")
Back to Journals » Journal of Inflammation Research » Volume 18
Clinical Value of Complement C3a, C5a, and sC5b-9 in Evaluating the Severity of Patients with Severe Fever with Thrombocytopenia Syndrome
Authors Chen T , Liu Y, Liu Y, Hu N, Dai Y, Zhu C , Han Y, Jin K, Li J
Received 11 February 2025
Accepted for publication 26 June 2025
Published 10 July 2025 Volume 2025:18 Pages 9001—9014
DOI https://doi.org/10.2147/JIR.S520425
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Tianyan Chen,1,* Yawen Liu,2,* Yuan Liu,1 Nannan Hu,1 Yan Dai,1 Chuanlong Zhu,1 Yaping Han,1 Ke Jin,1 Jun Li1
1Department of Infectious Disease, the First Affiliated Hospital with Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China; 2Department of Clinical Medical Engineering, the First Affiliated Hospital with Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jun Li; Ke Jin, Department of Infectious Disease, the First Affiliated Hospital with Nanjing Medical University, No. 300 Guangzhou Road, Nanjing, Jiangsu, 210029, People’s Republic of China, Email [email protected]; [email protected]
Purpose: Hyperactive immune responses in severe fever with thrombocytopenia syndrome (SFTS) is considered to associated with disease severity, prognosis and complications. This article aims to evaluate the validity of complement C3a, C5a, and sC5b-9 in predicting the severity and clinical outcomes in SFTS.
Patients and Methods: Patients diagnosed with SFTS at the First Affiliated Hospital with Nanjing Medical University from March to November 2021 were enrolled in this retrospective analysis. The study evaluated C3a, C5a, and sC5b-9 levels between SFTS patients and healthy controls. The diagnostic and prognostic efficiency of C3a, C5a, and sC5b-9 for SFTS was assessed utilizing receiver operating characteristic (ROC) curve analysis. Correlation analysis was performed to examine the relationships between these complement components and clinical laboratory parameters in SFTS patients.
Results: A total of 67 hospitalized SFTS patients were enrolled. SFTS patients exhibited significantly higher concentrations of C3a, C5a, and sC5b-9 compared to healthy controls. Non-survival and severe SFTS patients had notably higher C3a and sC5b-9 levels than survival and mild, respectively. ROC curve analysis revealed that C3a and sC5b-9 demonstrated effective performance for distinguishing severity in SFTS patients, with the area under the curve (AUC) of 0.784 (95% CI: 0.671– 0.896, p < 0.001) and 0.703 (95% CI: 0.573– 0.832, p = 0.005), respectively. The correlation analysis indicated that C3a and sC5b-9 positively correlated with SFTS RNA, CRP, PCT, ALT, AST, ALP, LDH, CK, HBDH, APPT, TT and D-dimer, while C3a negatively correlated with PLT.
Conclusion: This study revealed abnormalities in complement components among patients with SFTS. C3a and sC5b-9 levels show promise as biomarkers for linking with disease severity and prognosis, potentially providing therapeutic targets for the management of SFTS patients and guide future mechanistic research.
Keywords: severe fever with thrombocytopenia syndrome, complement anaphylatoxins, sC5b-9, risk factors
Introduction
Severe fever with thrombocytopenia syndrome (SFTS) is a highly lethal and acute zoonotic disease predominantly caused by severe fever with thrombocytopenia syndrome virus (SFTSV), which belongs to the genus bandavirus in the family Phenuiviridae, order Bunyavirales and has been officially named Dabie bandavirus (DBV).1 SFTS is chiefly transmitted by bites from infected ticks, but there is evidence that it can also be transmitted between people, mainly through close contact with the blood and bodily fluids of infected individuals.2–4 The SFTS presents with non-specific clinical manifestations primarily encompassing abrupt onset of high fever, diarrhea, fatigue, headache, nausea, vomiting, leukopenia, thrombocytopenia, coagulation abnormalities, and neurological symptoms. In critically patients with SFTS, the clinical condition may progress very rapidly, eventually leading to disseminated intravascular coagulation (DIC), multiple organ dysfunction, and even death.5 SFTS has been ranked by the World Health Organization among the priority infectious diseases because of its high fatality rate, wide geographic distribution, economic strain on families, and the potential for pandemics.6 The precise mechanisms underlying DBV pathogenesis remain incompletely elucidated. Treatment for SFTS is primarily symptomatic, with no specific antiviral drugs or effective vaccines available for treatment and prevention regrettably.7 Consequently, identifying risk factors and early intervention indicators associated with severe illness and death in SFTS are crucial to reducing mortality in patients.
The complement system is crucial for innate immunity consisting of soluble factors and cell surface receptors, generally provides the initial defense against pathogen infections. The complement system is increasingly recognized for playing an emerging role in various viral infections.8 C3a, C5a, and sC5b-9 stand as potent molecules in complement system, regulating chemotaxis of immune cells and inflammasome activation. Research indicates that complement activation, particularly the generation of anaphylatoxins C5a, is related to the progress of acute lung injury triggered by influenza A.9 Similarly, C5a may sustain inflammation during the immunopathological stage of COVID-19.10 The anaphylatoxins C3a expressed more upstream in the complement cascade response, may play the similar role to C5a in COVID-19. It has been shown that the inhibition of C3, which blocking the production of C3a and C5a, effectively reduces lung inflammation.11,12 In addition, sC5b-9 and C5a have been shown to co-mediate tissue damage following viral infection.13 Currently, there is scarce knowledge about complement and its clinical implications in DBV infection. Analysis of the single-cell landscape of fatal SFTS revealed that complement activation, especially the overactivated complement systems in intermediate monocytes, is seen as a key characteristic of DBV infection and is linked to negative outcomes,14 suggesting that complement and immune cells may jointly affect the disease progression of SFTS patients. This study aims to evaluate the clinical value of C3a, C5a, and sC5b-9 in the progression of SFTS, and to provide guidance for clinical practice in evaluating the condition and prognosis of SFTS patients.
