")
Back to Journals » Journal of Inflammation Research » Volume 17
Clinical Features and Electroencephalogram Analysis of Brain Network Functional Connectivity in Anti-Leucine-Rich Glioma-Inactivated 1 Antibody Encephalitis
Authors Guo X, Shi H, Sun Y, Xing Y, Guo X, Shen Z, Zheng M, Zhang Y , Jia Y, Li Y, Bao J, Tian S
Received 15 August 2024
Accepted for publication 24 October 2024
Published 29 October 2024 Volume 2024:17 Pages 7881—7891
DOI https://doi.org/10.2147/JIR.S485190
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Xiaosu Guo,1– 4,* Huimin Shi,1,2,* Yuteng Sun,1 Yuan Xing,1– 3 Xin Guo,1– 3 Zhiyuan Shen,1– 3 Mengyi Zheng,1 Yaxin Zhang,1 Yicun Jia,1 Ye Li,1 Junqiang Bao,1,2 Shujuan Tian1– 3
1Department of Neurology, The First Hospital of Hebei Medical University, Shijiazhuang, Hebei, People’s Republic of China; 2Department of Neurology, Hebei Hospital, Xuanwu Hospital, Capital Medical University, Shijiazhuang, Hebei, People’s Republic of China; 3Neuromedical Technology Innovation Center of Hebei Province, Shijiazhuang, Hebei, People’s Republic of China; 4Brain Aging and Cognitive Neuroscience Laboratory of Hebei Province, Shijiazhuang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shujuan Tian; Junqiang Bao, Department of Neurology, The First hospital of Hebei Medical University, Shijiazhuang, Hebei, 050030, People’s Republic of China, Tel +86-0311-87156309, Email [email protected]; [email protected]
Purpose: To summarize the clinical manifestations, laboratory findings, and magnetic resonance imaging (MRI) characteristics of anti-leucine-rich glioma-inactivated 1 (LGI1) antibody encephalitis (anti-LGI1 antibody encephalitis) and explore the electroencephalogram (EEG) features.
Patients and Methods: We retrospectively analyzed the medical history of 16 patients diagnosed with anti-LGI1 antibody encephalitis at the First Hospital of Hebei Medical University from 2021 to 2023. EEGs of patients with anti-LGI1 antibody encephalitis and healthy individuals were analyzed. Based on Video-EEG signal analysis of EEG δ, θ, α, β frequency bands, weighted phase lag index values were calculated to form brain network matrices, studying differences in coherence between brain regions of patients with anti-LGI1 antibody encephalitis and healthy individuals.
Results: Patients with anti-LGI1 antibody encephalitis often presented with subacute onset seizures and cognitive decline. Routine test of cerebrospinal fluid was mostly normal. Serum testing revealed hyponatremia in 62.50% of patients, along with positive serum antinuclear antibodies, decreased vitamin B12, and abnormal cytokines such as interleukin-6. Head MRI revealed abnormal lesions related to the disease in seven cases (43.75%), mainly located in the unilateral or bilateral frontal and temporal lobes of the hippocampus. The EEG mainly showed generalized and focal slow waves, sometimes with focal discharges. Brain network functional connectivity analysis found a significant weakening of functional connections in the frontal-temporal lobe in the δ and β frequency bands. Intravenous pulse corticosteroids and intravenous immunoglobulin are first-line immunotherapies for anti-LGI1 antibody-related encephalitis. The disease recovery and cognitive decline improved in most patients.
Conclusion: Anti-LGI1 antibody encephalitis is characterized by seizures and cognitive dysfunction. Serum may show abnormalities in immune indicators such as cytokines. Head MRI mainly reveals abnormal signals in the frontal-temporal lobes and the hippocampus. EEG brain network connectivity analysis reveals characteristic weakening of functional connections in the frontal-temporal lobe in the δ and β frequency bands.
Keywords: anti-LGI1 antibody encephalitis, epilepsy, electroencephalogram, brain network functional connectivity, immunotherapy
Introduction
Anti-leucine-rich glioma-inactivated 1 (LGI1) antibody encephalitis is an autoimmune disease mediated by anti-LGI1 antibodies. In 2010, Irani et al1 first identified a group of target antigens of non-neoplastic autoimmune encephalitis, mainly manifested by limbic system involvement, as the LGI1 protein, which opened the prelude to the study of this type of encephalitis. Anti- LGI1 antibody encephalitis is one of the most common borderline encephalitis, and its main clinical manifestations include Facio brachial dystonic seizure (FBDS), other forms of epilepsy, decreased proximal memory, psychobehavioral abnormalities, sleep disorders, and hyponatremia.2 Unlike anti-NMDA receptor encephalitis which is associated with tumors, anti-LGI1 antibody encephalitis is rarely associated with tumors.3,4 In this study, the clinical manifestations, laboratory tests, imaging, electroencephalogram (EEG) features, immunotherapy, and prognosis of patients with anti-LGI1 antibody encephalitis were retrospectively analyzed with an aim to assist in the early diagnosis and treatment of the disease.
