")
Back to Journals » Journal of Pain Research » Volume 17
Clinical Outcomes of Exercise Rehabilitation for Degenerative Tibial Meniscal Tears: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Authors Mao S , Xiao K, Xu H, Wang Y, Guo X
Received 15 March 2024
Accepted for publication 25 September 2024
Published 24 October 2024 Volume 2024:17 Pages 3431—3448
DOI https://doi.org/10.2147/JPR.S467423
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Sujie Mao,1 Kaiwen Xiao,2 Hong Xu,3 YanAn Wang,4 Xiujin Guo2
1Graduate Department, Harbin Sport University, Harbin, Heilongjiang, People’s Republic of China; 2School of Sports Industry and Leisure, Nanjing Sport Institute, Nanjing, Jiangsu, People’s Republic of China; 3College of Sports and Health, Sangmyung University, Seoul, South Korea; 4Academic Affairs Office, Jiangsu Police College, Nanjing, Jiangsu, People’s Republic of China
Correspondence: Xiujin Guo, Nanjing Sport Institute, No. 8, Linggu Temple, XuanWu District, Nanjing, Jiangsu, People’s Republic of China, Email [email protected]
Objective: This study aims to comprehensively evaluate the effectiveness of exercise rehabilitation therapy for patients with Degenerative Meniscal Lesions of the Tibia (DMLT), providing more effective and safer treatment options for DMLT patients and offering more reliable evidence-based medical recommendations.
Methods: Adhering to the PRISMA guidelines, this research conducted a literature search through databases such as PubMed, Web of Science, EMBASE, EBSCOhost, and Cochrane, with the search cut-off date being January 2024. Following the PICOS principles, a comprehensive search was conducted. Two researchers independently screened the literature and extracted data. Using R software, effect size analyses were conducted on indicators such as pain, knee joint function, lower limb muscle strength, and physical function in DMLT patients, with the significance level set at P< 0.05, aiming to comprehensively assess the impact of exercise therapy on the rehabilitation outcomes for DMLT patients.
Results: The study included 12 randomized controlled trials, encompassing 1336 DMLT patients. Based on the quality assessment using the modified Jadad scale, the overall quality of the included studies was determined to be moderate.The meta-analysis showed that exercise therapy significantly reduced pain (WMD=− 5.50, P< 0.05), improved lower limb muscle strength (SMD=0.05, P< 0.05), and enhanced physical function (SMD=0.65, P< 0.05). Subgroup analyses revealed that, compared to surgery alone, exercise therapy combined with surgery had a significant effect on improving muscle strength and physical function. Functional training and home-based exercises showed more pronounced effects on specific indicators. The study results indicate that exercise therapy alone has limited effectiveness in improving knee joint function, and combining exercise with surgery does not show a significant advantage (P > 0.05). Additionally, subgroup analysis revealed no significant impact of intervention duration, exercise type, or patient age on functional improvement.
Conclusion: Exercise therapy has shown potential in alleviating pain, enhancing lower limb muscle strength, and improving mobility in patients with degenerative meniscal lesions of the tibia (DMLT). Functional training and varied rehabilitation exercises may provide effective pathways for long-term recovery in these patients.
Registration: This study has been registered in a prospective registry platform with the registration number: CRD42024518643.
Keywords: degenerative meniscus injury, exercise rehabilitation, non-pharmacological treatment, pain
A Letter to the Editor has been published for this article.
A Response to Letter by Mr Ouyang has been published for this article.
Introduction
Meniscal injuries represent a common type of knee injury, frequently encountered among individuals engaged in long-term physical activities and the middle-aged to elderly population.1 These injuries typically include traumatic meniscal tears as well as Degenerative Meniscal Lesions of the Tibia2 (DMLT). Degenerative meniscal injuries are characterized by gradual degeneration and thinning of the meniscal tissue, leading to tears and wear. The incidence of degenerative meniscal injuries is closely associated with factors such as age, gender, body weight, occupation, and level of physical activity. With the aging of the population, age-related knee joint issues have become increasingly prominent.3 Epidemiological statistics indicate that the incidence rate of DMLT is between 12%-14%, with 60 out of every 100,000 people suffering from degenerative meniscal injuries, and this rate is progressively increasing.4 In the United States, 17 out of every 100,000 people undergo meniscal surgery, making it one of the most common orthopedic procedures.5
As age advances, meniscal tissue undergoes degenerative changes, becoming more fragile and prone to injury.6 Athletes and sports enthusiasts who frequently engage in high-intensity, bending, and twisting movements are at a higher risk of meniscal injuries.7 Additionally, individual anatomical structures and knee joint deformities can increase the risk of meniscal injuries, including knee instability or asymmetrical load distribution.8 Studies have shown that meniscal injuries are common even among asymptomatic individuals. A study involving 115 asymptomatic sedentary adults found that 97% of their knees exhibited at least one structural abnormality on MRI, with 30% showing meniscal tears. This indicates that meniscal injuries may be associated with various factors such as age and physical activity levels, and are not limited to symptomatic individuals.9 Moreover, Reid (2010) identified behaviors such as squatting, kneeling, crawling, and stair climbing as risk factors for degenerative meniscal injuries.10 Patients with DMLT typically experience knee pain and swelling, leading to a decrease in physical function and impacting daily life, thereby reducing the quality of life. If not treated timely, this can lead to joint degeneration, synovitis, and other long-term complications, increasing the difficulty of treatment and the risk of disease.11
Currently, the treatment options for DMLT mainly include surgical and conservative approaches.12 Conservative treatment aims to alleviate pain and swelling through rest, ice application, and the use of topical analgesics,13 as well as physical therapy and rehabilitation exercises to strengthen the supporting muscles around the knee and promote joint function recovery.14 Surgical treatment is the primary option for most meniscal injuries, comprising meniscal repair, meniscectomy, and meniscal transplantation.15 Meniscal repair involves fixing the damaged meniscal tissue using sutures or other techniques while preserving as much of the normal tissue as possible; meniscectomy mainly involves removing part or all of the damaged meniscal tissue; meniscal transplantation replaces the damaged meniscal tissue with healthy tissue from a donor, depending on the extent of the meniscal injury.16,17
Whether it’s conservative or surgical treatment, rehabilitation and recovery training are crucial steps.18 Through physical therapy and exercise rehabilitation, patients are assisted in restoring joint function, strengthening muscle support, reducing pain, and improving the quality of life. A plethora of past research has demonstrated that exercise therapy facilitates the healing and recovery of injured tissues.19 Appropriate exercise training can enhance muscle strength, improve joint stability, promote soft tissue repair, and bone reconstruction, thereby accelerating the recovery process.20 Regular physical exercise enhances the muscular resilience of DMLT patients, improves joint flexibility and balance, thereby aiding in the reduction of joint stress and consequently alleviating pain.21 It also helps in relieving anxiety and depression, improving self-perception and psychological state, returning to normal life and work conditions, and enhancing the quality of life.