Materials and Methods
Study Design and Participants
The retrospective study involved 107 admitted SFTS patients treated at the First Affiliated Hospital with Nanjing Medical University between March 2021 and November 2021. The diagnostic criteria of SFTS were as followed the 2023 edition of the diagnosis and treatment scheme on SFTS: patients with a history of employment, residing, or traveling in hills, forested, mountainous regions during the epidemic season, or history of being bitten by tick, or close contact with SFTSV-infected people or animals; patients consistent with clinical performance; patients with multiple organ function impairment; patients with positive DBV RNA.15 A total of 40 patients met the exclusion criteria: (1) patients with other viral infections; (2) patients with autoimmune disease; (3) patients with malignancies; (4) patients with rheumatological diseases, hematologic diseases, thyroid diseases, chronic renal failure, chronic liver disease, allergic disease, pregnancy, immunosuppressive medication, and transfusion of blood products within two weeks; (5) missing clinical data; (6) clinical outcomes are inconclusive. Ultimately, there are 67 patients fulfilled the inclusion criteria and were enrolled in the current survey (Figure 1). In addition, plasma samples from 24 individuals were analyzed as healthy controls. SFTS patients are classified as severe group if they meet at least one of the following criteria: acute respiratory distress syndrome (ARDS), DIC, encephalitis, infection-induced toxic shock, sepsis, failure of one or more organs, multi-organ dysfunction (MODS), or death.16 The study has shown that the critical time point for the progression of SFTS is the 7th day of the course of the disease.17 Blood samples were collected for detecting C3a, C5a, and sC5b-9 from the same SFTS patient cohort during the acute phase (within 7 days post-onset) and the convalescent phase (8–28 days post-onset), with the interval of illness being at least 3 days. The study was approved by the Research and Ethics Committee of the First Affiliated Hospital with Nanjing Medical University. This work was conducted in accordance with the principles of the Declaration of Helsinki.
 |
Figure 1 Illustrative overview of the research design. |
Data Collection
Clinical data of SFTS patients were collected from electronic medical records system, including demographic characteristics, laboratory parameters, and prognosis. The diagnostic criteria for SFTS patients with central nervous system (CNS) is defined as described above.18 Blood samples were collected by a team of professional nurses using standardized EDTA-anticoagulated tubes. Collected blood samples were centrifuged at 1500 × g for 15 minutes within 20 minutes, and the temperature was maintained at 4 °C throughout the process. The plasma was then immediately transferred to Eppendorf tubes and stored at −80 °C. Severe fever with thrombocytopenia syndrome bunyavirus nucleic acid detection kit (Da’an gene Co., Ltd., China) was used to quantitatively measure the viral load of DBV with a positive assessment standard ≥ 4.96×103 copies/mL.19 RT-qPCR was performed in the QuantStudioTM3 system (Applied Biosystems, United States). Patients who discontinued therapy and were automatically discharged were monitored for outcomes through phone calls for 28 days from the start of admission. The concentrations of C3a, C5a (Hycult Biotech, USA), and sC5b-9 (BD Biosciences, USA) in plasma were measured by ELISA using commercial kits, following the standard procedures provided by manufacturer’s instructions. In Brief, plasma samples were diluted following the guideline for dilution of samples. A volume of 100 μL from the diluted sample was transferred to the designated microplate wells and allowed to incubate for 60 minutes. Then, 100 μL of diluted tracer solution was added to each well after washing, followed by another 60-minute incubation. After a subsequent wash, 100 μL of diluted streptavidin peroxidase solution was added with the microplate was incubated for another hour. The procedure concluded with the addition of 100 μL TMB substrate, and termination with stop solution at the appropriate time. All incubations were performed at room temperature, and the optical density (OD) was measured at 450 nm. The standard curve for each complement component was derived by measuring the OD values through serially diluted standard samples with predetermined complement concentrations.
Statistical Analysis
All data were analyzed using SPSS version 25.0 (SPSS Inc., USA) and GraphPad Prism 9.3 (GraphPad Software Inc., USA). Categorical variables were expressed as frequencies and percentages, and analyzed by Chi-square test between the two groups. Continuous variables that followed normal distribution were presented as mean ± standard deviation ( ) and were compared with the Student’s t test, whereas non-normal distribution were presented as medians with interquartile range (IQR) and were compared with the Mann–Whitney U-test. Wilcoxon matched-pairs signed rank test was employed to compare complement components between acute phase and convalescent phase in the same SFTS patient cohort. Correlations between numerical variables were analyzed by Pearson correlation analysis and Spearman correlation analysis, with correlations considered significant if r > 0.2 and p < 0.05. Receiver operating characteristic (ROC) curve analysis were used to evaluate optimal cutoff values and the prognostic value of the risk factors. Differences with a two-tailed p < 0.05 were considered statistically significant, and the area under the curve (AUC) > 0.7 was considered of clinical value.
) and were compared with the Student’s t test, whereas non-normal distribution were presented as medians with interquartile range (IQR) and were compared with the Mann–Whitney U-test. Wilcoxon matched-pairs signed rank test was employed to compare complement components between acute phase and convalescent phase in the same SFTS patient cohort. Correlations between numerical variables were analyzed by Pearson correlation analysis and Spearman correlation analysis, with correlations considered significant if r > 0.2 and p < 0.05. Receiver operating characteristic (ROC) curve analysis were used to evaluate optimal cutoff values and the prognostic value of the risk factors. Differences with a two-tailed p < 0.05 were considered statistically significant, and the area under the curve (AUC) > 0.7 was considered of clinical value.
