")
Back to Journals » Journal of Asthma and Allergy » Volume 18
Comparative Analysis of ICS Combined with LABA versus Addition of Omalizumab on Transcriptomic Expression Profiles in Patients with Allergic Asthma
Authors Liang YR, Chang CH, Huang SY, Wu YK , Yang MC , Huang KL, Tzeng IS , Hsieh PC , Lan CC
Received 17 December 2024
Accepted for publication 15 May 2025
Published 5 June 2025 Volume 2025:18 Pages 941—954
DOI https://doi.org/10.2147/JAA.S511885
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Ya-Ru Liang,1,* Chuan-Hsin Chang,2,* Shiang-Yu Huang,1 Yao-Kuang Wu,3,4 Mei-Chen Yang,3,4 Kuo-Liang Huang,3,4 I-Shiang Tzeng,2 Po-Chun Hsieh,5,6,* Chou-Chin Lan3,4,*
1Division of Respiratory Therapy, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, New Taipei City, Taiwan; 2Department of Research, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, New Taipei City, Taiwan; 3Division of Pulmonary Medicine, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, New Taipei City, Taiwan; 4School of Medicine, Tzu-Chi University, Hualien, Taiwan; 5Department of Chinese Medicine, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, New Taipei City, Taiwan; 6School of Chinese Medicine, National Yang Ming Chiao Tung University, Taipei, Taiwan
*These authors contributed equally to this work
Correspondence: Chou-Chin Lan, Division of Pulmonary Medicine, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, 289, Jianguo Road, Xindian City, New Taipei City, 23142, Taiwan, Tel +886-2-6628-9779 ext. 2259, Fax +886-2-6628-9009, Email [email protected]
Introduction: Asthma causes airway inflammation, leading to symptoms that impair patients’ quality of life, making it a significant global public health issue. Inhaled corticosteroids (ICS) with long-acting beta-agonists therapy (LABA) is commonly used to manage moderate to severe asthma. For patients unresponsive to ICS with LABA, omalizumab may be added to improve asthma control. Understanding transcriptomic expressions is crucial as it provides insights into the molecular mechanisms underlying treatment. However, the impact of omalizumab on transcriptomic expressions remains unclear. Therefore, this study aims to investigate the transcriptomic expression profiles and clinical outcomes between patients receiving ICS with LABA therapy and those adding omalizumab.
Materials and Methods: This is a prospective, real-world study that enrolled 26 participants, divided into three groups: Group 1, ICS with LABA (n=10); Group 2, ICS with LABA plus omalizumab (n=12); and Group 3, healthy controls (n=4). Assessments included transcriptomic expression profiles, and bioinformatics analysis, IgE, airborne allergen test, pulmonary function test, blood tests, and asthma control test (ACT).
Results: ACT scores were significantly higher in Group 1 and 2 compared to Group 3. IgE levels, dust mite sensitivity, and dynamic pulmonary function changes after bronchodilator administration were notably higher in Group 2. In these patients, down-regulated genes included those related to immune response, NOD-like receptor signaling, RIG-I signaling, IL-17 signaling, and antioxidant activity. Conversely, up-regulated genes were found in the cGMP-PKG signaling pathway, cardiomyopathy-related pathways, and voltage-gated calcium channel activity.
Conclusion: Patients receiving ICS with LABA plus omalizumab still exhibited more dynamic airway changes and higher IgE levels. Downregulation of immune and inflammatory pathways suggests its potential as an add-on treatment for severe asthma. However, upregulated genes were observed in the cGMP-PKG signaling pathway, cardiomyopathy-related pathways, and voltage-gated calcium channel activity.
Keywords: asthma, airway inflammation, omalizumab, RNA transcriptome
Introduction
Asthma is a chronic respiratory condition that causes airway inflammation and obstruction, leading to symptoms such as wheezing, breathlessness, chest tightness, and coughing.1 Uncontrolled asthma often results in a diminished health-related quality of life and impairing daily activities. Asthma is therefore a significant global public health concern, affecting an estimated 334 million people worldwide.1 Understanding the importance of asthma and its proper management is crucial for minimizing its impact on both individuals and communities.
The Global Initiative for Asthma (GINA) provides evidence-based guidelines for asthma management, which focus on reducing symptoms, preventing exacerbations, and improving the overall quality of life for patients.2 According to GINA guidelines, the combination of inhaled corticosteroids (ICS) and long-acting beta-agonists (LABA) is recommended as an essential therapy for managing moderate to severe asthma. ICS is the cornerstone of asthma therapy and it are pivotal in reducing airway inflammation, while LABAs provide prolonged bronchodilation, helping to relieve asthma symptoms and prevent exacerbations.2 The GINA guidelines suggest that for patients who require regular controller therapy, starting with an ICS with LABA combination is often more effective than using ICS alone. This combination therapy can improve symptom control and reduce the risk of exacerbations.2
For patients with severe asthma who do not achieve adequate control by ICS with LABA, the addition of biologics may be considered, as outlined in the GINA framework.2 Omalizumab (Xolair®) is a monoclonal antibody that targets immunoglobulin (Ig) E.2 It plays a crucial role in the management of moderate to severe asthma, particularly in patients with allergic asthma. By binding to free IgE in the bloodstream, omalizumab prevents it from attaching to its high-affinity receptors (FcεR1) on mast cells and basophils, thereby inhibiting the allergic inflammatory response that contributes to asthma exacerbations.3 Clinical studies have demonstrated that omalizumab significantly reduces the frequency of asthma attacks, improves lung function, and enhances overall quality of life for patients.3 Additionally, its use has been associated with a decrease in the need for corticosteroids, reducing potential side effects.3
A central feature of asthma is the presence of symptoms caused by underlying airway inflammation. ICS with LABA therapy is the mainstay treatment for moderate to severe asthma. Omalizumab is often added when patients do not respond well to ICS with LABA. However, the molecular changes, such as differences in RNA transcription expressions, between ICS with LABA and ICS with LABA plus omalizumab remain unclear. Transcriptomic expression analysis plays a crucial role in understanding the molecular mechanisms underlying the effects of different treatments.4 By examining the transcriptome, which encompasses the entire set of RNA transcripts, we can gain insights into gene expression changes that occur in response to treatments such as ICS with LABA versus the addition of omalizumab. This approach allows for a comprehensive understanding of how these therapies influence immune responses, airway inflammation, and other biological processes at the molecular level.4,5 In the current study, we aimed to investigate the transcriptomic expression profiles and clinical outcomes between patients receiving ICS with LABA and those receiving ICS with LABA combined with omalizumab.
