")
Back to Journals » Clinical Ophthalmology » Volume 19
Clinical Evaluation of Faricimab in Real-World Diabetic Macular Edema in India- A Multicenter Observational Study
Authors Chakraborty D , Das S, Maiti A, Sinha TK, Das A, Sheth J , Boral SK , Mondal S, Nandi K
Received 21 October 2024
Accepted for publication 3 January 2025
Published 25 January 2025 Volume 2025:19 Pages 269—277
DOI https://doi.org/10.2147/OPTH.S502033
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Debdulal Chakraborty,1 Sudipta Das,2 Aniruddha Maiti,3 Tushar Kanti Sinha,1 Arnab Das,1 Jay Sheth,4 Subhendu Kumar Boral,1 Soumen Mondal,1 Krishnendu Nandi2
1Disha Eye Hospitals, Kolkata, India; 2Nethralayam Superspeciality Eye Care, Kolkata, India; 3Global Eye Hospitals, Kolkata, India; 4Department of Retina Services, Shantilal Shanghvi Eye Institute (SSEI), Mumbai, India
Correspondence: Debdulal Chakraborty, Department of Vitreo-retinal Services, Disha Eye Hospitals, 88 Ghosh Para Road Barrackpore, Kolkata, West Bengal, 700120, India, Tel +91 33 6636 0000, Email [email protected]
Purpose: To evaluate the efficacy of faricimab in real-world clinical settings in India for treating diabetic macular edema (DME) in treatment-naïve and recalcitrant eyes.
Patients and Methods: This retrospective study involved 39 eyes (16 treatment-naive and 23 recalcitrant) treated with intravitreal faricimab at four centers in India. Patients received three monthly loading doses followed by a pro-re-nata regimen, with outcomes measured for best-corrected visual acuity (BCVA), central macular thickness (CMT), intraretinal fluid (IRF), subretinal fluid (SRF), and hyperreflective foci (HRF).
Results: Significant improvements in BCVA were observed in both treatment-naïve and recalcitrant groups, with greater gains in the naïve group (p< 0.001). Overall, BCVA improved from 0.48 logMAR to 0.27 logMAR (P< 0.001), and 59% of eyes gained more than 10 ETDRS letters and 41% gaining > 15 ETDRS letters. Both groups showed significant reduction in CMT, with the naïve group achieving greater reduction (P< 0.001). The overall CMT reduction was statistically significant at 6 months (P< 0.001). Resolution of IRF and SRF was achieved in both groups, with SRF reducing from 82.1% to 20.5% (P< 0.001) and IRF from 87.2% to 17.9% (P< 0.001). Significant reductions in HRF were also observed across both inner (P< 0.001) and outer retinal layers (P< 0.001). No ocular or systemic adverse events were reported.
Conclusion: Faricimab treatment resulted in significant improvements in visual acuity and anatomical outcomes in both treatment-naïve and recalcitrant DME eyes, highlighting its potential as a valuable therapeutic option in diverse clinical settings. Further real-world studies are warranted to establish long-term efficacy and safety.
Keywords: diabetic macular edema, anti VEGF, faricimab
Introduction
Diabetic macular edema (DME) is a leading cause of vision loss among individuals with diabetic retinopathy, and its prevalence is rising due to the global diabetes epidemic.1,2 DME results from the breakdown of the blood-retinal barrier, leading to leakage of fluid and subsequent thickening of the macula, which impairs central vision.1 Timely and effective treatment is critical for preventing vision loss, with anti-vascular endothelial growth factor (anti-VEGF) therapy being the mainstay of treatment in recent years.3
Currently, several anti-VEGF agents are available for the treatment of DME, including ranibizumab, aflibercept, and bevacizumab.3,4 In recent years, the introduction of faricimab has expanded the options available for the treatment of DME. Faricimab is the first bispecific antibody designed for intraocular use, with a dual mechanism of action targeting both VEGF-A and angiopoietin-2 (Ang-2).5,6 VEGF-A is primarily responsible for increasing vascular permeability and promoting abnormal blood vessel growth, while Ang-2 plays a crucial role in destabilizing blood vessels and promoting inflammation, further exacerbating vascular leakage.5,6 By simultaneously inhibiting VEGF-A and Ang-2, faricimab provides more comprehensive protection against the processes driving DME.5,6 Faricimab received US Food and Drug Administration (FDA) approval for the treatment of DME in early 2022, based on the robust data from the YOSEMITE and RHINE trial.5,6 Faricimab made its entry into the Indian market in January 2024, offering an exciting new option for clinicians treating patients with DME. Its dual-action mechanism, combined with the potential for longer treatment intervals, has made it an appealing choice for both treatment-naive patients and those with recalcitrant disease who have not responded adequately to previous anti-VEGF therapies. In a country like India, where diabetes prevalence is high and the burden of DME is substantial,7 the introduction of faricimab could have a significant impact on patient outcomes.