Results
Demographic Characteristics and Clinical Laboratory Parameters in the SFTS Patients
A total of 67 eligible SFTS patients were finally enrolled in the study, comprising 32 males (47.8%) and 35 females (52.2%), with a median age of 66.0 (IQR 56.0–71.0) years. Among them, 37 (55.2%) patients were classified as the severe group, with a median age of 67.0 (IQR 63.5–73.0) years, while 30 (44.8%) patients, with a median age of 61.5 (IQR 52.0–69.0) years, were categorized into the mild group. There was significant difference between mild and severe groups in age (p < 0.05) but not in gender. As presented in Table 1, baseline demographic characteristics and laboratory indicators were comprehensively compared between mild and severe patients on admission. Fever was observed as the first symptom at the onset of illness in most patients (94.0%), and a higher proportion of severe patients had the symptoms of CNS manifestations and lymph node enlargement in contrast to the mild group. No significant differences were observed between diabetes and hypertension regarding underlying diseases. Subsequent analysis evaluated the differences in peripheral blood parameters between the two groups. Specifically, the viral load exhibited a significant increase in the severe group in comparison to the mild group (p < 0.001), while inflammatory parameters including PCT and CRP were also higher than those in mild patients. With respect to biochemical indexes, the severe group exhibited significantly higher levels of ALT, AST, LDH, CK, HBDH, and Urea. In addition, there was significant increase of coagulation indicators (PT, APTT, TT, D-D) between the two groups, and a lower level of PLT and FIB were observed in severe patients (all p < 0.05).
 |
Table 1 Comparisons of Clinical Characteristics Between Mild and Severe in SFTS Patients |
Altered Complement Components Observed in SFTS Patients
Complement components including C3a, C5a, and sC5b-9 were measured in both SFTS patients and healthy controls to investigate the levels of complement in SFTS patients. The levels of C3a, C5a, and sC5b-9, which are involved in the common pathway of complement activation, were significantly elevated in the SFTS group compared to healthy controls (all p < 0.001) (Figure 2A–C). Specifically, the level of C3a in healthy controls was 86.838 (60.013–150.609) ng/mL, while in SFTS patients it was 397.684 (239.112–563.149) ng/mL. In addition, the concentrations of C5a and sC5b-9 in the healthy controls were 29.027 (16.638–77.149) pg/mL and 185.820 (134.575–222.856) ng/mL, while in SFTS patients, the concentrations of C5a and sC5b-9 were 349.359 (53.956–615.217) pg/mL and 534.331 (312.500–1000.014) ng/mL, respectively.
 |
Figure 2 Comparison of complement components in SFTS patients and healthy individuals. (A) Levels of C3a between SFTS patients and healthy controls. (B) Levels of C5a between SFTS patients and healthy controls. (C) Levels of sC5b-9 between SFTS patients and healthy controls. Abbreviations: HC, healthy controls; SFTS, severe fever with thrombocytopenia syndrome. Notes: Data are presented using mean ± standard deviation. The significant difference between the two groups is designated by an asterisk (*). ***p< 0.001. |
Significant Increase in C3a and sC5b-9 Levels Observed in Severe and Fatal SFTS Patients
To examine the clinical significance of complement components in SFTS, we analyzed and compared the levels of C3a, C5a, and sC5b-9 between severe and mild patients, as well as survivors and non-survivors. Our findings revealed that both C3a and sC5b-9 were significantly higher in severe SFTS patients than in mild patients. The level of C3a was 288.772 (202.879–418.069) ng/mL in the mild group, and was 529.023 (370.802–716.600) ng/mL in critically ill patients (p < 0.001) (Figure 3A). Correspondingly, the sC5b-9 level was 450.532 (310.197–522.805) ng/mL in mild patients and 761.140 (382.260–1695.132) ng/mL in severe group (p = 0.005) (Figure 3C), nevertheless, no significant difference was observed in C5a levels between the two groups (p = 0.890) (Figure 3B). Additionally, we examined complement components in survival (n = 58) and non-survival patients (n = 9). The results indicate significantly increase in C3a and sC5b-9 levels among non-survival patients (Figure 3D and F). The concentration of C3a in the survival group was 349.417 (218.003–497.522) ng/mL, and in the fatal group it was 826.545 (640.035–1307.216) ng/mL (p < 0.001). The concentration of sC5b-9 in the survival group was 484.169 (310.197–774.832) ng/mL, and was 4184.018 (1041.007–12,553.546) ng/mL in the fatal group (p < 0.001). Similarly, there was no significant difference in C5a concentration between survivors and non-survivors (p = 0.869).