Materials and Methods
Participant Enrollment
This prospective real-world study included adult patients with asthma. Treatment followed GINA guidelines, initially with ICS with LABA.2 For patients with poor asthma control despite ICS with LABA, omalizumab was added according to Taiwan’s National Health Insurance criteria for those with elevated IgE levels and allergen positivity. The study included participants, categorized into three groups: Group 1 consisted of patients receiving ICS with LABA therapy, Group 2 consisted of patients receiving ICS with LABA plus omalizumab, and Group 3 was the healthy control group. The inclusion criteria required participants to be adults over 18 years old with a confirmed asthma diagnosis, verified through a provocation test, and receiving treatment in accordance with GINA guidelines. The ICS with LABA group included patients with asthma classified as stages III to V, while the ICS with LABA and omalizumab group comprised patients with inadequate asthma control despite ICS with LABA therapy, elevated IgE levels, and positive allergen test results. Only patients who were willing to participate in the study were included. Exclusion criteria included current smokers, individuals with other lung diseases (such as lung cancer, chronic obstructive pulmonary disease, bronchiectasis, or interstitial lung disease), or those with systemic conditions such as diabetes, hypertension, myocardial infarction, congestive heart failure, autoimmune diseases, renal dysfunction, hepatic dysfunction, and cancers. Healthy controls were chosen based on strict criteria, ensuring no prior history of asthma or other diseases, and no current medication use. Patients who were unwilling to participate in the study were excluded.
Severe asthma affects approximately 5% to 10% of the asthma population.6 Omalizumab is indicated only for patients with severe allergic asthma.7 To minimize the influence of other diseases on transcriptional expression, we applied strict screening criteria. Therefore, only 12 patients receiving omalizumab were included in this study. To ensure a balanced comparison, we included a similar number of asthma patients receiving ICS with LABA. From a statistical perspective, while the small sample size limits the power of certain comparisons, the inclusion of a comparable number of patients in each group allows for meaningful exploratory analysis, considering the rare nature of severe asthma and the stringent selection process for patients.
The study protocol was approved by the Ethics Committee of Taipei Tzu Chi Hospital (IRB number 10-XD-154). ClinicalTrials.gov has approved the study, and the registration number is NCT06869382. Informed consent was obtained from all participants. All participants underwent pulmonary function tests (PFT), general blood tests, allergen tests, IgE measurements, and RNA transcription analysis.
Pulmonary Function Test
Patients underwent pulmonary function tests following the guidelines of the American Thoracic Society,8 using a spirometer manufactured by Medical Graphics Corporation in the USA. Measurements included forced vital capacity (FVC) and forced expiratory volume in the one second (FEV1). Airflow obstruction was assessed by calculating the FEV1 percentage.9 Additional measurements included mid-maximum expiratory flow (MMEF, L/s and %), as well as peak expiratory flow rate (PEFR, mL).
Blood Test
All patients received thorough blood tests, which included RNA transcriptome analysis, airborne allergen test, total IgE levels, and complete blood counts with differentials, hemoglobin (Hb), aspartate aminotransferase (AST), alanine aminotransferase (ALT), total bilirubin, creatinine (Cr), blood urea nitrogen (BUN), C-reactive protein (CRP), potassium (K), and sodium (Na). Levels of total IgE and airborne allergen-specific IgE were determined by the ImmunoCAP system (Thermo Fisher Scientific, Uppsala, Sweden). IgE specific to inhaled allergens including Dermatophagoides pteronyssinus, dog dander, cat dander, fungi and cockroach were measured. Allergen-specific IgE levels ≥0.35 UA/mL regarded as positive.
Asthma Control
The Chinese-language Asthma Control Test (ACT) was used to assess asthma control level.10 The ACT contains five questions, each rated on a scale from 0 to 5, giving a possible total score between 0 and 25, where higher scores indicate improved asthma management.
Library Preparation and Sequencing
Purified RNA was utilized to create sequencing libraries using the TruSeq Stranded mRNA Library Prep Kit (Illumina, San Diego, CA, USA). mRNA was extracted from 1 µg of total RNA with oligo(dT)-coupled magnetic beads and then fragmented into smaller pieces through heat treatment. First-strand cDNA synthesis was carried out using reverse transcriptase along with random primers. After the synthesis and adenylation of double-stranded cDNA at the 3′ ends, adapters were ligated, and the library was purified with the AMPure XP system (Beckman Coulter, Beverly, USA). The quality of the library was evaluated using the Agilent Bioanalyzer 2100 system and real-time PCR. Qualified libraries were sequenced on the Illumina NovaSeq 6000 platform, producing 150 bp paired-end reads by Genomics (New Taipei City, Taiwan).
Bioinformatics Analysis
Raw data sequences were cleaned by removing adapter sequences and low-quality bases using the Fastp program (version 0.23.4). Filtered reads were aligned to reference genomes using STAR (version 2.7.11b). Transcript abundance was quantified with RSEM (version 1.2.28). Differentially expressed genes were identified using edgeR (version 4.2.1), and functional enrichment of Gene Ontology (GO) terms and Kyoto Encyclopedia of Genes and Genomes (KEGG) pathways among gene clusters was analyzed using the R package clusterProfiler (version 3.6.0) and a web tool, ShinyGO (version 0.80, http://bioinformatics.sdstate.edu/go/). The FASTQ files of RNA sequencing data are available at the National Center for Biotechnology Information.
