")
Back to Journals » Orthopedic Research and Reviews » Volume 17
Combination Hyaluronic Acid and Multipotent Stromal Cells Fails to Improve Rat Knee OA Outcomes Compared to Cells Alone
Authors Davis KM, Hamilton M , Muathe D, Wildey A, Harrington S, Bittel DC, Filla M, Stehno-Bittel L
Received 22 March 2025
Accepted for publication 21 June 2025
Published 11 July 2025 Volume 2025:17 Pages 299—312
DOI https://doi.org/10.2147/ORR.S525292
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Kennedy Michele Davis,1 Megan Hamilton,2 Donald Muathe,2 Aldyn Wildey,2 Stephen Harrington,2 Douglas C Bittel,1 Michael Filla,1 Lisa Stehno-Bittel2,3
1College of Biosciences, Kansas City University, Kansas City, MO, USA; 2Likarda, Inc, Kansas City, MO, USA; 3Department of Rehabilitation Science, University of Kansas Medical Center, Kansas City, KS, USA
Correspondence: Lisa Stehno-Bittel, University of Kansas Medical Center and Likarda, INC, 10330 Hickman Mills Drive, Kansas City, MO, 64137, USA, Tel +1 816 605 6604, Email [email protected]
Introduction: Multipotent Stromal Cells (MSCs) are utilized as therapeutic agents for addressing musculoskeletal conditions, including knee osteoarthritis (OA). However, major challenges in the clinical application include maintenance of the cells in the joint capsule. Hyaluronic acid (HA) is endogenous in synovial joints and commercially available as a joint lubricant. We tested the hypothesis that delivery of MSCs in HA into an OA rat knee model could improve outcomes.
Methods: Rat bone marrow MSCs were suspended in a commercially available HA paste, and cell viability measured with live/dead stains. Biomarkers for MSC chondrogenesis and osteogenesis were monitored with PCR. MSCs with or without HA were injected into the knees of OA rats and histology conducted 6 weeks later.
Results: Suspending MSC in HA resulted in a slight reduction in viability. The gene expression profile showed an increase in MSC biomarkers for cells in HA with a decrease in osteogenic markers. Four groups of treatment (vehicle, MSCs alone, HA alone, MSCs + HA) were injected into the knees of osteoarthritic rats. Pain scores, collected weekly, showed no difference between the groups. Immunohistochemistry for inflammatory markers illustrated no obvious differences between groups. Proteoglycans, indicative of cartilage, showed a loss in the vehicle group and modest signs of cartilage with MSCs alone, but when mixed with the HA, any benefit was lost. OARSI Histological Scoring completed by 2 independent technicians concluded no improvement in joint integrity with the addition of HA.
Conclusion: A commercially available HA failed to enhance joint regeneration compared to MSCs alone.
Keywords: Hyaluronic acid, multipotent stem cell, osteoarthritis
Introduction
Osteoarthritis (OA) affects the knee joint frequently, accounting for 4/5 of all OA cases,1 and many studies suggest that the overall prevalence of knee OA is underreported.2 Surveys have shown that patients with knee OA, receiving medical and surgical interventions, rank their quality of life as poor.3,4 Therefore, it is not surprising that patients and clinicians are searching for alternative therapies.5 In the field of regenerative medicine, multipotent stromal cells (MSCs) are key components of cell therapies characterized by their ability to self-renew, differentiate, and modulate the local immune system.6 MSCs have been shown to be capable of reconstructing bone, cartilage, meniscus, ligaments, tendons, and mesenchymal derived tissues.7 While MSCs can be stimulated to differentiate into tissue-specific cells, they also have the potential to release cytokines and other immunomodulatory factors into the microenvironment that may stimulate endogenous repair of tissues.7,8
Presently in the US, intra-articular (IA) injection of MSCs is a common practice to treat knee OA for the anti-inflammatory effects and potential to regenerate cartilage.9,10 Often, the treatments utilize autologous MSCs aspirated from the adipose tissue of the patient.11 There have been conflicting reports concerning the benefits of MSCs to treat knee OA. While animal studies have shown that MSCs can have positive effects on knee OA by reducing cartilage destruction and improving tissue repair,11–16 there have been conflicting reports concerning the benefits of MSC to treat humans. Some clinical studies have shown improved scores for physical function, pain, and stiffness in the MSC treated group.17–20 One of the largest clinical trials included over 320 OA patients that received autologous adipose-derived MSCs.21 The study concluded that the participants had lower pain scores, improved activity levels and increase cartilage regrowth with the MSC treatment, even two years later. Recently, allogeneic MSCs have been compared directly to microdrilling for human knee OA, and the MSC group had better cartilage regeneration 2 years after the procedure.22 Conversely, other studies and meta-analyses have shown no significant differences with MSC treatment,23–25 and mechanistic studies have shown that when the MSCs are placed in the articular inflammatory microenvironment, their effect is minimal.26 Thus, in spite of hundreds of clinical trials that have been undertaken or are currently underway, no MSC product has been approved to treat knee OA in the US.
One of the main challenges is the well-established fact that the injected MSCs do not remain localized to the knee joint. They are often pushed out of the joint with the forces asserted during weight bearing.27 The lack of cell retention is exacerbated by the high cell death due to exposure to the inflamed environment.26,28,29 In mice, no fluorescently labeled MSCs were detected in the knee 5 days after IA injections.30 In rats only 2% of human MSCs injected into the knees were detected 24 hours later.31 Only in immune-compromised mice the cells appear to last longer in the joint with 15% present 30 days after injection.32 One way to overcome the dramatic cell loss is to inject super-therapeutic doses to ensure that sufficient numbers of live MSCs remain long enough to have an effect33 or turn to repeated injections.28,34 However, high doses and frequent injections increase the cost to the healthcare system and introduce potential safety concerns.35 There is an urgent need for a slow-release delivery system that would protect and trap the cells in the articular space.
Hyaluronan, also known as hyaluronic acid (HA), is a linear polysaccharide that is present in the extracellular matrix of every tissue36 and has been used in eye surgery and wound healing.37 The use of HA to treat OA is not new. Over the past decades several companies have developed advanced HA preparations advertised as joint lubricants.38 In fact, stem cells in HA gels have been injected into large animal OA models with superior outcomes compared to HA alone39 and in select countries preparations of HA mixed with stem cells are commercially sold.40,41 The rational for the current study was to determine whether a suspension of MSCs delivered in a commercially sold HA, Monovisc, could have synergistic effects improving the outcomes of knee OA.