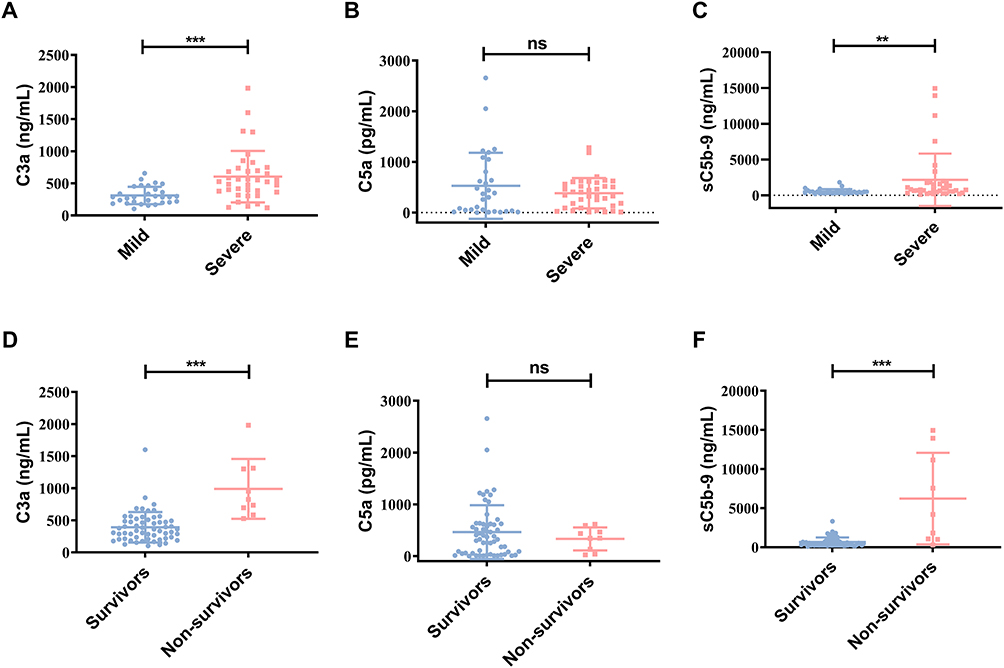 |
Figure 3 Comparison of complement components in SFTS patients. (A–C) Levels of C3a, C5a, sC5b-9 between mild and severe patients. (D–F) Levels of C3a, C5a, sC5b-9 between survival and non-survival patients with SFTS. Notes: Data are presented using mean ± standard deviation. The significant difference between the two groups is designated by an asterisk (*). **p < 0.01, ***p < 0.001. “ns” indicates not statistically significant. |
Dynamic Changes in the Complement Levels Among SFTS Patients
We further divided SFTS patients into acute and convalescent phases according to the time of onset. The results showed that C3a and sC5b-9 levels were elevated significantly at acute phase in comparison with convalescent phase in the same cohort of patients (Figure 4A and C). The concentrations of C3a in acute phase and convalescent phase were 397.684 (209.576–563.180) ng/mL and 187.968 (139.817–392.623) ng/mL, respectively (p = 0.001). Similarly, sC5b-9 concentrations showed a marked reduction from 458.386 (305.682–1139.178) ng/mL in the acute phase to 269.659 (132.217–480.724) ng/mL in the convalescent phase (p < 0.001). There was no significant difference of C5a between two phases (p = 0.820) (Figure 4B).
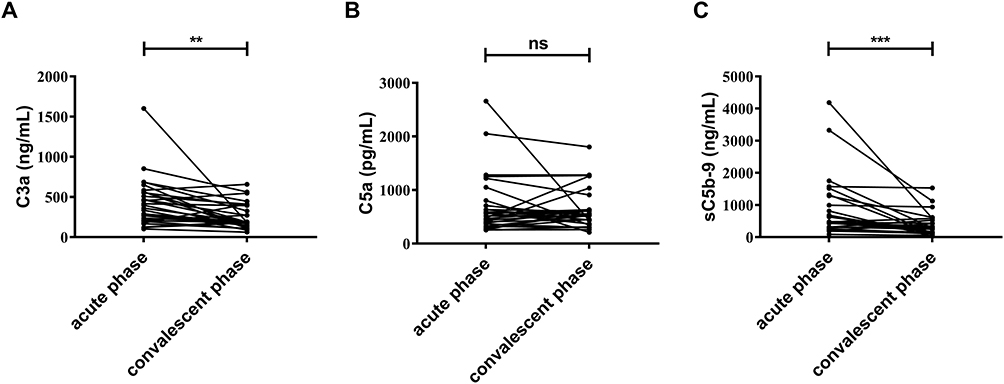 |
Figure 4 Dynamic changes in the complement levels among SFTS patients. (A) Comparison of C3a levels in the same cohort of SFTS patients during the acute and convalescent phases. (B) Comparison of C5a levels in the same cohort of SFTS patients during the acute and convalescent phases. (C) Comparison of sC5b-9 levels in the same cohort of SFTS patients during the acute and convalescent phases. Note: The significant difference between the two groups is designated by an asterisk (*). **p < 0.01, ***p < 0.001. “ns” indicates not statistically significant. |
Correlation Analysis Between Complement Components and Clinical Laboratory Indicators in Patients with SFTS
The correlation analysis of C3a, C5a, and sC5b-9 with laboratory parameters in SFTS patients was conducted by Pearson correlation coefficient and Spearman correlation coefficient (Figure 5). Quantifying viral load and inflammatory biomarker levels during hospitalization, we found the C3a and sC5b-9 levels showed significant positive correlation with viral load (r = 0.536, p < 0.001; r = 0.616, p < 0.001), CRP (r = 0.379, p = 0.002; r = 0.416, p < 0.001) and PCT (r = 0.421, p < 0.001; r = 0.367, p = 0.002). Given the significant coagulation abnormalities observed in SFTS patients, our research indicated that the C3a and sC5b-9 also showed positive correlation with D-D (r = 0.557, p < 0.001; r=0.361, p=0.003), TT (r = 0.415, p < 0.001; r=0.380, p=0.002), and APTT (r = 0.406, p = 0.001; r = 0.338, p = 0.005). Furthermore, the results revealed positive correlation between C3a and both ALT (r = 0.472, p < 0.001), AST (r = 0.572, p < 0.001), ALP (r = 0.255, p = 0.038), LDH (r = 0.400, p = 0.001), CK (r = 0.357, p = 0.003), HBDH (r = 0.451, p < 0.001), and BUN (r = 0.252, p = 0.039), while demonstrating significant negative correlation with PLT (r = −0.294, p = 0.016). sC5b-9 was positively correlated with ALT (r = 0.410, p = 0.001), AST (r = 0.514, p < 0.001), ALP (r = 0.274, p = 0.025), GGT (r = 0.286, p = 0.019), LDH (r = 0.373, p = 0.002), CK (r = 0.265, p = 0.030), and HBDH (r = 0.475, p < 0.001). There was no significant correlation between laboratory parameters and C5a.
