")
Back to Journals » Clinical Ophthalmology » Volume 18
Comparative Analysis of Effective Lens Position and Refractive Outcomes in Scleral-Fixated versus Intracapsular Intraocular Lenses
Authors Trivedi V, Lee S, Lee PSY , Me R, You Q, Im J, Ross B, Tran DV, Le KH, Malbin B, Lin X
Received 8 July 2024
Accepted for publication 22 November 2024
Published 25 December 2024 Volume 2024:18 Pages 3949—3955
DOI https://doi.org/10.2147/OPTH.S486044
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Vichar Trivedi,1 Stacey Lee,1 Patrick SY Lee,1 Rao Me,1 Qisheng You,1 Jacob Im,1 Bing Ross,1 David V Tran,1 Kim Hoang Le,2 Brett Malbin,1 Xihui Lin1
1Department of Ophthalmology, Visual and Anatomical Sciences, Kresge Eye Institute/Wayne State University School of Medicine, Detroit, MI, USA; 2Department of Ophthalmology, Henry Ford Hospital, Detroit, MI, USA
Correspondence: Xihui Lin, Kresge Eye Institute, Department of Ophthalmology, Visual and Anatomical Sciences, Wayne State University School of Medicine, 4717 St. Antoine Street Detroit, Detroit, MI, 48201, USA, Tel +1 313 577-8900, Email [email protected]
Purpose: To evaluate the outcomes of scleral-fixated intraocular lenses (IOLs) implanted using either Yamane technique or Gore-Tex suture fixation, in comparison to intracapsular lens fixation, and to assess the efficacy of various lens formulas in achieving predicted refractive targets.
Patients and Methods: This study included 45 eyes from 44 patients with scleral-fixated IOLs, comprising 37 Yamane eyes and 8 Gore-Tex eyes. Preoperative refractive predictions from various formulae were compared with final postoperative refraction. Outcomes assessed included effective lens position (ELP), postoperative predictive error, and changes in visual acuity. The ELP of scleral-fixated IOLs was compared with that of intracapsular IOLs in fellow eyes.
Results: Average ELP for Yamane IOLs was 0.62 mm more posterior relative to intracapsular IOLs but was not significantly different for Gore-Tex IOLs. Average postoperative logMAR acuity change was significant at – 1.30 (p=4.5x10− 11) and – 1.65 (p=5x10− 4) for Yamane and Gore-Tex eyes, respectively. Mean prediction error for Yamane eyes was +0.29± 1.3 D, − 0.53± 0.40 D, +0.80± 1.4 D, and +0.43± 1.4 D using Barrett Universal II, Holladay, Hill-RBF, and Hoffer QST formulas, respectively. Mean prediction error for Gore-Tex eyes was – 0.37± 1.24 D and +0.53± 1.19 D using Barrett Universal II and Holladay formulas, respectively.
Conclusion: Different scleral fixation techniques result in variations in ELP compared to intracapsular IOL placement. In our hands, when using the Yamane technique, surgeons should aim for a myopic refractive target to offset hyperopic errors when employing the Barrett Universal II, Hill-RBF, or Hoffer QST formulas, and a hyperopic target when using the Holladay formula. For Gore-Tex IOLs, a slightly hyperopic target is recommended to counter myopic error when using the Barrett Universal II formula, whereas a slightly myopic target is advised with the Holladay formula to offset hyperopic error. A limitation of our study is the small sample size for patients who underwent Gore-Tex suture fixation.
