")
Back to Journals » Journal of Inflammation Research » Volume 17
Clinical Features of Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis Induced by Immune Checkpoint Inhibitor versus Non-Immune Checkpoint Inhibitor Drugs in China: A Cross-Sectional Study and Literature Review
Authors Qin K , Gong T, Ruan SF, Lin M, Su X, Lv X, Cheng B, Ji C
Received 16 August 2024
Accepted for publication 17 October 2024
Published 22 October 2024 Volume 2024:17 Pages 7591—7605
DOI https://doi.org/10.2147/JIR.S491791
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Kun Qin,1,2,* Ting Gong,3,* Shi-Fan Ruan,1,* Min Lin,1 Xinhong Su,1 Xiaoqing Lv,1 Bo Cheng,1,4 Chao Ji1,4
1Department of Dermatology, The First Affiliated Hospital of Fujian Medical University, Fuzhou, Fujian, 350000, People’s Republic of China; 2Department of Dermatology, Jiangmen Central Hospital, Jiangmen, Guangdong, 529000, People’s Republic of China; 3Central Laboratory, The First Affiliated Hospital of Fujian Medical University, Fuzhou, Fujian, 350000, People’s Republic of China; 4Key Laboratory of Skin Cancer of Fujian Higher Education Institutions, The Fujian Medical University, Fuzhou, Fujian, 350000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chao Ji; Bo Cheng, Department of Dermatology, The First Affiliated Hospital of Fujian Medical University, 20 Chazhong Road, Taijiang District, Fuzhou, Fujian, 350000, People’s Republic of China, Tel +86 18651619908 ; Tel +86 13859024296, Email [email protected]; [email protected]
Purpose: Immune checkpoint inhibitors (ICIs) can cause life-threatening Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN). Large-scale original research on ICI-induced SJS/TEN is limited. This study aimed to explore the unique clinical characteristics and potential pathophysiological mechanisms of SJS/TEN induced by ICIs.
Methods: This cross-sectional study compared the clinical features of SJS/TEN induced by ICIs and non-ICIs, and reviewed the case characteristics of ICI-induced SJS/TEN. Clinical features were analyzed using independent t-tests, Mann–Whitney U-tests, and multivariable regression models.
Results: This study enrolled 41 cases of ICI-induced SJS/TEN and 107 non-ICI-induced cases from January 22, 2015, to May 28, 2024. ICI-induced SJS/TEN patients exhibited a trend towards a longer latency period (β: 17, 95% CI: − 1.49 to 35.48), a smaller affected body surface area (BSA) (β: − 40.68, 95% CI: − 71.59 to − 9.77), and milder oral and ocular mucositis than non-ICI-induced cases. A literature review identified PD-1 inhibitors as the primary ICIs involved and systemic corticosteroids as the most frequent intervention. No statistically significant difference in mortality rate was observed between patients treated with systemic corticosteroids alone and those receiving combination therapies (P= 0.85). The mortality rate for ICI-induced SJS/TEN was 24.5%.
Conclusion: This study offered the largest comparative analysis to date, highlighting the unique clinical features of ICI-induced SJS/TEN, including a smaller affected BSA, a prolonged latency period trend, and milder oral and ocular mucositis. We described the epidemiology, clinical presentation, and therapeutic strategies for ICI-induced SJS/TEN. These findings not only contribute to a deeper understanding of the complex immune-inflammatory pathways in severe immune-related cutaneous adverse events (ircAEs) but also may inform the development of more targeted and effective treatments.
Keywords: comparative analysis, clinical characteristic, latency period, body surface area, treatment
Introduction
Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are rare but severe mucocutaneous inflammatory reactions, predominantly induced by medications and characterized by extensive epidermal detachment and mucosal involvement, which can have fatal outcomes.1 SJS and TEN are categorized based on the proportion of the total body surface area (BSA) that represents the degree of detached and detachable epidermis. These conditions represent a continuum of disease severity, with SJS characterized by less than 10% BSA detachment, TEN involving more than 30%, and SJS/TEN overlap syndrome covering 10–30%.2,3 The etiology often includes a wide range of drugs, with antibiotics, anticonvulsants, and nonsteroidal anti-inflammatory drugs (NSAIDs) being the most common culprits.4–6
Immune checkpoint inhibitors (ICIs), including monoclonal antibodies targeting the cytotoxic T-lymphocyte associated protein 4 (CTLA4), the programmed death ligand 1 (PD-L1), and the programmed cell death receptor-1 (PD-1), represent a novel class of cancer immunotherapy drugs approved by the Food and Drug Administration (FDA).7,8 They have been used to treat a variety of cancers, such as melanoma and lung cancer. The advent of ICI has benefited the treatment of cancer patients in oncology, offering new hope for many cancer patients. However, the ICI therapies have been associated with unique skin adverse events known as immune-related cutaneous adverse events (ircAEs), with the most severe and fatal being SJS/TEN.9 The clinical features and outcomes of SJS/TEN induced by ICIs may differ from those caused by conventional non-immune checkpoint inhibitor (non-ICI) drugs due to the distinct mechanisms of action and immunological characteristics.
Despite the increasing use of ICIs in oncology, the existing studies on ICI-induced SJS/TEN primary are case reports, case series, and reviews.10–14 Most studies have focused on the overall incidence, risk factors, pathogenesis, mortality, therapies, and potential prevention strategies of SJS/TEN,5,15,16 but few comparative analyses examine the differences in presentation based on causative drug types.17 Until now, there has been no large-scale original research exploring the clinical manifestations of ICI-induced SJS/TEN. Understanding these differences is crucial, as they influence clinical decision-making, management strategies, and patient counseling. Patients who recover from ICI-induced SJS/TEN may require adjustments to their subsequent cancer treatment strategies.
This study aimed to compare the clinical manifestations of SJS/TEN induced by ICIs versus non-ICI medications, focusing on factors such as the extent of epidermal detachment, latency periods, and the severity of oral and ocular mucosal damage. We also aimed to perform a descriptive statistical analysis of clinical factors, including the Score of Toxic Epidermal Necrolysis (SCORTEN) score, specific ICIs and associated cancers, mucosal damage, and treatment outcomes of ICI-induced SJS/TEN. By integrating our institutional data with previously published literature (Supplementary Table S1), we hope to reveal the unique clinical characteristics and pathophysiological mechanisms of ICI-induced SJS/TEN, which might contribute to the development of more personalized and safer oncology interventions aimed at improving prognosis and quality of life for cancer patients.