However, while clinical trials such as YOSEMITE and RHINE have demonstrated the efficacy and safety of faricimab, real-world data is essential to validate these findings in diverse patient populations and clinical settings. India presents a unique healthcare environment, with variations in access to healthcare, treatment adherence, and patient demographics. Understanding how faricimab performs in real-world practice, especially in resource-constrained settings, is crucial for optimizing its use and establishing its role in the DME treatment algorithm in India.
Real-world studies play a critical role in complementing clinical trial data by assessing treatment outcomes in everyday clinical practice.8 They help identify factors influencing treatment response, adherence, and long-term effectiveness, which can vary significantly from the controlled settings of clinical trials.8 Limited real-world data currently exist on faricimab, making such studies particularly valuable.
The CLEAR-DME (Clinical Evaluation of FARicimab In Real-World Diabetic Macular Edema) in India study aims to address this gap by evaluating the clinical outcomes of faricimab in a real-world setting in India, focusing on both treatment-naive and recalcitrant cases of DME.
Materials and Methods
The CLEAR-DME INDIA study was a multi-center, retrospective observational study conducted at four tertiary eye care centers in India. The study adhered to the principles outlined in the Declaration of Helsinki and was approved by the Central Ethics committee at Disha Eye Hospital (ECR/846/Inst/WB/2016/RR-24). Written informed consent was obtained from all participants for treatment and data collection.
Design
A systematic review of medical records was conducted for patients with DME who received faricimab treatment between January 2024 and June 2024. Inclusion criteria encompassed patients aged ≥18 years diagnosed with DME, regardless of type (Type 1 or Type 2 diabetes). Recalcitrant DME was defined as patients who had received at least three anti-VEGF injections in the prior six months but exhibited a central macular thickness (CMT) of >350 μm and a suboptimal reduction in CMT (≤15%) during that time. Patients with other significant vitreoretinal pathologies, prior retinal surgeries, systemic autoimmune diseases, or any significant media opacities that would interfere with examination were excluded.
All eligible patients received intravitreal faricimab (6 mg in 0.05 mL) under sterile conditions following standard protocol. The treatment consisted of three loading doses of faricimab administered at monthly intervals, followed by a pro-re-nata (PRN) regimen, where subsequent injections were given based on clinical and imaging findings. Retreatment criteria included persistent macular edema and/or worsening of visual acuity (loss of ≥5 ETDRS letters). The administration of faricimab was preceded by a detailed discussion regarding potential risks and benefits, allowing patients to make informed decisions regarding their treatment options.
Clinical evaluations were conducted at baseline and at each follow-up visit, which occurred at four weeks, and then every four weekly for a total of 24 weeks. Best corrected visual acuity (BCVA) was assessed using the Early Treatment Diabetic Retinopathy Study (ETDRS) letter score and Snellen’s visual acuity chart, and CMT was measured using spectral-domain optical coherence tomography (SD-OCT) (Cirrus 5000, Carl Zeiss Meditec Inc., Dublin, CA). The presence of intraretinal fluid (IRF) and subretinal fluid (SRF) was also evaluated, alongside the number of hyperreflective foci in both the outer and inner retina.
The primary outcome measures included changes in BCVA (ETDRS letter score and LogMAR BCVA) and CMT over six months. Secondary outcomes involved assessing the resolution of IRF and SRF, along with the changes in the number of hyperreflective foci in the outer and inner retina, and safety.
The Statistical analysis was performed by SPSS 23.0 version. Categorical variables were described by taking percentages (analyzed using Chi Square test). Normality of the continuous data was analyzed using Shapiro Wilk test. Continuous variables were described as mean and variation of each observation from the mean value (Standard deviation; SD) represented as mean ± SD (analyzed using independent t-test) if they followed normal distribution and were described as Median (IQR) if they followed non normal distribution (analyzed using Mann Whitney U-Test). Continuous Paired data was analysed using Paired T test (for normal distribution) and Wilcoxon Signed Rank Test (For non-normal distribution). Paired categorical data was analyzed using Mcnemar test. Variables with a P value of <0.05 were considered as statistically significant.
Results
Study Cohort
A total of 39 eyes of 39 patients were included in the study, with 16 (41.03%) in the treatment-naïve group and 23 (58.97%) in the recalcitrant group. There were no significant differences between the groups in terms of age or gender. The mean age was 57.56 ± 9.58 years in the naïve group and 56.65 ± 6.91 years in the recalcitrant group (P=0.747). Males comprised 62.5% of the naïve group and 82.6% of the recalcitrant group (P=0.264). The recalcitrant group had previously received an average of 9.5 ± 4.76 injections. Over the course of the study, the average number of injections required between 3 to 6 months was 1.87 ± 0.34 in the naïve group and 1.78 ± 0.42 in the recalcitrant group (P=0.456). The total mean injections over the study period were comparable between the groups: 4.87 ± 0.34 for the naïve group and 4.78 ± 0.42 for the recalcitrant group (P=0.456). Table 1 summarizes the baseline characteristics of both groups.