Statistical Analysis
All statistical analyses were performed using IBM SPSS Statistics version 26.0 (IBM, Armonk, NY, USA). We assessed normality using the Shapiro–Wilk test, Chi-square tests, and Normal Q-Q plots. Demographic, laboratory, and clinical characteristics of the participants were summarized as means and standard deviations for continuous variables and as frequencies with percentages (n, %) for categorical variables. Fisher’s exact test was employed to assess differences among three groups for categorical data. For continuous variables, one-way ANOVA was applied when the normality assumption was met; otherwise, the Kruskal–Wallis test was utilized. If the results were significant in normally distributed data, post hoc multiple comparisons were conducted. For non-normally distributed data, the Mann–Whitney test with Bonferroni correction was used to adjust for type I error. The generalized estimating equations (GEE) approach was employed for multiple linear regression analysis to evaluate the time effects of pulmonary function tests among the three groups. The autoregressive of order 1 working correlation matrix was selected to account for time-dependent correlations in repeated measurements (pre- and post-bronchodilator). A p-value of less than 0.05 was considered statistically significant.
Results
Demographic and Clinical Features
The study included 26 participants: 10 participants in Group 1, 12 participants in Group 2, and 4 participants in Group 3. The baseline characteristics and clinical symptoms are shown in Table 1. The sex distribution, age, body height, body weight, and BMI and smoking status was similar across groups (all p > 0.5). Group 3 had better ACT scores than Group 1 (p = 0.010) and Group 2 (p = 0.033), with no significant difference between Group 1 and Group 2 (p = 0.417). Both Group 1 and Group 2 had 100% use of ICS with LABA, and LAMA use did not differ between the two groups (all p > 0.05). The mean duration of ICS with LABA was 362.1 ± 208.6 days in Group 1, while the mean duration of ICS with LABA plus omalizumab in Group 2 was 423.0 ± 145.8 days (p=0.431). No participants in the three groups had other respiratory or systemic diseases, as participants with other pulmonary and systemic diseases were excluded from the study based on the inclusion and exclusion criteria.
 |
Table 1 Comparing the Baseline Characteristics Among Three Groups |
Laboratory Data
The comparison of laboratory data, IgE level, and allergen levels among the three groups is shown in Table 2. Most laboratory parameters, including WBC count, hemoglobin, and platelets, showed no significant difference between the groups (all p>0.05). IgE levels were significantly higher in the Group 2 compared to Group 3 (p=0.003). Additionally, dust mite sensitivity was significantly higher in the Group 2 group (35.8 ± 36.3) compared to Group 1 (4.0 ± 4.1, p=0.021) and Group 3 (0.2 ± 0.2, p=0.003). Fungus sensitivity was significantly higher in the Group 2 (1.0 ± 2.7) compared to the Group 3 (0.0 ± 0.0, p=0.021).
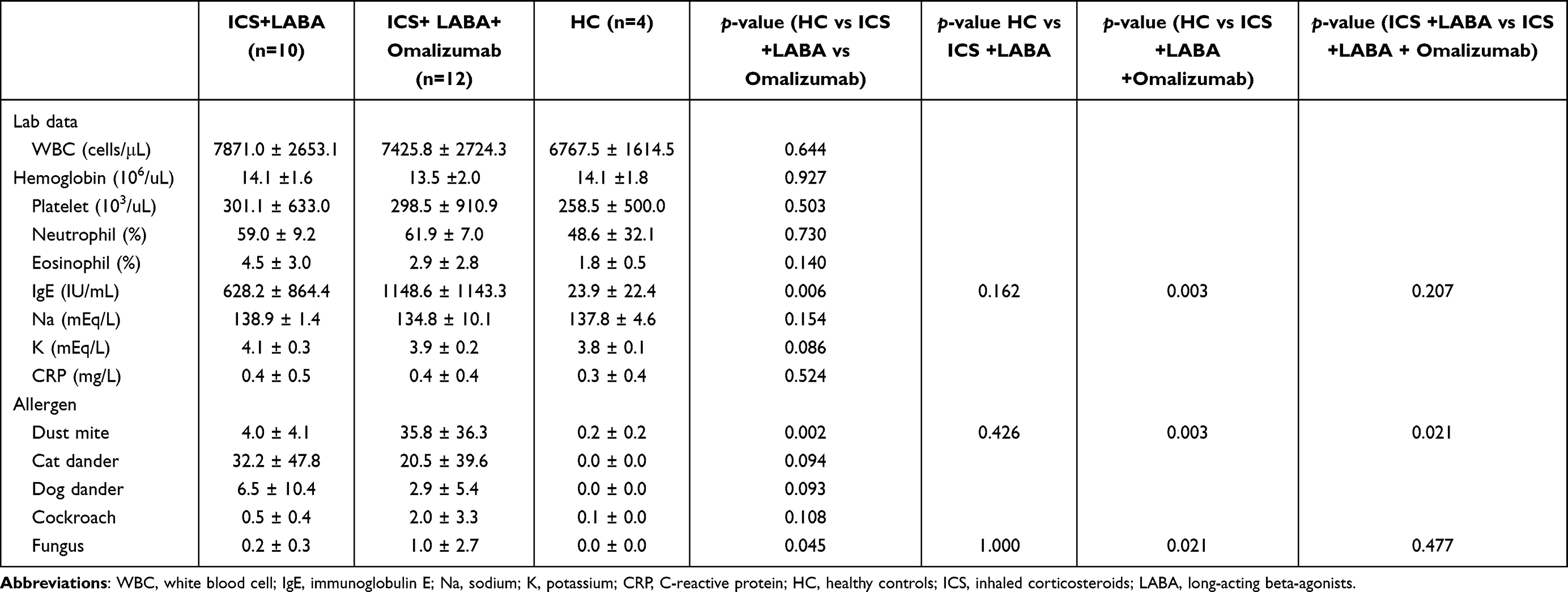 |
Table 2 Comparing the Laboratory Data and Allergens Among Three Groups |
Pulmonary Function Test
Pulmonary function test results are shown in Table 3. The result of GEE method’s multiple linear regression was used to compare the differences of the time effects among three groups is shown in Table 4. The results of the GEE multiple linear regression comparing the treatment effects among the three groups to show significant differences in several lung function parameters. For FVC, Group 2 had a significantly lower value compared to Group 1 (B = −0.468, p = 0.048), and the interaction between Group 2 and Time 2 (post-bronchodilator) was also significant (B = 0.181, p < 0.001). Similarly, for FVC%, Group 2 showed a significant decrease compared to Group 1 (B = −11.367, p = 0.042), with significant interaction for Group 2 and Time 2 (B = 5.617, p < 0.001). In terms of FEV1, Group 2 also exhibited a significant reduction compared to Group 1 (B = −0.465, p = 0.041), although there was no significant interaction between Time 2 and the groups. For FEV1/FVC%, Group 3 demonstrated a higher ratio compared to Group 1 (B = 10.200, p = 0.004), while Group 2 showed no significant difference. MMEF and MMEF% were markedly higher in Group 3 compared to Group 1 (B = 1.422, p < 0.001 and B = 37.300, p = 0.002, respectively). Group 2 had a significant interaction with Time 2 for MMEF (B = 0.901, p < 0.001) and MMEF% (B = 29.667, p < 0.001).