Methods
Multipotent Stromal Cells
Rat Bone Marrow MSCs were obtained from Cyagen Biosciences (Santa Clara, CA; RASMX-01001) and expanded and cultured according to the manufacturer’s instructions. Cells were seeded into T-175 flasks and cultured in high-glucose Dulbecco’s Modified Eagle Medium (Corning, Glendale, AR; 10–017-CV) containing 10% FBS (fetal bovine serum), 1% Glutagro (Gibco, Thermo Fisher Scientific, Waltham MA) and 1% Anti–Anti (Corning, Corning NY) until they reached a confluency of 90%. Cell numbers were obtained using the Eve Automated Cell Counter (NanoEntek; Waltham, MA) at the time of passage and during expansion. The target cell seeding density of 2000 cells/cm2 into T175 flasks.
Viability Measurements
Cells were suspended in HA and viability tested when held at 37°C or room temperature (24°C) for 48 hours. Cells were suspended in HA by first mixing the cells in media with a commercially available HA paste, Monovisc (Anika Therapeutics, Inc., Bedford, MA) in a 1:1 volume ratio using vigorous pipetting due to the viscous nature of the HA. The control MSCs in standard culture media were diluted to the same concentration and vigorously pipetted so that the total cell numbers/sample and cell handling were approximately the same. Aliquots of cells (100 μL) were placed in 96-well plates and stored in the different temperature conditions. The 37°C group was cultured in a standard incubator with 5% CO2. The 24°C group was cultured on the bench with temperatures fluctuating between 23.3°C and 24.8°C for the course of this study.
A 1:1 solution of calcein AM (Life Technologies, Carlsbad, CA) and ethidium bromide (Thermo Fisher; Waltham, MA) were mixed in cell culture media. About 10 μL of the calcein/ethidium bromide solution was added to each well and incubated 30 minutes at the prescribed storage condition prior to the initiation of imaging. For the first time point (30 minutes) the calcein/ethidium bromide was added at the time of plating in the 96-well plates. Images were collected on a Biotek Cytation 5 Multi-Mode Reader (Agilent, Santa Clara, CA). A set of 3 images were collected for each region of interest including a brightfield image, ethidium bromide fluorescence emission captured at 603 nm and a calcein emission image captured at 501nm. The data presented represent the average of 3 independent trials (3 replicates/trial).
The percentage of live cells calculated from the images was obtained using the following equation:

Gene Expression
MSCs cultured in standard conditions or were suspended in HA as described above and maintained in an incubator at 37°C for 7 days. In order to conduct gene expression tests, the cells were isolated from the HA suspension by exposure to 10,000 units/mL of hyaluronidase (Sigma Aldrich, St. Louis MO) (pH 6.0) for 1 hour, followed by multiple rinses in media. Control cells were exposed to the same concentration of hyaluronidase. Subsequently, TrypLE (Thermo Fischer Scientific) was applied to flasks to release adhered cells. MSCs blended in HA and controls were spun down and resuspended in 3.0 mL DPBS to perform cell counts. Cells were lysed using 600 uL TRI-Reagent (Zymo Research, Irvine, CA).
Total RNA was extracted using a Direct-zol RNA Miniprep Kit (Zymo Research, Irvine, CA, USA) following the manufacturer’s protocol. A primary DNase treatment was completed at room temperature. RNA was quantified using a NanoDrop 1000 Spectrophotometer (Thermo-Fisher, Waltham, MA) at 260 nm and 280 nm and was used immediately or aliquoted and stored at −20°C. Equivalent amounts of RNA obtained from the control MSCs and HA suspended MSCs were used for qRT-PCR using AgPath-ID One-Step RT-PCR Kit (Applied Biosystems by Thermo Fisher Scientific, Carlsbad, CA) following the manufacturer’s instructions carried out on the Bio-Rad CFX96 Real-Time PCR Detection System (Bio-Rad, Hercules, CA). The biomarkers used to identify MSCs as well as biomarkers that identify chondrogenic and osteogenic differentiation are listed in Table 1. CT results with values that averaged over 35 were defined as not detected. A total of 3 independent trials were conducted on both groups. The amount of target amplified in the samples was normalized to GUSB (glucuronidase beta), a housekeeping gene, and reported as delta CT (dCT).
 |
Table 1 Animal Groups |
Established Rat Knee OA Model
To determine whether the MSC-HA suspension enhanced the ability of the MSCs to reverse articular cartilage degradation, a well-established model of rat OA was utilized.14,42 All animal studies were carried out under the approved IACUC protocol (2019–2527) at the University of Kansas Medical Center and were performed in compliance with policies on animal use and ethics in accordance with the US Animal Welfare Act. The university animal facility is registered with the United States Department of Agriculture and the NIH’s Office of Laboratory Welfare. The knee joints of Sprague-Dawley rats (total of 31 animals, 8–10 weeks age) were randomized into 4 groups. Briefly, the knee joints were exposed through a medial parapatellar incision, and the joint capsule was incised. The medial meniscotibial ligament was transected resulting in destabilization of the medial meniscus. The cruciate ligaments and other ligaments around the knee joint were preserved to maintain normal mobility of the animal after surgery. Four weeks following the meniscus surgical procedure, the joints were randomized into the groups shown in Table 2. Three additional rats were maintained without the destabilization surgery as a comparison of healthy joints. Each treatment dose consisted of a volume of 100 µL, and treatments with cells contained approximately 2 × 106 MSCs.
 |
Table 2 Indicators of MSC Identity Biomarkers |
Pain Assessment
Pain examinations were administered prior to the destabilization surgery, prior to the IA injections of the treatments described above and weekly thereafter. Pain assessments employed the standardized squeeze test to measure vocalizations produced by animals.14,43 Briefly, animal subjects were held in a knee extension position until they displayed a stable temperament, subsequently physical pressure was applied to the joint. Recorded vocalizations were collected for 5 periods of extensions. Once vocalizations were recorded upon pressure being applied to knee joint, the joint was returned to the natural position.
Histopathological Examination
At 6 weeks post treatment, the study was terminated and joints collected for processing for histological analysis. Whole joints were removed for histological staining of the medial and lateral femoral condyles and the tibial plateaus (conducted by Atlantic Bone Screen). Joints were fixed in 10% neutral buffered formalin for up to 3 weeks and then stored in decalcification buffer for 2 weeks. Sections were embedded in paraffin blocks followed by sectioning into 4 mm sections. To identify cartilage, sections were stained with Safranin-O and Fast Green. Safranin-O stains proteoglycans indicative of cartilage. For immunofluorescence, sections were stained with DAPI nuclear stain (Thermo Fisher Scientific) and with antibodies for collagen II, ADAMTS5 and MMP-13 (all purchased from Abcam, Cambridge, UK). Standard blocking, secondary antibody incubation, and rinsing procedures followed the manufacturers’ instructions.
As cartilage degradation is a hallmark symptom of knee OA, visible assessments of cartilage degradation were determined according to guidelines of the Osteoarthritis Research Society International (OARSI) Histopathological Scoring System.44 The OARSI Histopathology Scoring System scores the degree of cartilage degradation present among whole knee joint sections along with the integrity of the joint by scoring the degree of clefts and fibrillations.14,45,46 All histopathological sections were scored by 2 independent technicians and the values averaged. The higher the number, the greater the damage to the joint.
