")
Back to Journals » Journal of Inflammation Research » Volume 18
Clinical Features and Prognosis of Double-Positive Anti-MDA5 and Anti-CCP Antibodies in Dermatomyositis: A Retrospective Study
Authors Xu X , Zhu L, Li S, Wang G, Ge Y
Received 12 November 2024
Accepted for publication 30 January 2025
Published 10 February 2025 Volume 2025:18 Pages 1929—1939
DOI https://doi.org/10.2147/JIR.S503120
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Tara Strutt
Xiayu Xu,1 Longyang Zhu,2 Sizhao Li,3 Guochun Wang,3 Yongpeng Ge3
1Department of Rheumatology and Immunology, The Second Affiliated Hospital of Hainan Medical University, Haikou, Hainan Province, People’s Republic of China; 2Peking University, China-Japan Friendship School of Clinical Medicine, Beijing, People’s Republic of China; 3Department of Rheumatology, The Key Laboratory of Myositis, China-Japan Friendship Hospital, Beijing, People’s Republic of China
Correspondence: Yongpeng Ge, Department of Rheumatology, The Key Laboratory of Myositis, China-Japan Friendship Hospital, Beijing, 100029, People’s Republic of China, Email [email protected]
Objective: To investigate the clinical features and prognosis of anti-melanoma differentiation-related gene 5 (MDA5) antibody and anti-cyclic citrullinated peptide (CCP) antibody double-positive dermatomyositis (DM) (MDA5+/CCP+ DM).
Methods: A retrospective analysis of 264 consecutive cases of MDA5+ DM hospitalized from March 2018 to March 2022, and patients with anti-CCP antibodies were screened out. Patients from MDA5+/CCP- served as the control. Propensity score matching was used to compare the clinical features, as well as the treatment and survival outcomes between the two groups.
Results: A total of 18 patients (6.8%) with MDA5+/CCP+ DM were identified. Gottron’s sign in 17 cases (94.4%), Heliotrope rash in 14 cases (77.8%), and skin ulcer in 5 cases (27.8%). Arthritis occurred in 10 cases (55.6%) and presented as the initial symptom in 6 cases (33.3%). Only 8 (44.4%) of the patients met the criteria for rheumatoid arthritis (RA). Interstitial lung disease (ILD) was diagnosed in 17 cases (94.4%), with non-specific interstitial pneumonia (NSIP) and organizing pneumonia (OP) combined with NSIP being the most predominant, as they presented in 6 cases (33.3%) each. Two of the ILD cases (11.1%) developed into rapidly progressive ILD (RP-ILD). Arthritis (55.6% vs 15.3%, p = 0.001) and malignancy (22.2% vs 0%, p < 0.001) were significantly more common in the MDA5+/CCP+ group compared to the MDA5+/CCP- group. The clinical manifestations of MDA5+/CCP+ DM with or without anti-Ro-52 antibody were not significantly different from those of the ILD type. During the follow-up period, there was no significant difference in survival between the two groups.
Conclusion: More than half of the patients with MDA5+/CCP+ DM may present with arthritis as one of the initial symptoms. They may also have an increased risk of malignancy. For MDA5+ DM patients with positive anti-CCP antibodies, thorough screening for tumors is crucial to guide treatment and improve prognosis.
Keywords: dermatomyositis, anti-MDA5 antibody, anti-CCP antibody, rheumatoid arthritis, interstitial lung disease
Introduction
Dermatomyositis (DM) is a type of idiopathic inflammatory myopathy (IIM) that primarily affects the skin, muscles, and lungs. Different myositis-specific antibodies represent different clinical subtypes. Anti-melanoma differentiation-related gene 5 (MDA5) antibody-positive DM (MDA5+ DM) is a unique subtype of DM that presents as clinically amyopathic DM (CADM). It is typically characterized by ulcerative rash, interstitial lung disease (ILD), and mild or no muscle involvement.1 Other possible symptoms include arthritis, fever, Raynaud’s phenomenon, and mechanic’s hands. MDA5+ DM is of great concern to clinicians due to the risk of rapid progressive ILD (RP-ILD) which may develop early in the course of the disease, as well as the high mortality rate associated with the condition. Despite the significant threat posed by RP-ILD, no fully effective treatment for the condition is currently available, and this highlights the need to explore the relationship between different clinical phenotypes, laboratory indicators, treatment responses, and prognosis. The anti-cyclic citrullinated peptide (CCP) antibody is specific for rheumatoid arthritis (RA).2 Previous studies revealed that the anti-CCP antibody is a risk factor for ILD in RA.3 The complication of IIM and RA has been previously described. One study reported that among 142 IIM patients, 12 were diagnosed with RA prior to the onset of myositis.4 It has been reported that some patients have a history of RA before MDA5+ DM is diagnosed.5 MDA5+ DM patients may present with inflammatory arthritis as an initial manifestation that resembles RA. Moreover, the anti-MDA5 antibody has also been detected in RA patients.6 Research has found that MDA5+ DM combined with other related autoantibodies generally has a relatively good prognosis.7 However, the clinical features and prognosis of DM with both anti-CCP and anti-MDA5 antibody positive (MDA5+/CCP+ DM) have been explored to a limited extent. The aim of this study was to analyze MDA5+/CCP+ DM and explore the clinical characteristics and prognosis associated with it. This will help physicians to better understand this subtype and guide clinical decision-making.