However, some studies have pointed out that excessive exercise might lead to further damage and inflammatory responses in the meniscus,15 exacerbating the injury and questioning the long-term effectiveness of exercise rehabilitation for DMLT patients. Moreover, some research suggests that the effects of exercise therapy on meniscal injuries are minimal or even counterproductive.22 Pan (2020) indicated that arthroscopic partial meniscectomy combined with exercise therapy for degenerative meniscal tears helps improve patients’ pain, yet this study showed limitations such as not specifying the duration of exercise therapy, the form of exercise interventions, and the follow-up period, leading to biases that prevent determining the optimal exercise regimen.23
This study aims to comprehensively evaluate the efficacy of exercise therapy in patients with Degenerative Meniscal Lesions of the Tibia (DMLT) through a systematic review. It conducts a meta-analysis to assess the impact of exercise therapy on pain relief and functional improvement. Subgroup analyses are performed to evaluate the effectiveness of exercise therapy in different patient contexts, including those with or without surgery, and to determine the optimal exercise regimen in terms of duration, frequency, and specific forms. The goal is to provide more reliable evidence-based guidance for clinical practice, offering DMLT patients more effective and safer treatment options.
Research Methods
Search Strategy and Study Selection
The search strategy and selection of studies for this research were prospectively registered with PROSPERO,24 registration ID: CRD42024518643. Following the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines25(Annex 1), a comprehensive literature search on exercise therapy for degenerative meniscal injuries was conducted. Systematic electronic searches were performed in databases including PubMed, Web of Science, EMBASE, EBSCOhost, and Cochrane, covering all studies published up to January 2024. Additionally, manual searches of the reference lists of eligible articles were conducted to include other relevant publications. The search strategy was developed based on the PICOS principle, utilizing MeSH terms combined with free-text terms (Table 1) to broaden the scope of this study. During the literature search phase, the search was limited by study outcomes, control group interventions, and types of literature. Search terms included P: Tibial Meniscus Injuries OR Injuries, I: physical activity, with all search terms combined using Boolean operators AND and OR. The entire search was conducted by two independent reviewers (SJM, KWX) and in cases of disagreement on study inclusion, a third reviewer (HX) was consulted.
 |
Table 1 Literature Search Strategy |
Eligibility Criteria
This study employed a three-round screening process, initially importing the downloaded literature into EndNote X20 and removing duplicates based on title, author, and publication year. Following the study’s inclusion and exclusion criteria, titles and abstracts of the imported literature were reviewed to determine preliminarily selected articles. Full texts of articles meeting the criteria were then reviewed to assess their eligibility for inclusion.
Inclusion Criteria
- The article must report on patients with degenerative meniscal injuries (diagnosed according to the American Academy of Orthopaedic Surgeons’ guidelines on Knee Arthroscopy Surgery: Meniscal Tears and Arthritis26). Diagnostic methods include symptom assessment, knee joint examination, functional tests, and MRI of the posterior horn of the medial meniscus showing degenerative level tears;
- The intervention groups in the included studies consisted of exercise therapy, while the control groups did not receive any form of exercise intervention.
Exclusion Criteria
- Literature that is not randomized controlled trials (RCTs);
- Studies designed as animal experiments;
- Non-English publications;
- Meta-analyses, reviews, conference abstracts, case series, and similar studies;
- Studies from which data could not be extracted.
Data Extraction and Quality Assessment
In publications that met the inclusion and exclusion criteria, data were extracted by two independent researchers (HX and KWX) according to the requirements of the Cochrane Handbook for Systematic Reviews of Interventions, and recorded using a standardized data extraction form. Extracted data included literature characteristics (author, publication year, study design, outcome measures), participant characteristics (sample size, age, gender distribution), intervention measures (type of intervention, intervention cycle, intensity, duration), and post-intervention outcome measures (Mean±SD). If data presented in graphical form could not be extracted directly, Get-Data software was used for data extraction. For missing data or unclear information, the corresponding authors were contacted for further details.
All included studies were assessed for quality using the modified Jadad scale,27 which aims to comprehensively evaluate the quality of RCTs. This assessment focused on the studies’ randomization, blinding, withdrawals, and dropouts, as well as the description of the randomization process, the implementation of blinding, the description of participant withdrawals and losses, the transparency of statistical analysis, and other potential sources of bias. The quality score for each study was independently assessed by two researchers (SJM and KWX), and any discrepancies were resolved through discussion or by involving a third evaluator (HX) to make a decision.
Outcome Measures
This study evaluates the effectiveness of exercise therapy on patients with DMLT using indicators such as pain assessment, knee joint functionality, muscle strength, and physical function.
Primary Outcome
This study identified pain assessment using the Visual Analog Scale (VAS) as the primary outcome and endpoint. Pain relief is the most immediate and critical clinical outcome for patients with Degenerative Meniscal Lesions (DMLT). The VAS score accurately quantifies patients’ subjective pain experiences, directly reflecting the core efficacy of the intervention in this study.
Secondary Outcomes
Secondary outcomes included knee joint function assessment (KOOS, Lysholm, and IKDC questionnaires), lower limb strength indicators (eg, quadriceps and hamstring strength, isokinetic knee extension, and flexion peak torque), and mobility indicators (eg, single-leg hop and 6-minute walk test). These secondary outcomes not only supplement the study but also further explore the impact of exercise therapy on knee function and physical performance, providing a more comprehensive understanding of the intervention’s effects on DMLT patients.
Statistical Methods
This study employs R software (version 4.3.2) for statistical analysis, with all data processing and statistical inference conducted at a significance level of P<0.05. For continuous variables with the same measurement units, the Weighted Mean Difference (WMD) is used; for continuous variables with different units, the Standardized Mean Difference (SMD) serves as the effect size to compare differences between treatment groups, with the effect size’s confidence intervals represented by (95% CI).Given the significant heterogeneity among patients with degenerative meniscal lesions in terms of severity, study populations, and interventions, and considering that the systematic review included studies from different countries, we employed a random-effects model in all meta-analyses. This approach was particularly emphasized in subgroup analyses to ensure the robustness of the results.
