")
Back to Journals » Orthopedic Research and Reviews » Volume 17
Clinical Outcome of Achilles Tendon Rupture Repaired by a Modified Minimally Invasive Percutaneous Suturing
Authors Qi X, Zheng D, Lei Z, Yu J, Qiu X, Chen Y
Received 9 July 2024
Accepted for publication 2 January 2025
Published 14 January 2025 Volume 2025:17 Pages 21—29
DOI https://doi.org/10.2147/ORR.S486218
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Xiaoyang Qi,1,* Danxia Zheng,2,* Zhijie Lei,3,* Jianglin Yu,3 Xusheng Qiu,1,3 Yixin Chen2
1Department of Orthopedics, Nanjing Drum Tower Hospital, The Affiliated Hospital of Nanjing University Medical School, Nanjing, Jiangsu Province, People’s Republic of China; 2Department of Orthopedics, Nanjing Drum Tower Hospital Clinical College of Nanjing University of Chinese Medicine, Nanjing, Jiangsu Province, People’s Republic of China; 3Department of Orthopedics, Nanjing Drum Tower Hospital Clinical College of Jiangsu University, Nanjing, Jiangsu Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yixin Chen, Department of Orthopedics, Nanjing Drum Tower Hospital, The Affiliated Hospital of Nanjing University Medical School, No. 321, Zhongshan Road, Nanjing, Jiangsu Province, 210000, People’s Republic of China, Tel +86 15005149964, Email [email protected]
Purpose: Minimally invasive percutaneous techniques offer a promising alternative to open surgical repair of the Achilles tendon. However, the possibilities of recurrent rupture and nerve complications remain. Hence, the present study was conducted to describe a modified repair technique for the Achilles tendon able to overcome these limitations.
Patients and Methods: This retrospective study included 36 patients with acute closed Achilles tendon rupture treated at our institution between January 2020 and January 2022. All patients underwent surgery at our institution and were followed up for 12– 25 months. Functional evaluation was based on the American Orthopedic Foot and Ankle Society (AOFAS) Ankle-Hindfoot Scale and the Achilles tendon total rupture score (ATRS), along with local complications.
Results: None of the patients had sural nerve injury, infection or re-rupture at a minimum follow up of 12 months. At the final follow-up, the average AOFAS ankle-hindfoot score and ATRS were 95.5 and 90.0, respectively. The final magnetic resonance imaging showed continuity and thicker regeneration of the tendon.
Conclusion: The modified percutaneous repair of the Achilles tendon is an effective procedure which yields good functional outcome with few complications, and it could be widely promoted in clinical practice.
Keywords: Achilles tendon, acute rupture, percutaneous repair, minimally invasive technique, clinical outcome
Introduction
The Achilles tendon, recognized as the strongest tendon in the human body, plays a pivotal role in facilitating movement by connecting the calf muscles to the heel bone. This tendon endures significant stress during activities such as walking, running, and jumping, making it susceptible to injuries, particularly ruptures. With the increased public awareness and the rise of competitive sports, Achilles tendon rupture (ATR) has become increasingly prevalent, affecting not only athletes but also the general population.1
The optimal treatment for acute ATR remains controversial. A multicenter, randomized, controlled trial showed that neither open repair surgery nor minimally invasive surgery resulted in better outcomes compared to non-surgical treatment at 12 months, but the non-surgical treatment had a higher re-rupture rate than surgical treatment (6.2% vs 0.6%).2 Non-surgical management aims to facilitate natural healing of the tendon. However, the biomechanical strength of the severed end is not guaranteed in non-surgically treated patients, functional exercise is relatively delayed, and tendon tone might be reduced, resulting in longer rehabilitation periods that might not meet patient expectations.3 Surgical treatment can significantly increase the rate of postoperative resumption of sports activities and result in improved ankle movement,4 which includes open repair surgery and minimally invasive technique. Traditional open repair surgery allows for direct visualization and precise repair of the rupture but carries risks like infection, skin necrosis, scarring, and prolonged recovery time.5
Percutaneous suturing technique, first proposed by Ma and Griffith, is a minimally invasive technique that has functional results similar to open repair, with few soft tissue related complications.6 However, the major problem with a percutaneous suturing technique is a high incidence of re-rupture and sural nerve injury.7–9 Some minimally invasive surgeries have subsequently been developed and improved to avoid the risk of nerve injury.10,11 Although the proportion of favorable outcomes is increasing, the possibilities of recurrent rupture and nerve complications remain.