Materials and Methods
General Information
Sixteen patients with autoimmune encephalitis who were diagnosed with anti-LGI1 antibody positivity at the First Hospital of Hebei Medical University from May 2020 to May 2023 were selected. The study passed the review of the Ethics committee of the First Hospital of Hebei Medical University. Prior to the start of the study, we obtained informed consent from these patients. The study complied with the Declaration of Helsinki. All 16 patients met the diagnostic criteria for autoimmune encephalitis published by Lancet Neurol in 2016 and the Expert Consensus on Diagnosis and Treatment of Autoimmune encephalitis in China (2022 edition).5,6 The diagnostic criteria for definite anti-LGI1 antibody-associated encephalitis included the following four criteria: (1) acute or subacute onset, with limbic system symptoms such as seizures, near memory loss, mental and behavioral abnormalities, or FBDS. (2) Abnormalities in at least one of the following auxiliary examination items: increased cerebrospinal fluid white blood cell count (>5 × 106/L), cerebrospinal fluid cytology showing a lymphocyte reaction or specific oligoclonal zone positivity. Head magnetic resonance imaging (MRI) revealing T2WI or FLAIR imaging abnormal signals in the limbic system or PET/CT showing hypermetabolism in the limbic system and basal ganglia. (3) The presence of anti-LGI1 antibodies in the cerebrospinal fluid or serum, determined by indirect immunofluorescence based on a cell-substrate assay, which is the main diagnostic condition. (4) Exclusion of other causes, such as infection, metabolism, tumors, or genetic causes. (5) Relapse is defined as the recurrence of central nervous system symptoms when clinical symptoms improve for the first time when new central nervous system symptoms appear after the disease has been stable for at least 2 months, or when clinical symptoms tend to improve after immunotherapy.7
Among the 16 patients with anti-LGI1 antibody encephalitis, there were 10 males and 6 females, with a male-to-female ratio of 1.67:1. The average age of onset was 60.50 ± 3.47 years, ranging from 33 to 81 years. The time from onset to admission was 3–180 days, with a median of 28.5 days. One patient had a history of pre-infection. None of the 16 patients had any other autoimmune diseases.
Methods
Baseline data, such as the age and sex of 16 patients, were collected. The clinical symptoms of all patients, including clinical manifestations, auxiliary examinations, treatment plans, and disease outcomes, were evaluated by an attending physician in the Department of Neurology. Case data were retrospectively analyzed.
EEG data of 10 patients and 10 healthy individuals matching their age and sex were collected using a 32-channel PN-NET EEG system (Beijing Yunshen Technology Co., Ltd. Beijing, China). The patients remained quiet, closed their eyes, relaxed, and reduced blinking, eye movements, and limb movements as much as possible. Five minutes of continuous unspaced resting EEG data with eyes closed were collected. The original EEG data were exported in EDF format, and EEG preprocessing was performed using the EEGLAB toolbox in MATLAB (Natick, MathWorks, MA, USA). Non-relevant electrodes, such as the oculoelectrogram and myoelectrogram, were deleted, the average reference of the entire brain was retrieved, and the EEG waves were filtered using a 0.5–50 hz band. The EEG data were divided into segments every 2 s, and artifacts such as blinking, head movement, and myoelectric artifacts were removed. Data segments with absolute voltage amplitude greater than 100 μV were also removed. Weighted phase lag index (WPLI) brain network matrix was established based on EEG signals: five main bands of EEG were defined: δ band: 0.5–4 hz, θ band: 4–8 hz, α band: 8–12 hz, β band: 12–30 hz, and γ band: 30–50 hz. Vinck et al8 constructed a functional brain network by calculating (WPLI), which measures the strength of the phase coupling between two signals. The WPLI considers the statistical properties of the signal phase difference, avoiding the sensitivity of traditional coherence indicators, such as the PLV, to volume conduction effects.
The specific calculation steps are as follows. When calculating the WPLI, the EEG signal is first transformed by a Fourier transform to convert the time-domain signal into a frequency-domain signal. This allows the amplitude and phase information of the signal to be obtained at each frequency point. The phase difference is then calculated, and for the two signals x(t) and y(t), the phase difference Δϕ(t, f) at the frequency f can be calculated using the formula Δϕx(t, f) = ϕx(t, f) -ϕ y(t, f), where ϕx(t, f) and ϕy(t, f) represent the phase of the signals x(t) and y(t) at time t and frequency f, respectively. The next step is to convert the phase difference into a binary positive or negative value, that is, to take the sinusoidal sign of the phase difference Δϕ(t, f) to represent the positive or negative direction of the phase difference. Finally, the WPLI was calculated by considering the average values in the positive and negative directions of the phase difference. The specific formula is as follows:  (N indicates the number of phase differences, and sign (Δϕ(tn, f)) indicates the positive or negative direction of the phase difference). Calculated WPLI values were converted into a brain network matrix. Each value in the matrix represents the degree of coherence between the corresponding brain regions, with colors from blue to yellow representing the strength of the connection.