In our meta-analysis, we will assess study heterogeneity using the I² statistic. The I²ranges from 0% to 100%, indicating the degree of heterogeneity among studies. The suitability of a meta-analysis is determined by the I²: if it is below 50%, heterogeneity is considered low, making the meta-analysis results more reliable. If I²is ≥50%, higher heterogeneity suggests the meta-analysis may be less suitable, requiring further investigation into the sources of heterogeneity to ensure robustness. Subgroup analyses in this study also explore potential heterogeneity sources, such as intervention duration, surgical treatment, exercise type, and participant age, enhancing the interpretation and reliability of the meta-analysis. Publication bias of the included studies will be assessed through funnel plot analysis to evaluate the presence of publication bias in this meta-analysis. To identify sources of heterogeneity, subgroup analyses will be conducted based on intervention duration, whether surgical treatment was administered, the form of exercise intervention, and the average age of participants.
Research Results
Literature Review
Study Selection
A search of five databases (PubMed, Embase, Web of Science, EMBSCOhost, Cochrane Library) using the keywords “exercise therapy” and “degenerative tibial meniscal injury” yielded 622 records, from which 40 duplicate articles were removed. A further screening of 582 articles led to the exclusion of 499 studies due to irrelevance to the topic, animal studies, non-English publications, and review articles. After full-text review of the remaining 83 studies, 71 were excluded for reasons including not being RCTs, the intervention group not receiving exercise therapy, inability to obtain the literature, irrelevance to the topic, and inability to extract data. Ultimately, 12 papers were included in this systematic review and meta-analysis (Figure 1).
 |
Figure 1 Literature Search Flowchart. |
Study Characteristics
This meta-analysis included 12 studies (Table 2), all of which were RCTs on exercise therapy for meniscal injuries. The interventions typically comprised neuromuscular training, strength training, or home-based exercises, with durations ranging from 3 to 12 weeks and frequencies mostly between 2 to 3 times per week. The main outcomes focused on knee joint functionality and muscle strength, as well as assessments of pain and physical function. The studies involved experimental groups receiving exercise therapy, while control groups underwent meniscectomy, and in some cases, experimental groups received surgical treatment combined with exercise therapy, compared to control groups treated solely by surgery.
 |
Table 2 Characteristics of Included Literature |
Participant Characteristics
This meta-analysis involved participants from multiple countries, including Norway, Sweden, the United Kingdom, the Netherlands, and South Korea, encompassing a total of 1,336 subjects. The injury type primarily focused on was degenerative meniscal tears, with a particular emphasis on the middle-aged to elderly adult population. The average age distribution for both the experimental and control groups ranged from 30 to 60 years.
Specifically, the studies from Norway showed that participants were mostly middle-aged, while those from Sweden included a younger to middle-aged population. The study subjects from the United Kingdom were slightly younger, whereas those from the Netherlands spanned from young adults to the middle-aged and elderly. The research from South Korea focused on the middle-aged to elderly population. There was considerable variation in the sample size of the studies, but the age data overall demonstrated a degree of consistency, reflecting a relatively uniform age distribution among the study participant group.
Publication Bias Assessment
Publication bias for pain, knee joint functionality, and muscle strength was analyzed using Egger’s test combined with funnel plots, examining whether the slope and bias results were statistically significant and assessing the symmetry of the funnel plots to determine bias (Table 3). Due to the inclusion of fewer than ten studies on physical function, publication bias analysis for this indicator could not be performed.
 |
Table 3 Egger’s Test |
The intercept coefficient for the pain indicator was 1.60996 (P=0.013), 95% CI [0.40, 2.82], indicating a significant publication bias among the studies included for the pain indicator. Observing the funnel plot (Figure 2a) reveals an asymmetric distribution of the included studies, suggesting selective reporting and a potential influence of publication bias on the results for the pain indicator. The analysis of publication bias for the knee joint functionality indicator found an intercept coefficient of 1.796263 (P=0.019), 95% CI [0.33, 3.26], indicating a strong publication bias, with published reports tending towards studies with higher effect sizes. Egger’s test, through its significant intercept, indeed revealed issues of selective reporting, and the funnel plot (Figure 2b) similarly indicated significant publication bias affecting this indicator. Analysis of the lower limb muscle strength indicator showed a slope coefficient of −0.19, P<0.001, indicating a preference for publishing studies that found significant effects in small sample studies, while large sample studies were less affected by this bias. The intercept (represented as bias) was −2.114361, P<0.001, 95% CI [−3.15, −1.08]. The asymmetry observed in the funnel plot (Figure 2c) suggests a significant publication bias may exist for the lower limb strength indicator.
 |
Figure 2 Funnel Plot of Publication Bias Analysis; (a) Publication Bias in Pain Indicators; (b) Publication Bias in Knee Joint Functional Indicators; (c) Publication Bias in Lower Limb Strength. |
Quality Assessment
A systematic quality assessment of the 12 included studies was conducted using the modified Jadad scale (Table 4). The scoring criteria were as follows: studies scoring 4–5 points were considered “high quality”, indicating good performance in key areas such as randomization, blinding, and handling of withdrawals, despite minor shortcomings; studies scoring 2–3 points were considered “low quality”, reflecting significant design or execution flaws that could affect reliability. Eight studies were rated as “high quality”, while the remaining four were rated as “low quality”. However, most studies showed inadequate blinding, which significantly impacted the overall quality assessment. Given the widespread weaknesses in blinding and allocation concealment, the overall quality of the literature should be more cautiously defined as “moderate quality”. Future studies should focus on strengthening these critical areas to improve the overall quality and reliability of meta-analyses.
 |
Table 4 Quality Evaluation of the Modified Jadad Scale |
Meta-Analysis Results
The Impact of Exercise Therapy on Pain in Patients with DMLT
The pain indicator included 6 articles and 15 studies involving 662 DMLT patients, with interventions including exercise therapy alone or in combination with surgical treatment, compared to control groups receiving no exercise or surgical treatment alone. The combined effect size analysis (Figure 3) showed that, compared to the control groups, the exercise groups had a significant improvement in VAS scores, with WMD = −1.14, 95% CI [−1.72, −0.56], P< 0.05. Although the change in pain scores was statistically significant (P<0.05), the clinical significance did not meet the conventional threshold for clinical importance (aligned with the minimum clinically significant difference in VAS, typically considered to be between 7 and 13 mm, as indicated in40). Therefore, despite the statistical differences observed, the results should be interpreted with caution in clinical practice.