 |
Table 3 Pulmonary Function Test Among Three Groups |
 |
Table 4 Results of GEE Multiple Linear Regression in Comparing the Treatment Effects Among Three Groups |
Transcriptomic Signature of Healthy Subjects, Asthmatic Patients Treated with ICS with LABA, and ICS with LABA Plus Omalizumab
To investigate the effect of drug treatments on transcriptomics, we used the RNA-seq method to identify the differentially expressed genes (DEGs) among the three groups. The principal component analysis (PCA) revealed that the three groups were clustered differently (Supplementary Figure 1). Further analysis showed that there were 145 DEGs (fold change ≥ 2, FDR <0.05) between healthy subjects and ICS with LABA groups, 63 DEGs between healthy subjects and ICS with LABA plus omalizumab groups, and 281 DEGs between ICS with LABA and ICS with LABA plus omalizumab treatment groups (Figure 1).
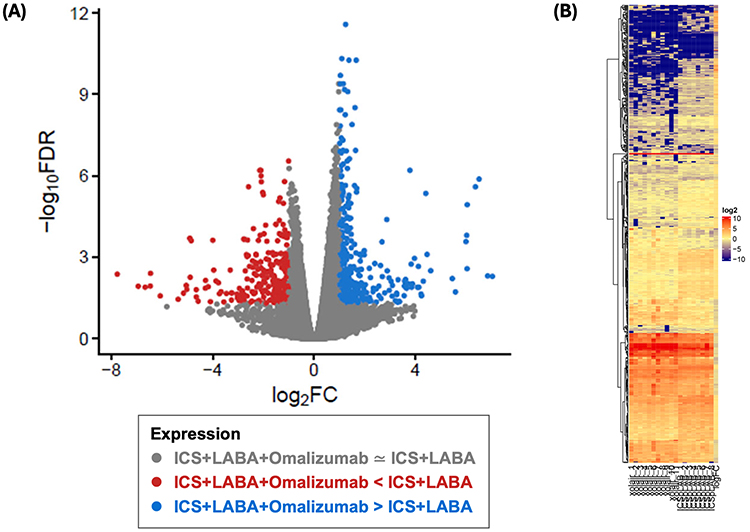 |
Figure 1 Comparison of global gene expression between asthmatic patients treated with ICS with LABA plus omalizumab and those treated with ICS with LABA. For RNA sequencing analysis, the expression levels of differentially expressed genes (DEGs) are visualized using a volcano plot (A) and a clustering heatmap (B). In the heatmap, red indicates upregulated genes, and blue indicates downregulated genes, while yellow (in the heatmap) and grey (in the volcano plot) represent genes with no significant difference. Abbreviations: DEG, differentially expressed gene; ICS, inhaled corticosteroids; LABA, long-acting beta-agonists; FC, fold change; FDR, false discovery rate; GO, gene ontology; RNA, ribonucleic acid. |
We further investigated the different RNA expressions and pathways between patients with asthma that were treated with ICS with LABA and ICS with LABA plus omalizumab. The KEGG pathways or the enriched categories of GO functional annotation and pathway for down-regulated genes in ICS with LABA plus omalizumab group compared to ICS with LABA groups included immune system process/ innate immune response (eg CAMP, DEFA4, IFITM1, LTF, USP18, ISG15, RPL39, OAS1, OAS2, IFI6, RSAD2, HERC5, LCN2, and CXCL10), nucleotide-binding oligomerization domain (NOD)-like receptor signaling pathway (eg DEFA4, OAS1, OAS2, and CAMP), retinoic acid-inducible gene I (RIG-I) like receptor signaling pathway (eg CXCL10 and ISG15), IL-17 signaling pathway (eg CXCL10 and LCN2), and Haptoglobin binding/ oxygen carrier activity/ antioxidant activity (eg MPO and HBA2) (Figure 2 and Supplementary Table 1).