Methods
Study Design and Patient Population
This cross-sectional study was conducted from January 22, 2015, to May 28, 2024, using detailed medical records of drug eruption patients from the dermatology inpatient department of the First Affiliated Hospital of Fujian Medical University (FJMU), China. As the largest grade-A tertiary hospital in the South China region, this study also encompassed SJS/TEN cases referred from lower-tier hospitals for specialized diagnosis and treatment at our institution. Histological examinations were conducted on all patients. These cases were identified and included based on the clinical diagnosis and causative agent confirmed by the treating physicians.
Additionally, we reviewed the literature to summarize the data of ICI patients with SJS/TEN in previously published studies. We searched PubMed through June 2024 using the following search parameters: [“Stevens Johnson Syndrome” OR “SJS/TEN” OR “Toxic Epidermal Necrosis”] AND [“immune checkpoint inhibitors” OR “PD-L1” OR “PD1” OR “ICI” OR “CTLA-4” OR “penpulimab” OR “atezolizumab” OR “toripalimab” OR “relatlimab” OR “avelumab” OR “retifanlimab” OR “cemiplimab” OR “ipilimumab” OR “tremelimumab” OR “nivolumab” OR “camrelizumab” OR “dostarlimab” OR “pembrolizumab” OR “sintilimab” OR “durvalumab” OR “tislelizumab”]. There were only full-text articles in English, French, and German.
Ethical Considerations
The research protocol for this study was compliant with the Declaration of Helsinki, and it was approved by the Research Ethical Committee of the First Affiliated Hospital of FJMU (Ethical Committee Number: MRCTA, ECFAH of FMU [2023]400). It was also registered in the Clinical Trial Register Center (ClinicalTrials.gov, NCT06522048). Strengthening the Reporting of Observational Studies in Epidemiology Standards were followed in conducting this study. Written informed consent was obtained from every patient for the publication of their medical information. All data was anonymized to protect patient confidentiality.
Inclusion and Exclusion Criteria
Detailed patient records for SJS/TEN were available in the dermatology inpatient department according to the following inclusion criteria: 1) diagnosis of SJS/TEN induced by either ICI or non-ICI drugs, confirmed by skin histopathology; 2) Chinese Han nationality; and 3) availability of comprehensive medical records and exemplary photos for review. Exclusion criteria include: 1) incomplete medical records; 2) withdrawal from the study prior to data collection; and 3) unknown culprit drugs.
Clinical Data Collection
Primarily clinical data were meticulously collected, including demographics, detailed clinical information associated with SJS/TEN, family and medical history, complications (including diabetes, hypoproteinemia, hypertension, and hepatitis), allergic history, detailed drug exposure, latency period, laboratory examinations (including complete blood count, liver function tests, and other relevant biomarkers at admission), therapeutic interventions, and outcomes. Additional data included the severity of SJS/TEN, which was rated using the SCORTEN scale (Supplementary Table S2), 18 the severity of mucosal damage quantified with the World Health Organization’s (WHO) grading for oral mucositis,19 and the grading system for ocular involvement proposed by Sotozono et al as detailed in Supplementary Table S3. 20 The missing values were replaced by the mean or median values for continuous variables with missing values less than 5%.21 Variables missing more than 20% were removed from this analysis. All variables were extracted from electronic medical records and verified by two independent reviewers. Photographs of skin and mucosa lesions were taken for all patients.
For the literature review, clinical data were extracted based on available information, focusing on gender, age, latency period, SCORTEN, specific ICIs and cancers, treatment methods, therapy outcomes, and BSA.
Statistical Analysis
Data were collected and recorded by Microsoft Excel version 2023, and analysis was performed using R 4.2.1 (http://www.Rproject.org; The R Foundation, Vienna, Austria) and the Free Statistics software (version 1.9.2; Beijing Free Clinical Medical Technology Co., Ltd., Beijing, China). Descriptive statistics were used to summarize the demographic and clinical characteristics of the patients. Continuous variables were expressed as mean ± standard deviation (SD) or median with interquartile range (IQR), depending on the distribution, while categorical variables were summarized as frequencies and percentages. Nighty five-percent confidence intervals (95% CIs) are used to characterize prevalence. To compare the clinical factors between the two groups, independent t-tests (for normally distributed variables) or Mann–Whitney U-tests (for non-normally distributed variables) were used. Chi-square or Fisher’s exact tests were applied for categorical data.
Multivariable regression analysis was utilized to investigate the association between the types of culprit drugs and the area of epidermal detachment, latency period, and the severity of oral and ocular mucositis, adjusting potential confounders. The significance level for all statistical tests was a two-sided P-value of less than 0.05.
Results
Demographic and Clinical Characteristics of SJS/TEN Patients in Our Center
A total of 179 patients with SJS/TEN were initially considered for this study; however, thirty-one were excluded for various reasons: seventeen due to missing data, three lost to follow-up, ten with unknown sensitizing agents, and one who was not of Han Chinese ethnicity. Ultimately, the study enrolled 41 patients whose SJS/TEN was triggered by ICIs and 107 by non-ICI drugs. Figure 1 presents the study flowchart.