 |
Figure 3 Forest Plot for Pain Indicators. |
Subgroup analysis based on whether subjects underwent surgical treatment (Table 5) showed significant improvements in VAS scores both for exercise therapy compared to surgery alone and for exercise combined with surgery compared to surgery alone. For those who underwent surgery, WMD = −0.99, 95% CI [−1.551, −0.438], P< 0.05, and for those who did not undergo surgery, WMD = −5.50, 95% CI [−8.842, −2.152], P< 0.05. Subgroup analysis based on the duration of the intervention found positive effects on the VAS scores for DMLT patients regardless of the duration, with intervention periods ≤3 months, WMD = −1.05, P< 0.05, and >3 months, WMD = −1.29, 95% CI [−2.292,-0.287], P< 0.05. When categorizing exercise interventions into exercise therapy, home training, and coordination training for subgroup analysis, both exercise therapy and coordination training showed significant improvements, P< 0.05, while home training showed no statistical significance, WMD = −0.24, 95% CI [−0.593,0.118], P > 0.05. Dividing participants by average age into <45 years, 45–54 years, and >54 years for subgroup analysis revealed that the improvement in pain was not significant for patients aged <45 or >54 years, P > 0.05, whereas patients aged 45–54 years showed significant improvements, WMD = −1.38, P< 0.05.
 |
Table 5 Summary of Subgroup Analysis Results of Pain, Knee Joint Function, Lower Limb Muscle Strength Physical Function |
The Effect of Exercise Therapy on Knee Joint Function in Patients with DMLT
The knee joint function indicator included 8 articles and 18 studies involving 662 DMLT patients. Measurements were conducted using the KOOS scale, IKDC scale, and Lysholm score, thus the Standardized Mean Difference (SMD) was used to combine effect sizes. Among these, 9 studies compared exercise therapy with surgical treatment, and 9 studies compared exercise combined with surgery to surgery alone. The combined effect size analysis (Figure 4) indicated that compared to surgical treatment, exercise therapy alone showed inferior improvement in knee joint functionality, with an SMD of −2.06, 95% CI [−4.1, −0.02].
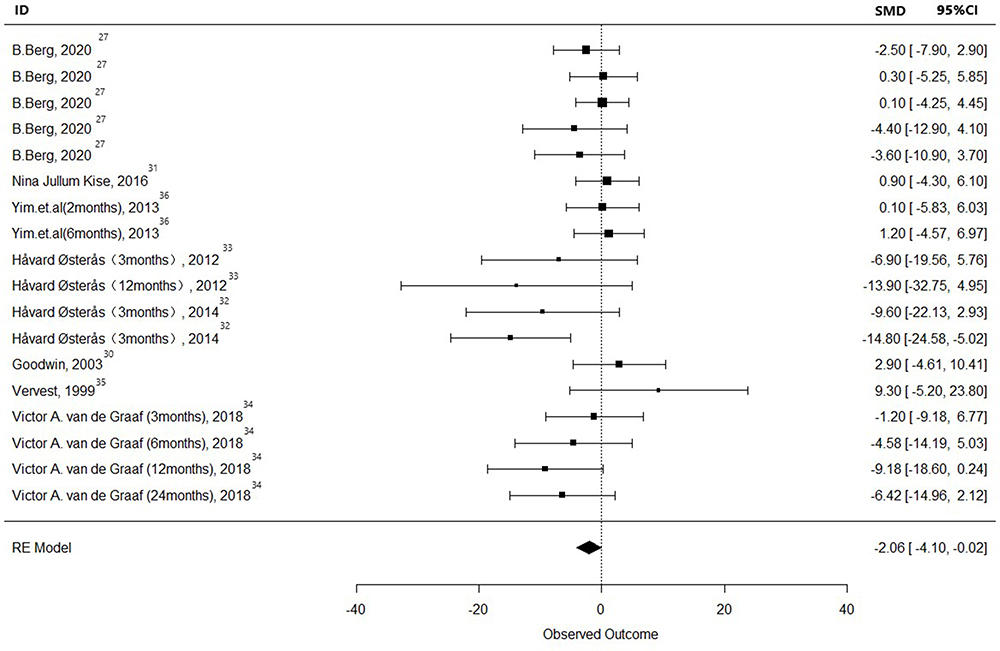 |
Figure 4 Forest Plot for Knee Joint Function Indicators. |
Subgroup analysis based on the comparison between experimental and intervention groups (Table 5) showed that, compared to surgery alone, exercise therapy combined with surgical treatment did not show statistical significance, with an SMD of −2, P > 0.05. However, comparing exercise therapy alone to surgical treatment revealed that surgical treatment had a significantly better improvement effect than exercise therapy, with an SMD= −2.25, 95% CI [−4.469,-0.038], P< 0.05. Subgroup analysis based on follow-up duration and the form of exercise therapy showed that neither the duration of the intervention nor the form of exercise therapy had a statistically significant impact on the functionality of DMLT patients, P > 0.05. Subgroup analysis based on average age showed that for patients aged <45 or >54 years, there was no significant difference compared to the surgery group, P > 0.05. However, patients aged 45–54 years showed better improvement with surgical treatment, with an SMD = −2.91, 95% CI [−5.735, −0.086], P< 0.05.
The Effectiveness of Exercise Therapy on Improving Lower Limb Muscle Strength in Patients with DMLT
The assessment of lower limb muscle strength included 5 articles and 33 studies involving 216 DMLT patients, measured using quadriceps, hamstrings, isokinetic knee extension, and Hamstrings Peak Torque, among others, with the Standardized Mean Difference (SMD) used to combine effect sizes. The comparison methods included exercise therapy versus surgical treatment, and exercise therapy combined with surgical treatment versus surgery alone. The combined effect size analysis (Figure 5) showed no significant difference compared to surgical treatment, with an SMD of 0.05, 95% CI [−0.09, 0.2].
 |
Figure 5 Forest Plot for Lower Limb Strength Indicators. |
Subgroup analysis based on the comparison between the experimental and intervention groups (Table 5) found that exercise therapy combined with surgical treatment compared to surgery alone had an improvement effect, with an SMD=1.33, 95% CI [0.622,2.029], P< 0.05. Comparing exercise therapy alone to surgical treatment showed that the improvement effect of surgical treatment was significant, with an SMD= −2.3, 95% CI [−0.342,-0.113], P< 0.05. Thus, it can be seen that undergoing exercise rehabilitation after surgical treatment offers better improvement in muscle strength for DMLT patients. Subgroup analysis based on the duration of the intervention found that exercise interventions longer than 3 months had a better improvement effect on muscle strength, with an SMD=0.81, 95% CI [0.237,1.386], P< 0.05. Subgroup analysis based on the form of exercise therapy intervention revealed that, compared to the control group, exercise therapy and functional training significantly improved muscle strength, P< 0.05, while neuromuscular training combined with strength training showed less improvement in strength. As the average age of participants included in this indicator was between 45–54 years, no age subgroup analysis was conducted.