(N indicates the number of phase differences, and sign (Δϕ(tn, f)) indicates the positive or negative direction of the phase difference). Calculated WPLI values were converted into a brain network matrix. Each value in the matrix represents the degree of coherence between the corresponding brain regions, with colors from blue to yellow representing the strength of the connection.
Statistical Methods
SPSS 27.0 statistical software was used for the analysis. Normally distributed data were expressed as mean ± standard deviation, and the two-sample t-test was used for comparison between the two groups. The skewed distribution data were expressed as median (interquartile distance), and the non-parametric rank sum test was used for comparison between groups. For the EEG data, the MATLAB toolbox was used for statistical analysis, and a paired sample t-test was used. Finally, the WPLI value was corrected by FDR, and P < 0.05 after the correction was considered statistically significant.
Results
Clinical Manifestations
In this study, there were 10 males and 6 females among the 16 patients with anti-LGI1 antibody encephalitis, with an average age of 60.50 ± 3.47 years. There were 11 patients with subacute onset, 4 with acute onset, and 1 with chronic onset. Epilepsy alone was the first symptom in eight patients (50.00%), and cognitive decline, such as slow reactions and memory loss, in two patients (12.50%). Two patients (12.50%) had both epilepsy and cognitive decline. Two patients (12.50%) had abnormal mental behaviors. Dizziness was the first symptom in two patients (12.50%). Among the 16 patients, 9 (56.25%) had cognitive decline, such as slow reaction and memory decline, and 9 (56.25%) had sleep disorders.
Laboratory Indicators
Detection of Cerebrospinal Fluid
Among the 16 patients, 14 had normal cerebrospinal fluid pressure, all between 80 and 180 mmH2O, and 2 patients had slightly elevated cerebrospinal fluid pressure. In all 16 patients (100%), cerebrospinal fluid (CSF) white blood cell counts were normal, CSF protein was increased in two patients (12.50%), CSF chloride was decreased in one patient (6.25%), and no obvious abnormalities were found in routine and biochemical analyses of the brain and spine of the remaining patients. CSF cytology was performed in 13 patients; 9 showed no obvious abnormality, 2 showed a neutrophil reaction with a large number of red blood cells, 1 showed a lymphocyte reaction, and 1 showed 57 lymphocytes and 10 monocytes.
In this study, serum and CSF anti-LGI1 antibodies were detected at the time of diagnosis in 16 patients. Among them, seven patients (43.75%) were positive for anti-LGI1 antibodies in the blood and CSF, and five patients (31.25%) were positive only for serum anti-LGI1 antibodies, of which one patient (6.25%) was suspected to be positive for CSF anti-LGI1 antibodies. CSF was negative in four patients (25.00%). Other serum or CSF anti-neuronal surface antigen antibodies: Anti-nmdar, anti-alpha-amino-3-hydroxyl-5-methyl-4-isozolazopropanic acid receptors 1 and 2, anti-gamma-amino butyric acid B-type receptor, anti-glutamate decarboxylase 65, anti-contact protein-related proteins 2 antibodies and para-tumor syndrome antibody profiles, including anti-RI, anti-HU, anti-Yo, anti-Amphiphysin, anti-MA2, anti-collapse response regulatory protein antibodies were negative. Additionally, 10 patients underwent second-generation sequencing for pathogenic microorganisms in the CSF, all of which tested negative.
Serological Indices
Among the 16 patients, there were no obvious abnormalities in liver, kidney, or thyroid function. However, 10 patients (62.50%) had hyponatremia, including 7 with mild hyponatremia and 3 with severe hyponatremia. Antinuclear antibody, ANCA, and ENA antibody profiles were detected in 12 patients, among whom, 5 were antinuclear antibody-positive, 3 were anti-mitochondrial M2 antibody-positive, and 1 was anti-ribosomal P protein antibody-positive; no significant abnormalities were found in the rest. Twelve patients were tested for anemia; ferritin and folate levels were normal, but vitamin B12 (VitB12) levels were decreased in five patients. Serum cytokines were measured in 13 patients, including 5 with elevated interleukin-6 (IL-6), 3 with elevated interleukin-10 (IL-10), and 3 with elevated Interleukin-8 (IL-8). Interleukin-4 (IL-4) was increased in one patient, interleukin-12P70 (IL-12P70) was increased in one patient, tumor necrosis factor α was increased in one patient, and tumor necrosis factor α was decreased in one patient. Twelve patients underwent triglyceride and cholesterol examinations, all of which were normal, and two patients had decreased high-density lipoprotein levels.
Tumor Screening
Fourteen patients underwent chest CT examination, of which twelve (85.71%) had small nodules in the lung lobes requiring dynamic observation, and two had inflammatory lesions. Total abdominal CT examinations were performed in 11 patients, revealing 4 patients with low-density shadows in the liver, 1 with hepatic cystic lesions combined with low-density lesions in the kidney, 1 with transverse colon wall thickening, 1 with spleen enlargement, 1 with accessory splenic nodules, 1 with kidney space-occupying lesions, and 2 with no obvious abnormalities. Two patients underwent FDG-PET examination, of which, one patient showed abnormally high metabolism in the caudate nucleus, lenticular nucleus, temporal lobe, right thalamus, and insular lobe, which was consistent with the metabolic pattern of autoimmune encephalitis, and one patient had splenomegaly. Fourteen patients underwent tumor marker screening, of which one patient had a slight increase in carcinoembryonic antigen and carbohydrate antigen 125, one patient had a slight increase in cytokeratin 19 fragments, and the remaining patients had no abnormalities.