Materials and Methods
Study Design
The clinical data of 264 consecutive adult patients with MDA5+ DM, hospitalized in the Department of Rheumatology at the China-Japan Friendship Hospital from March 2018 to March 2022, was retrospectively analyzed. DM diagnosis was based on the 2017 European League of Rheumatology (EULAR) /American College of Rheumatology (ACR) Classification criteria8 or the 2018 European Neuromuscular Centre (ENMC) criteria.9 Patients with anti-MDA5 and anti-CCP antibodies were enrolled. The controls were selected using propensity score matching, which included MDA5+ DM patients without anti-CCP antibodies (MDA5+/CCP- DM). The presence of ILD was evaluated via chest high-resolution computed tomography (HRCT). RP-ILD was defined as a condition of worsening radiologic interstitial change with progressive dyspnea and hypoxemia within one month of the onset of respiratory symptoms.10 The study was conducted per the declaration of Helsinki, and the protocol was approved by the Ethics Committee of the China-Japan Friendship Hospital (reference number: 2022-KY-156). All patients signed an informed consent form on admission.
Clinical Findings, Laboratory Parameters, and Treatment
The backgrounds of the patients, along with clinical findings and treatment regimens were evaluated. Laboratory tests included lymphocyte count, creatine kinase (CK), lactic acid dehydrogenase (LDH), serum ferritin, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP). Pulmonary function test (PFT) results, which included forced vital capacity (FVC) and diffusing capacity of the lungs for carbon monoxide (DLCO), were also evaluated. Patients were initially divided into three groups according to the initial PFT values as referenced in previous studies. The groups were as follows: mild group (% predicted FVC > 75% and % predicted DLCO > 55%); moderate group (% predicted FVC from 50% to 75% or % predicted DLCO from >35% to 55%); and severe group (% predicted FVC < 50% and % predicted DLCO < 35%).11,12 In addition, the HRCT pattern was evaluated. Patient treatment parameters, including dosages of glucocorticoids (GC), steroid pulse therapy, immunosuppressive agents, intravenous immunoglobulin (IVIG), and biological agents, were also recorded.
Autoantibody Detection
Anti-MDA5 antibodies were quantified via immunoblotting according to the manufacturer’s instructions (Euroimmun, Lübeck, Germany). Myositis-associated antibodies (MAAs), antigens including Ro-52, antikeratin antibody (AKA), and antiperinuclear factor (APF), were quantified using the same method. The anti-CCP antibodies were quantified using the enzyme-linked immunosorbent assay (ELISA).
Propensity Score Methods
Propensity score matching to eliminate confounding factors in which the MDA5+ DM patients with or without anti-CCP antibodies would be balanced according to key baseline covariates. The selected independent covariates encompassed age, gender, smoking history, relevant past medical history (such as hypertension, diabetes mellitus, and hyperlipidemia), and the treatment regimen received prior to admission. For the matched analysis, the MDA5+/CCP+ group was matched with the MDA5+/CCP- group according to the propensity score, using a 1:4 matching ratio with the help of statistical software.
Statistical Analyses
All analyses were performed using the IBM SPSS software (version 26.0, Armonk, NY, USA). Continuous data were presented as mean ± SD. Categorical variables were presented as frequencies and percentages. The continuous variables were compared using ANOVA with a Bonferroni post hoc test when normally and homogeneously distributed. The Kruskal Wallis H-test with subsequent pairwise comparisons was used when the variables were not normally or inhomogeneous distributed. The Fisher’s exact test was employed for comparing categorical variables and Chi-square with Bonferroni adjustment for post hoc tests. Survival between the two groups was evaluated by applying the Kaplan-Meier (log-rank) test. All analyses were two-tailed and p values < 0.05 were considered to indicate statistical significance.