 |
Figure 2 Enrichment analysis for downregulated DEGs in asthma patients post-Omalizumab treatment compared to those treated with ICS with LABA. Gene set enrichment analysis of DEGs identified significantly enriched KEGG pathways (A), Biological Process (B) Molecular Function (C), and Cellular component (D) pathway. (fold change ≥ 2; false discovery rate < 0.05) in ICS with LABA plus omalizumab group compared with ICS with LABA group. Abbreviations: DEG, differentially expressed gene; KEGG, Kyoto Encyclopedia of Genes and Genomes; ICS, inhaled corticosteroids; LABA, long-acting beta-agonists; FDR, false discovery rate; N. of genes, number of genes. |
The enrichment analysis of up-regulated DGEs was also performed in Group 2 treated patients compared to those treated with Group 1. According to KEGG and GO classifications, we found that the targeted genes were significantly enriched in cGMP-PKG signaling pathway (eg MYH6, MYH7, NPPA, and PLN), cardiomyopathy and cardiac failure (including Dilated cardiomyopathy, Hypertrophic cardiomyopathy, Cardiac muscle contraction, and Adrenergic signaling in cardiomyocytes; eg MYH6, MYH7, MYL3, CACNG8, ACTC1, TNNT2, and CACNB2), heart contraction/striated muscle contraction/ cardiac muscle contraction (eg Microfilament motor activity and Cytoskeletal protein binding (eg MYH7, TNNT2, ACTC1, and MYH6), Voltage-gated calcium/cation/ion channel activity (eg CACNG8, CACNA1H, CACNB2, and TSPOAP1), Voltage-gated calcium channel activity involved in regulation of cytosolic/presynaptic calcium levels (eg TSPOAP1 and CACNB2) (Figure 3 and Supplementary Table 2).
 |
Figure 3 The KEGG and GO enrichment analysis for upregulated DEGs in post-Omalizumab treatment asthma patients compared to those treated with ICS with LABA. The KEGG (A) and GO enrichment analyses of DEGs, and the result of the biological process (B), molecular function (C), and cellular component (D)-associated GO terms. (fold change ≥ 1.5, FDR < 0.05) in transcriptome analysis that the different expression levels of genes between ICS with LABA plus omalizumab group compared with ICS with LABA group. Abbreviations: KEGG, Kyoto Encyclopedia of Genes and Genomes; GO, Gene Ontology; DEG, differentially expressed gene; HC, healthy controls; ICS, inhaled corticosteroids; LABA, long-acting beta-agonists; FDR, false discovery rate; N. of genes, number of genes. |
Discussion
This study presents important and novel findings regarding transcriptional expressions and clinical outcomes for patients on ICS with LABA and those with adding omalizumab. Transcriptomic analysis revealed a downregulation of immune and inflammatory response pathways, including the NOD-like receptor signaling pathway, RIG-I-like receptor signaling pathway, IL-17 signaling pathway, and haptoglobin binding/oxygen carrier activity/antioxidant activity in patients with ICS with LABA plus omalizumab. In contrast, there was an upregulation of the cGMP-PKG signaling pathway, cardiac-related and ion channel activity genes in the ICS with LABA plus omalizumab group. For clinical outcomes, patients treated with ICS with LABA plus omalizumab exhibited still higher IgE levels, greater dust mite sensitivity, and more dynamic airway changes post-bronchodilator.
Elevated CXCL10 levels are found in approximately 50% of patients with severe asthma and correlate with poor asthma control.11 CXCL10 can be secreted by various cell types, including airway epithelial cells, smooth muscle cells, monocytes, and macrophages. High expression of the CXCL10 gene is linked to a mast cell signature.11 The CXCL10 axis is central to persistent type 1 inflammation, which may be enhanced by corticosteroid therapy through cooperation between the glucocorticoid receptor (GR) and Signal Transducer and Activator of Transcription 1 (STAT1) at the CXCL10 promoter.11 Therefore, CXCL10 its association with mast cell markers in the airways of severe asthmatics.11 A previous study found that responders to omalizumab had significantly higher baseline CXCL10 than non-responders.12 Elevated CXCL10 levels may serve as a predictive marker for a positive response to omalizumab in asthmatic patients and could be more effective than IL-5 or IgE in predicting clinical response.12 In the current study, we further found that omalizumab downregulated the gene expression of CXCL10. The reduction of CXCL10 mRNA expression suggests decreased chemokine signaling in allergic asthma.
The NOD-like receptor (NLR) signaling pathway, which was also downregulated in the ICS with LABA plus omalizumab group, includes genes such as DEFA4 and OAS1/OAS2. This pathway is essential for the activation of innate immunity through inflammasomes, playing a significant role in inflammation associated with respiratory diseases.13 Lung epithelial cells express various recognition receptors, including NLRs, C-type lectin receptors, RIG-I-like receptors, protease-activated receptors, and purinergic receptors, all of which respond to cytokines derived from epithelial cells and contribute to asthma.14 Previous studies have indicated that NLRs, as a family of innate immune sensors, and their downstream signaling pathways are critical in regulating asthma development.15 Additionally, RIG-I inflammasome activation has been associated with the onset, exacerbation, and progression of viral asthma.16 In the current study, omalizumab may help control excessive inflammation triggered by reducing NLR pathway activation.
Dysregulation of IL-17 has been associated with asthma, as evidenced by genetic analyses,17,18 clinical studies,19,20 and murine models.21–23 IL-17 is known to induce the differentiation of IgE-secreting cells and promoting IgE production.24 This pathway is frequently linked to severe asthma phenotypes. The downregulation of these genes may contribute to the alleviation of airway inflammation, particularly in patients with an IL-17-driven asthma endotype, who often exhibit a suboptimal response to standard ICS treatments. In the current study, we noted the downregulation of the IL-17 signaling pathway, including genes such as CXCL10 and LCN2, in the omalizumab group. While research on the impact of omalizumab on IL-17 levels in asthma is limited, previous studies have indicated that treatment with omalizumab can reduce IL-17 secretion in patients with allergic urticaria.25
Haptoglobin has been implicated in the modulation of the Th1/Th2 response and plays a role in both innate and adaptive immune responses.26 It has been reported that patients with asthma have elevated haptoglobin levels.26 Myeloperoxidase (MPO), an enzyme released from the primary azurophilic granules of neutrophils.27 MPO and human beta-defensin 2 (HBA2) are associated with oxidative stress and inflammation in the lungs.28 Previous studies show increased MPO levels in sputum or blood in severe asthma in both children and adults.29,30 The reduced expression of these genes may indicate a decrease in inflammation and oxidative burden, which is beneficial for asthma management, as oxidative stress often exacerbates airway inflammation and damage.