Statistical Analysis
All data are reported as the average with the standard error of the mean. One-Way Analysis of Variance (ANOVA) was used to determine the statistical significance between groups of the OARSI scores. Student’s T-tests were used to compare the gene expression (dCT) between the control and HA-suspended cells. Repeated measures ANOVA was used for the viability and pain scores. When normality failed, ANOVA on Ranks was performed. Statistical differences were defined as p < 0.05.
Results
Cell Viability in HA
Symptomatic relief of knee OA has been correlated with higher cell viability at transplantation.47 It was therefore essential to know the average viability of cells in HA prior to injecting into the knee. Since the majority of MSC therapies to treat OA are autologous procedures conducted in local clinics, different storage conditions were tested to mimic the conditions that might be used in clinics including room temperature (24°C) and incubated at 37°C with 5% CO2.
The MSCs maintained in standard 37°C conditions without HA had the highest viability through the 48 hour periods, ranging between 90–100% viability (Figure 1A). At 24°C storage, the highest percentage of dead cells was recorded when cultured in HA. The viability images revealed less cell death without HA. However, at 37°C, the amount of cell death was minimal even in HA, with nearly 90% viability at 48 hours (Figure 1B). Thus, the viability of the cells in HA maintained in an incubator was sufficient to use in animal studies.
 |
Figure 1 Live/Dead Staining of HA-Entrapped MSCs. (A) Cells were cultured in standard conditions (37°C and 5%CO2) or at room temperature (24°C) in either standard cell culture media or suspended in a media-HA paste (MSCs-HA). The viability of the cells in standard culture media was higher than cells in HA, especially when held at room temperature (p < 0.05 at 48 hours). (B) The images provide examples of the dead cells (red) in each condition at the first time point at 48 hours. Scale bar = 500 μm. (C) Changes in cell morphology were observed under brightfield microscopy of MSCs alone and MSC-HA suspension over time. At the final reading of 48 hours, cells suspended in HA displayed greater amounts of cell clustering than MSCs alone when stored at 4°C and 24°C. When cultured in an incubator at 37°C, both groups had similar cell morphology. Scale bar = 1000 μm. |
HA and Cell Morphology
As illustrated in Figure 1C, not only did the cell viability change over time but so did the cell morphology. Changes in cell morphology can be observed from brightfield microscopy of MSCs alone and MSC-HA suspensions over time. Cells suspended in HA demonstrated a higher propensity to cluster, while cells in standard culture remained predominantly single cell morphology. The clustering was especially apparent in the room temperature group (24°C) at 48 hours. When cultured in an incubator at 37°C, there was less clustering, especially of the MSC-HA group.
Effects of HA on MSC Gene Expression
Cells were cultured for 1 week in standard conditions (37°C and 5% CO2) with or without HA. The gel electrophoresis of the amplified DNA shows clear bands at the anticipated size, demonstrating the efficiency of the extraction method (Figure 2A). The biomarkers used to identify MSCs showed positive amplification of CD29, CD44, and CD90 as shown by the dCT (normalized to GUSB) values in Table 3 with MSCs in HA expressing higher levels of the markers. CD34 or CD45 should not be detected in MSCs, which was the case for both groups (not detected = ND). Probes that averaged a Ct value of 35 or greater were defined as not detected. Biomarkers of chondrogenic differentiation were either similar between groups (ACAN) or higher with HA (SOX9). While a third biomarker of chondrogenesis, collagen II (COL2A1) was not detected in either group. Biomarkers of osteogenic differentiation (RUNX2 and ALPL) were poorly expressed in the control MSCs and not detected in the HA suspended MSCs. Figure 3B provides a direct comparison of the differences between the 2 groups, by graphing the fold difference of the cells in HA compared to controls. Markers that were not detected in a group were not included in the comparison.
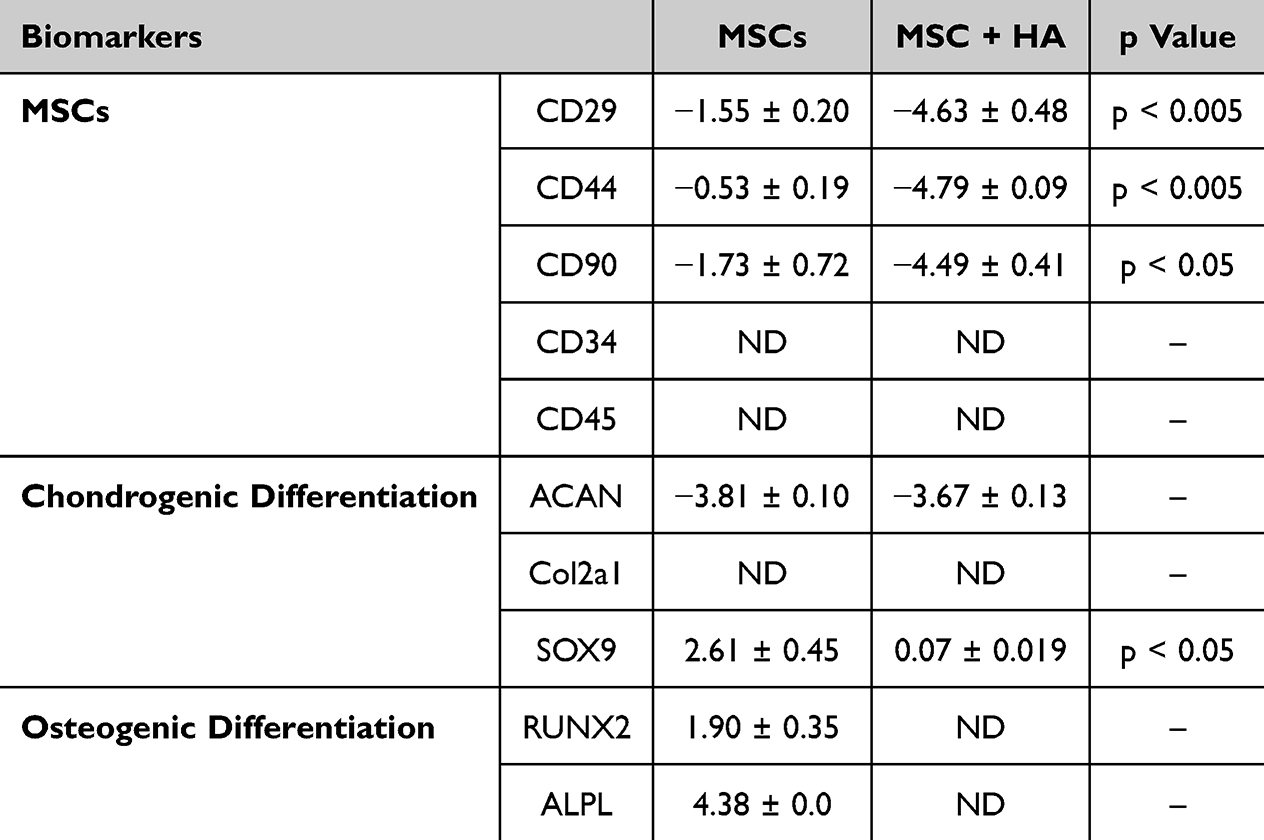 |
Table 3 Monovisc dCt Values |
 |
Figure 2 Gene Expression Profile of MSCs in HA. (A) The gel electrophoresis of the amplified probes shows clear bands of the anticipated size, demonstrating the efficiency of the extraction method. CD34 and CD45 are negative markers for MSCs. (B) The fold change in the dCT levels after 7 days of suspension in HA are shown. The panel of biomarkers used to identify MSCs showed clear positive amplification of CD29, CD44, and CD90. Biomarkers of chondrogenic differentiation were either the same between groups (ACAN) or higher with HA (SOX9). Probes that averaged a Ct value of 35 or greater were defined as not detected and not included in analysis. |
 |
Figure 3 Pain Scores of Rats with Knee OA. OA was induced in rat knees by destabilizing the medial meniscus. Prior to the destabilization procedure, each animal was tested for pain in the knees using a standard rodent pain assessment, providing a baseline measurement of non-painful joints. After the knee destabilization but before injection of the treatments (Pre-Tx) the pain levels went up in all 4 groups. A week after the intra-articular injections of the treatments, only animals receiving HA alone had a transient reduction in pain for 2 weeks. By week 3, there were no differences between scores for the 4 groups. |
Effects of Treatment on Knee Pain