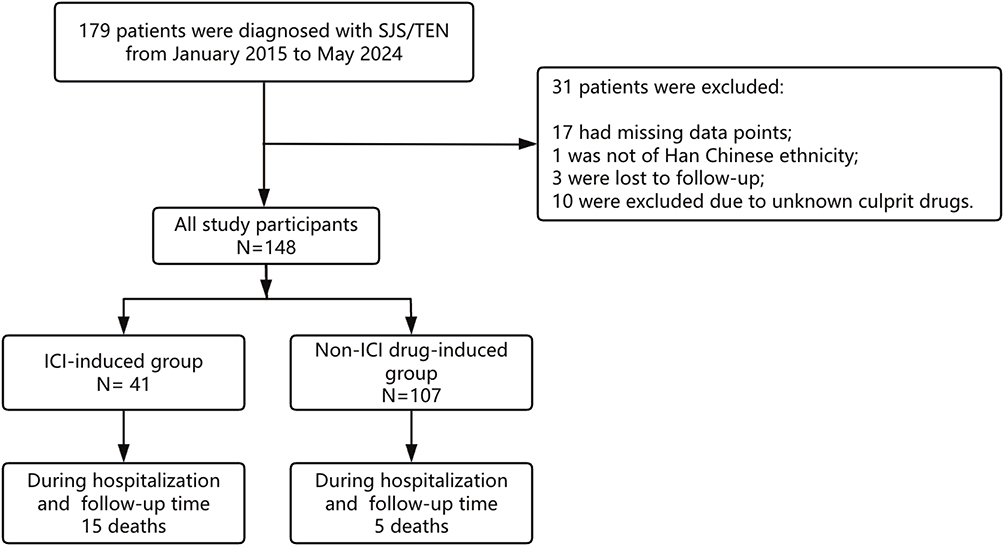 |
Figure 1 Flowchart of the study. Abbreviations: ICI, immune checkpoint inhibitor; SJS, Stevens-Johnson syndrome; TEN, toxic epidermal necrolysis. |
Among patients, 88 were males, representing 59.5%. The average age was 53.3 years, with a median of 55.5 years and a range from 42.8 to 66 years. The median latency period for the group induced by ICIs was 20 days (range: 10 to 45 days), while for those induced by non-ICI drugs, it was 7 days, ranging from 4 to 15.5 days. The mean SCORTEN score for the cohort was 2.7, with the ICI group recording a higher average of 3.5 compared to 2.4 in the non-ICI group. A total of 45 patients (30.4%) had a history of cancer. Among 148 patients, 21 (14.2%) had neoplasmic metastasis. The ICI-induced group recorded a mortality rate of 36.6% (15 deaths), whereas the non-ICI group reported a rate of 4.7% (5 deaths). Gastrointestinal (GI) cancer was the most prevalent type in the ICI-induced group, accounting for 46.3% of cases, followed by lung cancer at 39% and melanoma at 4.9%. In patients with SJS/TEN induced by ICIs, the distribution was 63.4% with SJS, 29.3% with SJS/TEN overlap syndrome, and 7.3% with TEN. Conversely, in the non-ICI group, the figures were 6.2% for SJS, 18.7% for SJS/TEN overlap syndrome, and 55.1% for TEN. No significant differences were observed in body mass index (BMI), temperature, or complications between the two groups. However, significant differences (p < 0.05) were found in gender, age, BSA, latency period, grading of ocular and oral mucositis, history of cancer, neoplasm metastasis, history of drug allergy, SCORTEN scores, mucosal damage, baseline neutrophil to lymphocyte ratio (NLR), eosinophil count, and C-reactive protein (CRP) levels between the two groups. Table 1 presents the comparison of baseline characteristics and health conditions of patients.
 |
Table 1 Baseline Epidemiological and Clinical Characteristics of SJS/TEN Patients in ICI and Non-ICI Drugs Groups in Our Center |
The predominant causative agents in the ICI group were PD-1 inhibitors (68.3%), PD-L1 inhibitors (7.3%), and a combination of PD-1 with CTLA4 inhibitors (24.4%). In contrast, the non-ICI group included NSAIDs (10.3%), antibiotics (29.9%), antiepileptic drugs (15%), urate-lowering therapy (ULT) (14%), and other medications (30.8%). Figure 2A and B show the specific culprit drugs for both groups. Of the 41 ICI-induced SJS/TEN cases at our hospital, almost all patients discontinued ICI therapy, except one who attempted a rechallenge with the ICI, which resulted in a recurrence of TEN.
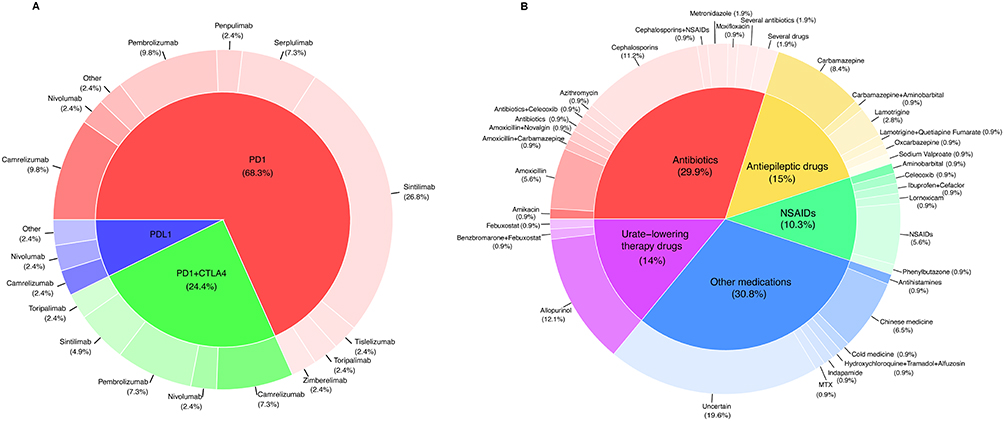 |
Figure 2 Doughnut charts illustrating the culprit drugs in SJS/TEN cases induced by ICIs and non-ICI drugs at our center. (A) Culprit drugs in 41 cases of SJS/TEN induced by ICIs at our center. (B) Culprit drugs in 107 cases of SJS/TEN induced by non-ICI drugs at our center. Abbreviations: SJS/TEN, Stevens-Johnson syndrome/toxic epidermal necrolysis; non-ICI, non-immune checkpoint inhibitor; CTLA4, cytotoxic T-lymphocyte associated protein 4; PD-L1, the programmed death ligand 1; PD-1, the programmed cell death receptor-1. |
Uni- and Multiple-Variable Analyses
Univariable analysis revealed significant differences in latency period, area of epidermal detachment (BSA), and severity of oral and ocular mucositis between groups (all P < 0.05; see Table 1). In the multivariable linear regression analysis, the SJS/TEN group induced by ICIs exhibited significantly less extensive epidermal detachment, with a mean difference of −40.68% (95% CI: −71.59% to −9.77%; P = 0.011) compared to the group induced by non-ICI drugs. This model was adjusted for age, gender, BMI, immunoglobulin E (IgE) levels, NLR, CRP, procalcitonin (PCT), complication, history of drug allergy, latency period, the number of suspected drugs, cancer history, and neoplasmic metastasis. Additionally, the ICI-induced group exhibited a trend toward a longer latency period of 17 days (95% CI: −1.49 to 35.48; P = 0.074), after adjustments for age, gender, BMI, history of drug allergy, number of suspected drugs, cancer history, and neoplasmic metastasis. Multivariable logistic regression analysis showed milder mucosal damage in the ICI-induced group compared to the non-ICI-induced group. Details are shown in Table 2.