Results
General Characteristics
Among the 264 adult MDA5+ DM patients, 18 (6.8%) of them had MDA5+/CCP+ DM, and this included 11 females, with an average onset age of 43.8 years and a median course of disease of 4 months. Three cases had a history of smoking. All patients exhibited at least one typical rash, including 17 cases of Gottron’s sign (94.4%), 14 cases of Heliotrope rash (77.8%), 10 cases of shawl sign (55.5%), 8 cases of V-type rash (44.4%), 9 cases of mechanic hand (50%), and 7 cases of periungual erythema (38.9%). More results were as follows: skin ulcers (5 cases, 27.8%); Raynaud phenomenon (2 cases, 11.1%); subcutaneous calcification and subcutaneous edema (1 case each, 5.6%); myalgia (10 cases, 55.6%); mild muscle weakness (13 cases, 72.2%); and elevated CK levels (1 case, 5.6%). Muscle MRI examinations were performed in 5 cases, and inflammatory changes were observed in all of them. However, one of the cases also showed both fat infiltration and muscle atrophy.
Among the four patients with concomitant tumors, two had breast cancer and parotid mucoepidermoid carcinoma detected 10 and 14 months before diagnosis, respectively. One patient was diagnosed with breast cancer and uterine cancer 25 months after the DM diagnosis. Another patient developed natural killer (NK) cell lymphoma 3 years after the diagnosis.
Pulmonary Involvement in MDA5+/CCP+ DM
At the onset of the disease, 11 patients presented with dyspnea while seven had a cough. Lung HRCT was performed in all patients and the findings showed that 17 (94.4%) and 2 (11.1%) were diagnosed with ILD and RP-ILD, respectively. The main manifestations of HRCT were consolidation (50%), reticular shadowing (44%), and ground-glass opacity (38%) (Figure 1). In contrast, nodules (27%) and pleural effusion (11.1%) were less common among the patients. According to the CT pattern, there were 6 cases (33.3%) of nonspecific interstitial pneumonia (NSIP), 6 cases (33.3%) of NSIP combined with organizing pneumonia (OP), 4 cases (22.2%) of OP, and 1 case that could not be classified. A total of 11 patients underwent PFT and the results were as follows: four patients had mild limited diffusion function; five patients had moderate limited diffusion function; and two patients had severe limited diffusion function.
 |
Figure 1 Lung HRCT changes from two DM patients with MDA5+/CCP+. (A) A patient was diagnosed with RA. (B) The evolution of HRCT in a patient after treatment. |
Differences Between the MDA5+/CCP+ and MDA5+/CCP- Group
Based on the propensity matching method, 72 patients with MDA5+/CCP- DM were included for comparison. Arthritis [10 (55.6%) vs 11 (15.3%), p = 0.001] and malignancy [4 (22.2%) vs 0 (0%), p < 0.001] were significantly more common in the double antibody-positive group compared to the MDA5 +/CCP- DM group. In the MDA5+/CCP+ group, 33.3% of the patients presented with arthritis as an initial symptom. Contrastingly, arthritis was not observed as an initial symptom in the MDA5+/CCP- group. No significant differences were observed in gender, age of onset, smoking history, other clinical manifestations, lung function, and frequency and type of ILD between the two groups (Table 1). Correlation analysis within the MDA5+/CCP+ group revealed that the anti-CCP antibody titer did not correlate with the CRP, ESR, T lymphocyte count, LDH, or serum ferritin levels.
 |
Table 1 Characteristics of MDA5+ DM Patients with or Without Anti-CCP Autoantibody |
DM Combined with RA
Arthritis occurred in 10 cases (55.6%), and it mainly involved the wrist joints (100%), followed by the shoulder joints (50%), metacarpophalangeal joints (40%), proximal interphalangeal joints (40%), and knee joints (40%). Among the MDA5+/CCP+ DM patients, only 8 cases (44.4%) fulfilled the 2010 ACR/EULAR classification criteria for RA [12], and most of these were young and middle-aged men (62.5%). One case had a family history of RA. For MDA5+/CCP+ DM combined with RA (DM/RA) patients, symmetry arthritis was observed to be the initial manifestation in 6 cases. These patients subsequently developed DM typical skin rash and ILD at an average of 32.5 months and 33.2 months after the onset of arthritis, respectively. Anti-CCP antibodies were all high titer in these DM/RA, with APF positive in 2 cases, AKA positive in 3 cases, RF positive in 6 cases (high titer in 2 cases), and ANA positive in 7 cases. The ANA patterns were most commonly nuclear granular and nuclear homogeneous types (50%), and the anti-Ro-52 antibody was positive in 5 cases. Additionally, ESR, CRP, and serum ferritin were elevated in 6, 3, and 8 cases, respectively. Moreover, reduced T lymphocyte count and increased LDH were observed in 6 cases. The X-ray showed joint space stenosis in 2 cases and cystic degeneration in 1 case. Joint ultrasonography revealed joint effusion and synovial hyperplasia in 2 cases. The findings from joint MRI indicated the presence of bone marrow edema in 3 cases, cystic degeneration in 2 cases, as well as joint effusion and synovial hyperplasia in 2 cases. Five patients had articular bone erosion compatible with RA, and two of them took anti-rheumatic drugs. The CT patterns of ILD were predominantly NSIP or NSIP combined with OP. Five patients underwent PFTs, all of whom had reduced diffusion function. Two patients died, one from respiratory failure and the other from lung lymphoma. The clinical features and typical imaging findings are shown in Table 2 and Figure 2A and B. Compared with MDA5+/CCP+ DM without RA, patients with RA had higher CCP antibody levels (871.13±882.75 vs 446.90±983.40, p = 0.013) (see supplemental Table S1).