Once the conditions for viability above 80% for cells in HA were determined along with a favorable gene expression profile in HA (decrease in osteogenic biomarker expression), in vivo studies were undertaken. Rats underwent a standard procedure to destabilize the medial meniscus resulting in overt OA.14,42 Later, the joints were randomly divided into control (vehicle treated), HA only, MSCs only, and MSCs suspended in HA (MSC-HA). Joint pain measurements were captured prior to the destabilization procedure (baseline), prior to the treatment (pre-Tx), and weekly after the cell therapy treatments. The pre-injury pain values were not statistically different and averaged between 0–0.5, which indicated no pain (Figure 3). After the OA-inducing injury, there was a significant increase in the pain values for all 4 groups. Knee pain scores revealed that treatment with HA alone was associated with a transient reduction in pain for weeks 2 and 3. In contrast, the other 3 groups had no significant reduction in pain for weeks 1–6 after treatment. In general, the control group receiving vehicle alone had the highest pain scores across the study duration.
Progression of OA
Six weeks after the injection of the 4 treatment groups, the animals were euthanized, and the joints collected for histological assessment. The brightfield images illustrate the uneven surface of the bones from the injury model (Figure 4). As a comparison, an image from an age-matched healthy knee that did not undergo the medial meniscus destabilization procedure is provided. Collagen II synthesis in joints has been shown to increase in early stages of OA, but in later stages is found in subchondral bone. In joints from healthy (uninjured) and MSC-HA animals, there was a low level of background staining noted for collagen II (Figure 4). However, there was little detectable levels of collagen II in the 4 experimental groups. Staining for the metalloproteinase, ADAMTS5, illustrated a low level of punctate staining in joints from all groups with no obvious differences in the pattern or intensity. ADAMTS5 is known to be secreted early in the OA process. MMP-13, also known as collagenase 3, is a key enzyme in the breakdown of type II collagen.48 Punctate MMP-13 staining was noted in each of the groups. Together the irregular bone surface with clefts and the lack of collagen II staining on the surface, especially in the vehicle control group, indicate that the animal model represented advanced OA.
 |
Figure 4 Immunohistochemistry of Rat Knee Joints. Knee joints were stained for markers of early and advanced OA. The knees of healthy (non-injury model) animals were included as a comparison. The brightfield images illustrated the abnormal surface of the joints with crevices and fibrillations in the knees of the OA rats regardless of the treatment group. Collagen II was clearly identified in the healthy animal but not in other groups. Staining for the metalloproteinase, ADAMTS5, illustrated a low level of punctate staining in joints from all groups. MMP-13 staining was similar across groups. The scale bar = 1mm. |
Effects of Treatment on Joint Integrity
Joint sections were stained with Fast Green and Safranin O to visualize the bone area (green) and proteoglycans (red), indicative of cartilage. Pathological signs of knee OA typically consist of decreased concentrations of proteoglycans.49 Figure 5 provides typical examples of the joint sections for each group. Again, an image of a healthy knee that did not undergo the meniscus instability procedure is included for comparison. The red staining in the healthy joint indicates significant amounts of cartilage at the joint surface with a smooth bony facade. After destabilization of the meniscus, severe changes were seen in the joints with a lack of cartilage and a rough surface (Figure 5, vehicle). In addition, there was excessive subchondral bone noted at the surface. When HA alone was injected into the joints, there were minor improvements in the joint integrity with minimal cartilage staining, but still the joints exhibited a rough surface with clefts and excessive subchondral bone. With MSC treatment, there was some improvement with more cartilage and a smoother bony surface. However, when the MSCs were delivered to the knee in HA (MSC-HA), the improvement noted with the MSCs alone was absent. Again, there was a lack of cartilage, excessive subchondral bone and an irregular surface.
 |
Figure 5 Blinded Scoring of Knee Joint Integrity. Joint sections were stained with Fast Green and Safranin O (red) to visualize the bone morphology and proteoglycan level (red), indicative of cartilage. An image of a healthy knee shows red staining (proteoglycan) along the surface of the bone. However, animals that underwent OA induction and received the different treatments all showed lower levels of proteoglycans and a rougher bony surface. Multiple images from each animal were scored by blinded scientists using the OARSI Histopathology Scoring System. Lower scores indicate better joint integrity. The results showed no statistical difference between the treatment groups. |
The OARSI’s Histopathological Scoring System was utilized as a semi-quantitative measurement to assess patterns of fibrillations and clefts in the bony surface and quantify the amounts of proteoglycans denoted in cartilage.44 Two research associates independently reviewed the lateral and femoral condyles and tibial plateaus, scoring multiple sections per joint and the values for each section were summed with a greater value indicating worse joint damage. While there were no statistically significant differences between the groups, the OARSI Histopathology scores were the lowest for the joints that received MSCs alone and the vehicle groups (Figure 5).