 |
Table 2 Multivariable Regression Analysis of the Association Between Culprit Drugs and Clinical Manifestations in SJS/TEN: Severity of Epidermal Detachment, Latency Period, and Extent of Mucosal Involvement (Oral and Ocular), with Non-ICI Drug-Induced Cases as a Reference |
Subgroup Analysis
Our concurrent subgroup analysis of the prolonged latency period trend and BSA revealed no significant differences across various genders, ages, BMIs, and histories of drug allergies, with all interaction P-values exceeding 0.05, as shown in Figure 3.
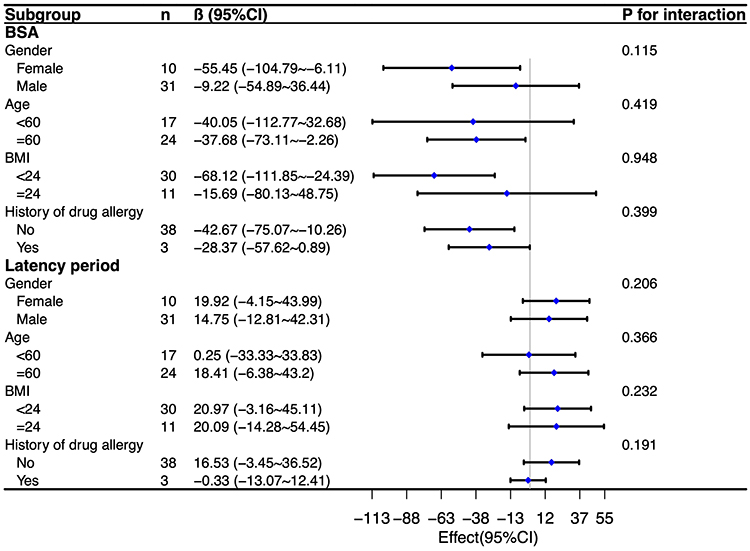 |
Figure 3 Subgroup analysis of the effects of types of culprit drugs on clinical presentation in SJS/TEN: association with the degree of epidermal detachment and the latency period. Abbreviations: 95% CI, 95% confidence interval; BSA, body surface area; BMI, body mass index; SJS, Stevens-Johnson syndrome; TEN, toxic epidermal necrolysis. |
Literature Review on Patients with ICI-Induced SJS/TEN
We present a descriptive analysis of 139 patients with ICI-induced SJS/TEN, including 98 cases previously reported and 41 unpublished cases from our institution, as detailed in Supplementary Table S1. Patients were categorized by diagnosis: SJS (55 patients, 39.6%), SJS/TEN overlap syndrome (37 patients, 26.6%), and TEN (47 patients, 33.8%). The average age was 62.0 ± 12.6 years, with 85 males (61.2%). Latency periods ranged from 1 day to 1095 days, with a median of 28.0 days. Among these patients, 20 (14.4%) received combination therapy with ICIs, with a mortality rate of 35.0% (7 deaths), compared to 22.7% (27 deaths) among the 119 patients on monotherapy (P = 0.012; see Supplementary Table S4). The overall mortality rate was 24.5%. The median total BSA involvement was 25%, ranging from 10% to 31%. No significant differences were observed between groups in age, latency period, ICI combination therapy, or types (P > 0.05). The mean SCORTEN score was 3.5, with a standard deviation of 1.1, with subgroup scores of 2.9 for SJS, 3.8 for the SJS/TEN overlap group, and 4.0 for TEN, showing significant differences among the three groups (P < 0.001; see Table 3 and Supplementary Table S5).
 |
Table 3 Demographics and Clinical Characteristics of ICI-Induced SJS/TEN Patients: Integrated Cases from Our Center and a Review of the Existing Literature |
The most common ICI associated with SJS/TEN was PD-1 inhibitor (112 cases, 80.6%), followed by a combination of PD-1 and CTLA4 inhibitors (20 cases, 14.4%), PD-L1 inhibitor (6 cases, 4.3%), and CTLA4 inhibitor alone (1 case, 0.7%). Mucosal damage was reported in 103 patients (74.1%), with oral and ocular mucosa damage noted in 79 (56.8%) and 59 (42.4%) patients, respectively. A preceding rash that evolved into epidermal necrosis was more common in deceased patients, occurring in 75 patients (54.0%). Pain and itching were reported by 69 (49.6%) and 45 (32.4%) patients, respectively. Pathological examination of skin tissue in 116 patients (83.5%) revealed common manifestations, including epidermal necrosis, apoptotic keratinocytes, inflammatory presentations, superficial perivascular involvement, and lichenoid or interface dermatitis. No statistical differences were observed in oral mucosal damage, pain, or itching across different groups (P > 0.05, Table 3). Among PD-1 inhibitors, pembrolizumab was the most prevalent, comprising 29.5% of cases. The most frequently occurring cancer was lung, accounting for 33.3% of cases, followed by gastrointestinal (GI) cancers (26.7%), melanoma (16.3%), and nasopharyngeal cancer (4.3%), with cervical, genitourinary (GU), lymphomas, renal, thymic cancers, cancers of uncertain origin, and two types of combination cancers also represented, as shown in Figure 4.