This retrospective study described the application of a modified minimally invasive percutaneous technique for patients with acute ATR. The aim of the study is to assess the outcomes in modified percutaneous Achilles tendon repair, and to provide a reference for the promotion of this technique.
Patients and Methods
All data were collected from patients with acute and closed ATR who attended our hospital between January 2020 and January 2022. This study received approval from our hospital’s ethics committee (Approval number: 2024–392-01). The inclusion criteria were: (1) patients aged 18 years or older; (2) fresh ATR (≤14 days); and (3) complete follow-up data. The exclusion criteria included: (1) open rupture; (2) tendon insertion rupture; (3) treatment with steroid or quinolone drugs; and (4) re-rupture. The patient flow diagram is presented in Figure 1. ATR was diagnosed by the surgeon based on magnetic resonance imaging (MRI) and physical examination findings (Figure 2). Positive Thompson test results were used to confirm the diagnosis of ATR, and MRI identified the precise location of the tear. All patients were followed up through clinic visits and telephone calls with our surgeon.
 |
Figure 1 Flow diagram of patient enrollment. |
 |
Figure 2 Acute Achilles tendon rupture of a 37-year-old man. (A) Appearance of Achilles tendon rupture. (B) Dorsiflexion of the injured side. (C) Plantar flexion of the injured side. (D) Preoperative MRI showing Achilles tendon rupture. |
Surgical Technique
The patients underwent surgery under general anesthesia and in the prone position with a thigh tourniquet. A 2- to 3-cm median parainternal longitudinal incision was performed at the site of ATR. The proximal and distal stumps of the Achilles tendon were exposed through the incision. An artery forceps was inserted in the space between the peritendinous membrane and Achilles tendon to blunt dissection, facilitating insertion of the right-angle forceps.
From a point 3 cm above the lower edge of the defect, a needle loaded with a No. 1 Ethibond suture was percutaneously passed from the lateral to medial side. Then a right-angle forceps was introduced in the space between the peritendinous membrane and Achilles tendon to pull the sutures through the incision. At a point 2 cm proximal to the rupture site, the needle was inserted obliquely towards the initial insertion point and passed percutaneously. The suture was drawn out again using the right-angle forceps. This process was repeated on the opposite side. The needle was inserted at a point 2 cm proximal to the rupture site on the contralateral side, angled obliquely towards the initial exit point. The suture was again drawn out using the right-angle clamp. Similarly, the same procedure was repeated on the distal stump of the ruptured Achilles tendon.
After all sutures were passed through, each end of the sutures was tied with three surgical knots in a 20° plantarflexed position of the ankle joint. The tails of the stumps were reset, and the suture knots were buried in a deeper position underneath the peritendinous membrane to prevent irritation. A 2–0 absorbable suture was used to perform a continuous interlocking suture at the rupture site to provide additional integrity and stability. Subsequently, the peritendinous membrane and subcutaneous tissue were closed with a 2–0 absorbable suture and the skin incision with a 3–0 absorbable suture. All surgeries were performed by the same senior surgeon. Figure 3 demonstrates the schematic diagrams of the modified minimally invasive percutaneous technique for the ATR. The procedure performed in a 37-year-old man is shown in Figure 4.