 |
Table 2 Clinical Features of MDA5+/CCP+ DM with RA at Initial Admission |
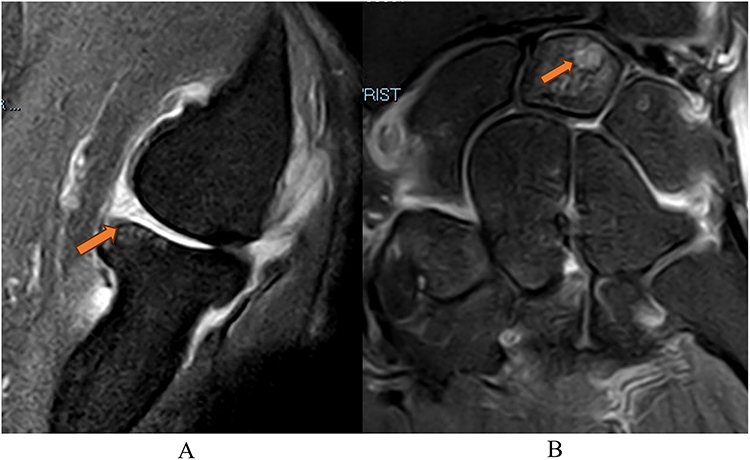 |
Figure 2 MRI (T2WI) revealed joint space narrowing, synovitis, and cartilage damage. (A) Right elbow joint effusion and bone erosion (arrow). (B) Cystic lesion in right carpal bone (arrow). |
Clinical Features of MDA5+/CCP+ DM with or Without Anti-Ro-52 Antibody
Among DM patients with MDA5+/CCP+, 8 cases (44.4%) were positive for anti-Ro-52 antibodies. Further comparison of clinical features between the anti-Ro52+ and the Ro52- groups revealed no statistically significant differences in gender, age, clinical manifestations, and ILD type between the two groups (supplemental Table S2).
Analysis of Co-Infection
The incidence of infection after immunotherapy was higher in the MDA5+/CCP+ group than in the MDA5+/CCP- group, but the difference was not statistically significant (66.6% vs 56.9%, p = 0.453). Viral infection was the most common, with 4 cases of Cytomegalovirus (CMV) infection, and 1 case each of Epstein-Barr virus (EBV) infection and herpes simplex virus (HSV) infection. Bacterial infection occurred in 2 cases while fungal infection was observed in 4 cases, including Pneumocystis jiroveci pneumonia (PJP) (3 cases) and Candida albicans (1 case).
Treatment and Follow-up
All MDA5+/CCP+ DM patients received glucocorticoids combined with at least one immunosuppressant, including cyclosporine (n = 5), tacrolimus (n = 4), cyclophosphamide (n = 5), baricitinib (n = 3), tofacitinib (n = 1), and/or intravenous immunoglobulin (IVIG) (n = 3). In the anti-MDA5+/CCP- group, 3 cases were treated with glucocorticoid alone due to severe pulmonary infection, while the remaining patients received combination therapy included cyclosporine (n = 35), tacrolimus (n = 13), cyclophosphamide (n = 2), methotrexate (n = 1), mycophenolate (n = 1), baricitinib (n = 7), tofacitinib (n = 11), and/or intravenous immunoglobulin n = 18). Cyclophosphamide was used more frequently in the anti-MDA5+/CCP+ group (27.8% vs 2.8%, p = 0.002). However, there were no other significant differences in the treatment regimens between the two groups. In the MDA5+/CCP+ group, three deaths (16.7%) were recorded. Two of the deaths were due to respiratory failure and were attributed to lymphoma. In the MDA5+/CCP- group, 17 patients died (23.6%), 11 of whom succumbed to respiratory failure while six of the deaths were due to respiratory failure combined with pulmonary infection. The mortality rate of the antibody double-positive group was lower than that of the anti-CCP-negative group. However, the Kaplan-Meier survival analysis showed that there was no statistically significant difference in survival rates between the two groups (p = 0.3525) (Figure 3).