 |
Table 1 Demographic Characteristics of the Study Population |
Best-Corrected Visual Acuity
Table 2 illustrates the changes in logMAR BCVA over time. At baseline, the BCVA for the naive group was 0.43 ± 0.13, while the recalcitrant group was 0.53 ± 0.24, with no significant difference between the two (P=0.149). Significant improvements were observed at all follow-up intervals for both groups (P<0.001). When comparing the two groups, the BCVA improvements were greater in the naïve group at 3 months (p=0.001) and 6 months (P=0.003). The overall BCVA across all participants improved from 0.48 ± 0.21 at baseline to 0.27 ± 0.11 at 6 months (P<0.001).
 |
Table 2 Changes in the Best-Corrected Visual Acuity (BCVA) in the Study Population Through 6 months |
The ETDRS letter scores are presented in Table 3. The naïve group demonstrated a significant increase from a baseline score of 63.81 ± 6.63 to 75 ± 4.47 at 6 months (P<0.001), while the recalcitrant group improved from 58.61 ± 12.33 at baseline to 69.83 ± 5.93 at 6 months (P<0.001). Statistically significant differences were observed between the two groups at 2 months (P=0.023), 3 months (P<0.001), and 6 months (P=0.004). Across the entire cohort, ETDRS scores improved significantly from 60.74 ± 10.59 at baseline to 71.95 ± 5.91 at 6 months (P<0.001). Furthermore, 59% of the study eyes improved by more than 10 ETDRS letters, while 41% improved by more than fifteen ETDRS letters. Table 4 summarizes the baseline characteristics of both groups.
 |
Table 3 Changes in the ETDRS Letter Score in the Study Population Through 6 months |
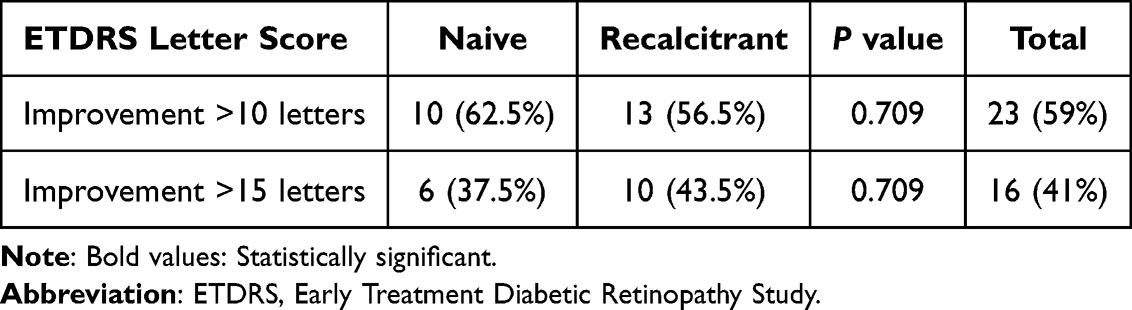 |
Table 4 Proportion of Patients With >10 and >15 ETDRS Letter Improvement |
Central Macular Thickness (CMT)
As shown in Table 5, both groups showed significant reductions in CMT from baseline. In the naïve group, CMT decreased from 424.81 ± 38.6 µm at baseline to 303.87 ± 23.58 µm at 6 months (P<0.001). The recalcitrant group experienced a reduction from 417.13 ± 55.75 µm at baseline to 300.39 ± 39.39 µm at 6 months (P<0.001). There were no significant differences between the two groups at any time point (P=0.732). The overall mean CMT decreased from 420.28 ± 49.02 µm at baseline to 301.82 ± 33.48 µm at 6 months (P<0.001).
