-103349
7. Schwartz G, Gadsden JC, Gonzales J, et al. A Phase 3 active-controlled trial of liposomal bupivacaine via sciatic nerve block in the popliteal fossa after bunionectomy. J Clin Anesth. 2024;94:111402. doi:10.1016/j.jclinane.2024.111402
8. Remérand F, Godfroid HB, Brilhault J, et al. Chronic pain 1 year after foot surgery: epidemiology and associated factors. Orthop Traumatol Surg Res. 2014;100(7):767–773. doi:10.1016/j.otsr.2014.07.012
9. Kohring JM, Orgain NG. Multimodal analgesia in foot and ankle surgery. Orthop Clin North Am. 2017;48(4):495–505. doi:10.1016/j.ocl.2017.06.005
10. Liu Y, Zeng Y, Zeng J, Li M, Wei W, Shen B. The efficacy of liposomal bupivacaine compared with traditional peri-articular injection for pain control following total knee arthroplasty: an updated meta-analysis of randomized controlled trials. BMC Musculoskelet Disord. 2019;20(1):306. doi:10.1186/s12891-019-2660-7
11. Kehlet H, Wilmore DW. Multimodal strategies to improve surgical outcome. Am J Surg. 2002;183(6):630–641. doi:10.1016/s0002-9610(02)00866-8
12. Dysart SH, Barrington JW, Del Gaizo DJ, Sodhi N, Mont MA. Local infiltration analgesia with liposomal bupivacaine improves early outcomes after total knee arthroplasty: 24-hour data from the PILLAR study. J Arthroplasty. 2019;34(5):882–886.e881. doi:10.1016/j.arth.2018.12.026
13. Ma J, Zhang W, Yao S. Liposomal bupivacaine infiltration versus femoral nerve block for pain control in total knee arthroplasty. A systematic review and meta-analysis. Int J Surg. 2016;36(Pt A):44–55. doi:10.1016/j.ijsu.2016.10.007
14. Capdevila X, Bringuier S, Borgeat A, Riou B. Infectious risk of continuous peripheral nerve blocks. Anesthesiology. 2009;110(1):182–188. doi:10.1097/ALN.0b013e318190bd5b
15. Neal JM, Bernards CM, JFt B, et al. ASRA practice advisory on local anesthetic systemic toxicity. Reg Anesth Pain Med. 2010;35(2):152–161. doi:10.1097/AAP.0b013e3181d22fcd
16. Ilfeld BM. Continuous peripheral nerve blocks: a review of the published evidence. Anesth Analg. 2011;113(4):904–925. doi:10.1213/ANE.0b013e3182285e01
17. Joshi G, Gandhi K, Shah N, Gadsden J, Corman SL. Peripheral nerve blocks in the management of postoperative pain: challenges and opportunities. J Clin Anesth. 2016;35:524–529. doi:10.1016/j.jclinane.2016.08.041
18. Kirkham KR, Jacot-Guillarmod A, Albrecht E. Optimal dose of perineural dexamethasone to prolong analgesia after brachial plexus blockade: a systematic review and meta-analysis. Anesth Analg. 2018;126(1):270–279. doi:10.1213/ANE.0000000000002488
19. Muñoz-Leyva F, Cubillos J, Chin KJ. Managing rebound pain after regional anesthesia. Korean J Anesthesiol. 2020;73(5):372–383. doi:10.4097/kja.20436
20. Chan EY, Fransen M, Sathappan S, Chua NH, Chan YH, Chua N. Comparing the analgesia effects of single-injection and continuous femoral nerve blocks with patient controlled analgesia after total knee arthroplasty. J Arthroplasty. 2013;28(4):608–613. doi:10.1016/j.arth.2012.06.039
21. Bramlett K, Onel E, Viscusi ER, Jones K. A randomized, double-blind, dose-ranging study comparing wound infiltration of DepoFoam bupivacaine, an extended-release liposomal bupivacaine, to bupivacaine HCl for postsurgical analgesia in total knee arthroplasty. Knee. 2012;19(5):530–536. doi:10.1016/j.knee.2011.12.004
22. Bergese SD, Ramamoorthy S, Patou G, Bramlett K, Gorfine SR, Candiotti KA. Efficacy profile of liposome bupivacaine, a novel formulation of bupivacaine for postsurgical analgesia. J Pain Res. 2012;5:107–116. doi:10.2147/JPR.S30861
23. Balocco AL, Van Zundert PGE, SS G, TJ G, Hadzic A. Extended release bupivacaine formulations for postoperative analgesia: an update. Curr Opin Anaesthesiol. 2018;31(5):636–642. doi:10.1097/ACO.0000000000000648
24. McCann ME. Liposomal Bupivacaine. Anesthesiology. 2021;134(2):139–142. doi:10.1097/ALN.0000000000003658
25. Administration FaD. In brief: FDA approves new use of Exparel for nerve block pain relief following shoulder surgeries. 2018. Available from: https://wwwfdagov/news-events/fda-brief/fda-brief-fdaapproves-new-use-exparel-nerve-block-pain-relief-following-shoulder-surgeries.