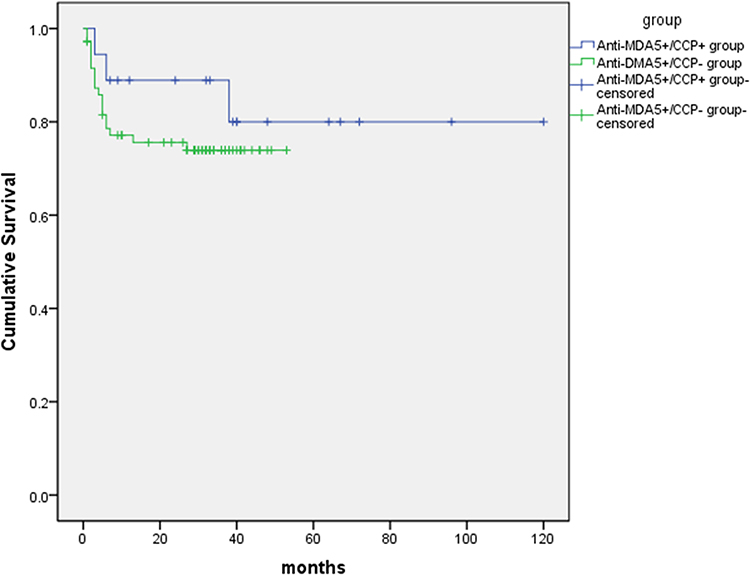 |
Figure 3 Kaplan-Meier curves for the MDA5+/CCP+ and MDA5+/CCP- subgroups. |
Discussion
This study reported the clinical features and prognosis of MDA5+/CCP+ DM patients. The findings showed that the prevalence rate of anti-CCP was low in MDA5+ DM patients, though the majority of them had concurrent ILD. Additionally, nearly half the MDA5+/CCP+ patients met the diagnosis criteria of RA, and most of them were middle-aged males. It’s important to note that this group of patients exhibited a higher risk of developing tumors.
The significance of anti-CCP antibodies in IIM was first analyzed by in 2009.13 Among the 90 IIM patients who were included in this study, 13.3% were anti-CCP antibody positive. Although the prevalence of RF in anti-CCP-positive patients was high, no statistically significant clinical correlation was found. This suggests the possibility of a false positive result with no clinical significance. Previous study reported that the prevalence of anti-CCP in IIM was 4.96%,14 which was lower than other studies, but still, no clinical correlation of this antibody was observed. Contrary to these findings, Meyer et al, who was the first to evaluate the clinical significance of anti-CCP in anti-synthetase syndrome (ASS) patients, found that about 88% of anti-CCP-positive ASS had polyarthralgia and/or polyarthritis as the initial symptom. Additionally, all anti-CCP-positive ASS patients had arthritis and met the RA classification criteria.15 The joint distribution was similar to that of RA and was associated with more severe erosive arthritis. It is suggested that anti-CCP in ASS can be regarded as a marker of overlap with RA. Similarly, this study also found that MDA5+/CCP+ DM patients was associated with a higher incidence of arthritis, where solitary arthritis could be the first symptom. Considering that a small number of patients underwent imaging examination in our study, it’s not possible to determine whether anti-CCP antibodies cause severe erosive arthritis in patients with MDA5+/CCP+ DM or not.
There was no difference in the joint involvement pattern between MDA5+/CCP+ DM patients with or without RA. Both groups could present with symmetric arthritis, with more facet joint involvement and a distribution similar to that of RA. Unlike isolated RA, which predominantly affects middle-aged women, MDA5+/CCP+ DM/RA is more common in young and middle-aged men.
Skin lesions and ILD were the most common symptoms in MDA5+/CCP+ DM patients. In a single-center study in China, the most common imaging manifestations of MDA5+ DM-ILD were OP, NSIP, and NSIP+OP. Histopathology results also showed that NSIP and NSIP+OP dominated, while usual interstitial pneumonia (UIP) was rare.16 This study had similar results, DM patients with MDA5+/CCP+, the most common diagnoses were NSIP, followed by OP+NSIP and OP. UIP was not observed in the MDA5+/CCP+ group. There was no significant difference in ILD radiological patterns observed in the MDA5+/CCP+ group, compared with the CCP- group. The occurrence of RA-ILD is related to the anti-CCP antibody. It’s also crucial to note that in RA-ILD, the most common CT patterns are UIP and NSIP.17 Unlike RA-ILD, DM with double positive anti-MDA5 and anti-CCP antibodies may exhibit independent ILD phenotypes, and these need to be further confirmed by lung histopathology.
Previous studies have shown that the positive anti-Ro-52 antibody MDA5+ DM patients are associated with higher RP-ILD incidence and mortality.18 In this study, anti-Ro-52 antibodies were present in nearly half of MDA5+/CCP+ DM patients, and only one of them developed RP-ILD. No significant difference in clinical manifestations and ILD types was observed between patients with and without Ro-52. This finding could have been influenced by the small sample size used in this study, which could have interfered with getting meaningful results. Therefore, future studies with larger sample sizes are required to further explore the serological significance of anti-Ro-52 antibodies in MDA5+/CCP+ DM patients.