Discussion
Autologous MSCs are being utilized as therapeutic agents for addressing tissue regeneration for knee OA. Challenges in clinical applications involve poor MSC viability after isolation, shear stress during injections, poor retention time in the knee joint after weight bearing and maintenance of cell health in the inflammatory environment of knee OA.50 As HA is a synovial joint polymer that maintains cartilage viscoelastic integrity, HA-based intra-articular injections that deliver MSCs into the joint cavity are a possibility for improving the symptoms of knee OA. The purpose of this study was to determine whether MSCs carried in a commercially available lightly crosslinked HA (Monovisc) could ameliorate the OA-associated changes in joint integrity in an animal model.
HA gels can be characterized by their molecular weight with low molecular weight (mw) of less than 1 MDa, shown to activate pro-inflammatory responses,51 and is rapidly cleared from the joint with a half-life of only a few hours.52 In contrast, high mw (>1 MDa) HA may last in the joint for up to 9 days. For even longer retention times, fully crosslinked HA microbeads have been shown to reside in the joint for up to 6 weeks.14 In this study, a high mw HA was chosen with a reported molecular weight of 2.5 MDa53,54 and 2.2% crosslinking,55 which would theoretically provide an increased retention time for the cells in the joint. At 22 mg/mL packaging, Monovisc is also one of the most concentrated and viscous commercial forms of HA,54 which could partially explain the slightly higher cell death noted in the in vitro studies described here. In fact, previous publications have shown that exposure of MSCs to other commercially available HA gels like Synvisc® and Orthovisc®, also led to significant cell death.56
It is important to know whether the exposure to HA changes the MSC phenotype. In this study, we examined the effect of maintaining cells in an HA suspension for 1 week on the gene expression profile for select biomarkers for MSCs, chondrogenesis and osteogenesis. The genetic profile of MSCs is characterized by positive expression of CD29 and CD44.57–60 These receptor molecules are also able to bind hyaluronic acid and other extracellular ligands that are involved in regulating cellular migration and invasion.58 Given the role of these factors in cell adhesion to the extracellular matrix, including HA, it was not surprising that there was greater expression of CD29 and CD44 in the HA suspension group compared to MSCs grown in cell culture. CD90, another MSC biomarker,61 was also more highly expressed in the HA suspension group. The absence of CD34 and CD45 was expected as they are negative identity markers for MSCs and they were absent in both of the groups studied here. This study focused on the role of HA to retain the cells in the joint for longer periods of time. However, there may also be synergistic effects of HA on MSCs. HA has been shown to promote MSC differentiation and the increased expression of the MSC biomarkers CD29, CD44 and CD90 in cells cultured in HA. Yet, given the positive in vitro effect, there was no translation to the animal model.
Aggrecan (ACAN) and SOX9 are transcription factors that regulate chondrogenesis, specifically aiding MSC in the early stages of differentiation.62–65 In this study, there was no difference in the amount of ACAN expression in the control and MSC-HA groups. There was very little expression of SOX 9 over the housekeeping gene. Collagen type II is an extracellular signaling molecule, associated with MSCs, that partners with other molecules, like aggrecan, to form cartilage like tissues.66 No collagen II was detected in either group of MSCs. Thus, there did not appear to be a strong tendency towards chondrogenic differentiation in cells cultured with HA.
Osteogenic differentiation should be avoided with a cell therapy treatment for joints. Runt-related transcription factor 2 (RUNX2) enables MSCs to differentiate into osteoblasts,67 regulating genes that promote the development of osteoblasts and osteogenic biomarker genes, such as alkaline phosphatase (ALPL).68 Both RUNX2 and ALPL were poorly expressed in the control MSC and were not detected in the MSC-HA suspensions.
More important than the in vitro changes associated with culturing MSC in lightly crosslinked HA was the changes noted in a rodent model of OA. All the groups showed the same pain level as the first week after injury. It is critical to note that the HA alone and the MSCs-HA groups each failed to reduce pain scores from weeks 1–6 after the treatments. Pain scores using the pinch test are known to have large variance in values. This may be due to the test itself, but also to the variations in the surgical techniques of destabilizing the medial menisci of rat subjects.69,70 In order to minimize the variance as much as possible, the same surgeon conducted all of the destabilizing procedures and the same technician administered all of the pain assessment tests.
At 6 weeks during the post-injection time frame, joints were collected for histological evaluations, which showed an uneven bony surface with clefts and fibrillations in all the groups except the healthy (non-injured) animals. Based on the gold standard, OARSI Histopathological Scoring System, there were no statistical differences in the histopathology scores for any of the treatment groups. The results conclude that Monovisc, when blended with MSCs, was unable to aid in tissue regeneration.
This is in stark contrast to other publications that have shown improvement in joint integrity with a combination of HA and MSCs.39,71,72 However, in many of the previous publications, the comparison group was HA alone or there were no controls.73 Thus, in those studies, there was no direct comparison between MSCs alone and MSCs in HA. A meta-analysis reviewing 79 randomized controlled studies with over 8500 patients summarized the comparison of intra-articular injections of MSCs, HA, corticosteroids, platelet-rich plasma and a number of other treatments. In all of those studies, there were no randomized trials of MSCs delivered in HA.74 Our previous publication using the same animal model demonstrated the positive impact of MSCs with HA, however the HA polymer in that study was designed specifically as a cell carrier.14 In encapsulating cells in fully crosslinked HA microbeads designed with rheological properties that match those of synovial fluid, the MSCs thrived with high viability over 7 days in culture. When injected into OA rat knees, there were statistically lower OARSI scores in the encapsulated MSC group when compared to cells alone, HA alone or the sham controls.
Conclusion
While some HA formulations may offer benefits in administering MSCs to treat knee degeneration, a high molecular weight, commercially available HA paste failed to improve the viability of the cells in vitro or the knee integrity in a rat knee degenerative model.
Abbreviations
ACAN, Aggrecan; ADAMTS5, A Disintegrin and Metalloproteinase with Thrombospondin Motifs5; ALPL, Alkaline Phosphatase; ANOVA, Analysis of Variance; CD29, Integrin Beta-1; CD34, Cluster of Differentiation 34; CD44, Cluster of Differentiation 44; CD45, Protein Tyrosine Phosphatase, Receptor Type C; CD90, Thy-1; COL2A1, Collagen type IIA; CT, Cycle Threshold; dCT, Delta Cycle Threshold; DNA, Deoxyribonucleic Acid; FBS, Fetal Bovine Serum; GUSB, Glucuronidase beta; HA, Hyaluronic Acid; IA, Intra-articular; IACUC, Institutional Animal Care and Use Committee; MMP-13, Collagenase 3; MSC, Multipotent Stem Cells; MSC-HA, Multipotent Stromal Cells in Hyaluronic Acid; ND, Not Detected; OA, Osteoarthritis; OARSI, Osteoarthritis Research Society International; PCR, Polymerase Chain Reaction; RNA, Ribonucleic Acid; RUNX2, Runt-related transcription factor 2; RT-PCR, Reverse Transcription Polymer Chain Reaction; SOX9, Transcription Factor SOX9.