Exercise Therapy Enhances Physical Function in Patients with DMLT
The evaluation of physical function indicators included 3 articles and 6 studies involving 85 DMLT patients, measured using the One-leg hop test, 6MWT (Six Minute Walk Test), among others, with the Standardized Mean Difference (SMD) used to combine effect sizes. The combined effect size analysis (Figure 6) showed a significant improvement compared to surgical treatment, with an SMD =0.65, 95% CI [0.19, 1.11].
 |
Figure 6 Forest Plot for physical function Indicators. |
Subgroup analysis based on the comparison between the experimental and intervention groups (Table 5) found that exercise therapy combined with surgical treatment compared to surgery alone had an improvement effect, with an SMD =1.15, 95% CI [−2.399,4.704], P< 0.05. Comparing exercise therapy alone to surgical treatment found no significant difference, P< 0.05, indicating no statistical significance. Subgroup analysis based on the duration of the intervention found that exercise interventions longer than 3 months had a better improvement effect on physical function, with an SMD =0.53, 95% CI[0.183,0.871], P< 0.05, while interventions shorter than 3 months showed no significant difference. Subgroup analysis based on the form of exercise therapy intervention revealed that improvements through functional training and exercise therapy were significant, while neuromuscular training combined with strength training showed no statistical significance. Since the average age of participants included in this indicator was between 45–54 years, no age subgroup analysis was performed.
Discussion
Patients with DMLT often suffer from pain, reduced muscle strength, and decreased physical function.41 Previous studies have confirmed that exercise therapy can effectively alleviate pain, enhance muscle quality, and improve physical function.42 However, the specific effects and intervention methods of exercise therapy for DMLT patients remain unclear. In this study, we conducted a meta-analysis to explore the effects of exercise therapy versus no exercise therapy on DMLT patients, focusing on indicators such as VAS score, KOOS-ADL, Lysholm score, single-leg hop height, and hamstring peak torque. While the analysis demonstrated positive effects of exercise therapy, particularly in enhancing lower limb muscle strength, the medium quality of the included studies and the presence of significant publication bias may affect the interpretation and clinical application of these results. Future research should address these biases and control for their impact.
Patients with DMLT commonly experience pain, which intensifies with activity, particularly when bearing weight or rotating the knee.41 This study found that exercise therapy significantly improves pain indicators in patients with tibial meniscal injuries, consistent with a large body of previous research. One past study, through a meta-analysis of six RCTs involving 879 patients, compared medical exercise therapy alone to arthroscopic partial meniscectomy followed by medical exercise therapy for middle-aged patients with degenerative meniscal tears. It found that exercise therapy, both alone and in combination with surgery, effectively improved patients’ pain indicators, with WMD=0.56, P<0.05.43 A previous meta-analysis found that both arthroscopic surgery and exercise therapy have positive effects on DMLT patients, particularly in pain relief and functional recovery. Although surgery showed a slight statistical advantage in pain relief in the short term (3 to 6 months), this difference was not clinically significant and diminished over time. In long-term follow-ups, there was no significant difference between the two treatments in terms of pain relief and functional improvement.44 A recent study with a 5-year follow-up of DMLT patients aged 45 to 70 years explored whether the efficacy of exercise-based therapy was non-inferior to arthroscopic partial meniscectomy. It found no significant or clinically relevant differences in patient-reported knee joint function between groups, confirming that exercise therapy intervention is not inferior to surgical treatment and should be the preferred treatment option for DMLT patients over surgery.45 However, a previous systematic review and meta-analysis including 12 studies found no significant difference in pain outcomes between exercise therapy and no exercise therapy following meniscectomy, and various types of exercise therapy did not improve pain (MD 19.30 [−6.60,45.20]) or knee joint function (SMD 0.01 [−0.27,0.28]), which aligns with the findings of this study.46
DMLT not only causes pain and discomfort in the knee joint but is also often accompanied by a decrease in lower limb muscle strength and reduced physical function.47 The integrity of the meniscus being compromised affects the knee joint’s stability and weight-bearing capacity, leading to a decline in patients’ physical function. The weakening of lower limb muscle strength can limit patients’ range of motion, reduce their activity levels, and thus impact their quality of life. This meta-analysis indicates that exercise therapy can effectively enhance lower limb muscle strength and improve physical function in patients with DMLT (P< 0.05). A previous systematic review found that exercise therapy and arthroscopic partial meniscectomy have comparable effects on pain relief and joint function improvement. In patients who underwent meniscectomy, long-term follow-up indicated that exercise therapy had a more pronounced advantage in restoring joint function. This suggests that while the short-term effects may not be immediately apparent, exercise therapy holds long-term potential for promoting joint function recovery in patients with meniscal injuries, supporting its application as an effective rehabilitation method in clinical practice.46 A recent cross-sectional study assessing 252 DMLT patients through Kellgren-Lawrence grading, magnetic resonance imaging, and knee osteoarthritis scores found that greater quadriceps and hamstring muscle strength were associated with lower pain symptoms and higher physical function in patients with DMLT.48 This suggests that training to enhance muscle strength can effectively improve lower limb muscle strength and physical function. Furthermore, a two-year follow-up randomized controlled trial indicated that exercise therapy has a positive effect on improving thigh muscle strength compared to surgery, considering supervised exercise therapy as a treatment option. This result is consistent with the findings of this study.48
The causes of DMLT include a variety of factors such as the accumulation of micro-tears in the meniscus due to long-term load, knee joint imbalance, and a decrease in cell activity.49 The treatment of DMLT aims to alleviate pain symptoms, restore knee joint function, and improve joint stability and flexibility. This study confirms the significant efficacy of exercise therapy.50,51 This may be because exercise therapy can strengthen the muscle groups around the knee joint, including the quadriceps and hamstrings, which play a key role in maintaining knee joint stability.52 This, in turn, better supports and protects the knee joint, reducing the direct pressure on the meniscus and thereby achieving pain relief. Additionally, enhancing the strength of the muscles around the knee joint can effectively improve the internal and external balance of the knee joint.53 These muscles can increase the stability of the knee joint, reduce local load, thereby protecting the meniscus and alleviating pain.54
The synovial fluid in the knee joint serves to lubricate and nourish the joint.55 Through exercise, the activity of synovial cells in patients with DMLT can be stimulated, leading to the production of a large amount of synovial fluid.56 This not only lubricates the knee joint but also provides more nutrition to the meniscus, aiding in the recovery and improvement of DMLT. Furthermore, exercise can promote blood circulation in the body. Improving blood circulation means more oxygen and nutrients are transported to the knee joint and meniscus, and metabolic waste is removed.57 This process also plays a crucial role in the repair of DMLT. Inflammation is one of the main factors causing stiffness, pain, and limited range of motion in the knee joint. Moderate physical activity can modulate the immune system, reducing pro-inflammatory cytokines (including Tumor Necrosis Factor-alpha (TNF-α) and Interleukin-1 beta (IL-1β)).58 These inflammatory factors can exacerbate inflammation and neurosensitivity, leading to an increased pain response in the damaged area. Exercise therapy can effectively suppress the inflammatory response and promote the healing of damaged tissue.59
During exercise, the dopamine released by the brain can enhance the pain threshold by altering the brain’s processing of pain signals, thereby reducing the sensation of pain.60 Simultaneously, dopamine also boosts mood and feelings of happiness; increasing its release can help alleviate anxiety and depression caused by chronic pain.61 Beyond dopamine, other hormones and neurotransmitters released during exercise work together to reduce pain and improve overall health. Endorphins, a group of naturally occurring opioid peptides62 (including β-endorphin, enkephalins, and dynorphins), known as “feel-good” hormones,63 are stimulated by exercise. These substances can bind to opioid receptors in the brain and central nervous system, naturally relieving pain and generating pleasure. Growth hormone also increases after exercise, crucial for promoting tissue repair and regeneration, helping accelerate the healing process of meniscal injuries and facilitating the repair of damaged tissue.