 |
Figure 5 Correlation analysis of complement C3a, C5a, sC5b-9 with clinical parameters. Note: The significant difference between the two groups is designated by an asterisk (*). *p < 0.05. |
ROC Analysis for Predicting Disease Severity Risk of Complement Components in SFTS Patients
ROC curve analysis was used to assess C3a, C5a, and sC5b-9 for their ability to distinguish between severe and mild patients (Figure 6). The AUCs of the C3a and sC5b-9 were 0.784 (95% CI: 0.671–0.896, p < 0.001) and 0.703 (95% CI: 0.573–0.832, p = 0.005), respectively. The sensitivity and specificity of C3a at a optimal cutoff value of 362.046 ng/mL were 0.784 and 0.733. And the optimal cutoff value for sC5b-9 was 516.867 ng/mL, determined by the maximum Youden index, yielding a sensitivity of 0.730 and a specificity of 0.767 for predicting severity in SFTS patients (Table 2). However, the AUC of C5a for severe outcome was 0.510 (p > 0.05). These findings highlight the potential of C3a and sC5b-9 as prognostic indicators for predicting severity of SFTS patients.
 |
Table 2 ROC Analysis of Complement Biomarkers for Predicting Severe Disease in SFTS Patients |
 |
Figure 6 Analysis of receiver operating characteristic (ROC) curve to assess the ability of C3a, C5a, and sC5b-9 in distinguishing between mild and severe patients. |
Discussion
Since its discovery in 2009, SFTS has been characterized by a rapid onset and high lethality, which poses a major challenge. The disease remains primarily endemic to Asia and has been increasing in incidence in recent years, with morbidity rates of 5–40% and an average mortality rate of 12.2%. Our study examined 67 patients with SFTS, yielding a mortality rate of 13.43%. Early-stage SFTS lacks distinctive clinical symptoms. High levels of AST, LDH, APTT, and viral load, along with advanced age and neurological symptoms, are established risk factors for poor clinical outcomes.20,21 In our study, fever was present in 94.0% of SFTS patients, followed by fatigue, diarrhoea, nausea, vomiting, rigor, and myalgia as common clinical manifestations. Our study also found that patients with SFTS were more common in the elderly population, and the occurrence of CNS manifestations and lymph node enlargement was more frequent in severe patients. SFTS can inflict damage on various organs. This study provided a comprehensive analysis of laboratory indicators indicative of multi-organ injury in DBV-infected patients, including hematology, liver function indicators, myocardial function indicators, renal function indicators, coagulation indicators, and infection indicators. Comparison of the parameters between the mild and severe groups revealed that viral load, PCT, liver function parameters including AST and ALT, cardiac enzyme parameters (LDH, CK, HBDH) and coagulation indicators were more critical in severe cases, which is consistent with previous reports.20,22
The underlying mechanism of SFTS viruses remains unclear. Bunyaviruses commonly contribute to lethal outcomes through excessive inflammation triggered by mitochondrial dysfunction following DBV infection.23–26 In severe and critically ill cases, the aberrant production of pro-inflammatory and anti-inflammatory cytokines may trigger the systemic inflammatory response syndrome (SIRS), which elevates the risk of secondary infections, multiple organ failure, and fatal outcomes.27–29 Early diagnosis and effective symptomatic treatment are critical for improving the prognosis of patients with this disease.30 Our study appears to be the first one that explores the role of complement C3a, C5a, and sC5b-9 in prognosis and severity in SFTS. Although the complement system plays a crucial role in protecting against viral pathogens, its excessive activation and dysregulation may lead to extensive systemic damage affecting multiple organs.31,32 The complement cascade response constitutes an intricate network of plasma proteins with major effector fragments, including C1q, C3a, C3b, C5a, and C5b9/MAC, as potent coordinators between the innate and adaptive immune systems. C3a and C5a are powerful and multifaceted complement peptides, often referred to as “anaphylatoxins”. In the context of innate immunity, these peptides play well-defined roles and interact with multiple leukocyte targets, promoting or inhibiting immune cell chemotaxis, granulocyte degranulation, phagocytosis, inflammatory vesicle activation, and cytokine production. Consequently, C3a and C5a are considered as regulators of adaptive immune responses.33 It was determined that the SARS-CoV-2-induced complement activation generates an inflammatory environment that fosters the differentiation of T cells with a high immunopathogenic potential, crucial for the infectious progression. Complement C5a, C3a, and serum inflammatory cytokine levels were positively correlated with in-hospital mortality in critical patients of COVID-19, emphasizing the complement system’s potential for predicting severity and mortality in COVID-19.34 Furthermore, elevated C3a production was observed in adenovirus type 7 (HAdV-7) infections, triggering cytotoxic effects and higher viral loads in the lungs, accompanied by an increase in proinflammatory cytokines.35 In this study, we focused on complement cascade activation in SFTS patients after DBV infection in vivo. We found that anaphylatoxins (C3a, C5a) and soluble membrane attack complex (sC5b-9) were all significantly higher in SFTS patients than in healthy controls. Further, C3a and sC5b-9 levels were consistently increased in critical patients and non-surviving patients. This suggests that the body initiates complement immune responses following DBV infection, which may serve as an indicator of the severity of the viral infection. Previous studies have also shown that the complement cascade is a prominent feature of DBV infection, and in deceased SFTS patients, viral infection significantly induced the secretion of C3b/iC3b and complement factor D in the complement cascade.36