Keywords: secondary intraocular lens, Yamane technique, flanged technique
Introduction
During cataract surgery, intracapsular placement of the intraocular lens (IOL) is not only the most common method of lens implantation, but also the most desirable. However, other methods of IOL fixation are necessary when there is a loss of capsular support, such as in patients with a history of subluxated IOLs, damage to the capsular bag from surgery, pseudoexfoliation syndrome, or trauma.1,2 The Yamane technique is an increasingly popular method of secondary IOL implantation via scleral fixation, which involves passing a lens haptic through the sclera via two sclerotomies created by 30-gauge needles that are positioned 2.0 mm posterior to the corneal limbus and spaced 180 degrees apart.3,4 Low-temperature cautery is then used to create a flange at the end of the haptic, which is subsequently buried into the external sclera to secure the IOL.1,3 Compared to iris fixated or anterior chamber IOLs, scleral fixation has fewer associated complications, such as glaucoma, peripheral anterior synechiae, and corneal endothelial decompensation.2,3 However, scleral fixation is technically challenging and associated with a unique set of complications, including suture breakage and erosion of the suture material.2,5 Flanged haptic techniques have gained popularity as they reduce these risks; however, they can be associated with increased rates of tilt and decentration.2
Given patients’ increasingly demanding postoperative expectations in the modern era, it is critical to ensure that the best possible refractive outcome is achieved with scleral-fixated intraocular lenses. Most of the formulae for calculation of IOL power assume that the lens is placed within the capsular bag. When an IOL is scleral-fixated, lens calculation parameters such as effective lens position (ELP) and anterior chamber depth (ACD) may be altered, introducing unpredictability to surgical outcomes.6 It is therefore important to better understand how these parameters differ between a scleral fixated versus intracapsular IOL. The aim of this study was to evaluate the postoperative ELP and the resulting residual refractive error following scleral fixation of IOL with Yamane technique or Gore-tex suture fixation versus intracapsular IOL placement.
Materials and Methods
This retrospective chart review analyzed patients who underwent secondary IOL placement via scleral fixation between March 2019 and March 2023. Patient data was collected from the electronic medical record from January 2019 to February 2024. Eligible participants were all individuals aged 18 years or older who received a scleral fixated IOL with or without sutures within the study period. The study was submitted for review to the Wayne State University Institutional Review Board and deemed as exempt research by, and consent was waived due to its retrospective nature. All data was maintained with confidentiality. The study adhered to the Declaration of Helsinki.
Patient demographics, medical history, diagnoses, and indications for surgical intervention were extracted from medical records. Patient data were collected retrospectively from all preoperative and postoperative visits. Interval examinations at each visit included slit lamp exams and pupil dilation with posterior segment exam. Preoperative measurements for IOL calculations were obtained using the IOL Master 700 (Carl Zeiss Meditec, Jena, Germany). Preoperative visual acuity and manifest refraction were also recorded.
At our institution, sclerotomy sites for the Yamane procedure are placed 2.0 mm posterior to the limbus. For the Gore-tex fixated technique, sutures are positioned 2.5 mm posterior to the limbus. All surgeries were performed by a single surgeon (X.L.) in the same operating room at our institution. All patients underwent scleral-fixated IOL placement without any intraoperative complications for both the Yamane and Gore-tex fixated groups.
Postoperatively, all patients had a manifest refraction to assess their refractive error after a stabilization period of two months. A predicted refractive error was then calculated. Predicted refractive error is equal to the spherical equivalent of the actual refraction measured after surgery minus the refraction that was predicted before the surgery using the intended IOL calculation formula. The ELP was also determined 2 months post-operatively after scleral fixation. This was calculated by UBM or utilizing IOL Master 700 using anterior chamber depth as a surrogate value. The refractive error of the scleral fixated lens was also compared to intracapsular lens placement in the fellow eye.
A two-tailed Student’s t-test was performed to compare IOL position and postoperative residual refractive error in eyes with scleral-fixated IOLs compared to intracapsular IOLs. A p-value of <0.05 was used to determine statistical significance. All analyses were performed on GraphPad Prism 6 software.