 |
Figure 3 Schematic diagrams of the modified minimally invasive percutaneous technique. (A) The suture is passed from the lateral to medial side. (B) The right-angle forceps is introduced in the space between the peritendinous membrane and Achilles tendon to pull the suture through the incision. (C) The suture is inserted obliquely towards the initial insertion point and drawn out using the right-angle forceps. (D) The same procedure is repeated on the distal stump of the ruptured Achilles tendon. (E) The proximal and distal sutures are tied underneath the peritendinous membrane with the ankle in 20° of plantar flexion. (F) A continuous interlocking suture at the rupture site in the incision. |
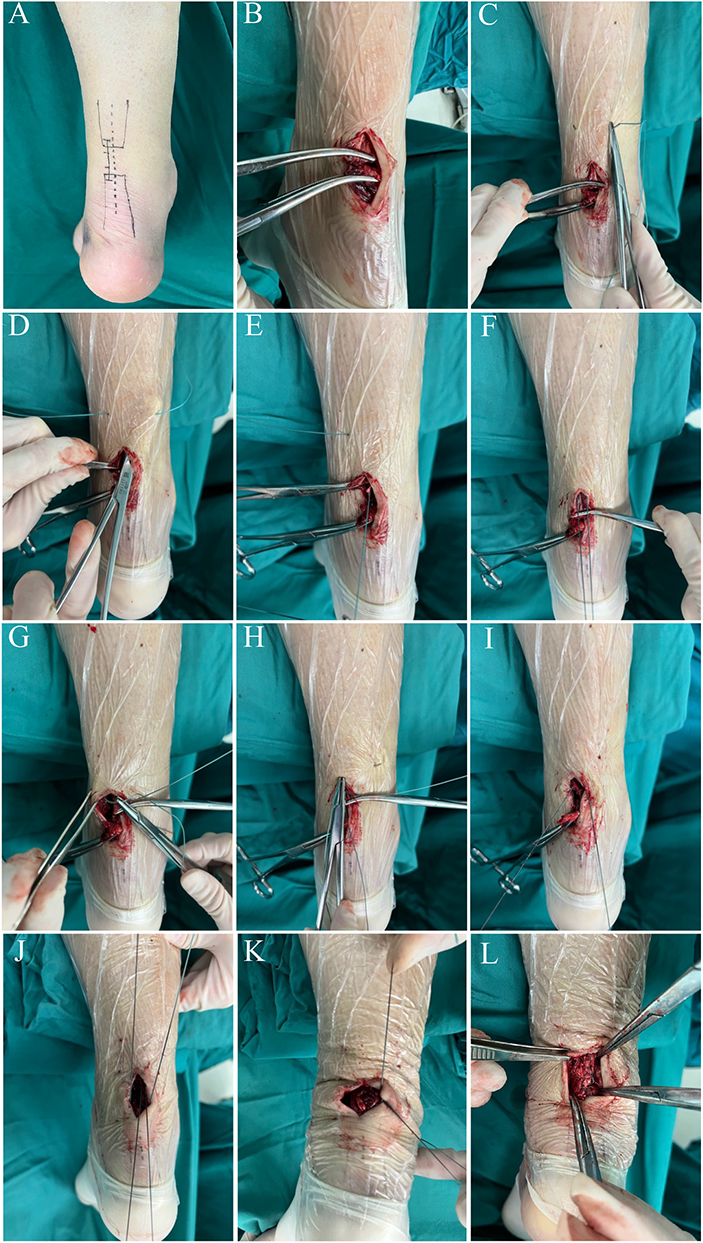 |
Figure 4 Diagrams of surgical procedure. (A) The location of the ends and the incision. (B) The proximal and distal stumps of the Achilles tendon were pulled out from the incision. (C) Loaded with No. 1 Ethibond suture, the needle is inserted percutaneously. (D–F) After bluntly dissect the space between the peritendinous membrane and Achilles tendon by an artery forceps, the right-angle forceps is introduced in the space to pull the suture. (G–I) At a point 2 cm proximal to the rupture site, the suture is inserted obliquely towards the initial insertion point and drawn out using the right-angle forceps. This process is repeated on the opposite side. (J) The same procedure is repeated on the distal stump of the ruptured Achilles tendon. (K) The proximal and distal sutures are tied underneath the peritendinous membrane with the ankle in 20° of plantar flexion. (L) Rupture site is enhanced by the continuous interlocking suture. |
Postoperative Rehabilitation and Follow-up
A polymer short leg cast in 20° of plantar flexion was applied, with weight-bearing restricted for 4 weeks. 4 weeks after surgery, the Achilles tendon shoe with adjustable range of motion was applied, the fixed angle of the ankle was gradually reduced by approximately 5° per week until it was adjusted to a neutral position at 8 weeks, and the shoe was removed. Then, the subjects could perform weight-bearing and daily activities. After 12 weeks, the subjects could gradually return to light sports activities.