 |
Figure 4 Distribution of tumor types in SJS/TEN patients induced by ICI-associated drugs: based on an integrated analysis of data from our center and the literature review. Abbreviations: SJS/TEN, Stevens-Johnson syndrome/toxic epidermal necrolysis; ICIs, immune checkpoint inhibitors; GU, genitourinary; GI, gastrointestinal. |
Therapy Methods
In the group with ICI-induced SJS/TEN, treatment approaches were varied: 55 patients (39.6%) were treated solely with corticosteroids, while 28 patients (20.1%) received a combination of corticosteroids and intravenous immunoglobulin G (IVIG). Additionally, 9 patients (6.5%) were treated with a combination of corticosteroids and other immunosuppressants, including cyclosporine A (CsA) or tumor necrosis factor alpha inhibitors (anti-TNF-α). A smaller group of 7 patients (5.0%) received topical corticosteroids, conventional antihistamines, and symptomatic supportive therapy. Common treatment methods for ICI-induced SJS/TEN included systemic corticosteroid therapy, either alone or combined with IVIG or TNF-α inhibitors. However, the mortality rates for these treatments were 23.6% for corticosteroids alone, 28.6% for corticosteroids with IVIG, and 28.6% for combinations with other immunosuppressants, with no statistically significant statistical difference in outcomes between these approaches (P > 0.05). Details are available in Table 4 and Supplementary Table S6. Supplementary Table S7 presents the specific therapy methods of the non-ICI drug-induced SJS/TEN group.
 |
Table 4 Treatment Approaches for ICI-Induced SJS/TEN: a Combined Analysis Data from Our Center and Literature Review |
Discussion
The pathogenic mechanisms underlying classical SJS/TEN are complex and involve a dysregulated immune response where cytotoxic T cells and natural killer (NK) cells play an important role.22–24 Activated T cells infiltrate lesional skin, with CD4+ T cells predominating in the dermis and CD8+ T cells in the epidermis.25 The immune reaction induces widespread keratinocyte apoptosis, largely via granulysin secretion, a major mediator in SJS/TEN.26 Other mediators, such as Fas-Fas ligand (FasL) interactions and the perforin/granzyme B pathway, also contribute to keratinocyte death and epidermal detachment.27–29 Regarding ICI-induced SJS/TEN, while the specific pathogenesis remains to be fully elucidated, current hypotheses focus on the potential disruption of T-lymphocyte homeostasis in the skin and mucous membranes by ICIs.30 This disruption may lead to self-targeted cytotoxic and inflammatory reactions.
Clinical Comparison of ICI and Non-ICI-Induced SJS/TEN in Our Center
This was the first larger original study to compare the clinical characteristics of SJS/TEN patients induced by ICIs and non-ICIs. Our results indicate that ICI-induced SJS/TEN compares to non-ICI-induced cases with a tendency toward a longer latency period, a smaller affected BSA, and milder oral and ocular mucositis. These observations may reflect the distinct inflammatory mechanisms induced by ICIs. The delayed onset of symptoms in ICI-induced SJS/TEN is consistent with a previous retrospective cohort study17 and could be attributed to the unique mechanism by which ICIs modulate the immune system. Unlike SJS/TEN induced by non-ICI drugs, which can immediately react to a medication, ICI-induced reactions may have a longer latency period trend, potentially due to the disrupting T-lymphocyte homeostasis in the skin and mucous membranes.31 This latency suggests that ICIs may require a change in the internal environment or subsequent exposure to trigger an immune response.31 The tendency of prolonged latency period and the initially mild symptoms of ICI-induced SJS/TEN pose significant challenges for early diagnosis and treatment.9,32
An interesting finding among cases of ICI-induced SJS/TEN is that 63.4% were diagnosed with SJS, which involves minor epidermal detachment. In contrast, 55.1% of non-ICI-induced SJS/TEN cases were classified as TEN, indicating a higher prevalence of severe epidermal detachment. Previous immunohistochemical studies have noted an infiltration of CD8+ lymphocytes in the dermoepidermal layer of SJS/TEN induced by ICIs, with a relatively absence of CD14+ monocytes, contrasting with the substantial presence of both cell types in the blister fluid of non-ICI-induced SJS/TEN cases.31 In non-ICI-induced SJS/TEN, keratinocyte apoptosis is induced by the combined action of CD8+ lymphocytes and CD14+ monocytes.33,34 However, in ICI-induced SJS/TEN, keratinocyte apoptosis predominantly relies on CD8+ lymphocytes.31 This differential cellular infiltration may lead to the milder epidermal detachment observed in patients with ICI-induced SJS/TEN. Furthermore, it has been hypothesized that the milder severity of skin adverse reactions with ICIs may be related to increased tumor burden, reflecting an immunosuppressed state, potentially leading to decreased activation of anti-tumor T-cell activity.35 Therefore, ircAEs that occur following the initiation of ICI therapy are generally milder, and the risk of severe immune-related adverse events (irAEs) appears to be lower.36 Additionally, the genetic predispositions, particularly certain HLA-B alleles, which are known to influence the development of SJS/TEN,37 could also be implicated in the varied expression of disease severity and warrant further investigation in the context of ICI-induced SJS/TEN.
Our comparative study also underscores the importance of biomarkers such as NLR, and eosinophil counts in predicting outcomes in drug-induced SJS/TEN.38–40 These biomarkers reflect the underlying distinctions in the inflammatory response and immune system dynamics associated with each drug class,41 offering a potential prognostic tool in the management of these conditions.
Synthesizing and Analyzing Combined Data on ICI-Induced SJS/TEN from Our Center and the Literature
Our descriptive analysis of ICI-induced SJS/TEN cases, integrating data from previously reported literature with our center, offers new insight into the epidemiology and clinical characteristics of these adverse events. The observed lower rate of oral mucosal damage and slightly higher rate of ocular mucosal damage in our study compared to previous reports may reflect the differences in sample sizes and populations studied.42 An important finding was the higher SCORTEN scores and a trend toward higher in-hospital mortality rates among ICI-induced TEN patients at admission. Notably, patients with SJS/TEN induced by ICI combination therapy had increased mortality rates during hospitalization compared to those with ICI monotherapy. Previous studies have suggested that combination ICI therapy may enhance immune activation via checkpoint inhibition, potentially exacerbating the severity and mortality of SJS/TEN.43 The enhanced immune response through checkpoint inhibition may cause more frequent and severe irAEs among patients on combined ICI therapy.14
Our study presented a lower mortality rate in ICI-induced SJS/TEN patients than previously reported.12,14 This discrepancy may be attributed to advancements in medical practices, improved treatment protocols, and the improved identification and management of risk factors, contributing to the observed decrease in mortality. While our findings suggest a positive trend, it is important to recognize the limitations of our study and the need for further research for validation and an exploration into the causes of the reduction in mortality.