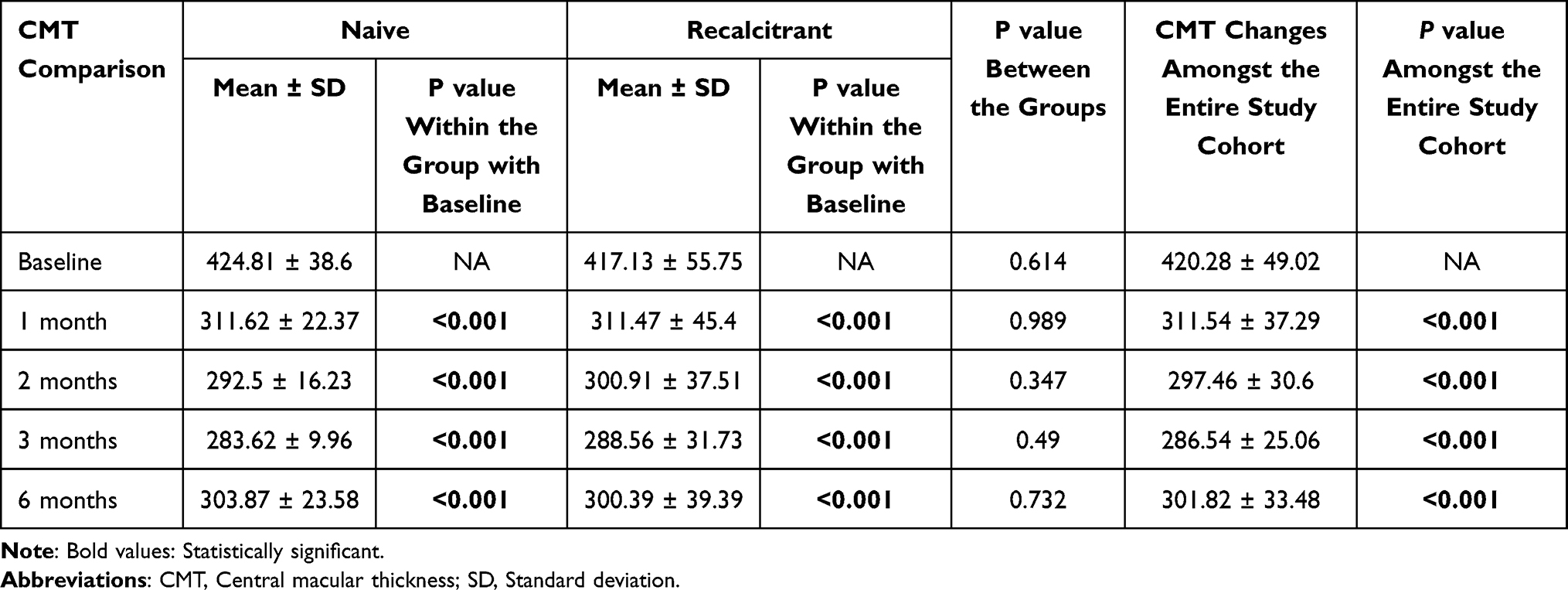 |
Table 5 Changes in the Central Macular Thickness (CMT) in the Study Population Through 6 months |
Fluid Resolution
SRF resolution is summarized in Table 6. At baseline, SRF was present in 75% of naïve patients and 87% of recalcitrant patients (P=0.415). By 6 months, SRF had resolved significantly in both groups (P<0.001), with residual fluid in only 25% of the naïve group and 17.4% of the recalcitrant group (P=0.694). Overall, SRF decreased from 82.1% at baseline to 20.5% at 6 months (P<0.001).
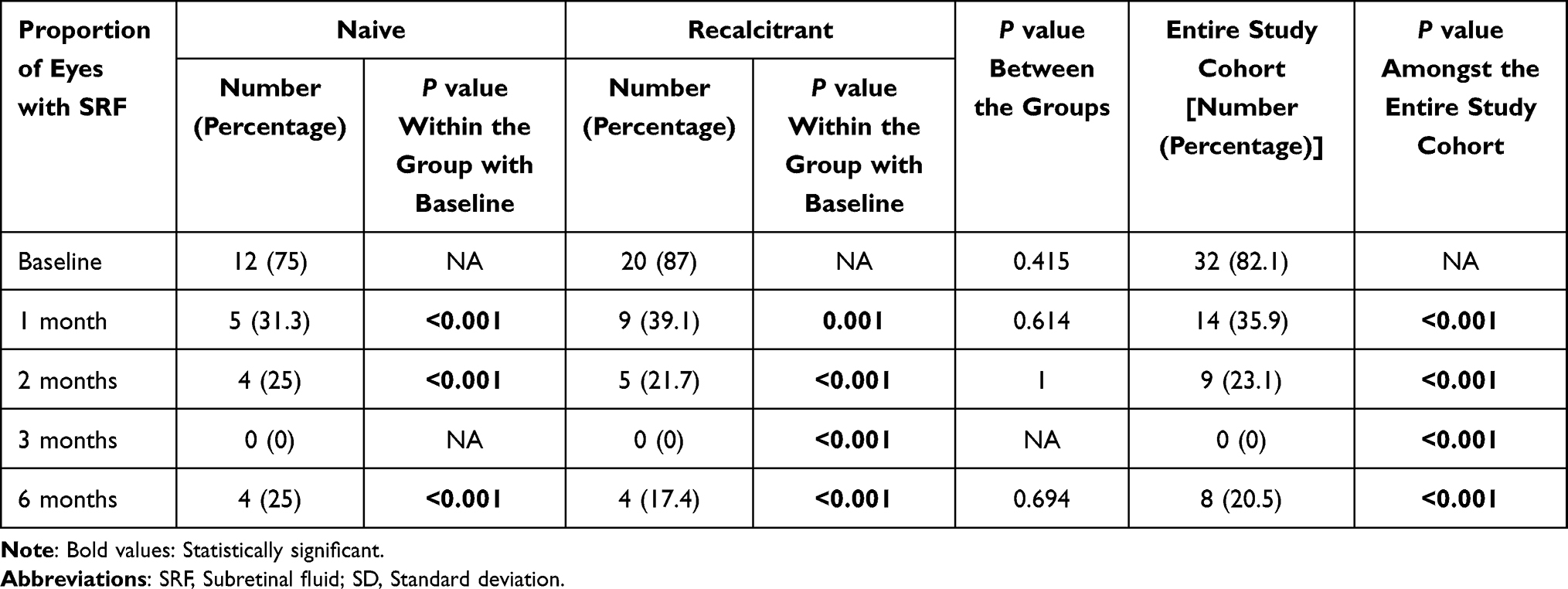 |
Table 6 Changes in the Proportion of Eyes With Resolution of Subretinal Fluid in the Study Population Through 6 months |
Table 7 presents the IRF data. At baseline, 81.3% of naïve patients and 91.3% of recalcitrant patients had IRF (P=0.631). By 6 months, this reduced to 25% in the naïve group and 13% in the recalcitrant group (P=0.415). Across the entire cohort, IRF prevalence decreased from 87.2% at baseline to 17.9% at 6 months (P<0.001).