It has been reported that the risk of malignant tumors in adult DM is 4.66 times higher than in the general population.19 Malignant tumors can occur before, during, or after the diagnosis of DM. However, the results from most studies agree that the risk is highest within one year of diagnosis. The occurrence of tumors is related to MSA, anti-TIF1-γ showing the strongest correlation with malignant growths.20 In contrast, the anti-MDA5 antibody is associated with a relatively low risk of malignancy.21 Other studies have found no correlation between anti-MDA5 antibodies and malignant tumors.22 A long-term study on the risks of malignant tumors in MSA-positive IIM revealed that there is no risk of early malignant growths in individuals with anti-MDA5 antibodies. However, the standardized incidence ratio of malignant tumors increased significantly 4–10 years after the onset, indicating a potential link to a higher risk of advanced malignant tumors.23 In this study, nearly a quarter of the patients with MDA5+/CCP+ DM developed malignant tumors. Three had solid tumors, one had hematological malignancy, and death was recorded three years after diagnosis. Cancer is one of the most common causes of death in patients with DM.24 So early detection is crucial for improving prognosis. Anti-CCP positivity has been reported in both solid and hematological malignancies,25 and Chatzidionysiou et al found that anti-CCP antibody positivity and serum double positive (RF and CCP) are powerful and independent risk factors for lung cancer in RA patients.26 Although it is unclear whether autoantibodies play a direct role in cancer pathogenesis or not, the anti-CCP antibody may be a risk factor for tumor development in MDA5+ DM patients. Screening for these antibodies might aid in the early detection of malignancies, though larger population studies are needed to confirm this notion.
Viral and fungal infections are particularly common complications of MDA5+ DM. It’s important to note that the presence of the anti-MDA5 antibody is an independent risk factor for infection.27 Both MDA5+/CCP+ and MDA5+/CCP - patients were affected by the infections at similar rates, with viral and fungal infections being the most common in both groups.
In the DM subgroup, MDA5+ DM patients have the worst prognosis, especially in the East Asian population. Although respiratory failure due to RP-ILD is the leading cause of death, especially during the early stages, Infection is also a significant cause of mortality. In this study, most deaths were due to ILD-induced respiratory failure and co-infection, with no statistically significant difference in mortality observed between the two groups. Therefore, the presence of anti-CCP antibodies may not increase the incidence of infection and RP-ILD.
Kochi et al showed that WDFY4 (a variant of the WDFY family member 4) gene have a significant association with MDA5+ DM.28 Interestingly, the association of variants in WDFY4 is also reported in RA.29 These findings suggest that these genetic factors may be associated with ILD occurrence in not only MDA5+ DM patients but also those with RA-ILD. Recently, Oka et al reported anti-MDA5 antibodies levels were higher in RA patients with airway diseases and chronic lung diseases.30 Further investigations will be needed to clarify the relationship between MDA5+ DM and CCP or RA.
This study had some limitations. First, as a retrospective study, it lacked standardized clinical assessment, which possibly led to partial data loss and an incomplete reflection of the clinical features of anti-MDA5 and anti-CCP antibody double-positive dermatomyositis. Second, the pathogenesis of anti-CCP autoantibodies in MDA5+DM remains unclear. Besides, bias may be introduced in patient selection and data analysis due to the retrospective nature of this study. Additionally, the reliance on self-reported clinical features and potential variations in follow-up protocols can impact the robustness of the data. Further basic research and large-scale prospective observational studies are necessary to elucidate the specific mechanisms and clinical significance of these autoantibodies.
Conclusions
This study described the clinical features and prognosis of patients with and without anti-CCP antibodies in anti-MDA5-positive DM. The findings suggest that some patients with MDA5+/CCP+ DM present with arthritis as the initial symptom and have an increased risk of malignancy. For the majority of MDA5+/CCP+ DM/RA patients, RA symptoms precede DM onset. Therefore, it is important to be vigilant against the occurrence of rashes and non-UIP ILD in CCP-positive RA patients, as these could be signs that may indicate the development of MDA5+ DM. For MDA5+ DM patients with symmetric arthritis who are positive for anti-CCP antibodies, regular follow-ups for tumor screening are crucial. This approach is significant for guiding treatment and improving patient prognosis.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Informed Consent
The research protocol was granted approval by the Ethics Committee of the China Japan Friendship Hospital (reference number 2022-KY-156). All patients signed an informed consent form on admission.