The current study observed an upregulation of the cGMP-PKG signaling pathway in patients treated with omalizumab, while no previous research specifically investigating the relationship between omalizumab and this pathway. However, one prior study has suggested that the cGMP-PKG signaling pathway plays a role in the pathogenesis of allergic asthma.31 Omalizumab has been shown to reduce airway hyperresponsiveness (AHR) in patients with asthma.32 Our results, however, seem to be inconsistent with these findings. It is important to note that previous studies investigating the reduction of AHR with omalizumab typically compared pre- and post-treatment within the same patient group.32 In contrast, our study compares AHR between different groups. Omalizumab was administered to patients with poor asthma control despite ICS and LABA treatment, suggesting possible more severe inflammation in these patients. Although ACT scores were similar in both groups after treatment, the omalizumab group still exhibited poorer lung function and more dynamic airway changes. Thus, despite similar clinical symptoms, the increased cGMP-PKG expression, poor lung function and more dynamic airway changes in the omalizumab group may suggest ongoing cGMP-PKG-related inflammation. These findings highlight the need for further research about the role of cGMP-PKG-related inflammation in asthma.
Gene expression related to cardiomyopathy and cardiac failure was elevated in patients receiving ICS with LABA plus omalizumab. A previous study showed that serum IgE and FcεR1 expression levels were significantly increased in patients with heart failure.33 FcεR1, expressed in cardiomyocytes, mediates IgE-induced cardiac remodeling and cardiomyocyte hypertrophy.33 Additionally, a case report documented mid-apical akinesia and basal hyperkinesia after the 11th administration of omalizumab.34 An observational study found a higher incidence of cardiovascular and cerebrovascular events in omalizumab-treated patients,35 and the Food and Drug Administration reported a slightly elevated risk of such events.36 Based on our findings and existing literature, we recommend evaluating cardiac function in asthmatic patients with elevated IgE levels or those receiving omalizumab treatment.
This study is the first to report that upregulated genes involved in voltage-gated calcium/cation/ion channel activity in patients treated omalizumab. Voltage-gated calcium channel activity regulates muscle contraction, neuronal signaling, and cellular excitability by controlling calcium transport and levels.37 Vascular smooth muscle and endothelial cells collaborate to regulate blood pressure, with ion channels in these cells controlling membrane potential.37 Elevated calcium influx increases arterial tone, and sustained high arterial tone can lead to cardiac remodeling and dysfunction over time.37 Persistent increases in calcium influx also lead to myocardial fibrosis, arrhythmogenicity, and conduction abnormalities.38 Additionally, calcium channels in cardiomyocytes are associated with left ventricular hypertrophy in response to pressure overload.39 The upregulation of these genes by omalizumab could be linked to the observed cardiovascular effects.34–36 However, the mechanisms behind omalizumab’s upregulation of these genes are not yet fully understood.
Clinical Implication
This study was the first study to highlight transcriptional differences on asthma treatments by comparing patients on ICS with LABA therapy alone with those requiring omalizumab as an add-on. Transcriptomic analysis revealed a downregulation of immune and inflammatory pathways in the ICS with LABA plus omalizumab group, suggesting that omalizumab may help mitigate excessive inflammatory responses. These results underscore Omalizumab’s potential as a targeted anti-inflammatory option for asthma patients who do not achieve sufficient control with ICS with LABA alone, which could lead to better management of severe asthma cases.
Study Limitations
While our research highlights many novel and significant aspects of asthma, it also has several limitations. The first limitation of this study is its relatively small sample size, which may limit the generalizability of the findings to the broader population of patients with asthma. A larger sample size would provide more robust data and allow for better extrapolation of the results to diverse patient groups. Additionally, a small sample size may increase the risk of Type II errors, potentially leading to underestimating the effects or associations observed in the study. However, despite this limitation, the study still provides novel findings about the transcriptional differences between patients receiving ICS with LABA and those receiving ICS with LABA plus omalizumab, contributing valuable insights to the field. Additionally, while transcriptomic analysis provides insights into gene expression changes, it does not capture functional protein-level alterations, which may influence the observed effects. Future studies with larger cohorts are needed to confirm these findings and evaluate the durability of the therapeutic benefits observed.
Conclusions
The current study highlights the potential benefit of adding omalizumab to ICS with LABA therapy in asthma patients who do not achieve sufficient control with ICS with LABA alone. The observed downregulation of immune and inflammatory pathways in patients on ICS with LABA and omalizumab suggests a potential influence on anti-inflammatory effects, which may contribute to a more targeted therapeutic approach for severe allergic asthma. These findings support the role of omalizumab as an effective add-on therapy for improving asthma management. However, upregulated gene expression related to cardiomyopathy should be approached with caution due to potential cardiovascular effects.
Data Sharing Statement
The data underlying the findings of this study can be obtained from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Taipei Tzu Chi Hospital [IRB number 10-XD-154]. ClinicalTrials.gov has approved the study, and the registration number is NCT06869382. The study was conducted in accordance with the Declaration of Helsinki. Informed consent was obtained from all participants or their legal guardians before participation. All research activities followed the ethical guidelines and regulations set by the institution.
Informed Consent
Informed consent was obtained from all participants.
Acknowledgments
The study was conducted at the core laboratory of the Department of Research at Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, located in New Taipei City, Taiwan.