Acknowledgments
The authors would like to thank the Kansas City Consortium on Musculoskeletal Diseases (KCCMD) for funding the project (grant awarded to DCB). We are indebted to Dr. Jinxi Wang and the staff of the Harrington Research Laboratory at the University of Kansas Medical Center for assistance with the DMM model and IA knee injections. We thank the Atlantic Bone Screen for their work on histological processing of the joint sections.
Author Contributions
All authors made a significant contribution to the work reported, whether that was in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Funding was provided by the Kansas City Consortium on Musculoskeletal Diseases (KCCMD).
Disclosure
MH, DM, AW, SH and LSB are employees of Likarda, Inc, which gains no benefit from the results of this study. LSB is also the founder and has equity in Likarda, Inc. The authors report no other conflicts of interest in this work.
References
1. Cui A, Li H, Wang D, Zhong J, Chen Y, Lu H. Global, regional prevalence, incidence and risk factors of knee osteoarthritis in population-based studies. EClin Med. 2020;2020:29–30.
2. Arslan I, Damen J, deWilde M, et al. Incidence and prevalence of knee osteoarthritis using codified and narrative data from electronic health records: a population-based study. Arthritis Care Res. 2022;74(6):937–944. doi:10.1002/acr.24861
3. Verges J, Vitaloni M, Bibas M, et al. Global management of patients with knee osteoarthritis begins with quality of life assessment: a systematic review. BMC Musculoskelet Disord. 2019;20(1):493. doi:10.1186/s12891-019-2895-3
4. Kawano M, Araujo I, Castro M, Matos M. Assessment of quality of life in patients with knee osteoarthritis. Acta Ortop Bras. 2015;23(6):307–310. doi:10.1590/1413-785220152306150596
5. Fuggle N, Cooper C, Oreffo R, et al. Alternative and complementary therapies in osteoarthritis and cartilage repair. Aging Clin Exp Res. 2020;32(4):547–560. doi:10.1007/s40520-020-01515-1
6. Karanu F, Ott L, Webster D, Stehno-Bittel L. Improved harmonization of critical characterization assays across cell therapies. Reg Med. 2020;15(5):1661–1678. doi:10.2217/rme-2020-0003
7. Wei C, Lin A, Hung S-C. Mesenchymal stem cells in regenerative medicine for musculoskeletal diseases: bench, bedside, and industry. Cell Transplant. 2014;23(4–5):505–512. doi:10.3727/096368914X678328
8. Hofer H, Tuan R. Secreted trophic factors of mesenchymal stem cells support neurovascular and musculoskeletal therapies. Stem Cell Res Ther. 2016;7(1):131. doi:10.1186/s13287-016-0394-0
9. Pizza N, Ng M, Chughtai M, et al. The stem cell market for the treatment of knee osteoarthritis: a patient perspective. J Knee Surg. 2018;31(6):551–556. doi:10.1055/s-0037-1604443
10. Zhu C, Wu W, Qu X. Mesenchymal stem cells in osteoarthritis therapy: a review. Am J Transl Res. 2021;13(2):448–461.
11. Lv Z, Cai X, Bian Y, et al. Advances in mesenchymal stem cell therapy for osteoarthritis: from preclinical and clinical perspectives. Bioengineering. 2023;10(2):195. doi:10.3390/bioengineering10020195
12. Black L, Gaynor J, Gahring D, et al. Effect of adipose-derived mesenchymal stem and regenerative cells on lameness of dogs with chronic osteoarthritis of the coxofemoral joints: a randomized, double blinded, multicenter, controlled trial. Vet Ther. 2007;8:272.
13. He L, He T, Xing J, et al. Bone marrow mesenchymal stem cell-derived exosomes protect cartilage damage and relieve knee osteoarthritis pain in a rat model of osteoarthritis. Stem Cell Res Ther. 2020;11:276. doi:10.1186/s13287-020-01781-w
14. Hamilton M, Wang J, Dhar P, Stehno-Bittel L. Controlled-release hydrogel microspheres to deliver multipotent stem cells for treatment of knee osteoarthritis. Bioengineering. 2023;10(11):1315. doi:10.3390/bioengineering10111315
15. Hunakova K, Kluchy M, Spakova T, et al. Study of bilateral elbow joint osteoarthritis treatment using conditioned medium from allogeneic adipose tissue-derived MSC in Labrador retrievers. Res Vet Sci. 2020;132:513–520. doi:10.1016/j.rvsc.2020.08.004
16. Xing D, Wang K, Wu J, et al. Clinical-grade human embryonic stem cell-derived mesenchymal stem cells ameliorate the progression of osteoarthritis in a rat model. Molecules. 2021;26:604. doi:10.3390/molecules26030604
17. Partan R, Putra K, Kusuma N, et al. Umbilical cord mesenchymal stem cell secretome improves clinical outcomes and changes biomarkers in knee osteoarthritis. J Clin Med. 2023;12(22):7138. doi:10.3390/jcm12227138
18. Lee W, Kim H, Kim K, Kim G, Jin W. Intra-articular injection of autologous adipose tissue-derived mesenchymal stem cells for the treatment of knee osteoarthritis: a Phase Iib randomized, placebo-controlled clinical trial. Stem Cells Transl Med. 2019;8:504–511. doi:10.1002/sctm.18-0122
19. Gupta P, Chulikana A, Rengasamy M, et al. Efficacy and safety of adult human bone marrow-derived, cultured, pooled allogeneic mesenchymal stromal cells (Stempeucel): preclinical and clinical trial in osteoarthritis of the knee joint. Arthritis Res Ther. 2016;18:301. doi:10.1186/s13075-016-1195-7
20. Garay-Mendoza D, Villarreal-Martinez L, Garza-Bedolla A, et al. The effect of intra-articular injection of autologous bone marrow stem cells on pain and knee function in patients with osteoarthritis. INt J Rheum Dis. 2018;21(1):140–147. doi:10.1111/1756-185X.13139
21. Freitag J, Wickman J, Shah K, Tenen A. Real-world evidence of mesenchymal stem cell therapy in knee osteoarthritis: a large prospective two-year case series. Reg Med. 2022;17(6):355–373. doi:10.2217/rme-2022-0002
22. Jung S-H, Nam B-J, Choi C-H, et al. Allogeneic umbilical cord blood-derived mesenchymal stem cell implantation versus micro drilling combined with high tibial osteotomy for cartilage regeneration. Sci Rep. 2024;14(1):3333. doi:10.1038/s41598-024-53598-9
23. Sadeghirad B, Rehman Y, Khosravirad A, et al. Mesenchymal stem cells for chronic pain secondary to osteoarthritis: a systematic review and meta-analysis of randomized trials. Osteoarth Cart. 2024;2024:1.