The analysis of dynamic laboratory indicators revealed a critical time point of 7 days following the onset of SFTS.17 We compared the dynamic levels of complement components in the acute phase (4–7 days after onset) and the convalescent phase (8–20 days after onset). Longitudinal analyses revealed that the concentrations of complement proteins (C3a and sC5b-9) decreased over time, with both C3a and sC5b-9 being higher in the acute phase than in the convalescent phase, implying that they may predict the prognosis of SFTS in its early stages. In general, C3a and sC5b-9 contribute to the acute response and are quickly cleared from the circulation by receptor involvement or secretion.37 Some soluble forms of some activated complement components remain stable during storage at 4°C after thawing and freezing.38 The fact that such a high concentration of complement components is present in SFTS says a lot about the speed of its production and may be a sign of complement system activation. We assume that this is caused by active viral replication, but more research is needed to confirm this. In view of complement and inflammation are closely cross-talking, high concentration of complement proteins in the acute phase may promote inflammation after DBV infection.39 Consequently, we investigated the relationship between complement and biomarkers, including indicators of inflammation in acute phase. Notably, we found that high C3a and sC5b-9 levels were positively correlated with high DBV viral load, which itself was associated with severe disease progression and similarly predicted poor outcome.40 Severe SFTS often accompanied by inflammatory response, and previous research has shown that ferritin and PCT serve as discriminative inflammatory biomarkers of SFTS in its early stages.41 Our study evaluated the association between complement proteins and indicators of inflammation subsequently. The results show that PCT levels are elevated in severe SFTS patients, and C3a and sC5b-9 are positively correlated with PCT. In addition, abnormalities in other early predictors of adverse outcomes in SFTS patients were associated with a higher risk of death from SFTS, aiding in identifying those at high risk for severe complications.20 Thrombocytopenia is a defining hallmark of SFTS, and it may be related to increased cytokine network activation, endothelial cell dysfunction, and abnormal coagulation reactions. Patients who died with severe PT, APTT, TT prolongation, and increased D-dimer levels, indicating a risk of disseminated intravascular coagulation and thus mortality.42,43 In view of the relationship between the complement and coagulation pathways which has long been recognized, it may be associated with coagulation dysfunction and hemorrhagic risk following DBV infection.44 This study showed that coagulation indices and PLT were affected in patients with SFTS, more so in critical patients. C3a and sC5b-9 were correlated with coagulation parameters (D-D, TT, APTT), and C3a was positively correlated with PLT. Our study also revealed that the levels of C3a and sC5b-9 were positively correlated with severity indicators such as ALT, AST, ALP, CK, HBDH, and LDH. This suggests that elevated levels of C3a and sC5b-9 are associated with increased impairment of liver, myocardial, and renal function to varying extents. The ROC curve analysis indicates that the sensitivity and specificity for predicting SFTS severity were higher when the concentration of C3a and sC5b-9 was above 362.046 ng/mL and 516.867 ng/mL, respectively.
In the current investigation, we observed elevated C5a in SFTS patients compared to healthy controls. Unfortunately, we were unable to detect activation of the C5 axis in critical patients or throughout disease dynamics. C5a is a powerful allergenic toxin, ranking just below C3a in potency. It serves as a significant activator of neutrophils, monocytes, and macrophages. This activation typically results in smooth muscle contraction, vasodilation, and increased vascular permeability. Additionally, C5a induces the degranulation of basophils and mast cells, leading to the release of lysosomal enzymes. These processes collectively contribute to the release of proinflammatory cytokines and the induction of inflammation. Given these properties, it has been implicated as a driver or exacerbator of pathology in a variety of inflammatory or autoimmune diseases.45 Circulating neutrophils possess high-affinity C5a receptors (C5aR), which rapidly bind C5a, resulting in its brief half-life of approximately one minute. C5a can only be tested in plasma after C5aR has been saturated on leukocytes, making it technically challenging to detect. However, this does not mean that C5a is not formed during DBV infection, as we demonstrated significantly increased C5a concentrations in SFTS patients compared to healthy controls. There was no significant difference in C5a between severe and mild cases, as well as between death and survival in SFTS patients. We considered that the difference might be distinguished due to the low concentration of C5a in plasma or the low sensitivity of the reagent.
Nevertheless, our study has some limitations that must be noted. Firstly, this is a single-center retrospective study, and considering the small sample size of this study, more studies are needed to prove the interaction between complement C3a and sC5b-9 and SFTS. Secondly, we only analyzed anaphylatoxin (C3a and C5a) and the membrane attack complex (sC5b-9), and did not involve other complement system molecules and regulatory factors. At the same time, the mechanism between complement molecules and the immune system or virus is not clear. Therefore, further multicenter, large-sample, prospective randomized controlled trials and systematic mechanism exploration are still needed to confirm the role of the complement system in DBV infection.
Conclusion
This study demonstrated significant abnormalities in complement components of SFTS patients, characterized by notable increase of C3a, C5a, and sC5b-9. Additionally, we evaluated the potential utility of C3a and sC5b-9 as diagnostic and prognostic biomarkers for DBV infection and aids in risk stratification among SFTS patients. The evaluation of complement activation markers may serve as a monitoring tool for disease severity and a reference for therapeutic strategies during SFTS epidemic seasons.
Abbreviations
SFTS, severe fever with thrombocytopenia syndrome; CRP C-reactive protein; PCT, procalcitonin; ALT, alanine aminotransferase; AST, aspartate aminotransferase; ALP, alkaline phosphatase; LDH, lactate dehydrogenase; CK, creatine kinase; HBDH, hydroxybutyrate dehydrogenase; APPT, activated partial thromboplastin time; TT, thrombin time; D-D, D-dimer; PLT, platelet; SFTSV, severe fever with thrombocytopenia syndrome virus; DBV, Dabie bandavirus.
Data Sharing Statement
The datasets during and/or analyzed during the current study available from the corresponding author (Please contact Jun Li, [email protected]) on reasonable request. The data are not publicly available due to privacy or ethical restrictions.