Results
This study included 45 eyes from 44 patients that received a scleral fixated IOL. The Yamane technique using an Alcon MA60AC lens (Alcon, Fort Worth, Texas) was utilized in 37 eyes, whereas 8 eyes underwent the Gore-Tex suture technique using an Akreos AO60 lens (Bausch & Lomb, Bridgewater, New Jersey). The majority of participants were male (31 out of 45), with an age range of 30 to 91 years (Table 1). The most prevalent indications for surgery included post-surgical aphakia without an intact capsular bag in 22 patients, traumatic subluxation of the crystalline lens in 9 patients, and dislocation of an artificial IOL in 8 patients (Table 2). The mean preoperative uncorrected and postoperative best corrected logMAR acuity in the Yamane group were 2.01± 0.13 and 0.71± 0.11, respectively, with a mean difference of −1.30 (p = 4.5×10-11). For the Gore-Tex group, the mean preoperative uncorrected and postoperative best corrected logMAR acuity were 1.94± 0.30 and 0.29± 0.10, respectively, with a mean difference of −1.65 (p = 5×10-4).
 |
Table 1 Patient Demographics |
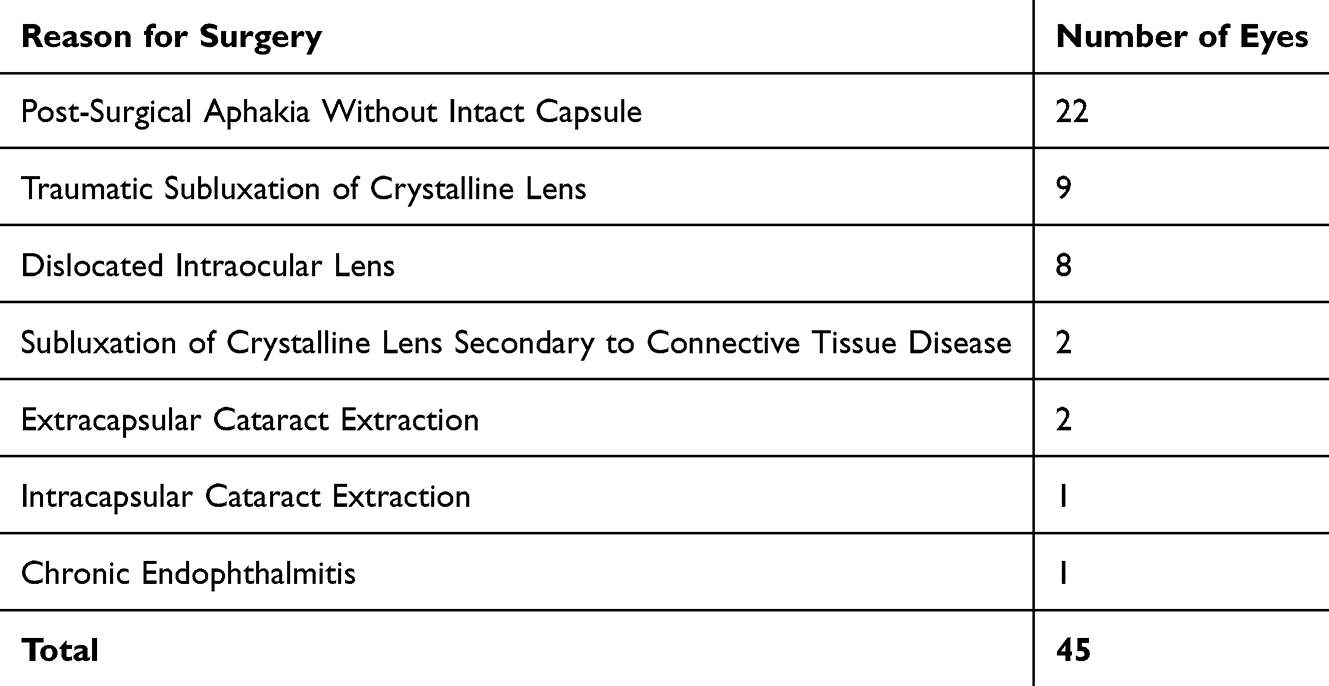 |
Table 2 Patient Condition Necessitating Placement of Scleral-Fixated Intraocular Lens |
Lens positioning was evaluated based on the postoperative effective lens position (ELP). Postoperative ELP data was available for 23 of the Yamane patients and 2 of the Gore-Tex patients. The average ELP in post-Yamane patients was 5.01 ± 0.55 mm. Of these patients, 8 had intracapsular posterior chamber IOLs in the contralateral eye with an average ELP of 4.39 ± 0.78 mm, a difference of 0.62 mm (p = 0.021) between the more posterior final position of the Yamane-fixated IOLs versus intracapsular IOLs. In contrast, the average ELP in patients with Gore-Tex suture fixated IOLs was 3.50 ± 0.37 mm, which was 0.77 mm (p = 0.11) more anterior in comparison to an ELP of 4.27 ± 0.17 mm in their contralateral eyes with intracapsular IOLs (Table 3).