Head MRI Findings
All 16 patients with anti-LGI1 antibody encephalitis underwent a head MRI examination. The results showed that seven patients (43.75%) had abnormal intracranial lesions, mainly located in one or both frontotemporal lobes and the hippocampus, showing isointense and long T1, long T2, and high FLAIR signals. Six patients underwent head MRI enhancement, and one patient showed hippocampal enhancement. No clear anomalies were detected on residual enhancement scans. Among the other nine patients, eight (50.00%) had old lacunar infarction or ischemia, mostly located in the frontal-parietal lobe and basal ganglia. The head MRI of one patient (6.25%) showed no significant abnormality.
EEG Characteristics
General Analysis
All 16 patients with anti-LGI1 antibody encephalitis underwent video EEG monitoring; 4 patients (25.00%) showed no abnormal EEG activity, and 10 patients (62.50%) showed increased generalized slow waves or focal slow waves, mainly in the bilateral frontal region (Figure 1A). Focal slow waves with sphenoid discharge were found in one patient (6.25%) (Figure 1B). In one patient (6.25%), the video EEG detected background EEG with more myoelectric interference during the FBDS attack (Figure 1C).
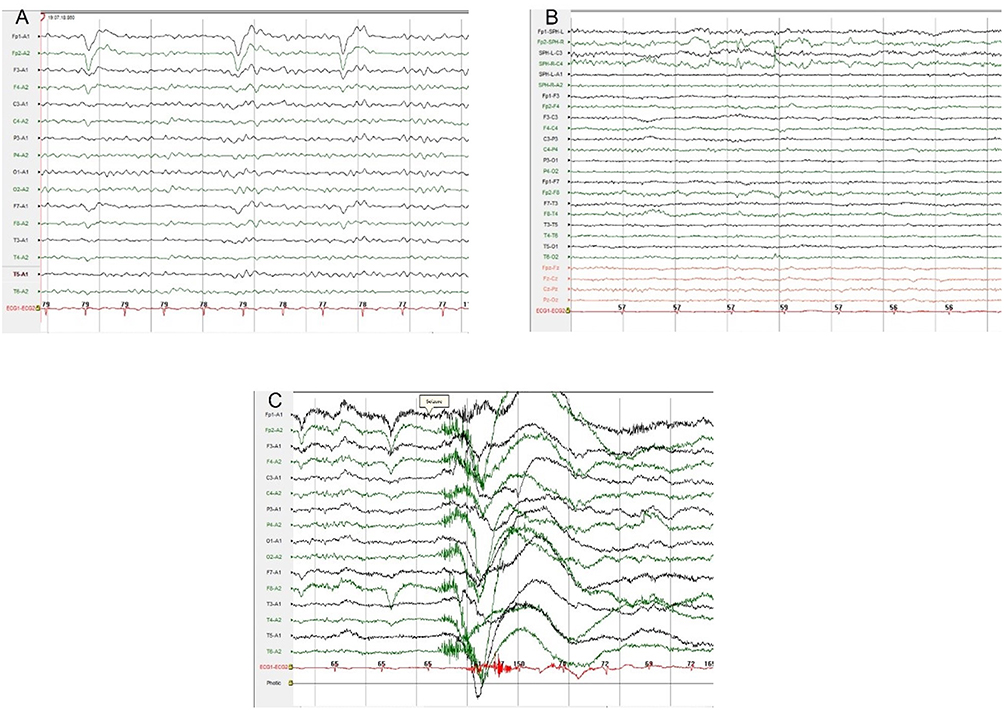 |
Figure 1 Video-EGG of anti-LGI1-antibody encephalitis. (A) Generalized slow wave increase; (B) focal slow wave with atypical sharp wave near the right sphenoid bone; (C) background EEG with more myoelectric interference in patients with FBDS. |
Analysis of Functional Connectivity of Brain Network
Ten patients with anti-LGI1 antibody encephalitis and ten healthy individuals matched by sex and age were included in the resting-state EEG analysis. The WPLI value matrix of the anti-LGI1 antibody encephalitis group and the healthy control group in the δ, θ, α, β, and γ bands were compared and analyzed, as shown in Figure 2. The differences in the figure represent the average results for all participants. The size of the connection difference between the LGI1 antibody encephalitis group and the healthy control group is indicated by color. The results showed that the LGI1 antibody encephalitis group had significantly lower connection strength in the δ and β bands than the healthy control group (P < 0.001).