Ethics Approval and Consent to Participate
This study was approved by the Research and Ethics Committee of the First Affiliated Hospital with Nanjing Medical University (No.2022-SR-633). Written informed consent was obtained from each enrolled patient or their guardians.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Supported by the National Natural Science Foundation of China (No. 81871242).
Disclosure
All authors report no conflicts of interest in this work.
References
1. Casel MA, Park SJ, Choi YK. Severe fever with thrombocytopenia syndrome virus: emerging novel phlebovirus and their control strategy. Exp Mol Med. 2021;53(5):713–722. doi:10.1038/s12276-021-00610-1
2. Seo JW, Kim D, Yun N, Kim DM. Clinical update of severe fever with thrombocytopenia syndrome. Viruses. 2021;13(7):1213. doi:10.3390/v13071213
3. Zhang N, Mu X, Liu J, Liu T. Risk assessment of human-to-human transmission of severe fever with thrombocytopenia syndrome virus based on 10-year clustered analysis. Front Public Health. 2024;12:1419425. doi:10.3389/fpubh.2024.1419425
4. Huang D, Jiang Y, Liu X, et al. A cluster of symptomatic and asymptomatic infections of severe fever with thrombocytopenia syndrome caused by person-to-person transmission. Am J Trop Med Hyg. 2017;97(2):396–402. doi:10.4269/ajtmh.17-0059
5. Li H, Lu QB, Xing B, et al. Epidemiological and clinical features of laboratory-diagnosed severe fever with thrombocytopenia syndrome in China, 2011-17: a prospective observational study. Lancet Infect Dis. 2018;18(10):1127–1137. doi:10.1016/s1473-3099(18)30293-7
6. Mehand MS, Millett P, Al-Shorbaji F, Roth C, Kieny MP, Murgue B. World Health Organization methodology to prioritize emerging infectious diseases in need of research and development. Emerg Infect Dis. 2018;24(9). doi:10.3201/eid2409.171427
7. Takayama-Ito M, Saijo M. Antiviral drugs against severe fever with thrombocytopenia syndrome virus infection. Front Microbiol. 2020;11:150. doi:10.3389/fmicb.2020.00150
8. Stoermer KA, Morrison TE. Complement and viral pathogenesis. Virology. 2011;411(2):362–373. doi:10.1016/j.virol.2010.12.045
9. Bjornson AB, Mellencamp MA, Schiff GM. Complement is activated in the upper respiratory tract during influenza virus infection. Am Rev Respir Dis. 1991;143(5 Pt 1):1062–1066. doi:10.1164/ajrccm/143.5_Pt_1.1062
10. Chouaki Benmansour N, Carvelli J, Vivier E. Complement cascade in severe forms of COVID-19: recent advances in therapy. Eur J Immunol. 2021;51(7):1652–1659. doi:10.1002/eji.202048959
11. Mastellos DC, Pires da Silva BGP, Fonseca BAL, et al. Complement C3 vs C5 inhibition in severe COVID-19: early clinical findings reveal differential biological efficacy. Clin Immunol. 2020;220:108598. doi:10.1016/j.clim.2020.108598
12. Georg P, Astaburuaga-García R, Bonaguro L, et al. Complement activation induces excessive T cell cytotoxicity in severe COVID-19. Cell. 2022;185(3):493–512.e25. doi:10.1016/j.cell.2021.12.040
13. Magro C, Mulvey JJ, Berlin D, et al. Complement associated microvascular injury and thrombosis in the pathogenesis of severe COVID-19 infection: a report of five cases. Transl Res. 2020;220:1–13. doi:10.1016/j.trsl.2020.04.007
14. Li H, Li X, Lv S, et al. Single-cell landscape of peripheral immune responses to fatal SFTS. Cell Rep. 2021;37(8):110039. doi:10.1016/j.celrep.2021.110039
15. China NHCotPsRo. Diagnosis and treatment scheme for severe fever with thrombocytopenia syndrome(2023 Edition). EB/OL. 2023.
16. Huang T, Fan Y, Xia Y, et al. Association of low HDL-c levels with severe symptoms and poor clinical prognosis in patients with severe fever and thrombocytopenia syndrome. Front Microbiol. 2023;14:1239420. doi:10.3389/fmicb.2023.1239420
17. Hao Y, Sun J, Wang X, et al. Difference in hematocrit and plasma albumin levels as an early biomarker of severity and prognosis in patients with severe fever and thrombocytopenia syndrome. J Med Virol. 2024;96(10):e29941. doi:10.1002/jmv.29941
18. Wang M, Huang P, Liu W, et al. Risk factors of severe fever with thrombocytopenia syndrome combined with central neurological complications: a five-year retrospective case-control study. Front Microbiol. 2022;13:1033946. doi:10.3389/fmicb.2022.1033946
19. Zhang Q, Zhao J, Dai Y, et al. A high viral load in urine correlates with acute kidney injury and poor outcomes in hospitalized patients with severe fever with thrombocytopenia syndrome: a noninvasive and convenient prognostic marker. Open Forum Infect Dis. 2023;10(4):ofad085. doi:10.1093/ofid/ofad085
20. Yang M, Yin M, Hou B, Zhou L, Wang J, Zhao Z. Analysis of early warning indicators of death in patients with severe fever with thrombocytopenia syndrome. BMC Infect Dis. 2024;24(1):765. doi:10.1186/s12879-024-09599-0
21. Zhang YZ, He YW, Dai YA, et al. Hemorrhagic fever caused by a novel Bunyavirus in China: pathogenesis and correlates of fatal outcome. Clin Infect Dis. 2012;54(4):527–533. doi:10.1093/cid/cir804