26. Dinges HC, Wiesmann T, Otremba B, Wulf H, Eberhart LH, Schubert AK. The analgesic efficacy of liposomal bupivacaine compared with bupivacaine hydrochloride for the prevention of postoperative pain: a systematic review and meta-analysis with trial sequential analysis. Reg Anesth Pain Med. 2021;46(6):490–498. doi:10.1136/rapm-2020-102427
27. Pacira Pharmaceuticals, Inc. Bupivacaine Liposome Injectable Suspension (Exparel) Prescribing Information. 2024. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/022496s9lbl.pdf
28. Hussain N, Brull R, Sheehy B, et al. Perineural liposomal bupivacaine is not superior to nonliposomal bupivacaine for peripheral nerve block analgesia. Anesthesiology. 2021;134(2):147–164. doi:10.1097/ALN.0000000000003651
29. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;151(4):264–269,w264. doi:10.1371/journal.pmed.1000097
30. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. doi:10.1136/bmj.l4898
31. Guyatt G, Oxman AD, Akl EA, et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011;64(4):383–394. doi:10.1016/j.jclinepi.2010.04.026
32. Abildgaard JT, Chung AS, Tokish JM, Hattrup SJ. Clinical efficacy of liposomal bupivacaine: a systematic review of prospective, randomized controlled trials in orthopaedic surgery. JBJS Rev. 2019;7(7):e8. doi:10.2106/JBJS.RVW.18.00192
33. Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 2014;14(1):135. doi:10.2106/JBJS.RVW.18.00192
34. Luo D, Wan X, Liu J, Tong T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat Methods Med Res. 2018;27(6):1785–1805. doi:10.1177/0962280216669183
35. TJ HJPT, Chandler J, Cumpston M, Li T, Page MJ, Welch VA. Cochrane handbook for systematic reviews of interventions version 6.5 updated August 2024. Cochrane, 2024 Available from: wwwtrainingcochraneorg/handbook.
36. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539–1558. doi:10.1002/sim.1186
37. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–634. doi:10.1136/bmj.315.7109.629
38. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7(3):177–188. doi:10.1016/0197-2456(86)90046-2
39. Childs JD, Piva SR, Fritz JM. Responsiveness of the numeric pain rating scale in patients with low back pain. Spine. 2005;30(11):1331–1334. doi:10.1097/01.brs.0000164099.92112.29
40. Farrar JT, Young JP Jr, LaMoreaux L, Werth JL, Poole MR. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain. 2001;94(2):149–158. doi:10.1016/S0304-3959(01)00349-9
41. Sutton RM, McDonald EL, Shakked RJ, Fuchs D, Raikin SM. Determination of minimum clinically important difference (MCID) in visual analog scale (VAS) pain and foot and ankle ability measure (FAAM) scores after hallux valgus surgery. Foot Ankle Int. 2019;40(6):687–693. doi:10.1177/1071100719834539
42. Salaffi F, Stancati A, Silvestri CA, Ciapetti A, Grassi W. Minimal clinically important changes in chronic musculoskeletal pain intensity measured on a numerical rating scale. Eur J Pain. 2004;8(4):283–291. doi:10.1016/j.ejpain.2003.09.004
43. van Dijk JFM, Zaslansky R, van Boekel RLM, et al. Postoperative pain and age: a retrospective cohort association study. Anesthesiology. 2021;135(6):1104–1119. doi:10.1097/ALN.0000000000004000
44. DP TK, Wetterslev J, Wetterslev J. Can trial sequential monitoring boundaries reduce spurious inferences from meta-analyses? Int J Epidemiol. 2009;38(1):276–286. doi:10.1093/ije/dyn179
45. TK WJ, Brok J, Brok J, Gluud C. Trial sequential analysis may establish when firm evidence is reached in cumulative meta-analysis. J Clin Epidemiol. 2008;61(1):64–75. doi:10.1016/j.jclinepi.2007.03.013
46. JJ SK, Jonkman JN. A comparison of heterogeneity variance estimators in combining results of studies. Statistics in Medicine. 2007;26(9):1964–1981. doi:10.1002/sim.2688