 |
Figure 2 Anti-LGI1 antibody encephalitis group (A) and the healthy control group (B) showed differences in each frequency band and each lead connection matrix (the blue areas indicate that the functional connection of the experimental group was lower than that in the control group; while the yellow areas indicate the opposite). |
Additionally, according to the WPLI values of resting EEG in the anti-LGI1 antibody encephalitis group and the healthy control group, the functional connectivity maps of brain networks in the δ, θ, α, β, and γ bands were drawn respectively (Figure 3). The blue areas indicate that the functional connectivity of the experimental group is lower than that of the control group. Evidently, some functional connections in the frontal, parietal lobe of anti-LGI1 antibody encephalitis patients were significantly weakened compared with those in healthy individuals in the δ band (P = 0.042; < 0.05), and functional connections in the β band were significantly weakened in patients with LGI1 antibody encephalitis compared with those in healthy individuals (P < 0.001). There were no significant changes in functional connectivity in any other brain regions (P > 0.05).
 |
Figure 3 Brain functional network connection map. (A) shows the brain functional network connection map based on the WPLI values of EEG in δ, θ, α, β, and γ bands of the anti-LGI1 antibody encephalitis group. (B) is the brain functional network connection map drawn according to the WPLI value of EEG in the corresponding frequency band of the healthy control group (the red line indicates the lead position with the difference in WPLI value). |
Treatment
Immunotherapy
(1) First-line immunotherapy: Intravenous infusion of human immunoglobulin and/or glucocorticoids (intravenous shock therapy) was the first choice, including 13 patients treated with immunoglobulin combined with glucocorticoid shock therapy, 2 patients treated with glucocorticoids alone, and 1 patient treated with intravenous immunoglobulin IVIg alone. (2) Second-line immunotherapy: Six patients were treated with the oral immunosuppressant motemecolate. (3) Four patients with recurrent symptoms were readmitted to the hospital, and one patient received secondary intravenous human immunoglobulin therapy.
Antiepileptic drug therapy: All 14 patients with epilepsy symptoms received 1–2 antiepileptic drugs before immunotherapy. Among them, 10 showed significant improvement or complete remission, while 4 had poor effects of antiepileptic drug therapy. At the time of discharge, 10 patients were administered at least one antiepileptic drug.
Prognosis
Sixteen patients completed the follow-up period, achieving a follow-up rate of 100%. The mean follow-up time was 23.38 ± 2.75 months. Among them, (1) 14 patients with epilepsy symptoms and 7 patients without seizures following antiepileptic drug treatment had a completely seizure-free rate of 50%. Drug treatment improved in four patients, of which one patient did not stop after the attack, six patients maintained a single drug, four patients maintained two or more drugs, one patient discontinued due to unsatisfactory drug effects, and two patients died. (2) Nine patients with cognitive impairment reported that their cognitive ability had improved compared to before admission. (3) There was no significant difference in the activities of daily living scores of the patients during follow-up compared with those at admission (P = 0.104).
Discussion
Anti-LGI1 antibody encephalitis is a type of autoimmune encephalitis caused by a combination of autoantibodies and neuronal surface proteins and is relatively rare in clinical settings. In China, the annual incidence of anti-LGI1 antibody encephalitis is estimated at 0.5 cases per million people. Owing to increased awareness, its incidence may increase.9 The diagnosis should be combined with the patient’s clinical manifestations, CSF examination, neuroimaging, and EEG examination results; positive antineuronal antibodies are the main basis for diagnosis. Among the 16 patients observed in this study, no specific changes were found in the routine and biochemical analysis of CSF; abnormal lesions related to this disease were found intracranially in 7 patients through imaging examination, abnormal EEG was found in 12 patients through EEG examination, anti-LGI1 antibodies in blood and cerebrospinal fluid were positive in 7 patients through neuronal antibody examination, and anti-LGI1 antibodies in blood were positive in 5 patients. One patient had CSF anti-LGI1 antibody (+ / -) and four patients exhibited negative CSF results. According to the expert consensus, all 16 patients in this study met the diagnostic criteria.
Our study found that anti-LGI1 antibody encephalitis was mostly subacute and occurred in middle and old age (> 50 years old), with more males than females. The clinical manifestations were borderline encephalitis triad, that is, seizures, near memory loss, and mental behavior abnormalities. This is often accompanied by refractory hyponatremia, consistent with the findings of Rodriguez et al.10
Seizures are the most common clinical manifestation of anti-LGI1 antibody encephalitis and are one of the main reasons for patient visits, which is consistent with the findings of this study. In this study, more than half (62.5%, 10/16) of the patients with anti-LGI1 antibody encephalitis showed persistent slow EEG background rhythms during the active period of encephalitis, which is consistent with the EEG characteristics of autoimmune encephalitis described in other studies.11 FBDS is a clinical manifestation of anti-LGI1 encephalitis. FBDS is typically characterized by frequent (tens of times per day) and brief (lasting a few seconds) episodes of altered muscle tone on the same side and arm, sometimes involving the lower extremities and alternating on both sides.12 However, the nature of the FBDS remains controversial. Among the patients included in this study, only one patient showed FBDS, and this proportion was much lower than that reported in the literature. Video EEG detected background EEG with more myoelectric interference during FBDS attacks.