This study’s findings reveal that compared to surgical treatments, exercise therapy offers less favorable outcomes in knee joint functionality recovery. This is consistent with a previous systematic review, suggesting that exercise therapy, in some instances, may delay the need for surgery, yet its effectiveness in improving knee joint functionality is limited compared to knee replacement surgery.64 The reason for these findings might be due to the assessment tools used in the included literature (such as the KOOS scale, IKDC scale, and Lysholm score) potentially not fully capturing the comprehensive impact of exercise therapy on patients’ knee joint functionality and quality of life, particularly in assessing long-term effects, leading to selection bias and measurement bias. Furthermore, the follow-up periods in the study might not have been long enough to observe the long-term benefits of exercise therapy. Future research needs to ensure the reliability and applicability of the study results through more stringent randomized controlled designs, implementation of blinded assessments, and the selection of more sensitive and comprehensive assessment tools. Additionally, publication bias analysis highlighted the issue of selective reporting in studies on pain, knee joint functionality, and lower limb muscle strength, particularly emphasizing the tendency to publish positive results. Significant intercept values and asymmetry in funnel plots underscore the extent to which study conclusions are affected by bias. Therefore, future research should impartially report all outcomes to ensure a comprehensive and accurate understanding of the impact of exercise therapy on patients with DMLT.
Limitations
- To avoid duplicate inclusion of studies and ensure the quality of included studies, this review did not assess grey or unpublished literature based on the PRISMA checklist, nor did it include non-English language publications. This decision may limit the comprehensiveness of our review, and the exclusion of non-English literature could impact the generalizability of the findings. We recommend that future research consider including these types of literature to reduce potential biases.
- Publication bias was assessed using Egger’s test and funnel plots, revealing issues with selective reporting. Therefore, future studies should focus on objectively assessing the effectiveness of exercise therapy.
- Lack of long-term effects and follow-up: The majority of included studies focused on the short-term effects of exercise therapy, with short follow-up periods, lacking in the assessment of long-term effects. Thus, future controlled studies should focus on long-term follow-ups to understand the long-term efficacy of exercise therapy for DMLT.
Conclusion
This study conducted a systematic review and meta-analysis to explore the effects of exercise therapy on patients with degenerative meniscal tears (DMLT), particularly focusing on pain relief, knee function enhancement, and lower limb strength improvement. The overall quality of the 12 included RCTs was moderate. Although exercise therapy showed statistically significant benefits over surgical treatment in terms of pain relief and strength enhancement, its clinical significance may be limited. Additionally, due to publication bias, the results should be interpreted cautiously. Future research should include grey literature and studies in various languages to reduce bias and improve the reliability of findings. Further exploration of optimal exercise methods, intervention duration, and long-term follow-up is needed to provide more personalized and effective treatment plans for DMLT patients.
Acknowledgments
We extend heartfelt thanks to the team committed to advancing non-surgical treatments for meniscal injuries. This research aims to enhance non-surgical approaches for meniscal tears, and I hope it brings us closer to better treatments. We also wish all those affected by meniscal injuries a quick recovery.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Englund M, Guermazi A, Gale D, et al. Incidental meniscal findings on knee MRI in middle-aged and elderly persons. N Engl J Med. 2008;359(11):1108–1115. doi:10.1056/NEJMoa0800777
2. Lento PH, Akuthota V. Meniscal injuries: a critical review. J Back Musculoskelet Rehabil. 2000;15(2):55–62. doi:10.3233/bmr-2000-152-302
3. Snoeker BA, Bakker EW, Kegel CA, Lucas C. Risk factors for meniscal tears: a systematic review including meta-analysis. J Orthop Sports Phys Ther. 2013;43(6):352–367. doi:10.2519/jospt.2013.4295
4. Bhan K. Meniscal tears: current understanding, diagnosis, and management. Cureus. 2020;12(6):e8590. doi:10.7759/cureus.8590
5. Luvsannyam E, Jain MS, Leitao AR, Maikawa N, Leitao AE. Meniscus tear: pathology, incidence, and management. Cureus. 2022;14(5):e25121. doi:10.7759/cureus.25121
6. Wesdorp MA, Eijgenraam SM, Meuffels DE, et al. Traumatic meniscal tears are associated with meniscal degeneration. Am J Sports Med. 2020;48(10):2345–2352. doi:10.1177/0363546520934766
7. Kirkendall DT, Sayers A. Soccer Anatomy. Human Kinetics Publishers; 2020.
8. Heijink A, Vanhees M, van den Ende K, et al. Biomechanical considerations in the pathogenesis of osteoarthritis of the elbow. Knee Surg Sports Traumatol Arthrosc. 2016;24(7):2313–2318. doi:10.1007/s00167-015-3518-7
9. Horga LM, Hirschmann AC, Henckel J, et al. Prevalence of abnormal findings in 230 knees of asymptomatic adults using 3.0 T MRI. Skeletal Radiol. 2020;49(7):1099–1107. doi:10.1007/s00256-020-03394-z
10. Reid CR, Bush PM, Cummings NH, McMullin DL, Durrani SK. A review of occupational knee disorders. J Occup Rehabil. 2010;20(4):489–501. doi:10.1007/s10926-010-9242-8
11. Filbay SR, Skou ST, Bullock GS, et al. Long-term quality of life, work limitation, physical activity, economic cost and disease burden following ACL and meniscal injury: a systematic review and meta-analysis for the OPTIKNEE consensus. Br J Sports Med. 2022;56(24):1465–1474. doi:10.1136/bjsports-2022-105626
12. Mordecai SC, Al-Hadithy N, Ware HE, Gupte CM. Treatment of meniscal tears: an evidence based approach. World J Orthop. 2014;5(3):233. doi:10.5312/wjo.v5.i3.233
13. Bleakley C, McDonough S, MacAuley D. The use of ice in the treatment of acute soft-tissue injury: a systematic review of randomized controlled trials. Am J Sports Med. 2004;32(1):251–261. doi:10.1177/0363546503260757
14. Brindle T, Nyland J, Johnson DL. The meniscus: review of basic principles with application to surgery and rehabilitation. J Athl Train. 2001;36(2):160–169.