The analysis of these data reveals the association of specific ICIs, particularly PD-1 inhibitors such as pembrolizumab, with life-threatening skin adverse reactions.12,14 The higher mortality rates of ICI-related SJS/TEN highlight the importance of early identification and prompt treatment of severe skin reactions,44 especially in patients with lung cancer, GI cancers, and melanoma treated with these inhibitors. These insights can help physicians make more informed treatment decisions and potentially optimize therapeutic regimens for cancer patients.
Treatment Options for ICI-Induced SJS/TEN
Systemic corticosteroids have been well documented as the primary treatment for ICI-induced SJS/TEN.45,46 Our review of treatment methods from our institution and the literature revealed various therapeutic approaches, including corticosteroids monotherapy and combination therapies with TNF-α inhibitors, IVIG, CsA, or methotrexate (MTX).4,47–50 The management of ICI-induced SJS/TEN in our study predominantly involved systemic corticosteroids, with or without additional immunosuppressive agents. The absence of a statistically significant difference in mortality between patients treated with corticosteroids alone and those receiving combined therapy suggests therapeutic complexity. This finding was contrasted with previous suggestions that combining adalimumab with corticosteroids may improve treatment efficacy by enhancing anti-inflammatory effects and reducing corticosteroid-related adverse reactions.50 Instead, our results were consistent with Satoh TK et al’s observation of no significant benefit from adding TNF-α inhibitors to corticosteroid therapy,14 highlighting the complex mechanism of ircAEs and the potential impact of immune pathway modulation by TNF-α inhibitors.51 Despite their design to suppress pro-inflammatory cytokines, these agents may not always produce beneficial effects in severe ICI-related dermatologic toxicities. Our study underscores the complexity of clinical management and the need for individualized treatment approaches based on a deeper understanding of immunopathogenesis. By summarizing the diversity of therapeutic strategies, our research provided a valuable reference for dermatologic oncologists and might contribute to the development of more targeted and effective treatments for severe ircAEs.
Limitations
There are several limitations in this retrospective study. Firstly, the reliance on clinical records and literature reviews might lead to bias in data completeness and accuracy. Secondly, the results might predominantly reflect the characteristics of Chinese patients. Additionally, there may be pharmacogenetics and environmental heterogeneity that can influence the manifestation and outcomes of these severe cutaneous adverse reactions. Finally, future multi-center, prospective studies with larger sample sizes will be necessary to confirm our findings and assess the applicability of these findings to other geographical areas.
Conclusion
Our study offered the largest comparative analysis of ICI-induced versus non-ICI-induced SJS/TEN, revealing distinct clinical features and potential immunopathogenic differences. ICI-induced SJS/TEN patients exhibited a smaller affected BSA, a prolonged latency period trend, and milder oral and ocular mucositis. By integrating cases from the literature and our center, we described the epidemiology, clinical presentation, and therapeutic strategies of ICI-induced SJS/TEN. These insights enhance our understanding of the complex immune pathways in severe ircAEs associated with ICI therapy, potentially contributing to the development of more targeted and effective treatment strategies.
Data Sharing Statement
The original contributions presented in the study are included in the article/Supplementary material. Further inquiries can be directed to the corresponding authors.
Statement of Ethics and Consent to Participate
The study protocol complied with the Declaration of Helsinki and received approval from the Research Ethical Committee of the First Affiliated Hospital of FJMU (Ethical Committee Number: MRCTA, ECFAH of FMU [2023] 400). Additionally, it was registered at the Chinese Clinical Trial Register Center (ClinicalTrials.gov Identifier: NCT06522048). Written informed consent was obtained from each participant. Patients signed informed consent regarding publishing their data in a journal article.
Acknowledgments
We would like to express our gratitude to physicians who recommended SJS/TEN patients to our institution and contributed to this article.
Author Contributions
Chao Ji and Bo Cheng are co-corresponding authors. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by National Natural Science Foundation of China (No. 82373469) and Joint Funds for the Innovation of Science and Technology, Fujian Province (No. 2020Y9120).
Disclosure
The authors have no relevant financial or non-financial interests to disclose.
References
1. Gerull R, Nelle M, Schaible T. Toxic epidermal necrolysis and Stevens-Johnson syndrome: a review. Crit Care Med. 2011;39(6):1521–1532. doi:10.1097/CCM.0b013e31821201ed
2. Roujeau JC, Kelly JP, Naldi L, et al. Medication use and the risk of Stevens-Johnson syndrome or toxic epidermal necrolysis. N Engl J Med. 1995;333(24):1600–1607. doi:10.1056/NEJM199512143332404
3. Phillips EJ, Chung WH, Mockenhaupt M, Roujeau JC, Mallal SA. Drug hypersensitivity: pharmacogenetics and clinical syndromes. J Allergy Clin Immun. 2011;127(3 Suppl):S60–66. doi:10.1016/j.jaci.2010.11.046