47. JJ SK. Simple heterogeneity variance estimation for meta-analysis. J Royal Statisti Soc. 2005;54:367–384.
48. Vandepitte C, Kuroda M, Witvrouw R, et al. Addition of liposome bupivacaine to bupivacaine HCL versus bupivacaine HCL alone for interscalene brachial plexus block in patients having major shoulder surgery. Reg Anesth Pain Med. 2017;42(3):334–341. doi:10.1097/AAP.0000000000000560
49. Hattrup SJ, Chung AS, Rosenfeld DM, et al. Liposomal bupivacaine interscalene nerve block in shoulder arthroplasty is not superior to plain bupivacaine: a double-blinded prospective randomized control trial. J Shoulder Elbow Surg. 2021;30(3):587–598. doi:10.1016/j.jse.2020.09.017
50. Hubler CP, Bevil KM, Greiner JJ, Hetzel SJ, Borden SB, Cios HA. Liposomal bupivacaine versus standard bupivacaine in the adductor canal for total knee arthroplasty: a randomized, controlled trial. Orthopedics. 2021;44(4):249–255. doi:10.3928/01477447-20210621-01
51. Elmer DA, Coleman JR, Renwick CM, et al. Comparing bupivacaine alone to liposomal bupivacaine plus bupivacaine in interscalene blocks for total shoulder arthroplasty: a randomized, non-inferiority trial. Reg Anesth Pain Med. 2023;48(1):1–6. doi:10.1136/rapm-2022-103997
52. Berg AA, Flaherty JM, Habeck JM, et al. Evaluation of diaphragmatic function after interscalene block with liposomal bupivacaine: a randomized controlled trial. Anesthesiology. 2022;136(4):531–541. doi:10.1097/ALN.0000000000004118
53. Chan TCW, Wong JSH, Wang F, Fang CX, Yung CS, Wong SSC. Addition of liposomal bupivacaine to standard bupivacaine versus standard bupivacaine alone in the supraclavicular brachial plexus block: a randomized controlled trial. Anesthesiology. 2024;141(4):732–744. doi:10.1097/ALN.0000000000005035
54. Quaye A, McAllister B, Garcia JR, et al. A prospective, randomized trial of liposomal bupivacaine compared to conventional bupivacaine on pain control and postoperative opioid use in adults receiving adductor canal blocks for total knee arthroplasty. Arthroplasty. 2024;6(1):6. doi:10.1186/s42836-023-00226-y
55. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. 2021;10(1):89. doi:10.1186/s13643-021-01626-4
56. Alijanipour P, Tan TL, Matthews CN, et al. Periarticular injection of liposomal bupivacaine offers no benefit over standard bupivacaine in total knee arthroplasty: a prospective, randomized, controlled trial. J Arthroplasty. 2017;32(2):628–634. doi:10.1016/j.arth.2016.07.023
57. Hu D, Onel E, Singla N, Kramer WG, Hadzic A. Pharmacokinetic profile of liposome bupivacaine injection following a single administration at the surgical site. Clin Drug Investig. 2013;33(2):109–115. doi:10.1007/s40261-012-0043-z
58. Zadrazil M, Marhofer P, Opfermann P, et al. Liposomal bupivacaine for peripheral nerve blockade: a randomized, controlled, crossover, triple-blinded pharmacodynamic study in volunteers. Anesthesiology. 2024;141(1):24–31. doi:10.1097/ALN.0000000000004988
59. Namdari S, Nicholson T, Abboud J, Lazarus M, Steinberg D, Williams G. Interscalene block with and without intraoperative local infiltration with liposomal bupivacaine in shoulder arthroplasty: a randomized controlled trial. J Bone Joint Surg Am. 2018;100(16):1373–1378. doi:10.2106/JBJS.17.01416
60. Gerbershagen HJ, Aduckathil S, van Wijck AJ, Peelen LM, Kalkman CJ, Meissner W. Pain intensity on the first day after surgery: a prospective cohort study comparing 179 surgical procedures. Anesthesiology. 2013;118(4):934–944. doi:10.1097/ALN.0b013e31828866b3
61. Hutchins JL, Habeck J, Novaczyk Z, et al. Patient complications after interscalene block: a retrospective comparison of liposomal bupivacaine to nonliposomal bupivacaine. Anesthesiol Res Pract. 2020;2020:6704303. doi:10.1155/2020/6704303
62. Xing JG, Abdallah FW, Brull R, et al. Preoperative femoral nerve block for hip arthroscopy. a randomized, triple-masked controlled trial. Am J Sports Med. 2015;43(11):2680–2687. doi:10.1177/0363546515602468
63. Shin JJ, McCrum CL, Mauro CS, Vyas D. Pain management after hip arthroscopy. systematic review of randomized controlled trials and cohort studies. Am J Sports Med. 2018;46(13):3288–3298. doi:10.1177/0363546517734518
64. Gailey AD, Ostrum RF. The use of liposomal bupivacaine in fracture surgery: a review. J Orthop Surg Res. 2023;18(1):267. doi:10.1186/s13018-023-03583-1
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.