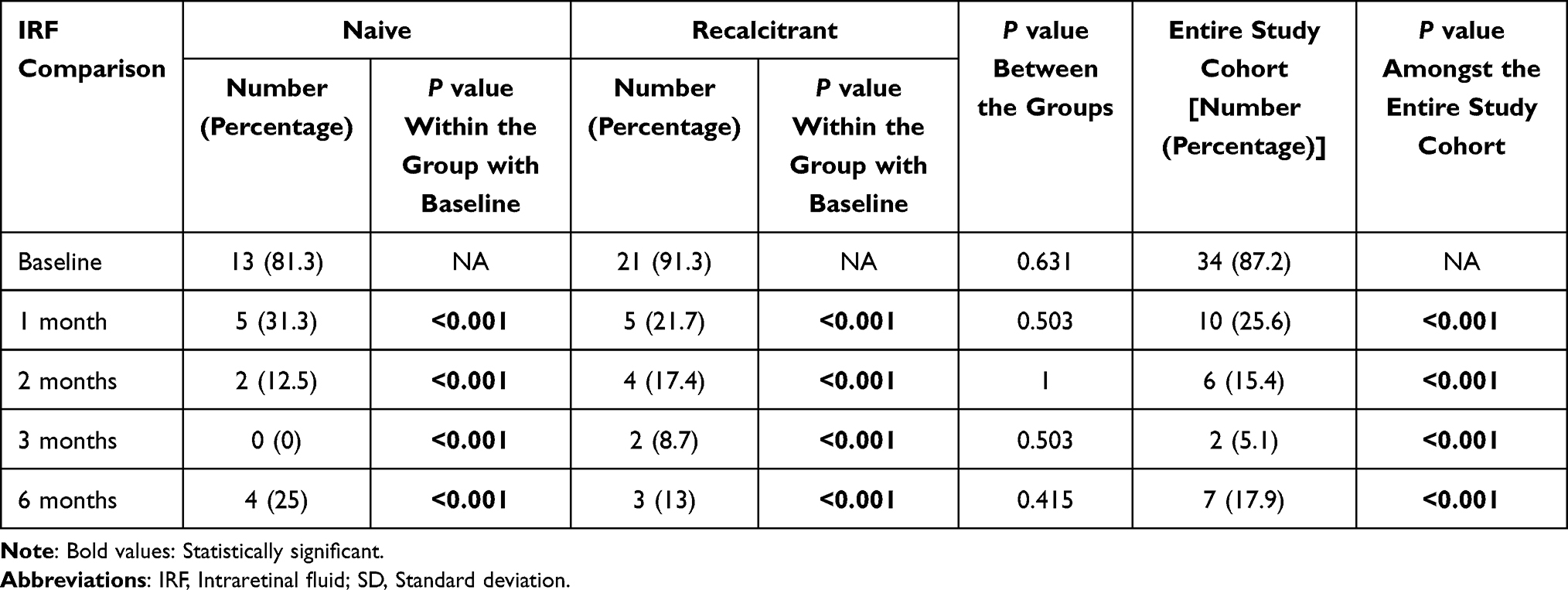 |
Table 7 Changes in the Proportion of Eyes With Resolution of Intraretinal Fluid in the Study Population Through 6 months |
Hyperreflective Foci
The analysis of HRF is displayed in Table 8 and Table 9. At baseline, the naive group had a median HRF inner of 6.5 (IQR 5–9), which significantly decreased to 0 (IQR 0–2) by 6 months (P<0.001). The recalcitrant group started with a median of 10 (IQR 8–13) and decreased to 5 (IQR 4–6) at 6 months (P<0.001). The total median HRF inner improved from 9 (IQR 7–12) at baseline to 4 (IQR 0–6) at the conclusion of the study (P<0.001). For HRF outer, the naive group began with a median of 2 (IQR 2–3) and reduced to 1 (IQR 0–1) (P<0.001), while the recalcitrant group showed a decrease from 4 (IQR 3–5) to 1 (IQR 1–2) (P<0.001) at 6 months. The total median HRF outer improved from 3 (IQR 2–4) at baseline to 1 (IQR 0–2) at 6 months (P<0.001).