4. Zhang J, Lu CW, Chen CB, et al. Evaluation of combination therapy with etanercept and systemic corticosteroids for Stevens-Johnson syndrome and toxic epidermal necrolysis: a multicenter observational study. J Allergy Clin Immunol Pract. 2022;10(5):1295–1304.e6. doi:10.1016/j.jaip.2022.01.038
5. Gronich N, Maman D, Stein N, Saliba W. Culprit medications and risk factors associated with Stevens-Johnson syndrome and toxic epidermal necrolysis: population-based nested case-control study. Am J Clin Dermatol. 2022;23(2):257–266. doi:10.1007/s40257-021-00661-0
6. Jun I, Rim JH, Kim MK, et al. Association of human antigen class I genes with cold medicine-related Stevens-Johnson syndrome with severe ocular complications in a Korean population. Brit J Ophthalmol. 2019;103(4):573–576. doi:10.1136/bjophthalmol-2018-313263
7. Ferrara R, Imbimbo M, Malouf R, et al. Single or combined immune checkpoint inhibitors compared to first-line platinum-based chemotherapy with or without bevacizumab for people with advanced non-small cell lung cancer. Cochrane Db Syst Rev. 2021;4(4):CD013257. doi:10.1002/14651858.CD013257.pub3
8. Buchbinder EI, Desai A. CTLA-4 and PD-1 pathways: similarities, differences, and implications of their inhibition. Am J Clin Oncol. 2016;39(1):98–106. doi:10.1097/COC.0000000000000239
9. Zhu J, Chen G, He Z, et al. Stevens-Johnson syndrome/toxic epidermal necrolysis in patients treated with immune checkpoint inhibitors: a safety analysis of clinical trials and FDA pharmacovigilance database. EClinicalMedicine. 2021;37:100951. doi:10.1016/j.eclinm.2021.100951
10. Huang Y, Zhu L, Ma X, et al. A case of sintilimab-induced SJS/TEN:dermatologic adverse reactions associated with programmed cell death protein-1 inhibitors. Dermatol Ther. 2022;35(9):e15663. doi:10.1111/dth.15663
11. Logan IT, Zaman S, Hussein L, Perrett CM. Combination therapy of ipilimumab and nivolumab-associated toxic epidermal necrolysis (TEN) in a patient with metastatic melanoma: a case report and literature review. J Immunother. 2020;43(3):89–92. doi:10.1097/CJI.0000000000000302
12. Bray ER, Lin RR, Li JN, Elgart GW, Elman SA, Maderal AD. Immune checkpoint inhibitor associated epidermal necrosis, beyond SJS and TEN: a review of 98 cases. Arch Dermatol Res. 2024;316(6):233. doi:10.1007/s00403-024-03061-6
13. Salati M, Pifferi M, Baldessari C, et al. Stevens-Johnson syndrome during nivolumab treatment of NSCLC. Ann Oncol off J Eur Soc Med Oncol. 2018;29(1):283–284. doi:10.1093/annonc/mdx640
14. Satoh TK, Neulinger MM, Stadler PC, Aoki R, French LE. Immune checkpoint inhibitor-induced epidermal necrolysis: a narrative review evaluating demographics, clinical features, and culprit medications. J Dermatol. 2024;51(1):3–11. doi:10.1111/1346-8138.17039
15. Ozhathil DK, Powell CM, Corley CV, et al. A retrospective analysis of mortality risk and immunosuppressive therapy for Stevens-Johnson syndrome and toxic epidermal necrolysis syndrome using the TriNetX research network. Burns: J Int Soc Burn Inj. 2024;50(1):75–86. doi:10.1016/j.burns.2023.08.009
16. Lin CC, Chen CB, Wang CW, Hung SI, Chung WH. Stevens-Johnson syndrome and toxic epidermal necrolysis: risk factors, causality assessment and potential prevention strategies. Expert Rev Clin Immunol. 2020;16(4):373–387. doi:10.1080/1744666X.2020.1740591
17. Chen A, Kolodney JA, Kolodney MS. Retrospective cohort study characterizing PD-1/PD-L1 checkpoint inhibition associated Stevens-Johnson syndrome and toxic epidermal necrolysis. J Am Acad Dermatol. 2024;S0190-9622(24):1003–1005. doi:10.1016/j.jaad.2024.06.066
18. Bastuji-Garin S, Fouchard N, Bertocchi M, Roujeau JC, Revuz J, Wolkenstein P. SCORTEN: a severity-of-illness score for toxic epidermal necrolysis. J Invest Dermatol. 2000;115(2):149–153. doi:10.1046/j.1523-1747.2000.00061.x
19. Sonis ST, Elting LS, Keefe D, et al. Perspectives on cancer therapy-induced mucosal injury: pathogenesis, measurement, epidemiology, and consequences for patients. Cancer-Am Cancer Soc. 2004;100(9 Suppl):1995–2025. doi:10.1002/cncr.20162
20. Sotozono C, Ueta M, Nakatani E, et al. Predictive factors associated with acute ocular involvement in Stevens-Johnson syndrome and toxic epidermal necrolysis. Am J Ophthalmol. 2015;160(2):228–237.e2. doi:10.1016/j.ajo.2015.05.002
21. Shen Y, Zhang W, Shen Y. Early diuretic use and mortality in critically ill patients with vasopressor support: a propensity score-matching analysis. Crit Care. 2019;23(1):9. doi:10.1186/s13054-019-2309-9
22. Nassif A, Bensussan A, Boumsell L, et al. Toxic epidermal necrolysis: effector cells are drug-specific cytotoxic T cells. J Allergy Clin Immun. 2004;114(5):1209–1215. doi:10.1016/j.jaci.2004.07.047
23. Le Cleach L, Delaire S, Boumsell L, et al. Blister fluid T lymphocytes during toxic epidermal necrolysis are functional cytotoxic cells which express human natural killer (NK) inhibitory receptors. Clin Exp Immunol. 2000;119(1):225–230. doi:10.1046/j.1365-2249.2000.01119.x
24. Correia O, Delgado L, Ramos JP, Resende C, Torrinha JA. Cutaneous T-cell recruitment in toxic epidermal necrolysis. Further evidence of CD8+ lymphocyte involvement. Arch Dermatol. 1993;129(4):466–468. doi:10.1001/archderm.1993.01680250078010
25. Rzany B, Hering O, Mockenhaupt M, et al. Histopathological and epidemiological characteristics of patients with erythema exudativum multiforme major, Stevens-Johnson syndrome and toxic epidermal necrolysis. Brit J Dermatol. 1996;135(1):6–11.