 |
Table 3 Effective Lens Position (ELP) for Scleral-Fixated versus Intracapsular Intraocular Lenses |
In the Yamane cohort, the mean predictive errors of the Barrett Universal II, Holladay, Hill-RBF, and Hoffer QST formulae were +0.29 ± 1.3 D, −0.53 ± 0.40 D, +0.80 ± 1.4 D, and +0.43 ± 1.4 D, respectively (Table 4).
 |
Table 4 Predictive Errors of Intraocular Lens Calculation Formulas |
In the Gore-Tex suture-fixated group, the mean predictive errors of the Barrett Universal II and Holladay formulae were –0.37 ± 1.24 D and +0.53 ± 1.19 D, respectively. The Hill-RBF and Hoffer QST formulae were not evaluated in this cohort because they required a preoperative anterior chamber depth, which was only available for two patients.
Discussion
Our study demonstrates that there are significant differences in lens positioning and refractive outcomes between primary intracapsular IOL placement and secondary IOL implantation by scleral fixation techniques. When compared to the intracapsular IOLs in the contralateral eyes, IOLs fixated with the Yamane technique had a more posterior final position (delta ELP = −0.62 mm) while those that were Gore-Tex suture fixated were more anterior (delta ELP = +0.77 mm). In the Yamane cohort, the mean predictive errors of the Barrett Universal II, Holladay, Hill-RBF, and Hoffer QST formulae were +0.29 ± 1.3 D, −0.53 ± 0.40 D, +0.80 ± 1.4 D, and +0.43 ± 1.4 D, respectively (Table 4). In the Gore-Tex suture-fixated group, the mean predictive errors of the Barrett Universal II and Holladay formulae were –0.37 ± 1.24 D and +0.53 ± 1.19 D, respectively.
Residual refractive errors following scleral fixation of IOLs in the literature have been variable. Schranz et al reported an average ELP of 4.05 mm using the Yamane technique and variability in predictive error across depending on the IOL power formula used: the SRK/T formula tended towards myopic errors, while the Holladay 1 and Hoffer Q formulas typically resulted in hyperopic errors. However, regardless of the type of error, their multivariable analysis demonstrated that ELP significantly influences predictive error irrespective of the formula used.1 Aykut et al employed a Yamane technique and noted a hyperopic error of +0.85 D ± 1.15 D. This comparison was relative to preoperative intracapsular calculations using the SRK/T formula for eyes with an axial length of 22–26 mm and the Haigis formula for eyes with axial length of more than 26 mm.7 Similarly, Lee et al also reported a hyperopic refractive error of +0.39 D ± 1.42 D, relative to preoperative intracapsular calculations using the Barrett Universal Formula.8 McMillin et al consistently found a hyperopic predictive error for eyes with the Yamane technique across several formulas: +0.48 D with Holladay 1, +0.46 D with Barrett Universal II, +0.57 D with SRK/T, and +0.67 D with Hoffer Q, with the predictive error for each formula being statistically significant.4
Conversely, Rocke et al did not observe a significant residual refractive error in eyes with scleral fixation using the Yamane technique relative to those with intracapsular placement.9 Similarly, Yamane’s original study also did not demonstrate a significant mean refractive error using the SRK/T formula.3 However, the reason for this discrepancy is unclear as neither group evaluated the effect of ELP on final outcomes. Interestingly, a similar study that was previously done at our institution also did not identify a significant overall residual refractive error in patients that underwent scleral fixation with the Yamane technique. Holladay 2, SRK, and Barrett Universal II resulted in a mild myopic error (−0.55, −0.18, and −0.20 D), while Haigis and Hill-RBF (Radial Basis Function) resulted in mild hyperopic error (+0.28 and +0.28 D). Hoffer Q and Holladay 1 were the most accurate (−0.02 D and −0.08 D).10
In this current study, a hyperopic error was observed for the Barrett Universal II formula, Hill-RBF, and Hoffer QST, while the Holladay 2 produced a myopic error when all patients with fixation using the Yamane technique were included in the calculation. The Holladay 2 formula resulted in a smaller standard deviation and thus less variability with this calculation, though further study is necessary to determine if this remains true with a larger sample size.