All patients were followed up regularly for 12–25 months (mean:13.1 months). The operation time and the average postoperative hospital stay were recorded. During follow-up, physical examination was conducted, and the sural nerve sensation was assessed to determine the presence of any injury. The occurrence of complications, such as infection, re-rupture, and sural nerve injury, was documented. At 6 months after surgery, MRI scans of the ankle were obtained to visually evaluate the healing of the Achilles tendon. Clinical results were evaluated using the American Orthopaedic Foot and Ankle Society (AOFAS) ankle-hindfoot functional score and the Achilles Tendon Total Rupture Score (ATRS).12,13
Statistical Analysis
SPSS software (version 26.0; IBM, Corp.) were used for the statistical analysis. The data were presented as mean values ± SD.
Results
Demographic and Surgical Information
A total of 36 patients were included in this study (35 males and 1 female), ranging in age from 23 to 59 years (mean 37.5 ± 8.5 years). One patient experienced the left ATR one year following minimally invasive percutaneous repair of the right ATR. The injury modalities were categorized as sports-related injuries (31 cases, 83.8%), sprains (5 cases, 13.5%), and falls (1 case, 2.7%). The average time from injury to surgery was 5.8 ± 3.0 days (Table 1). The mean operation time was 35.4 ± 5.8 min. The postoperative hospital stay was 3.3 ± 0.7 days (Table 2).
 |
Table 1 Demographics of Patients |
 |
Table 2 Clinical Results After Surgery |
Postoperative Functional Assessment
The follow-up period was 13.1 ± 2.3 months. The MRI showed continuity and thicker regeneration of the Achilles tendon, which had been properly repaired and shaped at 6 months after the operation (Figure 5). At the final follow-up, the mean AOFAS ankle-hindfoot score was 95.5 ± 3.7, the mean ATRS was 90.0 ± 3.2 (Table 2).
 |
Figure 5 Repaired ruptured Achilles tendon of 37-year-old man. (A) Appearance of tendon with heel raised. (B) Postoperative plantar flexion of the injured side. (C) Postoperative dorsiflexion of the injured side. (D) Postoperative MRI showing continuity and thicker regeneration of the Achilles tendon. |
Postoperative Complications
No sural nerve injury, infection or re-rupture was observed during surgery or during the follow-up visits.
Discussion
The present study demonstrates that the minimally invasive percutaneous technique for ATR yields good clinical outcomes with few complications. The postoperative AOFAS ankle-hindfoot score and ATRS indicate substantial levels of functional recovery. No wound complications were observed in this study, which may be attributed to less injury to the peritendinous membrane. The peritendinous membrane can prevent superficial infection spreading into the deep layers and ensures a valuable blood supply to the repaired tendon. Another reason is the operation time, the mean operation time was 35.4 ± 5.8 min, including the time for polymer plaster casting. In addition, we located the suture knots outside the repaired tendon, minimizing the disruption of the blood supply to the tendon. Previous studies have highlighted the advantages of reduced scarring, lower infection rates, less nerve injury, and faster recovery times with minimally invasive approaches.14,15 Our study further substantiates these benefits by showing a complete absence of postoperative complications.
Avoiding sural nerve injury is critical in Achilles tendon repair due to its proximity to the surgical site. Studies have shown that sural nerve injuries can lead to chronic pain and functional impairments, underscoring the importance of techniques that prioritize nerve preservation.16,17 The sural nerve travels in the lower 1/3 of the calf with significant variability and exhibits an extremely variable relationship with the Achilles tendon.18 Our technique’s emphasis on careful needle entry point after the blunt dissection in the space between the peritendinous membrane and Achilles tendon significantly mitigates this risk of inadvertently injuring the sural nerve. During surgery, the needle entry point was selected, and the angle of needle penetration was adjusted to avoid the nerve travel area. Simultaneously, surgery was performed mainly underneath the peritendinous membrane, which lessen the likelihood of sural nerve entrapment. In this study, the patients did not experience any sural nerve entrapment.