Cognitive impairment is one of the most common manifestations of anti-LGI1 antibody encephalitis, mainly manifesting as acute or subacute memory impairment, with near-memory impairment being the most prominent; approximately 25% of patients can fully recover their cognitive function.13 Studies have found that the connectivity of the hippocampal brain functional network is decreased in patients with anti-LGI1 antibody encephalitis, which is related to disease severity and memory decline.14 However, the current study showed that EEG abnormalities in patients with LGI1 antibody encephalitis were visible in the frontal, temporal, and parietal lobes. This suggests that the pathological changes induced by anti-LGI1 antibodies are not limited to the medial hippocampus and temporal lobes.
To clarify the functional network connectivity in various brain regions of these patients, we analyzed the resting-state EEG of patients with anti-LGI1 antibody encephalitis and drew functional connectivity maps. Some functional network connections in the frontoparietal lobes of patients with anti-LGI1 encephalitis were significantly weakened in the delta band. The frontal and parietal regions at the front and top of the brain are responsible for executive function, attention control, working memory, and sensory-motor tasks, respectively. The decreased delta band in the brain may reflect a decline in neuroplasticity or the brain’s ability to adapt to external stimuli and tasks. Previous functional MRI studies have shown that the functional network connections between the frontal and supplementary motor areas in patients with anti-LGI1 encephalitis have decreased significantly,15 which is consistent with our results, suggesting that functional connections related to motor regulation in the brains of patients have been damaged. We also found that patients with anti-LGI1 antibody encephalitis had significantly weaker functional connectivity in the beta band than healthy individuals. Beta waves in the brain are mainly produced in the frontal and parietal regions. Previous neuroscientific studies have shown that beta waves are closely associated with brain activity and concentration. Therefore, when beta waves are weakened, it may indicate that the brain is less activated to perform tasks, resulting in problems such as lack of attention and decreased cognitive function. This may manifest as symptoms, such as difficulties with learning and memory, reduced mental agility, and reduced ability to perform tasks. Therefore, the decreased beta connectivity between the frontal and parietal regions observed in this study may explain some of the neurological symptoms in patients with anti-LGI1 antibody encephalitis, such as memory loss, decreased responsiveness, and clinical symptoms of sleepiness. In addition, previous studies have pointed out16 that lesions in the frontal pole can lead to mental and behavioral abnormalities in patients, such as abnormal behavior, impulsive behavior, and emotional instability. This finding is consistent with the results of the present study. Therefore, abnormal functional network connectivity in the frontal region of the brain may be one of the mechanisms leading to mental and behavioral abnormalities in patients.
Some neurological diseases, such as Alzheimer’s and Parkinson’s diseases, have been found to be related to the weakening of functional connectivity in the frontal-parietal region of the brain.17,18 Therefore, weakened functional connectivity may act as an early indicator of neurological diseases or may be associated with disease development and progression. However, further study is required to determine whether the functional connections between the frontal and parietal lobes in anti-LGI1 antibody encephalitis can be used as neuroelectrophysiological biomarkers for disease development.
In this study, 62.50% (10/16) of the patients had hyponatremia, which is within the previously reported incidence range of 39–80%.19 This is because the hypothalamus and kidney co-express LGI1 and the LGI1 antibody acts on the neurons of the paraventricular nucleus of the hypothalamus, causing abnormal secretion of antidiuretic hormones.20 Among the patients, 38.46% (5/13) showed elevated IL-6, a pleiotropic pro-inflammatory cytokine. Its imbalance is associated with chronic inflammation and multifactorial autoimmune diseases.21 Wesselingh et al elucidated the role of the innate immune system in autoimmune encephalitis by testing IL-6 in the peripheral blood of 40 patients with autoimmune encephalitis. They found that elevated IL-6 levels reflected their persistent pro-inflammatory state and may lead to poor long-term prognosis.22 In the detection of serum cytokines in patients in this study, in addition to IL-6, a small number of patients showed elevated levels of IL-10, IL-8, IL-4, and IL-12P70, suggesting that an imbalance in the cytokine signaling network is inherently related to the pathogenesis of anti-LGI1 antibody encephalitis, which is worthy of further attention and discussion. The study also found that nearly half (5/12, 41.67%) of patients had reduced serum VitB12, while ferritin and folate levels were normal. Studies have shown that VitB12 deficiency can reduce the proportion of regulatory T cells, affect the immune system, and pro-inflammatory cytokines are reduced after vitamin supplementation,23 however, whether a direct relationship between serum VitB12 reduction and anti-LGI1 antibody encephalitis exists requires further investigation.
Typical MRI findings of anti-LGI1 antibody encephalitis include long T1 and T2 signals in the medial temporal lobe, hippocampus, or basal ganglia; high FLAIR sequences; and hippocampal atrophy in the later stage of the disease. This is consistent with our observation that 43.75% of patients with anti-LGI1 antibody encephalitis in this study had skull MRI lesions located in one or both frontotemporal lobes or the hippocampus, showing isointense and long T1, long T2, and high FLAIR signals, and 16.67% (1/6) of patients with skull MRI-enhanced scans showed hippocampal enhancement. FDG-PET is very important in the early stages of inflammation or when structural imaging is negative. The characteristic manifestation of anti-LGI1 antibody encephalitis on FDG-PET is high metabolism in the medial temporal lobe and basal ganglia, with a sensitivity of 87%, which is significantly higher than that of MRI (56%).24 In this study, 7 of the 16 patients (43.75%) were MRI-positive, and 1 of the 2 patients who underwent FDG-PET examination (50%) had abnormal metabolism. The sensitivity was higher than that of MRI. However, owing to the small number of patients who underwent FDG-PET examinations, the sensitivity could not be accurately evaluated.