Funding
This study was funded by Taipei Tzu Chi Hospital and the Buddhist Tzu Chi Medical Foundation under grant number TCRD-TPE-109-59 and TCRD-TPE-109-60.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kirenga BJ, de Jong C, Katagira W, et al. Prevalence and factors associated with asthma among adolescents and adults in Uganda: a general population based survey. BMC Public Health. 2019;19(1):227. doi:10.1186/s12889-019-6562-2
2. Infante AF, Wells C, Loza J, Hobbs K, Jarrett JB, Elmes AT. Be SMART about asthma management: single maintenance and reliever therapy. J Am Board Fam Med. 2024;37(4):745–752. doi:10.3122/jabfm.2023.230456R1
3. Chen F, Liang L, Chu FF, Lu C, Xu C. Effects of omalizumab combined with budesonide formoterol on clinical efficacy, pulmonary function, immune function, and adverse reactions in children with moderate and severe allergic asthma. Allergol Immunopathol. 2023;51(4):182–188. doi:10.15586/aei.v51i4.926
4. Yin H, Duo H, Li S, et al. Unlocking biological insights from differentially expressed genes: concepts, methods, and future perspectives. J Adv Res. 2024;
5. Liang YR, Tzeng IS, Hsieh PC, et al. Transcriptome analysis in patients with asthma after inhaled combination therapy with long-acting β2-agonists and corticosteroids. Int J Med Sci. 2022;19(12):1770–1778. doi:10.7150/ijms.76013
6. Wang E, Wechsler ME, Tran TN, et al. Characterization of severe asthma worldwide: data from the international severe asthma registry. Chest. 2020;157(4):790–804. doi:10.1016/j.chest.2019.10.053
7. Soong W, Yoo B, Pazwash H, Holweg CTJ, Casale TB. Omalizumab response in patients with asthma by number and type of allergen. Ann Allergy Asthma Immunol. 2021;127(2):223–231. doi:10.1016/j.anai.2021.04.002
8. Culver BH, Graham BL, Coates AL, et al. Recommendations for a standardized pulmonary function report. An official American thoracic society technical statement. Am J Respir Crit Care Med. 2017;196(11):1463–1472. doi:10.1164/rccm.201710-1981ST
9. Patel N. An update on COPD prevention, diagnosis, and management: the 2024 GOLD report. Nurse Pract. 2024;49(6):29–36. doi:10.1097/01.NPR.0000000000000180
10. Peng B, Sun L, Shang Y, et al. Translation and validation of the Chinese version of patient-completed asthma knowledge questionnaire and its implementation in patient education. J Thorac Dis. 2022;14(4):905–918. doi:10.21037/jtd-21-1604
11. Gauthier M, Chakraborty K, Oriss TB, et al. Severe asthma in humans and mouse model suggests a CXCL10 signature underlies corticosteroid-resistant Th1 bias. JCI Insight. 2017;2(13):e94580. doi:10.1172/jci.insight.94580
12. Akenroye A, Nopsopon T, Hacker JJ, Laidlaw TM. Ratio of plasma IL-13/TNF- ∝ and CXCL10/CCL17 predicts mepolizumab and omalizumab response in asthma better than eosinophil count or immunoglobulin E level. Sci Rep. 2024;14(1):10404. doi:10.1038/s41598-024-60864-3
13. Hsieh PC, Wu YK, Yang MC, Su WL, Kuo CY, Lan CC. Deciphering the role of damage-associated molecular patterns and inflammatory responses in acute lung injury. Life Sci. 2022;305:120782. doi:10.1016/j.lfs.2022.120782
14. Hammad H, Lambrecht BN. The basic immunology of asthma. Cell. 2021;184(6):1469–1485. doi:10.1016/j.cell.2021.02.016
15. Alvarez-Simon D, Ait Yahia S, de Nadai P, et al. NOD-like receptors in asthma. Front Immunol. 2022;13:928886. doi:10.3389/fimmu.2022.928886
16. Radzikowska U, Eljaszewicz A, Tan G, et al. Rhinovirus-induced epithelial RIG-I inflammasome suppresses antiviral immunity and promotes inflammation in asthma and COVID-19. Nat Commun. 2023;14(1):2329. doi:10.1038/s41467-023-37470-4
17. Du J, Han JC, Zhang YJ, et al. Single-nucleotide polymorphisms of IL-17 gene are associated with asthma susceptibility in an Asian population. Med Sci Monit. 2016;22:780–787. doi:10.12659/MSM.895494
18. Kawaguchi M, Takahashi D, Hizawa N, et al. IL-17F sequence variant (His161Arg) is associated with protection against asthma and antagonizes wild-type IL-17F activity. J Allergy Clin Immunol. 2006;117(4):795–801. doi:10.1016/j.jaci.2005.12.1346
19. Molet S, Hamid Q, Davoine F, et al. IL-17 is increased in asthmatic airways and induces human bronchial fibroblasts to produce cytokines. J Allergy Clin Immunol. 2001;108(3):430–438. doi:10.1067/mai.2001.117929
20. Al-Ramli W, Préfontaine D, Chouiali F, et al. T(H)17-associated cytokines (IL-17A and IL-17F) in severe asthma. J Allergy Clin Immunol. 2009;123(5):1185–1187. doi:10.1016/j.jaci.2009.02.024
21. Chesné J, Braza F, Chadeuf G, et al. Prime role of IL-17A in neutrophilia and airway smooth muscle contraction in a house dust mite–induced allergic asthma model. J Allergy Clin Immunol. 2015;135(6):1643–1645.e5. doi:10.1016/j.jaci.2014.12.1872
22. He R, Oyoshi MK, Jin H, Geha RS. Epicutaneous antigen exposure induces a Th17 response that drives airway inflammation after inhalation challenge. Proc Natl Acad Sci. 2007;104(40):15817–15822. doi:10.1073/pnas.0706942104
23. Hynes GM, Hinks TSC. The role of interleukin-17 in asthma: a protective response? ERJ Open Res. 2020;6(2):00364–2019. doi:10.1183/23120541.00364-2019
24. Milovanovic M, Drozdenko G, Weise C, Babina M, Worm M. Interleukin-17A promotes IgE production in human B cells. J Invest Dermatol. 2010;130(11):2621–2628. doi:10.1038/jid.2010.175
25. Hoşgören-Tekin S, Eyüboğlu İP, Akkiprik M, Giménez-Arnau AM, Salman A. Inflammatory cytokine levels and changes during omalizumab treatment in chronic spontaneous urticaria. Arch Dermatol Res. 2024;316(6):261. doi:10.1007/s00403-024-02966-6
26. Abd Al-Aziz AM, Shaaban H, Talaat AA, Awad MAM, Ali R, Walaa A. Assessment of ceruloplasmin, hemopexin, and haptoglobin in asthmatic children. Macedonian J Med Sci. 2020;8(B):31–37.