Funding
This study was supported by the Elite Medical Professionals Project of China-Japan Friendship Hospital (ZRJY2023-GG02) and National High Level Hospital Clinical Research Funding (2022-NHLHCRF-YS-02).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lundberg IE, Fujimoto M, Vencovsky J, et al. Idiopathic inflammatory myopathies. Nat Rev Dis Primers. 2021;7(1):86. doi:10.1038/s41572-021-00321-x
2. Avouac J, Gossec L, Dougados M. Diagnostic and predictive value of anti-cyclic citrullinated protein antibodies in rheumatoid arthritis: a systematic literature review. Ann Rheum Dis. 2006;65:845–851. doi:10.1136/ard.2006.051391
3. Kelly CA, Saravanan V, Nisar M, et al. Rheumatoid arthritis-related interstitial lung disease: associations, prognostic factors and physiological and radiological characteristics--a large multicenter UK study. Rheumatology. 2014;53(9):1676–1682. doi:10.1093/rheumatology/keu165
4. Nakajima A, Yoshino K, Soejima M, et al. High frequencies and co-existing of myositis-specific autoantibodies in patients with idiopathic inflammatory myopathies overlapped to rheumatoid arthritis. Rheumatol Int. 2012;32(7):2057–2061. doi:10.1007/s00296-011-1931-x
5. Xiong H, Tan Q, Luo F, et al. Anti-MDA5 and anti-SSA /Ro52 antibodies double-positive dermatomyositis overlapping with rheumatoid arthritis-associated interstitial lung disease: a case report. Int J Rheum Dis. 2022;25(12):1437–1440. doi:10.1111/1756-185X.14430
6. Matsumoto H, Sato S, Fujita Y, et al. Rheumatoid arthritis complicated with anti-melanoma differentiation-associated Gene 5 antibody-positive interstitial pneumonia. Intern Med. 2019;58(5):737–742. doi:10.2169/internalmedicine.1613-18
7. Yamaguchi K, Yamaguchi A, Kashiwagi C, et al. Differential clinical features of patients with clinically amyopathic dermatomyositis who have circulating anti-MDA5 autoantibodies with or without myositis-associated autoantibodies. Respir Med. 2018;140:1–5. doi:10.1016/j.rmed.2018.05.010
8. Lundberg IE, Tjärnlund A, Bottai M, et al. 2017 European League against rheumatism/American College of Rheumatology classification criteria for adult and juvenile idiopathic inflammatory myopathies and their major subgroups. Ann Rheum Dis. 2017;76(12):1955–1964. doi:10.1136/annrheumdis-2017-211468
9. Mammen AL, Allenbach Y, Stenzel W, Benveniste O; ENMC 239th Workshop Study Group. 239th ENMC International Workshop: classification of dermatomyositis, Amsterdam, the Netherlands, 14–16 December 2018. Neuromuscul Disord. 2020;30(1):70–92. doi:10.1016/j.nmd.2019.10.005
10. Sato S, Hoshino K, Satoh T, et al. RNA helicase encoded by melanoma differentiation-associated gene 5 is a major autoantigen in patients with clinically amyopathic dermatomyositis: association with rapidly progressive interstitial lung disease. Arthritis Rheum. 2009;60(7):2193–2200. doi:10.1002/art.24621
11. Ley B, Ryerson CJ, Vittinghoff E, et al. A multidimensional index and staging system for idiopathic pulmonary fibrosis. Ann Intern Med. 2012;156(10):684–691. doi:10.7326/0003-4819-156-10-201205150-00004
12. Aletaha D, Neogi T, SIlman A, et al. 2010 rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Ann Rheum Dis. 2010;69:1580–1588. doi:10.1136/ard.2010.138461
13. Labrador-Horrillo M, Martinez MA, Selva-O’Callaghan A, et al. Anti-cyclic citrullinated peptide and anti-keratin antibodies in patients with idiopathic inflammatory myopathy. Rheumatology. 2009;48(6):676–679. doi:10.1093/rheumatology/kep065
14. Ide V, Bossuyt X, Blockmans D, De Langhe E. Prevalence and clinical correlates of rheumatoid factor and anticitrullinated protein antibodies in patients with idiopathic inflammatory myopathy. RMD Open. 2018;4(2):e000661. doi:10.1136/rmdopen-2018-000661
15. Meyer A, Lefevre G, Bierry G, et al. In antisynthetase syndrome, ACPA are associated with severe and erosive arthritis: an overlapping rheumatoid arthritis and antisynthetase syndrome. Medicine. 2015;94(20):e523. doi:10.1097/MD.0000000000000523
16. Chen X, Jiang W, Jin Q, et al. Clinical, radiological and pathological features of anti-MDA5 antibody-associated interstitial lung disease. RMD Open. 2023;9(2):e003150. doi:10.1136/rmdopen-2023-003150