 |
Table 8 Changes in the Number of Hyperreflective Foci (HRF) in the Outer Retina in the Study Population Through 6 months |
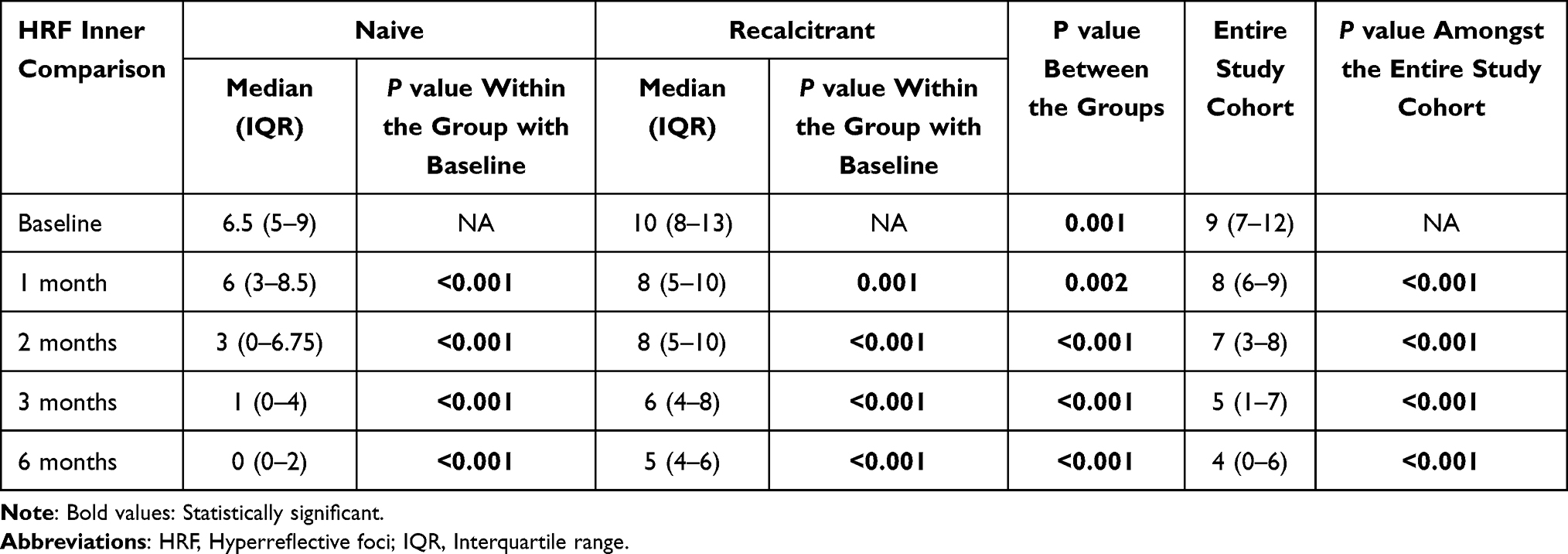 |
Table 9 Changes in the Number of Hyperreflective Foci (HRF) in the Inner Retina in the Study Population Through 6 months |
Safety Analysis
No ocular or systemic adverse events were noted during the study period.
Discussion
The CLEAR-DME INDIA study provides real-world insights into the efficacy of faricimab in treating DME in an Indian cohort. Both the treatment-naive and recalcitrant groups exhibited significant improvements in visual acuity and reductions in CMT over six months. Notably, both IRF and SRF resolved significantly, with similar trends in HRF reduction. The findings align with the current literature about Faricimab’s efficacy while also offering further real-world data pertinent to an Indian demographic.
Anti-VEGF therapies have revolutionized the management of DME by targeting VEGF-A, a key mediator of this vascular permeability and the abnormal growth of blood vessels.1,2 The introduction of anti-VEGF agents such as ranibizumab, bevacizumab, and aflibercept over the past decade has led to improved visual outcomes and reduced macular thickness in a large number of DME patients. These anti-VEGF agents work by neutralizing VEGF-A, thereby reducing vascular permeability and stabilizing blood vessels.1–3 However, some patients exhibit incomplete or suboptimal responses to anti-VEGF therapy, highlighting the need for additional therapeutic approaches. Faricimab, a bispecific antibody, has emerged as a promising option for this population.9–11
Faricimab is the first bispecific antibody designed for intraocular use, targeting both VEGF-A and Ang-2.5,6 VEGF-A is responsible for promoting vascular permeability and abnormal vessel growth, whereas Ang-2 destabilizes blood vessels and promotes inflammation, which exacerbates vascular leakage.5,6 By inhibiting both pathways, faricimab offers a more comprehensive therapeutic approach to managing DME.