27. Venge P. Soluble markers of allergic inflammation. Allergy. 1994;49(1):1–8. doi:10.1111/j.1398-9995.1994.tb00765.x
28. Bezerra FS, Lanzetti M, Nesi RT, et al. Oxidative stress and inflammation in acute and chronic lung injuries. Antioxidants. 2023;12(3):548. doi:10.3390/antiox12030548
29. Kim CB, Shim DH, Kim MJ, et al. Increased levels of human myeloperxidase (MPO) and neutrophil lipocalin (HNL/NGAL) in childhood asthma. Eur Respir Soc. 2019.
30. Sze E, Bhalla A, Nair P. Mechanisms and therapeutic strategies for non-T2 asthma. Allergy. 2020;75(2):311–325. doi:10.1111/all.13985
31. Zhang X, Zhang X, Feng S, et al. The specific microRNA profile and functional networks for children with allergic asthma. J Asthma Allergy. 2022;15:1179–1194. doi:10.2147/JAA.S378547
32. Domingo C, Mirapeix RM, González-Barcala FJ, Forné C, García F. Omalizumab in severe asthma: effect on oral corticosteroid exposure and remodeling. A randomized open-label parallel study. Drugs. 2023;83(12):1111–1123. doi:10.1007/s40265-023-01905-5
33. Zhao H, Yang H, Geng C, et al. Role of IgE-FcεR1 in pathological cardiac remodeling and dysfunction. Circulation. 2021;143(10):1014–1030. doi:10.1161/CIRCULATIONAHA.120.047852
34. Aguiar-Ricardo I, Nunes-Ferreira A, Roda Â, Bras-Rosario L. Omalizumab induced Takotsubo syndrome: case report. Eur Heart J Case Rep. 2019;3(1):yty155. doi:10.1093/ehjcr/yty155
35. Iribarren C, Rahmaoui A, Long AA, et al. Cardiovascular and cerebrovascular events among patients receiving omalizumab: results from EXCELS, a prospective cohort study in moderate to severe asthma. J Allergy Clin Immunol. 2017;139(5):1489–1495.e5. doi:10.1016/j.jaci.2016.07.038
36. Oni L, Wright RD, Marks S, Beresford MW, Tullus K. Kidney outcomes for children with lupus nephritis. Pediatr Nephrol. 2021;36(6):1377–1385. doi:10.1007/s00467-020-04686-1
37. Suzuki Y, Giles WR, Zamponi GW, Kondo R, Imaizumi Y, Yamamura H. Ca(2+) signaling in vascular smooth muscle and endothelial cells in blood vessel remodeling: a review. Inflamm Regen. 2024;44(1):50. doi:10.1186/s41232-024-00363-0
38. Zhang X, Ai X, Nakayama H, et al. Persistent increases in Ca(2+) influx through Cav1.2 shortens action potential and causes Ca(2+) overload-induced afterdepolarizations and arrhythmias. Basic Res Cardiol. 2016;111(1):4. doi:10.1007/s00395-015-0523-4
39. Guo Y, Yu ZY, Wu J, et al. The Ca(2+)-activated cation channel TRPM4 is a positive regulator of pressure overload-induced cardiac hypertrophy. Elife. 2021;10:e66582. doi:10.7554/eLife.66582
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Specific IgE Response and Omalizumab Responsiveness in Severe Allergic Asthma
Tajiri T, Suzuki M, Kutsuna T, Nishiyama H, Ito K, Takeda N, Fukumitsu K, Kanemitsu Y, Fukuda S, Umemura T, Ohkubo H, Maeno K, Ito Y, Oguri T, Takemura M, Yoshikawa K, Niimi A
Journal of Asthma and Allergy 2023, 16:149-157
Published Date: 22 January 2023
Characterization of Severe Uncontrolled Asthma in Japan: Analysis of Baseline Data from the PROSPECT Study
Koya T, Asai K, Iwanaga T, Hara Y, Takahashi M, Makita N, Hayashi N, Tashiro N, Tohda Y
Journal of Asthma and Allergy 2023, 16:597-609
Published Date: 2 June 2023
Antitussive Use in Patients with Inadequately Controlled Moderate-to-Severe Asthma: A Post Hoc Analysis of the Omalizumab EXTRA Trial
Rutland CJ, Iweala OI, Anders K, Ko J, Mital P, Gupta S, Mohan A
Journal of Asthma and Allergy 2023, 16:661-665
Published Date: 24 June 2023
Sputum Neurturin Levels in Adult Asthmatic Subjects
Sato S, Suzuki Y, Kikuchi M, Rikimaru M, Saito J, Shibata Y
Journal of Asthma and Allergy 2023, 16:889-901
Published Date: 31 August 2023
Role of the Gut-Lung Microbiome Axis in Airway Inflammation in OVA-Challenged Mice and the Effect of Azithromycin
Zheng J, Huang Y, Zhang L, Liu T, Zou Y, He L, Guo S
Journal of Inflammation Research 2025, 18:2661-2676
Published Date: 21 February 2025