15. Giuffrida A, Di Bari A, Falzone E, et al. Conservative vs. surgical approach for degenerative meniscal injuries: a systematic review of clinical evidence. Eur Rev Med Pharmacol Sci. 2020;24(6):2874–2885. doi:10.26355/eurrev_202003_20651
16. Bansal S, Floyd ER, A Kowalski M, et al. Meniscal repair: the current state and recent advances in augmentation. J Orthop Res. 2021;39(7):1368–1382. doi:10.1002/jor.25021
17. Spalding T, Damasena I, Lawton R. Meniscal repair techniques. Clin Sports Med. 2020;39(1):37–56. doi:10.1016/j.csm.2019.08.012
18. Kim JS, Lee MK, Choi MY, et al. Rehabilitation after repair of medial meniscus posterior root tears: a systematic review of the literature. Clin Orthop Surg. 2023;15(5):740–751. doi:10.4055/cios21231
19. Culvenor AG, Girdwood MA, Juhl CB, et al. Rehabilitation after anterior cruciate ligament and meniscal injuries: a best-evidence synthesis of systematic reviews for the OPTIKNEE consensus. Br J Sports Med. 2022;56(24):1445–1453. doi:10.1136/bjsports-2022-105495
20. Chen J, Zhou R, Feng Y, Cheng L. Molecular mechanisms of exercise contributing to tissue regeneration. Signal Transduct Target Ther. 2022;7(1):383. doi:10.1038/s41392-022-01233-2
21. Powers SK, Deminice R, Ozdemir M, Yoshihara T, Bomkamp MP, Hyatt H. Exercise-induced oxidative stress: friend or foe? J Sport Health Sci. 2020;9(5):415–425. doi:10.1016/j.jshs.2020.04.001
22. Sherman SL, DiPaolo ZJ, Ray TE, Sachs BM, Oladeji LO. Meniscus injuries: a review of rehabilitation and return to play. Clin Sports Med. 2020;39(1):165–183. doi:10.1016/j.csm.2019.08.004
23. Pan H, Zhang P, Zhang Z, Yang Q. Arthroscopic partial meniscectomy combined with medical exercise therapy versus isolated medical exercise therapy for degenerative meniscal tear: a meta-analysis of randomized controlled trials. Int J Surg. 2020;79:222–232. doi:10.1016/j.ijsu.2020.05.035
24. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
25. Page MJ, McKenzie JE, Bossuyt PM, et al. Updating guidance for reporting systematic reviews: development of the PRISMA 2020 statement. J Clin Epidemiol. 2021;134:103–112. doi:10.1016/j.jclinepi.2021.02.003
26. Abram SGF, Beard DJ, Price AJ. Arthroscopic meniscal surgery: a national society treatment guideline and consensus statement. Bone Joint J. 2019;101-b(6):652–659. doi:10.1302/0301-620x.101b6.Bjj-2019-0126.R1
27. Olivo SA, Macedo LG, Gadotti IC, Fuentes J, Stanton T, Magee DJ. Scales to assess the quality of randomized controlled trials: a systematic review. Phys Ther. 2008;88(2):156–175. doi:10.2522/ptj.20070147
28. Berg B, Roos EM, Englund M, et al. Development of osteoarthritis in patients with degenerative meniscal tears treated with exercise therapy or surgery: a randomized controlled trial. Osteoarthritis Cartilage. 2020;28(7):
29. Berg B, Roos EM, Kise NJ, Engebretsen L, Holm I, Risberg MA. Muscle strength and osteoarthritis progression after surgery or exercise for degenerative meniscal tears: secondary analyses of a randomized trial. Arthritis Care Res. 2022;74(1):
30. Ericsson YB, Dahlberg LE, Roos EM. Effects of functional exercise training on performance and muscle strength after meniscectomy: a randomized trial. Scand J Med Sci Sports. 2009;19(2):156–165. doi:10.1111/j.1600-0838.2008.00794.x
31. Goodwin PC, Morrissey MC, Omar RZ, Brown M, Southall K, McAuliffe TB. Effectiveness of supervised physical therapy in the early period after arthroscopic partial meniscectomy. Physical Ther. 2003;83(6):
32. Kise NJ, Risberg MA, Stensrud S, Ranstam J, Engebretsen L, Roos EM. Exercise therapy versus arthroscopic partial meniscectomy for degenerative meniscal tear in middle aged patients: randomised controlled trial with two year follow-up. BMJ. 2016;354:i3740. doi:10.1136/bmj.i3740
33. Østerås H. A 12-week medical exercise therapy program leads to significant improvement in knee function after degenerative meniscectomy: a randomized controlled trial with one year follow-up. J Bodyw Mov Ther. 2014;18(3):
34. Østerås H, Østerås B, Torstensen TA. Is postoperative exercise therapy necessary in patients with degenerative meniscus? A randomized controlled trial with one year follow-up. Knee Surg Sports Traumatol Arthrosc. 2014;22(1):
35. Stensrud S, Risberg MA, Roos EM. Effect of exercise therapy compared with arthroscopic surgery on knee muscle strength and functional performance in middle-aged patients with degenerative meniscus tears: a 3-mo follow-up of a randomized controlled trial. Am J Phys Med Rehabil. 2015;94(6):460–473. doi:10.1097/PHM.0000000000000209
36. van de Graaf VA, Noorduyn JCA, Willigenburg NW, et al. Effect of early surgery vs physical therapy on knee function among patients with nonobstructive meniscal tears: the ESCAPE randomized clinical trial. JAMA. 2018;320(13):
37. Vervest AM, Maurer CA, Schambergen TG, de Bie RA, Bulstra SK. Effectiveness of physiotherapy after meniscectomy. Knee Surg Sports Traumatol Arthrosc. 1999;7(6):
38. Yim JH, Seon JK, Song EK, et al. A comparative study of meniscectomy and nonoperative treatment for degenerative horizontal tears of the medial meniscus. Am J Sports Med. 2013;41(7):1565–1570. doi:10.1177/0363546513488518
39. Gauffin H, Tagesson S, Meunier A, Magnusson H, Kvist J. Knee arthroscopic surgery is beneficial to middle-aged patients with meniscal symptoms: a prospective, randomised, single-blinded study. Osteoarthritis Cartilage. 2014;22(11):1808–1816. doi:10.1016/j.joca.2014.07.017