Clinical trials like YOSEMITE and RHINE have been instrumental in demonstrating the efficacy and safety of faricimab for DME treatment.5,6 Both trials showed that faricimab provided comparable or superior visual and anatomical outcomes compared to aflibercept, with the added benefit of potentially extending the interval between treatments to 16 weeks in approximately 60% of the patients.5 The dual mechanism of action targeting both VEGF and Ang-2 has been suggested as the reason for this extended durability.5
Our findings are consistent with the outcomes reported in the YOSEMITE and RHINE trials.5 The significant improvements in BCVA and reductions in CMT observed in the CLEAR-DME INDIA study align with the results from the landmark trials, indicating that faricimab is effective across diverse patient populations. In the pooled analysis of the YOSEMITE and RHINE trials, patients receiving faricimab showed significant visual gains over two years, with improvements of +10.8 ETDRS letters in the every-8-week dosing group and +10.4 ETDRS letters in the treat-and-extend (T&E) group.5 These results closely align with the findings of our study, where the mean ETDRS letter score improvement across the entire cohort was + 11.21. Notably, this improvement was consistent between recalcitrant cases (+11.22) and treatment-naïve patients (+11.19), suggesting robust visual gains in both groups.
SRF and IRF are important biomarkers in DME, with persistent fluid often correlating with worse visual outcomes.12,13 In our study, SRF was present in 82.1% of patients at baseline, reducing to 20.5% at six months, while IRF decreased from 87.2% to 17.9%. These findings suggest that faricimab is highly effective in resolving both types of fluid, even in recalcitrant cases where previous anti-VEGF therapy had failed. These findings are consistent with those reported by Rush et al,14 who observed significant visual improvements, resolution of fluid, and reductions in CMT at 12 months in patients with aflibercept-resistant DME after switching to faricimab therapy.
Our findings regarding HRF are also noteworthy. HRF are believed to be associated with retinal inflammation and may predict a poor visual prognosis in DME.14 We observed a significant reduction in both inner and outer retinal HRF, particularly in treatment-naïve patients. This aspect has not been extensively reported in previous trials, making our study one of the few to explore the effect of faricimab on HRF. This reduction in HRF likely reflects faricimab’s dual mechanism of action, targeting both VEGF-A and Ang-2 to reduce vascular leakage and inflammation. This comprehensive analysis of fluid and HRF highlights the broader anti-inflammatory effects of faricimab, adding to the growing body of evidence supporting its use in DME.
In the present study, no occurrences of intraocular inflammation (IOI) or any other ocular or systemic complications were observed. These findings align with those reported in the YOSEMITE and RHINE trials, which similarly noted a low incidence of IOI, ranging from 1% to 2%.5
Despite the promising results, our study has several limitations. The sample size was relatively small, with only 39 eyes included, which may limit the generalizability of our findings. Additionally, the short follow-up period of 6 months does not allow for an assessment of long-term outcomes, including the sustainability of the visual and anatomical improvements observed. Another limitation is the reliance on a PRN dosing regimen, which could result in variability in treatment intervals and outcomes. Furthermore, the retrospective study design and lack of a comparator group limits the ability to directly assess the superiority or inferiority of Faricimab relative to the current standard treatment protocols for DME. It is also important to note that our study was not powered for a safety analysis; the focus was to report on the incidence of IOI, a key safety concern with newer intravitreal therapies. Future trials with larger sample sizes, extended follow-up periods, and inclusion of comparator groups are warranted to validate and expand upon our findings.
Despite these limitations, our study has several strengths. It is the first real-world evaluation of faricimab in an Indian population, providing valuable insights into how this new therapy performs outside the controlled environment of clinical trials. The inclusion of recalcitrant cases provides valuable insights into faricimab’s efficacy in patients unresponsive to prior anti-VEGF therapies. This aspect of the study enhances its clinical significance, as recalcitrant patients often pose greater therapeutic challenges, representing a subgroup with limited treatment options and a critical need for alternative approaches. Our detailed analysis of fluid data and HRF is another strength, offering a more comprehensive understanding of faricimab’s effects on DME. Finally, the study provides real-world data on the safety of faricimab, with no significant adverse events reported during the six-month follow-up period.
Conclusion
The CLEAR-DME INDIA study demonstrates that faricimab is an effective and safe treatment for DME in a real-world Indian population. Both treatment-naive and recalcitrant patients showed significant improvements in BCVA and reductions in CMT, along with high rates of fluid resolution. The reduction in HRF suggests that faricimab may have additional anti-inflammatory benefits, contributing to its longer treatment intervals.