24. Liu C, Yang Y, He G. Efficacy and safety of umbilical cord-mesenchymal stem cell transplantation for treating osteoarthritis. Osteoarth Cart. 2017;25:S389.
25. Law L, Hunt C, van Wijnen A, et al. Office-based mesenchymal stem cell therapy for the treatment of musculoskeletal disease: a systematic review of recent human studies. Pain Med. 2019;20(8):1570–1583. doi:10.1093/pm/pny256
26. Fan M, Tong P, Yan L, et al. Detrimental alteration of mesenchymal stem cells by an articular inflammatory microenvironment results in deterioration of osteoarthritis. BMC Med. 2023;21(1):215. doi:10.1186/s12916-023-02923-6
27. Toupet K, Maumus M, Luz-Crawford P, et al. Survival and biodistribution of xenogenic adipose mesenchymal stem cells is not affected by the degree of inflammation in arthritis. PLoS One. 2015;10:e0114962.
28. Ozeki N, Muneta T, Koga H, et al. Not single but periodic injections of synovial mesenchymal stem cells maintain viable cells in knees and inhibit osteoarthritis progression in rats. Osteoarthritis Cartilage. 2016;24(6):1061–1070. doi:10.1016/j.joca.2015.12.018
29. Wang A-T, Feng Y, Jia -H-H, Zhao M, Yu H. Application of mesenchymal stem cell therapy for the treatment of osteoarthritis of the knee: a concise review. World J Stem Cells. 2019;11(4):222–235. doi:10.4252/wjsc.v11.i4.222
30. ter Huurne M, Schelbergen R, Blattes R, et al. Antiinflammaotry and chondroprotective effects of intraarticular injection of adipose-derived stem cells in experimental osteoarthritis. Arthritis Rheum. 2012;64(11):3604–3613. doi:10.1002/art.34626
31. Horie M, Choi H, Lee R, et al. Intra-articular injection of human mesenchymal stem cells (MSCs) promote rat meniscal regeneration by being activated to express Indian hedgehog that enhances expression of type II collagen. Osteoarth Cart. 2012;20(10):1197–1207. doi:10.1016/j.joca.2012.06.002
32. Toupet K, Maumus M, Peyrafitte J-A, et al. Long-term detection of human adipose-derived mesenchymal stem cells after intraarticular injection in SCID mice. Arth Rheum. 2013;65:1786–1794. doi:10.1002/art.37960
33. Lamo-Espinosa J, Mora G, Blanco J, et al. Intra-articular injection of two different doses of autologous bone marrow mesenchymal stem cells versus hyaluronic acid in the treatment of knee osteoarthritis: multicenter randomized controlled clinical trial (phase I/II). J Transl Med. 2016;14(1):246. doi:10.1186/s12967-016-0998-2
34. Matas J, Orrego M, Amenabar D, et al. Umbilical cord-derived mesenchymal stromal cells (MSCs) for knee osteoarthritis: repeated MSC dosing is superior to a single MSC dose and to hyaluronic acid in a controlled randomized phase I/II trial. Stem Cells Transl Med. 2019;8(3):215–224. doi:10.1002/sctm.18-0053
35. Lukomska B, Stanaszek L, Zuba-Surma E, Legosz P, Sarzynska S, Drela K. Challenges and controversies in human mesenchymal stem cell therapy. Stem Cells Inter. 2019;2019:9628536. doi:10.1155/2019/9628536
36. Solis M, Chen Y-H, Wong T, Bittencourt V, Lin Y-C, Huang LLH. Hyaluronan regulates cell behavior: a potential niche matrix for stem cells. Biochem Res Int. 2012;2012:346972. doi:10.1155/2012/346972
37. Lopez-Ruiz E, Jimenez G, de Cienfuegos L, et al. Advances of hyaluronic acid in stem cell therapy and tissue engineering, including current clinical trials. Euro Cell Mat. 2019;37:186–213. doi:10.22203/eCM.v037a12
38. Bowman S, Awad M, Hamrick M, Hunter M, Fulzele S. Recent advances in hyaluronic acid based therapy for osteoarthritis. Clin Transl Med. 2018;7:6. doi:10.1186/s40169-017-0180-3
39. Li L, Duan X, Fan Z, Chen L, Xing F, Xu Z. Mesenchymal stem cells in combination with hyaluronic acid for articular cartilage defects. Sci Rep. 2018;8:9900.
40. Matas J, Garcia C, Pollute D, et al. A Phase I dose-escalation clinical trial to assess the safety and efficacy of umbilical cord-derived mesenchymal stromal cells in knee osteoarthritis. Stem Cells Transl Med. 2024;13(3):193–203. doi:10.1093/stcltm/szad088
41. Park Y-B, Ha C-W, Lee C-H, Yoon Y, Park Y-G. Cartilage regeneration in osteoarthritic patients by a composite of allogeneic umbilical cord blood-derived mesenchymal stem cells and hyaluronate hydrogel: results from a clinical trial for safety and proof-of-concept with 7 years of extended follow-up. Cells Trans Med. 2017;6:613–621. doi:10.5966/sctm.2016-0157
42. Iijima H, Aoyama T, Ito A, et al. Destabilization of the medial meniscus leads to subchondral bone defects and site-specific cartilage degeneration in an experimental rat model. Osteoarthr Cartil. 2014;22(7):1036–1043. doi:10.1016/j.joca.2014.05.009
43. Piel M, Kroin J, van Wijnen A, Kc R, Im H-J. Pain assessment in animal models of osteoarthritis. Gene. 2014;537:184–188. doi:10.1016/j.gene.2013.11.091
44. Glasson S, Chambers M, van den Berg W, L CB. The OARSI histopathology initiative - recommendations for histological assessments of osteoarthritis in the mouse. Osteoarth Cart. 2010;18:517–523. doi:10.1016/j.joca.2010.05.025
45. Schneider T, Welker P, Licha K, Haag R, Schulze-Tanzil G. Influence of dendritic polyglycerol sulfates on knee osteoarthritis: an experimental study in the rat osteoarthritis model. BMC Musculoskelet Disord. 2015;15:387. doi:10.1186/s12891-015-0844-3
46. Corciulo C, Lendhey M, Wilder T, et al. Endogenous adenosine maintains cartilage homeostasis and exogenous adenosine inhibits osteoarthritis progression. Nat Comm. 2017;8:15019. doi:10.1038/ncomms15019
47. Lepperdinger G. Inflammation and mesenchymal stem cell aging. Curr Opin Immunol. 2011;23:518–524. doi:10.1016/j.coi.2011.05.007
48. Hu Q, Ecker M. Overview of MMP-13 as a promising target for the treatment of osteoarthritis. Int J Mol Sci. 2021;22(4):1742. doi:10.3390/ijms22041742
49. Mobasheri A, Kalamegam G, Musumeci G, Batt M. Chondrocyte and mesenchymal stem cell-based therapies for cartilage repair in osteoarthritis and related orthopaedic conditions. Maturitas. 2014;78:188–198. doi:10.1016/j.maturitas.2014.04.017
50. Song Y, Zhang J, Xu H, et al. Mesenchymal stem cells in knee osteoarthritis treatment: a systematic review and meta-analysis. J Ortho Transl. 2020;24:121–130.