17. Kelmenson LB, Demoruelle MK, Deane KD. The complex role of the lung in the pathogenesis and clinical outcomes of rheumatoid arthritis. Curr Rheumatol Rep. 2016;18(11):69. doi:10.1007/s11926-016-0618-4
18. Lv C, You H, Xu L, et al. Coexistence of anti-Ro52 antibodies in anti-MDA5 antibody-positive dermatomyositis is highly associated with rapidly progressive interstitial lung disease and mortality risk. J Rheumatol. 2023;50(2):219–226. doi:10.3899/jrheum.220139
19. Qiang JK, Kim WB, Baibergenova A, Alhusayen R. Risk of malignancy in dermatomyositis and polymyositis. J Cutan Med Surg. 2017;21(2):131–136. doi:10.1177/1203475416665601
20. DeWane ME, Waldman R, Lu J. Dermatomyositis: clinical features and pathogenesis. J Am Acad Dermatol. 2020;82(2):267–281. doi:10.1016/j.jaad.2019.06.1309
21. Yang H, Peng Q, Yin L, et al. Identification of multiple cancer-associated myositis-specific autoantibodies in idiopathic inflammatory myopathies: a large longitudinal cohort study. Arthritis Res Ther. 2017;19(1):259. doi:10.1186/s13075-017-1469-8
22. Moghadam-Kia S, Oddis CV, Ascherman DP, Aggarwal R. Risk factors and cancer screening in myositis. Rheum Dis Clin North Am. 2020;46(3):565–576. doi:10.1016/j.rdc.2020.05.006
23. Izuka S, Komai T, Shoda H, Fujio K. Long-term risks of malignancy in myositis-specific antibody-positive idiopathic inflammatory myopathy. Rheumatol Int. 2023;43(2):335–343. doi:10.1007/s00296-022-05214-0
24. Marie I. Morbidity and mortality in adult polymyositis and dermatomyositis. Curr Rheumatol Rep. 2012;14(3):275–285. doi:10.1007/s11926-012-0249-3
25. Kısacık B, Albayrak F, Balcı MA, Koc E. Paraneoplastic arthritis: a series of 92 cases. Rheumatology. 2024;63(7):1923–1926. doi:10.1093/rheumatology/kead500
26. Chatzidionysiou K, Di Giuseppe D, Soderling J, Catrina A, Askling J. Risk of lung cancer in rheumatoid arthritis and in relation to autoantibody positivity and smoking. RMD Open. 2022;8(2):e002465. doi:10.1136/rmdopen-2022-002465
27. Ge YP, Shu XM, He LR, Wang GC, Lu X. Infection is not rare in patients with idiopathic inflammatory myopathies. Clin Exp Rheumatol. 2022;40(2):254–259. doi:10.55563/clinexprheumatol/yps7ai
28. Kochi Y, Kamatani Y, Kondo Y, et al. Splicing variant of WDFY4 augments MDA5 signalling and the risk of clinically amyopathic dermatomyositis. Ann Rheum Dis. 2018;77(4):602–611. doi:10.1136/annrheumdis-2017-212149
29. Zhang Y, Bo L, Zhang H, Zhuang C, Liu R. E26 transformation-specific-1 (ETS1) and WDFY family member 4 (WDFY4) polymorphisms in Chinese patients with rheumatoid arthritis. Int J mol Sci. 2014;15(2):2712–2721. doi:10.3390/ijms15022712
30. Oka S, Higuchi T, Furukawa H, et al. Antibodies against serum anti-melanoma differentiation-Associated Gene 5 in rheumatoid arthritis patients with chronic lung diseases. Medicina. 2023;59(2):363. doi:10.3390/medicina59020363
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Risk Factors and Predictive Model for Dermatomyositis Associated with Rapidly Progressive Interstitial Lung Disease
Wang K, Tian Y, Liu S, Zhang Z, Shen L, Meng D, Li J
Pharmacogenomics and Personalized Medicine 2022, 15:775-783
Published Date: 1 September 2022
Overview on the Link Between the Complement System and Auto-Immune Articular and Pulmonary Disease
Triggianese P, Conigliaro P, De Martino E, Monosi B, Chimenti MS
Open Access Rheumatology: Research and Reviews 2023, 15:65-79
Published Date: 15 May 2023
Positive HIV Screening Test in a Patient with Rapidly Progressive Interstitial Lung Disease: A Case Report
Chen X, Cai M, Ma Y, Zhang T, Zhang Y
Infection and Drug Resistance 2024, 17:5111-5116
Published Date: 20 November 2024
Clinical Significance of Abnormal Serum LGALS3BP Expression in Patients with Idiopathic Inflammatory Myopathies
Huang L, Huang X, Zhou W, Jiang Y, Zhu H, Lao Y, Deng Z, Tang Y, Wang J, Li X
Journal of Inflammation Research 2024, 17:9697-9710
Published Date: 25 November 2024
The Value of NLR and PLR in the Diagnosis of Rheumatoid Arthritis Combined with Interstitial Lung Disease and Assessment of Treatment Effect: A Retrospective Cohort Study
Cui P, Cheng T, Yan H, Xu D, Ren G, Ma S
International Journal of General Medicine 2025, 18:867-880
Published Date: 19 February 2025