For the 8 patients in our study undergoing the Gore-Tex suture technique, the average ELP was 3.50 ± 0.37 mm, compared to 4.27 ± 0.17 mm for intracapsular IOLs in the fellow eyes. This places the IOL at an average of 0.74 mm more anteriorly, though the difference was not statistically significant. It is worth nothing that the Holladay formula led to more hyperopic outcomes (predictive error of about +0.53 D) than the Barrett Universal II formula (predictive error of about −0.37D). However, determination of statistical significance is limited by the small sample size of this cohort, and further study is warranted.
For Gore-Tex suture fixation, the predicted refractive error appears to vary between different authors utilizing the same technique. Su et al found a nonsignificant mean predicted error of –0.43 ± 0.71 D for Gore-Tex fixation 3 mm posterior to the limbus and significantly myopic error of –1.35 ± 1.32 D for fixation 2 mm posterior to the limbus.11 In our institution, we perform Gore-Tex fixation at 2.5 mm posterior to the limbus. Wei et al demonstrated a nonsignificant error of −0.17 D ± 0.60 D using the SRK-T formula.12 In contrast, Li et al observed a myopic error in patients with a Gore-Tex sutured IOL across multiple formulas, including SRK/T, Holladay 1, Hoffer Q, Haigis, and Barrett II.13 Similarly, Botsford et al, Hayashi et al, and Fass et al described myopic predictive errors in the placement of suture-fixated lenses.14–16 Though these results are similar, the variability in results is likely due to both surgeon- and patient-specific factors, though further study is needed.
The average pre-op and post-op best corrected logMAR acuity for the Yamane group was 2.01 ± 0.13 and 0.71 ± 0.11, respectively, with a difference of −1.30 (p<0.001). For the suture-fixated group, the average pre-operative and post-operative best corrected logMAR acuity was 1.94 ± 0.30 and 0.29 ± 0.10, respectively, with a difference of −1.65 (p<0.001).17,18 Other studies have shown similar increases in vision after the placement of a scleral-fixated lens via both the Yamane and suture-fixated techniques.19–21 Though we did not assess this in our study, another factor potentially influencing visual acuity is the degree of IOL tilt, which is common but does not appear to significantly worsen visual outcomes.22–24
This study provides valuable insights into the practical applications and outcomes of newer scleral fixation methods. The detailed measurements of ELP allow for a better understanding of the resulting position of the IOL postoperatively. The diversity in patient demographics, with ages ranging from 30 to 91 and various surgical indications such as aphakia, subluxation, and lens dislocation, broadens the study’s applicability to a wider patient population.
However, the study also presents certain limitations. As surgical technique plays a critical role in refractive outcomes, the results may not be generalizable to other practices using different techniques for fixation. However, this study provides a framework that others may use to determine the optimal method to approach lens calculations for intrascleral fixation of intraocular lenses. The small number of patients undergoing the Gore-Tex suture technique limits the statistical power of the comparisons involving this method, potentially affecting the generalizability of these specific results. As a retrospective study, it is more prone to bias and the effects of confounding variables. Moreover, the absence of long-term follow-up data restricts our ability to assess the durability and stability of the lens placements, as well as the long-term refractive outcomes and complications in these patients. Lastly, this study does not include comparisons with more traditional secondary lens methods such as anterior chamber intraocular lenses.