While our results are consistent with clinical trial data, the real-world setting provides additional insights into how faricimab performs in diverse populations with different healthcare challenges. Further studies with larger sample sizes and longer follow-up periods are needed to confirm these findings and explore the potential for faricimab to improve long-term outcomes in DME management.
Consent to Participate
The authors confirm that all research participants provided informed consent for involvement in this study.
Acknowledgments
Dr Debasish Bhattacharya MS, Chairman Disha Eye Hospital, Kolkata, India
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gupta N, Mansoor S, Sharma A, et al. Diabetic retinopathy and VEGF. Open Ophthalmol J. 2013;7(1):4–10. doi:10.2174/1874364101307010004
2. Sun H, Saeedi P, Karuranga S, et al. IDF Diabetes Atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabet Res Clin Pract. 2023;204:110945. doi:10.1016/j.diabres.2023.110945
3. Chakraborty D, Sheth JU, Boral S, Sinha TK. Off-label intravitreal brolucizumab for recalcitrant diabetic macular edema: a real-world case series. Am J Ophthalmol Case Rep. 2021;24:101197. doi:10.1016/j.ajoc.2021.101197
4. Chakraborty D, Sharma A, Mondal S, et al. Brolucizumab versus aflibercept for recalcitrant diabetic macular edema in Indian real-world scenario - The BRADIR study. Am J Ophthalmol Case Rep. 2024;36:102152. doi:10.1016/j.ajoc.2024.102152
5. Wykoff CC, Abreu F, Adamis AP, et al. Efficacy, durability, and safety of intravitreal faricimab with extended dosing up to every 16 weeks in patients with diabetic macular oedema (YOSEMITE and RHINE): two randomised, double-masked, Phase 3 trials. Lancet. 2022;399(10326):741–755. doi:10.1016/S0140-6736(22)00018-6
6. Pradeepa R, Mohan V. Epidemiology of type 2 diabetes in India. Indian J Ophthalmol. 2021;69(11):2932–2938. doi:10.4103/ijo.IJO_1627_21
7. Kim HS, Lee S, Kim JH. Real-world evidence versus randomized controlled trial: clinical research based on electronic medical records. J Korean Med Sci. 2018;33(34):e213. doi:10.3346/jkms.2018.33.e213
8. Agostini H, Abreu F, Baumal CR, et al. Faricimab for neovascular age-related macular degeneration and diabetic macular edema: from preclinical studies to phase 3 outcomes. Graefes Arch Clin Exp Ophthalmol. 2024;262(11):3437–3451. doi:10.1007/s00417-024-06531-9
9. Penha FM, Masud M, Khanani ZA, et al. Review of real-world evidence of dual inhibition of VEGF-A and ANG-2 with faricimab in NAMD and DME. Int J Retina Vitreous. 2024;10(1):5. doi:10.1186/s40942-024-00525-9
10. Liberski S, Wichrowska M, Kocięcki J. Aflibercept versus faricimab in the treatment of neovascular age-related macular degeneration and diabetic macular edema: a review. Int J mol Sci. 2022;23(16):9424. doi:10.3390/ijms23169424
11. Kim JS, Lee S, Kim JY, Seo EJ, Chae JB, Kim DY. Visual/anatomical outcome of diabetic macular edema patients lost to follow-up for more than 1 year. Sci Rep. 2021;11(1):18353. doi:10.1038/s41598-021-97644-2
12. Khoramnia R, Nguyen QD, Kertes PJ, et al. Exploring the role of retinal fluid as a biomarker for the management of diabetic macular oedema. Eye. 2024;38(1):54–60. doi:10.1038/s41433-023-02637-2
13. Rush RB, Rush SW. Faricimab for treatment-resistant diabetic macular edema. Clin Ophthalmol. 2022;16:2797–2801. doi:10.2147/OPTH.S381503
14. Arthi M, Sindal MD, Rashmita R. Hyperreflective foci as biomarkers for inflammation in diabetic macular edema: retrospective analysis of treatment naïve eyes from south India. Indian J Ophthalmol. 2021;69(5):1197–1202. doi:10.4103/ijo.IJO_2627_20
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Faricimab for Treatment-Resistant Diabetic Macular Edema
Rush RB, Rush SW
Clinical Ophthalmology 2022, 16:2797-2801
Published Date: 24 August 2022
One Year Results of Faricimab for Aflibercept-Resistant Diabetic Macular Edema
Rush RB
Clinical Ophthalmology 2023, 17:2397-2403
Published Date: 16 August 2023
Faricimab Outcomes in Chorioretinal Disorders: Indian Real-World Analysis (FOCUS Study)
Agrawal V, Gupta A, Agrawal V, Sheth JU
Clinical Ophthalmology 2025, 19:1855-1862
Published Date: 12 June 2025