In this study, Achilles tendon repair was conducted by the crossed divergent suturing. This method requires only right-angle forceps, which on only simplifies the procedure but also enhances its economically attractive. Unlike the Achillon system and the Percutaneous Achilles Repair System requiring specialized equipment,19,20 this technique can be easily adopted in diverse clinical settings, making it particularly valuable in poor medical environments. For the treatment of the severed end, the distal and proximal ends were combed and drawn out at the small incision. A continuous interlocking suture was applied at the rupture site to provide additional reinforcement and effectively align the tendon ends. This suture configuration was specifically adapted to accommodate the constraints of the minimally invasive technique, ensuring adequate biomechanical support without compromising the procedure’s efficiency. This can enhance the structural integrity and mechanical strength of the tendon tissue at the rupture.
The median parainternal longitudinal incision was applied in our technique, contrasting with the transverse incision reported in the literatures.14,15 As is well known, the proximal end of the tear retracts as the muscles contract when an ATR occurs.21 The median parainternal longitudinal incision, being offset from the ATR site, minimizes direct trauma to the ruptured area and reduces the risk of wound complications. This approach avoids critical neurovascular structures that are more commonly encountered in the posterior and lateral regions. It reduces the risk of nerve damage, particularly to the sural nerve. This approach also allows for better visualization and handling of the tendon ends, facilitating precise suture placement, rupture ends alignment and tension adjustment. In addition, it also mitigates local discomfort and issues with shoe-wearing due to adhesions or scar contractures.
While our study provides strong evidence supporting the efficacy and safety of the minimally invasive percutaneous technique, future research should aim to address some limitations. Larger, multicenter trials with longer follow-up periods are necessary to further validate these findings and ensure their generalizability across diverse patient populations. And further comparative studies needed to confirm its superiority against the other techniques. Additionally, investigating the long-term biomechanical properties of the repaired tendons and comparing it with those treated with other techniques will provide deeper insights into the durability and functionality of the minimally invasive approach. Finally, this study did not systematically control for patients’ activity levels or Body Mass Index (BMI) during the postoperative period. Although personalized recommendations were provided during follow-ups, variations in activity levels and BMI may influence the risk of re-rupture and functional outcomes. Future studies should consider incorporating standardized protocols to control these factors and assess their impact on long-term recovery and complications.
Conclusion
The modified minimally invasive percutaneous technique for acute ATR provided a strong repair and yields good clinical outcome with few complications. Since no special instrument is required, this technique could be widely promoted in clinical practice.
Institutional Review Board Statement
Our study complies with the Declaration of Helsinki. This study was approved by the Ethics Committee of Nanjing Drum Tower Hospital, The Affiliated Hospital of Nanjing University Medical School (Approval number: 2024-392-01).
Informed Consent Statement
Informed consent was obtained from all the participants.
Data Sharing Statement
The clinical and imaging datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Key Project supported by Nanjing Municipal Health Bureau (grant no. ZKX21029).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gross CE, Nunley JA. Acute Achilles tendon ruptures. Foot Ankle Int. 2016;37(2):233–239. doi:10.1177/1071100715619606
2. Myhrvold SB, Brouwer EF, Andresen TKM, et al. Nonoperative or surgical treatment of acute Achilles’ tendon rupture. N Engl J Med. 2022;386(15):1409–1420. doi:10.1056/NEJMoa2108447
3. Wong J, Barrass V, Maffulli N. Quantitative review of operative and nonoperative management of achilles tendon ruptures. Am J Sports Med. 2002;30(4):565–575. doi:10.1177/03635465020300041701
4. Cetti R, Christensen SE, Ejsted R, Jensen NM, Jorgensen U. Operative versus nonoperative treatment of Achilles tendon rupture. A prospective randomized study and review of the literature. Am J Sports Med. 1993;21(6):791–799. doi:10.1177/036354659302100606
5. Gatz M, Driessen A, Eschweiler J, Tingart M, Migliorini F. Open versus minimally-invasive surgery for Achilles tendon rupture: a meta-analysis study. Arch Orthop Trauma Surg. 2021;141(3):383–401. doi:10.1007/s00402-020-03437-z
6. Ma GW, Griffith TG. Percutaneous repair of acute closed ruptured achilles tendon: a new technique. Clin Orthop Relat Res. 1977;128:247–255.