51. Rayahin J, Buhrman J, Zhang Y, Koh T, Gemeinhart R. High and low molecular weight hyaluronic acid differentially influence macrophage activation. ACS Biomater Sci Eng. 2016;1(7):481–493. doi:10.1021/acsbiomaterials.5b00181
52. Larsen N, Dursema H, Pollak C, Skrabut E. Clearance kinetics of hylan-based viscosupplement after intra-articular and intravenous administration in animal models. J Biomed Mater Res B Appl Biomater. 2012;100(2):457–462. doi:10.1002/jbm.b.31971
53. 0702 M. Pivotal Clinical Trial. FDA monovisc summary of safety and effectiveness. 2014.
54. Dernek B, Duymus T, Köseoğlu P, et al. Efficacy of single-dose hyaluronic acid products with two different structure in patients with early-stage knee osteoarthritis. J Rhys There Sci. 2016;28(11):3036–3040. doi:10.1589/jpts.28.3036
55. Testa G, Giardina S, Culmone A, et al. Intra-articular injections in knee osteoarthritis: a review of literature. J Funct Morph Kinesiology. 2021;6(1):15. doi:10.3390/jfmk6010015
56. Kaleka C, Zucconi E, Da Silva Vieria T, S M, Ferretti M, Cohen M. Evaluation of different commercial hyaluronic acids as a vehicle for injection of human adipose-derived mesenchymal stem cells. Rev Bras Ortop. 2018;53(5):557–563. doi:10.1016/j.rbo.2017.05.008
57. Togarrati P, Dinglasan N, Desai S, Ryan W, Muench M. CD29 is highly expressed on epithelial, myoepithelial and mesenchymal stromal cells of human salivary glands. Oral Dis. 2018;24(4):561–572. doi:10.1111/odi.12812
58. Isono M, Takeuchi J, Maehara A, et al. Effect of CD44 signal axis in the gain of mesenchymal stem cells surface antigens from synovial fibroblasts in vitro. Heliyon. 2022;8(10):e10739. doi:10.1016/j.heliyon.2022.e10739
59. Maleki M, Ghanbarvand F, Behvarz M, Ejtemaei M, Ghadirkhomi E. Comparison of mesenchymal stem cell markers in multiple human adult stem cells. Int J Stem Cells. 2014;7(2):118–126. doi:10.15283/ijsc.2014.7.2.118
60. Senbanjo LT, Chellaiah MA. CD44: a multifunctional cell surface adhesion receptor is a regulator of progression and metastasis of cancer cells. Front Cell Dev Biol. 2017;Volume 5. doi:10.3389/fcell.2017.00018
61. Moraes D, Sibov T, Pavon L, AlvimPQ. A reduction in CD90 (THY-1) expression results in increased differentiation of mesenchymal stromal cells. Stem Cell Res Ther. 2016;7:97. doi:10.1186/s13287-016-0359-3
62. Lefebvre V, Dumitriu B, Penzo-Mendez A, Han Y, Pallavi B. Control of cell fate and differentiation by Sry-related high-mobility-group box (Sox) transcription factors. Int J Biochem Cell Biol. 2007;39:2195–2214. doi:10.1016/j.biocel.2007.05.019
63. Bie Q, Zhai R, Chen Y, et al. Sox9 is crucial for mesenchymal stem cells to enhance cutaneous wound healing. Int J Stem Cells. 2021;14:465–474. doi:10.15283/ijsc21078
64. Krawetz R, Wu Y, Bertram K, et al. Synovial mesenchymal progenitor derived aggrecan regulates cartilage homeostasis and endogenous repair capacity. Cell Death Dis. 2022;13:470. doi:10.1038/s41419-022-04919-1
65. Roughley P, Mort J. The role of aggrecan in normal and osteoarthritic cartilage. J Exp Orthop. 2014;1:8. doi:10.1186/s40634-014-0008-7
66. Wu Z, Korntner S, Mullen A, Zeugolis D. From biosynthesis to advanced biomaterials for cartilage engineering. Biomaterial Biosyst. 2021;4:100030. doi:10.1016/j.bbiosy.2021.100030
67. Thiagarajan L, Abu-Awwad H, Dixon J. Osteogenic programming of human mesenchymal stem cells with highly efficient intracellular delivery of RUNX2. Stem Cell Transl Med. 2017;6:2146–2159. doi:10.1002/sctm.17-0137
68. Liu W, Zhang L, Xuan K,et al. ALPL prevents bone ageing sensitivity by specifically regulating senescence and differentiation in mesenchymal stem cells. Bone Res. 2018;6:27. doi:10.1038/s41413-018-0029-4
69. Malfait A, Little C, McDougall J. A commentary on modelling osteoarthritis pain in small animals. Osteoarthritis Cartilage. 2013;21:1316–1326. doi:10.1016/j.joca.2013.06.003
70. Kuyinu E, Narayanan G, Nair L, Laurencin C. Animal models of osteoarthritis: classification, update, and measurement of outcomes. J Orthop Surg Res. 2016;11:19. doi:10.1186/s13018-016-0346-5
71. Gupta P, Mahaeshwari S, Cherian J, et al. Efficacy and safety of stem-excel in osteoarthritis of the knee: a Phase 3 randomized, double-blind, multi center, placebo-controlled study. Am J Sports Med. 2023;51(9):2254–2266. doi:10.1177/03635465231180323
72. Chiang E-R, Ma H-L, Wang J-P, Liu C-L, Chen T-H, Hung S-C. Allogeneic mesenchymal stem cells in combination with hyaluronic acid for the treatment of osteoarthritis in rabbits. PLoS One. 2016;11(2):e0149835. doi:10.1371/journal.pone.0149835
73. Tjandra K, Novriansyah R, Sebastian Sudiasa I, Ar A, Mad R, Dilogo I. Modified mesenchymal stem cell, platelet-rich plasma and hyaluronic acid intervention in early stage osteoarthritis: a systematic review, meta-analysis and meta-regression of arthroscopic-guided intra-articular approaches. PLoS One. 2024;19(3):e0295876. doi:10.1371/journal.pone.0295876
74. Anil U, Markus D, Hurley E, et al. The efficacy of intra-articular injections in the treatment of knee osteoarthritis: a network meta-analysis of randomized controlled trials. Knee. 2021;32:173–182. doi:10.1016/j.knee.2021.08.008
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.