Intravenous glucocorticoid shock and IVIg are the first-line immunotherapy regimens for anti-LGI1 antibody-associated encephalitis. In this study, the response and recurrence rates in patients receiving glucocorticoid plus IVIg combination therapy were 87.50% (14/16) and 12.50 (2/16), respectively. The remission and recurrence rates were 100% (2/2) and 50% (1/2), respectively, in patients receiving glucocorticoid therapy alone. One patient who received IVIg alone showed a poor response. A study summarized the results of different immunotherapy for anti-LGI1 antibody encephalitis in 390 patients, of the patients who received glucocorticoid plus IVIg combination therapy, 96.67% (58/60) had remission or complete remission of symptoms, and only 8.33% (5/60) relapsed. In contrast, 93.02% (40/43) of patients who received glucocorticoid therapy alone achieved remission, but the recurrence rate was 20.93% (9/43). However, the symptom remission and recurrence rates of patients who received IVIg alone were 87.50% (14/16) and 6.25% (1/16), respectively.25 In our study, patients treated with the glucocorticoid plus IVIg combination had a lower response rate and a higher recurrence rate than those in this study, which may be related to the small number of patients included. Second-line immunotherapy mainly consists of immunosuppressants, including rituximab, azathioprine, mortemycophenolate, cyclophosphamide, tacrolimus, and cyclosporine, which have been used in patients with anti-LGI1 antibody encephalitis of different ethnic groups and disease courses; however, there are no clear data on their therapeutic efficacy. In this study, only six patients were administered mortemycophenolate. Owing to the small number of patients and their combination with other immune drugs, it was not possible to draw a definite conclusion about their efficacy.
Conclusion
In summary, the typical symptoms of patients with anti-LGI1 antibody encephalitis are seizures and cognitive dysfunction, and abnormal immune indicators such as antinuclear antibodies and cytokines can be observed in serology. Abnormalities in the frontal-temporal lobe and hippocampus are mainly detected on brain MRI. EEG functional network connectivity analysis found that the characteristic δ and β band functional network connectivity of the frontal-parietal lobe in patients with anti-LGI1 antibody encephalitis may be a main feature. These findings reveal brain function changes beyond obvious structural damage and provide evidence for our research on the relationship between clinical manifestations and pathogenesis of anti-LGI1 antibody encephalitis. This study also illustrates the value of EEG as a traditional diagnostic tool in investigating the pathogenesis of anti-LGI1 antibody encephalitis.
Abbreviations
MRI, magnetic resonance imaging; EEG, electroencephalogram; LGI1, leucine-rich glioma-inactivated 1; FBDS, Facio brachial dystonic seizure; WPLI, Weighted phase lag index; CSF, cerebral spinal fluid; VitB12, vitamin B12; IL-6, interleukin-6; IL-8, interleukin-8; IL-10, interleukin-10; IL-4, interleukin-4; IL-12P70, interleukin-12P70.
Acknowledgments
The authors would like to thank for the financial support from Ministry of Science and Technology of the People’s Republic of China, Committee of Nature Science Foundation of Hebei Province, Hebei Provincial Health Commission, Hebei Provincial Administration of Traditional Chinese Medicine and the First Hospital of Hebei Medical University.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the medical science research project of Hebei Province (20240390), the Project of Traditional Chinese Medicine of Hebei Province (2023065 and 2024260), the “Spark” scientific research project of the First Hospital of Hebei Medical University (XH202405), the Nature Science Foundation of Hebei Province (H2020206632) and the National Key Research and Development Program of China (2022YFC3600500, 2022YFC3600503), and the Hebei Province Government-funded Excellent Talents Project in Clinical Medicine (2025054)
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Sarosh RI, Sian A, Patrick W, et al. Antibodies to Kv1 potassium channel-complex proteins leucine-rich, glioma inactivated 1 protein and contactin-associated protein-2 in limbic encephalitis, Morvan’s syndrome and acquired neuromyotonia. Brain. 2010;133(9):2734–2748.
2. Krieger S, Cook K, Hersh C. Understanding multiple sclerosis as a disease spectrum: above and below the clinical threshold. Curr Opinion Neurol. 2024;37(3):189–201. doi:10.1097/WCO.0000000000001262
3. Maarten JT, Lindsey M, Iñigo G, et al. Treatment and prognostic factors for long-term outcome in patients with anti-NMDA receptor encephalitis: an observational cohort study. Lancet Neurol. 2013;12(2):157–165.