40. He Y, Lin Y, He X, Li C, Lu Q, He J. The conservative management for improving visual analog scale (VAS) pain scoring in greater trochanteric pain syndrome: a Bayesian analysis. BMC Musculoskelet Disord. 2023;24(1):423. doi:10.1186/s12891-023-06443-5
41. Howell R, Kumar NS, Patel N, Tom J. Degenerative meniscus: pathogenesis, diagnosis, and treatment options. World J Orthop. 2014;5(5):597–602. doi:10.5312/wjo.v5.i5.597
42. Neogi DS, Kumar A, Rijal L, Yadav CS, Jaiman A, Nag HL. Role of nonoperative treatment in managing degenerative tears of the medial meniscus posterior root. J Orthop Traumatol. 2013;14(3):193–199. doi:10.1007/s10195-013-0234-2
43. Ma J, Chen H, Liu A, Cui Y, Ma X. Medical exercise therapy alone versus arthroscopic partial meniscectomy followed by medical exercise therapy for degenerative meniscal tear: a systematic review and meta-analysis of randomized controlled trials. J Orthop Surg Res. 2020;15(1):219. doi:10.1186/s13018-020-01741-3
44. Rotini M, Papalia G, Setaro N, et al. Arthroscopic surgery or exercise therapy for degenerative meniscal lesions: a systematic review of systematic reviews. Musculoskelet Surg. 2023;107(2):127–141. doi:10.1007/s12306-022-00760-z
45. Noorduyn JCA, van de Graaf VA, Willigenburg NW, et al. Effect of physical therapy vs arthroscopic partial meniscectomy in people with degenerative meniscal tears: five-year follow-up of the ESCAPE randomized clinical trial. JAMA Network Open. 2022;5(7):e2220394. doi:10.1001/jamanetworkopen.2022.20394
46. Swart NM, van Oudenaarde K, Reijnierse M, et al. Effectiveness of exercise therapy for meniscal lesions in adults: a systematic review and meta-analysis. J Sci Med Sport. 2016;19(12):990–998. doi:10.1016/j.jsams.2016.04.003
47. Ozeki N, Koga H, Sekiya I. Degenerative meniscus in knee osteoarthritis: from pathology to treatment. Life. 2022;12(4):603. doi:10.3390/life12040603
48. Luc-Harkey BA, Safran-Norton CE, Mandl LA, Katz JN, Losina E. Associations among knee muscle strength, structural damage, and pain and physical function in individuals with osteoarthritis and symptomatic meniscal tear. BMC Musculoskelet Disord. 2018;19(1):258. doi:10.1186/s12891-018-2182-8
49. Duong V, Oo WM, Ding C, Culvenor AG, Hunter DJ. Evaluation and treatment of knee pain: a review. JAMA. 2023;330(16):1568–1580. doi:10.1001/jama.2023.19675
50. van der Heijden RA, Lankhorst NE, van Linschoten R, Bierma-Zeinstra SM, Van middelkoop M. Exercise for treating patellofemoral pain syndrome. Cochrane Database Syst Rev. 2015;1(1):Cd010387. doi:10.1002/14651858.CD010387.pub2
51. Zeng CY, Zhang ZR, Tang ZM, Hua FZ. Benefits and mechanisms of exercise training for knee osteoarthritis. Front Physiol. 2021;12:794062. doi:10.3389/fphys.2021.794062
52. Coombs R, Garbutt G. Developments in the use of the hamstring/quadriceps ratio for the assessment of muscle balance. J Sports Sci Med. 2002;1(3):56–62.
53. Sadeghi A, Rostami M, Khanlari Z, et al. Effectiveness of muscle strengthening exercises on the clinical outcomes of patients with knee osteoarthritis: a randomized four-arm controlled trial. Caspian J Intern Med. 2023;14(3):433–442. doi:10.22088/cjim.14.3.433
54. Monk AP, Davies LJ, Hopewell S, Harris K, Beard DJ, Price AJ. Surgical versus conservative interventions for treating anterior cruciate ligament injuries. Cochrane Database Syst Rev. 2016;4(4):Cd011166. doi:10.1002/14651858.CD011166.pub2
55. Tamer TM. Hyaluronan and synovial joint: function, distribution and healing. Interdiscip Toxicol. 2013;6(3):111–125. doi:10.2478/intox-2013-0019
56. Di Rosa M, Castrogiovanni P, Musumeci G. The synovium theory: can exercise prevent knee osteoarthritis? The role of “mechanokines”, a possible biological key. J Funct Morphol Kinesiol. 2019;4(1). doi:10.3390/jfmk4010011
57. Joyner MJ, Casey DP. Regulation of increased blood flow (hyperemia) to muscles during exercise: a hierarchy of competing physiological needs. Physiol Rev. 2015;95(2):549–601. doi:10.1152/physrev.00035.2013
58. Ott LW, Resing KA, Sizemore AW, et al. Tumor Necrosis Factor-alpha- and interleukin-1-induced cellular responses: coupling proteomic and genomic information. J Proteome Res. 2007;6(6):2176–2185. doi:10.1021/pr060665l
59. Scheffer DDL, Latini A. Exercise-induced immune system response: anti-inflammatory status on peripheral and central organs. Biochim Biophys Acta Mol Basis Dis. 2020;1866(10):165823. doi:10.1016/j.bbadis.2020.165823
60. Basso JC, Suzuki WA. The effects of acute exercise on mood, cognition, neurophysiology, and neurochemical pathways: a review. Brain Plast. 2017;2(2):127–152. doi:10.3233/bpl-160040
61. Dfarhud D, Malmir M, Khanahmadi M. Happiness & health: the biological factors- systematic review article. Iran J Public Health. 2014;43(11):1468–1477.
62. Sprouse-Blum AS, Smith G, Sugai D, Parsa FD. Understanding endorphins and their importance in pain management. Hawaii Med J. 2010;69(3):70–71.
63. Grothusen JR, Blendy JA, Barr GA. A brief overview of the neuropharmacology of opioid addiction. Transl Perioper Pain Med. 2022;9(4):491–496. doi:10.31480/2330-4871/165
64. Surakanti A, Demory Beckler M, Kesselman MM. Surgical versus non-surgical treatments for the knee: which is more effective? Cureus. 2023;15(2):e34860. doi:10.7759/cureus.34860
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.