26. Borchers AT, Lee JL, Naguwa SM, Cheema GS, Gershwin ME. Stevens-Johnson syndrome and toxic epidermal necrolysis. Autoimmun Rev. 2008;7(8):598–605. doi:10.1016/j.autrev.2008.06.004
27. Abe R, Shimizu T, Shibaki A, Nakamura H, Watanabe H, Shimizu H. Toxic epidermal necrolysis and Stevens-Johnson syndrome are induced by soluble fas ligand. Am J Pathol. 2003;162(5):1515–1520. doi:10.1016/S0002-9440(10)64284-8
28. Nassif A, Moslehi H, Le Gouvello S, et al. Evaluation of the potential role of cytokines in toxic epidermal necrolysis. J Invest Dermatol. 2004;123(5):850–855. doi:10.1111/j.0022-202X.2004.23439.x
29. Viard I, Wehrli P, Bullani R, et al. Inhibition of toxic epidermal necrolysis by blockade of CD95 with human intravenous immunoglobulin. Sci. 1998;282(5388):490–493. doi:10.1126/science.282.5388.490
30. Saw S, Lee HY, Ng QS. Pembrolizumab-induced Stevens-Johnson syndrome in non-melanoma patients. Eur J Cancer. 2017;81:237–239. doi:10.1016/j.ejca.2017.03.026
31. Kimura H, Hasegawa A, Takei I, et al. Characteristic pathological features of keratinocyte death in a case of Stevens-Johnson syndrome manifested by an immune checkpoint inhibitor. J Eur Acad Dermatol Venereol JEADV. 2021;35(2):e142–e145. doi:10.1111/jdv.16872
32. Barvaliya M, Sanmukhani J, Patel T, Paliwal N, Shah H, Tripathi C. Drug-induced Stevens-Johnson syndrome (SJS), toxic epidermal necrolysis (TEN), and SJS-TEN overlap: a multicentric retrospective study. J Postgrad Med. 2011;57(2):115–119. doi:10.4103/0022-3859.81865
33. Chung WH, Hung SI. Recent advances in the genetics and immunology of Stevens-Johnson syndrome and toxic epidermal necrosis. J Dermatol Sci. 2012;66(3):190–196. doi:10.1016/j.jdermsci.2012.04.002
34. Saito N, Qiao H, Yanagi T, et al. An annexin A1-FPR1 interaction contributes to necroptosis of keratinocytes in severe cutaneous adverse drug reactions. Sci Transl Med. 2014;6(245):245ra95. doi:10.1126/scitranslmed.3008227
35. Asdourian MS, Otto TS, Jacoby TV, et al. Association between serum lactate dehydrogenase and cutaneous immune-related adverse events among patients on immune checkpoint inhibitors for advanced melanoma. J Am Acad Dermatol. 2022;87(5):1147–1149. doi:10.1016/j.jaad.2022.02.024
36. Pan CX, Lau WC, Kim DY, et al. Association between baseline lactate dehydrogenase and immune-related adverse events among patients with melanoma varies by tumor stage at immune checkpoint inhibitor initiation. J Am Acad Dermatol. 2023;89(6):1264–1268. doi:10.1016/j.jaad.2023.07.1029
37. Chung WH, Hung SI, Hong HS, et al. Medical genetics: a marker for Stevens-Johnson syndrome. Nature. 2004;428(6982):486. doi:10.1038/428486a
38. Primisawitri PP, Mawardi P. The correlation of neutrophil-lymphocyte ratio and eosinophil count with SCORTEN in SJS/TEN. Clin Cosmet Invest Dermatol. 2022;15:547–556. doi:10.2147/CCID.S356450
39. Chuenboonngarm N, Puaratanaarunkon T, Washrawirul C, et al. Key factors predicting the in-hospital mortality of patients with severe cutaneous adverse reactions in Thailand. J Eur Acad Dermatol Venereol JEADV. 2023;37(9):1881–1890. doi:10.1111/jdv.19222
40. Wang Q, Lan YP, Qi B, Yin L, Zhang LX, Liu W. Neutrophil: lymphocyte ratio is associated with disease severity and mortality in patients with Stevens-Johnson syndrome/toxic epidermal necrolysis. J Dermatol. 2021;48(9):1394–1400. doi:10.1111/1346-8138.15968
41. Pham JP, Wark KJL, Woods J, Frew JW. Resident cutaneous memory T cells: a clinical review of their role in chronic inflammatory dermatoses and potential as therapeutic targets. Brit J Dermatol. 2023;189(6):656–663. doi:10.1093/bjd/ljad303
42. Molina GE, Yu Z, Foreman RK, Reynolds KL, Chen ST. Generalized bullous mucocutaneous eruption mimicking Stevens-Johnson syndrome in the setting of immune checkpoint inhibition: a multicenter case series. J Am Acad Dermatol. 2020;83(5):1475–1477. doi:10.1016/j.jaad.2020.03.029
43. Wolchok JD, Chiarion-Sileni V, Gonzalez R, et al. Efficacy and safety results from a Phase III trial of nivolumab (NIVO) alone or combined with ipilimumab (IPI) versus IPI alone in treatment-naive patients (pts) with advanced melanoma (MEL) (CheckMate 067). J Clin Oncol. 2015;33(18_suppl):LBA1–LBA1. doi:10.1200/jco.2015.33.18_suppl.lba1
44. Sommerfelt H, Sandvik LF, Bachmann IM, et al. Toxic epidermal necrolysis after immune checkpoint inhibition, case report, and review of the literature. Acta Oncol Stockh Swed. 2022;61(10):1295–1299. doi:10.1080/0284186X.2022.2119099
45. Araki Y, Sotozono C, Inatomi T, et al. Successful treatment of Stevens-Johnson syndrome with steroid pulse therapy at disease onset. Am J Ophthalmol. 2009;147(6):1004–1011. doi:10.1016/j.ajo.2008.12.040
46. Fernando SL. The management of toxic epidermal necrolysis. Australas J Dermatol. 2012;53(3):165–171. doi:10.1111/j.1440-0960.2011.00862.x
47. Jacobsen A, Olabi B, Langley A, et al. Systemic interventions for treatment of Stevens-Johnson syndrome (SJS), toxic epidermal necrolysis (TEN), and SJS/TEN overlap syndrome. Cochrane Db Syst Rev. 2022;3(3):CD013130. doi:10.1002/14651858.CD013130.pub2
48. Creamer D, Walsh SA, Dziewulski P, et al. U.K. guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Brit J Dermatol. 2016;174(6):1194–1227. doi:10.1111/bjd.14530
49. Zimmermann S, Sekula P, Venhoff M, et al. Systemic immunomodulating therapies for Stevens-Johnson syndrome and toxic epidermal necrolysis: a systematic review and meta-analysis. JAMA dermatol. 2017;153(6):514–522. doi:10.1001/jamadermatol.2016.5668
50. Lin M, Gong T, Ruan S, et al. Emerging insights into Stevens-Johnson syndrome and toxic epidermal necrolysis induced by immune checkpoint inhibitor and tumor-targeted therapy. J Inflammation Res. 2024;17:2337–2351. doi:10.2147/JIR.S454673
51. Karagianni N, Kranidioti K, Fikas N, et al. An integrative transcriptome analysis framework for drug efficacy and similarity reveals drug-specific signatures of anti-TNF treatment in a mouse model of inflammatory polyarthritis. PLoS Comput Biol. 2019;15(5):e1006933. doi:10.1371/journal.pcbi.1006933
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.