Conclusion
Our study provides an increased understanding regarding the anatomical and refractive differences with different scleral fixation techniques. IOL fixation with the Yamane technique resulted in a more posterior ELP compared to intracapsular fixation. Based on data from our surgical technique, with IOL fixation using the Yamane technique, surgeons should aim for a myopic refractive target to offset hyperopic errors when employing the Barrett Universal II, Hill-RBF, or Hoffer QST formulas, and a hyperopic target when using the Holladay formula. For a Gore-Tex IOL, a slightly hyperopic target is recommended to counter myopic error when using the Barrett Universal II formula, whereas a slightly myopic target is advised with the Holladay formula to offset hyperopic error. Individual surgeons may wish to assess the performance of these formulas in a similar manner in their own practice.
Funding
This work was supported by Research to Prevent Blindness [P30-EY04068], National Institutes of Health, Bethesda, MD (Non restricted grant to the Department of Ophthalmology, Visual and Anatomical Sciences).
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Schranz M, Reumüller A, Kostolna K, Novotny C, Schartmüller D, Abela-Formanek C. Refractive outcome and lens power calculation after intrascleral intraocular lens fixation: a comparison of three-piece and one-piece intrascleral fixation technique. Eye Vis. 2023;10(1):29. doi:10.1186/s40662-023-00341-6
2. Park CH, Moon K, Kim JH, Shim KY, Jun JH. contribution factors of effective lens position, tilt, and decentration during flanged scleral fixation of intraocular lens: A model eye study. Retina. 2024;44(2):324–332. doi:10.1097/IAE.0000000000003960
3. Yamane S, Sato S, Maruyama-Inoue M, Kadonosono K. Flanged Intrascleral Intraocular Lens Fixation with Double-Needle Technique. Ophthalmology. 2017;124(8):1136–1142. doi:10.1016/j.ophtha.2017.03.036
4. McMillin J, Wang L, Wang MY, et al. Accuracy of intraocular lens calculation formulas for flanged intrascleral intraocular lens fixation with double-needle technique. J Cataract Refract Surg. 2021;47(7):855–858. doi:10.1097/j.jcrs.0000000000000540
5. Solomon K, Gussler JR, Gussler C, Van Meter WS. Incidence and management of complications of transsclerally sutured posterior chamber lenses. J Cataract Refract Surg. 1993;19(4):488–493. doi:10.1016/S0886-3350(13)80612-8
6. Ohr MP, Wisely CE. Refractive outcomes and accuracy of IOL power calculation with the SRK/T formula for sutured, scleral-fixated Akreos AO60 intraocular lenses. Graefes Arch Clin Exp Ophth. 2020;258(10):2125–2129. doi:10.1007/s00417-020-04721-9
7. Aykut V, Esen F, Sali F, Oguz H. Refractive outcome of trocar-assisted sutureless scleral fixation with 3-piece intraocular lenses. Int Ophthalmol. 2021;41(8):2689–2694. doi:10.1007/s10792-021-01824-y
8. Lee R, Govindaraju V, Farley ND, et al. Refractive Outcomes After Sutureless Intrascleral Fixation Of Intraocular Lens With Pars Plana Vitrectomy. Retina. 2021;41(4):822–826. doi:10.1097/IAE.0000000000002916
9. Rocke JR, McGuinness MB, Atkins WK, et al. Refractive Outcomes of the Yamane Flanged Intrascleral Haptic Fixation Technique. Ophthalmology. 2020;127(10):1429–1431. doi:10.1016/j.ophtha.2020.03.032
10. Malach DS, Guest JM, Adam C, et al. Intraocular Lens Formula Comparison of Flanged Intrascleral Intraocular Lens Fixation with Double Needle Technique. Clin Ophthalmol. 2023;17:837–842. doi:10.2147/OPTH.S389325