4. Wei S, Huajun Y, Qun W. Neuronal surface antibody-medicated autoimmune encephalitis (Limbic Encephalitis) in China: a multiple-center, retrospective study. Front Immunol. 2021;12:621599.
5. Francesc G, Maarten JT, Ramani B, et al. A clinical approach to diagnosis of autoimmune encephalitis. Lancet Neurol. 2016;15(4):391–404. doi:10.1016/S1474-4422(15)00401-9
6. Wang JD, Xie L, Fang X, et al. Clinical validation of the 2020 diagnostic approach for pediatric autoimmune encephalitis in a single center. Zhonghua Er Ke Za Zhi. 2022;60(8):786–791. doi:10.3760/cma.j.cn112140-20220111-00039
7. Kundian G, Xu L, Jingfang L, et al. Clinical characteristics, long-term functional outcomes and relapse of anti-LGI1/Caspr2 encephalitis: a prospective cohort study in Western China. Ther Adv Neurol Disord. 2022;15:17562864211073203.
8. Martin V, Robert O, Marijn V, Franscesco B, Cyriel MAP. An improved index of phase-synchronization for electrophysiological data in the presence of volume-conduction, noise and sample-size bias. Neuroimage. 2011;57(1):55. doi:10.1016/j.neuroimage.2011.04.009
9. Li LH, Ma CC, Zhang HF, Lian YJ. Clinical and electrographic characteristics of seizures in LGI1-antibody encephalitis. Epilepsy Behav. 2018;88:277–282. doi:10.1016/j.yebeh.2018.08.019
10. Andrew R, Klein CJ, Elia S, et al. LGI1 antibody encephalitis: acute treatment comparisons and outcome. J Neurol Neurosurg Psychiatry. 2021;93(3):309–315. doi:10.1136/jnnp-2021-327302
11. Wesselingh R, Broadley J, Buzzard K, et al. Electroclinical biomarkers of autoimmune encephalitis. Epilepsy Behav. 2022;128:108571. doi:10.1016/j.yebeh.2022.108571
12. Irani S, Michell A, Lang B, et al. Faciobrachial dystonic seizures precede Lgi1 antibody limbic encephalitis. Ann Neurol. 2011;69(5):892–900. doi:10.1002/ana.22307
13. Sola-Valls N, Helena A, Domingo E, et al. Telemedicine assessment of long-term cognitive and functional status in anti-leucine-rich, glioma-inactivated 1 encephalitis. Neurol Neuroimmunol Neuroinflamm. 2019;7(2):e652.
14. Josephine H, Harald P, Michael S, et al. Transdiagnostic hippocampal damage patterns in neuroimmunological disorders. Neuroimage Clin. 2021;28:102515.
15. Josephine H, Harald P, Ute AK, et al. Beyond the limbic system: disruption and functional compensation of large-scale brain networks in patients with anti-LGI1 encephalitis. J Neurol Neurosurg Psychiatry. 2018;89(11).
16. Chow T. Personality in frontal lobe disorders. Current Psychiatry Reports. 2000;2(5):446–451. doi:10.1007/s11920-000-0031-5
17. Duan F, Huang Z, Sun Z, et al. Topological network analysis of early Alzheimer’s disease based on resting-state EEG. IEEE Trans Neural Syst Rehabil Eng. 2020;28(10):2164–2172. doi:10.1109/TNSRE.2020.3014951
18. Volker N, Andreas D, Nikolai A. Neuronal network oscillations in neurodegenerative diseases. Neuromolecular Med. 2015;17(3):270–284.
19. Li TR, Zhang YD, Wang Q, Shao XQ, Lyu DY, Lv RY. Clinical characteristics and long-term prognosis of Anti-LGI1 encephalitis: a single-center cohort study in Beijing, China. Front Neurol. 2021;12. doi:10.3389/fneur.2021.674368
20. Meizan L, Maartje GMH, Eric L, et al. Investigation of LGI1 as the antigen in limbic encephalitis previously attributed to potassium channels: a case series. Lancet Neurol. 2010;9(8):776–785.
21. Sukhvir K, Yogita B, Raj K, Gulshan B. A panoramic review of IL-6: structure, pathophysiological roles and inhibitors. Bioorg Med Chem. 2020;28(5):115327.
22. Robb W, Sarah G, James B, et al. Peripheral monocytes and soluble biomarkers in autoimmune encephalitis. J Autoimmun. 2023;135:103000.
23. Perran B, Selin Y, K-A E, et al. Vitamin B12 deficiency among asymptomatic healthy infants: its impact on the immune system. Minerva Pediatr. 2016;73(1):59–66.
24. Manon B, Mohammad BC, Matthieu D, et al. Brain (18)F-FDG PET for the diagnosis of autoimmune encephalitis: a systematic review and a meta-analysis. Eur J Nucl Med Mol Imaging. 2021;48(12):3847–3858.
25. Teng Y, Li T, Yang Z, et al. Clinical features and therapeutic effects of anti-leucine-rich glioma inactivated 1 encephalitis: a systematic review. Front Neurol. 2021;12:791014. doi:10.3389/fneur.2021.791014
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.