7. Aibinder WR, Patel A, Arnouk J, et al. The rate of sural nerve violation using the Achillon device: a cadaveric study. Foot Ankle Int. 2013;34(6):870–875. doi:10.1177/1071100712473097
8. Lansdaal JR, Goslings JC, Reichart M, et al. The results of 163 Achilles tendon ruptures treated by a minimally invasive surgical technique and functional aftertreatment. Injury. 2007;38(7):839–844. doi:10.1016/j.injury.2006.12.010
9. Metz R, van der Heijden GJ, Verleisdonk EJ, Kolfschoten N, Verhofstad MH, van der Werken C. Effect of complications after minimally invasive surgical repair of acute achilles tendon ruptures: report on 211 cases. Am J Sports Med. 2011;39(4):820–824. doi:10.1177/0363546510392012
10. Chen H, Ji X, Zhang Q, Liang X, Tang P. Channel-assisted minimally invasive repair of acute Achilles tendon rupture. J Orthop Surg Res. 2015;10:167. doi:10.1186/s13018-015-0310-9
11. Ding WG, Zhu YP, Yan WH. Treatment of acute and closed Achilles tendon ruptures by minimally invasive tenocutaneous suturing. J Foot Ankle Surg. 2013;52(2):143–146. doi:10.1053/j.jfas.2012.12.006
12. Kitaoka HB, Alexander IJ, Adelaar RS, Nunley JA, Myerson MS, Sanders M. Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes. Foot Ankle Int. 1994;15(7):349–353. doi:10.1177/107110079401500701
13. Nilsson-Helander K, Thomeé R, Silbernagel KG, et al. The Achilles tendon Total Rupture Score (ATRS): development and validation. Am J Sports Med. 2007;35(3):421–426. doi:10.1177/0363546506294856
14. Calder JD, Saxby TS. Early, active rehabilitation following mini-open repair of Achilles tendon rupture: a prospective study. Br J Sports Med. 2005;39(11):857–859. doi:10.1136/bjsm.2004.017509
15. Xu L, Jin J, Liu Z, et al. A new technique of Achilles tendon rupture repaired by double transverse mini-incision to avoid sural nerve injury: a consecutive retrospective study. Orthop Surg. 2023;15(2):517–524. doi:10.1111/os.13615
16. Li Y, Jiang Q, Chen H, Xin H, He Q, Ruan D. Comparison of mini-open repair system and percutaneous repair for acute Achilles tendon rupture. BMC Musculoskelet Disord. 2021;22(1):914. doi:10.1186/s12891-021-04802-8
17. Maes R, Copin G, Averous C. Is percutaneous repair of the Achilles tendon a safe technique? A study of 124 cases. Acta Orthop Belg. 2006;72(2):179–183.
18. Huang X, Liu JW, Jiang Y, et al. Peritendinous submembrane access technique for management of acute ruptures of the Achilles tendon: a retrospective study of 249 cases. Orthop Surg. 2024. doi:10.1111/os.14098
19. Assal M, Jung M, Stern R, Rippstein P, Delmi M, Hoffmeyer P. Limited open repair of Achilles tendon ruptures: a technique with a new instrument and findings of a prospective multicenter study. J Bone Joint Surg Am. 2002;84(2):161–170. doi:10.2106/00004623-200202000-00001
20. Hsu AR, Jones CP, Cohen BE, Davis WH, Ellington JK, Anderson RB. Clinical outcomes and complications of percutaneous Achilles repair system versus open technique for acute Achilles tendon ruptures. Foot Ankle Int. 2015;36(11):1279–1286. doi:10.1177/1071100715589632
21. M Khair RA, Stenroth L, Péter A, et al. Non-uniform displacement within ruptured Achilles tendon during isometric contraction. Scand J Med Sci Sports. 2021;31(5):1069–1077. doi:10.1111/sms.13925
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.