22. Zhao J, Ge HH, Wang G, et al. Fatal patients with severe fever with thrombocytopenia syndrome in China. Int J Infect Dis. 2022;125:10–16. doi:10.1016/j.ijid.2022.10.008
23. Liu Q, He B, Huang SY, Wei F, Zhu XQ. Severe fever with thrombocytopenia syndrome, an emerging tick-borne zoonosis. Lancet Infect Dis. 2014;14(8):763–772. doi:10.1016/s1473-3099(14)70718-2
24. Li S, Li H, Zhang YL, et al. SFTSV infection induces BAK/BAX-dependent mitochondrial DNA release to trigger NLRP3 inflammasome activation. Cell Rep. 2020;30(13):4370–4385.e7. doi:10.1016/j.celrep.2020.02.105
25. Park A, Park SJ, Jung KL, et al. Molecular signatures of inflammatory profile and B-cell function in patients with severe fever with thrombocytopenia syndrome. mBio. 2021;12(1). doi:10.1128/mBio.02583-20
26. Liu MM, Lei XY, Yu H, Zhang JZ, Yu XJ. Correlation of cytokine level with the severity of severe fever with thrombocytopenia syndrome. Virol J. 2017;14(1):6. doi:10.1186/s12985-016-0677-1
27. Mendoza CA, Ebihara H, Yamaoka S. Immune modulation and immune-mediated pathogenesis of emerging tickborne banyangviruses. Vaccines. 2019;7(4):125. doi:10.3390/vaccines7040125
28. Hu L, Kong Q, Yue C, et al. Early-warning immune predictors for invasive pulmonary aspergillosis in severe patients with severe fever with thrombocytopenia syndrome. Front Immunol. 2021;12:576640. doi:10.3389/fimmu.2021.576640
29. Hu LF, Wu T, Wang B, et al. The regulation of seventeen inflammatory mediators are associated with patient outcomes in severe fever with thrombocytopenia syndrome. Sci Rep. 2018;8(1):159. doi:10.1038/s41598-017-18616-z
30. Zhai Y, Li H, Xia P, et al. Intravenous immunoglobulin‑based adjuvant therapy for severe fever with thrombocytopenia syndrome: a single‑center retrospective cohort study. J Med Virol. 2024;96(11):e70017. doi:10.1002/jmv.70017
31. Carroll MV, Sim RB. Complement in health and disease. Adv Drug Deliv Rev. 2011;63(12):965–975. doi:10.1016/j.addr.2011.06.005
32. Mellors J, Tipton T, Longet S, Carroll M. Viral evasion of the complement system and its importance for vaccines and therapeutics. Front Immunol. 2020;11:1450. doi:10.3389/fimmu.2020.01450
33. Yadav MK, Maharana J, Yadav R, et al. Molecular basis of anaphylatoxin binding, activation, and signaling bias at complement receptors. Cell. 2023;186(22):4956–4973.e21. doi:10.1016/j.cell.2023.09.020
34. Alosaimi B, Mubarak A, Hamed ME, et al. Complement anaphylatoxins and inflammatory cytokines as prognostic markers for COVID-19 severity and in-hospital mortality. Front Immunol. 2021;12:668725. doi:10.3389/fimmu.2021.668725
35. Fu Y, Tang Z, Ye Z, et al. Human adenovirus type 7 infection causes a more severe disease than type 3. BMC Infect Dis. 2019;19(1):36. doi:10.1186/s12879-018-3651-2
36. Lee SY, Yun SH, Lee H, et al. Serum proteomics of severe fever with thrombocytopenia syndrome patients. Clin Proteomics. 2022;19(1):32. doi:10.1186/s12014-022-09368-8
37. Lo MW, Woodruff TM. Complement: bridging the innate and adaptive immune systems in sterile inflammation. J Leukoc Biol. 2020;108(1):339–351. doi:10.1002/jlb.3mir0220-270r
38. Bergseth G, Ludviksen JK, Kirschfink M, Giclas PC, Nilsson B, Mollnes TE. An international serum standard for application in assays to detect human complement activation products. Mol Immunol. 2013;56(3):232–239. doi:10.1016/j.molimm.2013.05.221
39. Barratt-Due A, Pischke SE, Nilsson PH, Espevik T, Mollnes TE. Dual inhibition of complement and toll-like receptors as a novel approach to treat inflammatory diseases-C3 or C5 emerge together with CD14 as promising targets. J Leukoc Biol. 2017;101(1):193–204. doi:10.1189/jlb.3VMR0316-132R
40. Jo HN, Kim J, Hwang SY, et al. Viral load as a factor affecting the fatality of patients suffering from severe fever with thrombocytopenia syndrome. Viruses. 2022;14(5):881. doi:10.3390/v14050881
41. Chen K, Sun H, Geng Y, Yang C, Shan C, Chen Y. Ferritin and procalcitonin serve as discriminative inflammatory biomarkers and can predict the prognosis of severe fever with thrombocytopenia syndrome in its early stages. Front Microbiol. 2023;14:1168381. doi:10.3389/fmicb.2023.1168381
42. Hou H, Zou S, Wei W, et al. Kinetics and prognostic significance of laboratory markers in patients with severe fever with thrombocytopenia syndrome: insight from a comprehensive analysis. J Infect Dis. 2024;229(6):1845–1855. doi:10.1093/infdis/jiad426
43. Deng B, Zhou B, Zhang S, et al. Clinical features and factors associated with severity and fatality among patients with severe fever with thrombocytopenia syndrome bunyavirus infection in Northeast China. PLoS One. 2013;8(11):e80802. doi:10.1371/journal.pone.0080802
44. Pryzdial ELG, Leatherdale A, Conway EM. Coagulation and complement: key innate defense participants in a seamless web. Front Immunol. 2022;13:918775. doi:10.3389/fimmu.2022.918775
45. Mastellos DC, Ricklin D, Lambris JD. Clinical promise of next-generation complement therapeutics. Nat Rev Drug Discov. 2019;18(9):707–729. doi:10.1038/s41573-019-0031-6
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.