11. Su D, Stephens JD, Obeid A, et al. Refractive Outcomes after Pars Plana Vitrectomy and Scleral Fixated Intraocular Lens with Gore-Tex Suture. Ophthalmol Retina. 2019;3(7):548–552. doi:10.1016/j.oret.2019.02.012
12. Wei W, Lin H, Zheng X, Wang S, Bai S, Zhao Z. Refractive outcomes of scleral-sutured posterior chamber intraocular lenses in post-traumatic eyes. Int Ophthalmol. 2023;43(2):423–429. doi:10.1007/s10792-022-02439-7
13. Li Z, Lian Z, Young CA, Zhao J, Jin G, Zheng D. Accuracy of intraocular lens calculation formulas for eyes with insufficient capsular support. Ann Transl Med. 2021;9(4):324. doi:10.21037/atm-20-3290
14. Botsford BW, Williams AM, Conner IP, Martel JN, Eller AW. Scleral Fixation of Intraocular Lenses with Gore-Tex Suture: refractive Outcomes and Comparison of Lens Power Formulas. Ophthalmol Retina. 2019;3(6):468–472. doi:10.1016/j.oret.2019.02.005
15. Hayashi K, Hayashi H, Nakao F, Hayashi F. Intraocular lens tilt and decentration, anterior chamber depth, and refractive error after trans-scleral suture fixation surgery. Ophthalmology. 1999;106(5):878–882. doi:10.1016/S0161-6420(99)00504-7
16. Fass ON, Herman WK. Four-point suture scleral fixation of a hydrophilic acrylic IOL in aphakic eyes with insufficient capsule support. J Cataract Refract Surg. 2010;36(6):991–996. doi:10.1016/j.jcrs.2009.12.043
17. Gregori NZ, Feuer W, Rosenfeld PJ. Novel method for analyzing Snellen visual acuity measurements. Retina. 2010;30(7):1046–1050. doi:10.1097/IAE.0b013e3181d87e04
18. Tsou BC, Bressler NM. Visual Acuity Reporting in Clinical Research Publications. JAMA Ophthalmol. 2017;135(6):651–653. doi:10.1001/jamaophthalmol.2017.0932
19. Jiang H, Chen H, Tan ZL, Zou M, ZP L, Fan W. Clinical Outcomes of the Scleral Fixation of Posterior Chamber Intraocular Lens using the Modified Yamane’s Technique: a Swept-source Optical Coherence Tomography Study. Sichuan Da Xue Xue Bao Yi Xue Ban. 2020;51(6):859–865. doi:10.12182/20201160506
20. Forlini M, Bedi R. Intraocular lens implantation in the absence of capsular support: scleral-fixated vs retropupillary iris-claw intraocular lenses. J Cataract Refract Surg. 2021;47(6):792–801. doi:10.1097/j.jcrs.0000000000000529
21. Kansal V, Onasanya O, Colleaux K, Rawlings N. Outcomes of Using Sutureless, Scleral-Fixated Posterior Chamber Intraocular Lenses. Semin Ophthalmol. 2019;34(7–8):488–496. doi:10.1080/08820538.2019.1652761
22. Kemer Atik B, Altan C, Agca A, et al. The effect of intraocular lens tilt on visual outcomes in scleral-fixated intraocular lens implantation. Int Ophthalmol. 2020;40(3):717–724. doi:10.1007/s10792-019-01233-2
23. Oli A, Yadav A, Babu JG, Balakrishnan D. Scheimpflug imaging for evaluation of intraocular lens position in modified flanged scleral fixated intraocular lens. Ther Adv Ophthalmol. 2023;15:25158414221147208. doi:10.1177/25158414221147208
24. Sül S, Kaderli A, Karalezli A, Kaya C. Comparison of decentration, tilt and lenticular astigmatism of ıntraocular lens between sutured and sutureless scleral fixation techniques. J Fr Ophtalmol. 2021;44(8):1174–1179. doi:10.1016/j.jfo.2020.12.031
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Intraocular Lens Formula Comparison of Flanged Intrascleral Intraocular Lens Fixation with Double Needle Technique

Malach DS, Guest JM, Adam C, Joffe J, Le K, Kim C, Lin X
Clinical Ophthalmology 2023, 17:837-842
Published Date: 12 March 2023