")
Back to Journals » Clinical Ophthalmology » Volume 18
Comparative Clinical Study of Surgical Performance of Quatera 700 versus Centurion and Signature Pro Phacoemulsification Systems
Authors Ganesh S , Brar S , Sriganesh S, Bhavsar HD
Received 9 February 2024
Accepted for publication 15 August 2024
Published 23 September 2024 Volume 2024:18 Pages 2685—2695
DOI https://doi.org/10.2147/OPTH.S456660
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Surgical Performance of Quatera700 Versus Centurion and Signature Pro – Video S3 [456660]
Views: 191
Sri Ganesh, Sheetal Brar, Supriya Sriganesh, Hemali D Bhavsar
Department of Phaco-Refractive Surgery, Nethradhama Super Speciality Eye Hospital, Bengaluru, Karnataka, India
Correspondence: Sheetal Brar, Department of Phaco-Refractive surgery, Nethradhama Superspeciality Eye Hospital, Jayanagar, Bengaluru, Karnataka, India, Tel +919591002092, Email [email protected]
Purpose: To compare the intra-operative surgical performance of Quatera 700 with Centurion and Signature Pro phacoemulsification systems.
Setting: Nethradhama Superspeciality Eye Hospital, Bangalore, India.
Study Design: Prospective, interventional, 3-arm, randomized comparison study.
Methods: A total of 180 non-consecutive eyes satisfying the eligibility criteria were recruited. N = 60 eyes were operated using each of the above systems, of which n = 30 eyes had LOCS III grade 1– 2, and n = 30 eyes had grade 3– 4 nuclear density. Phacoemulsification with foldable IOL implantation was performed by a single experienced surgeon. Chamber stability scores (1– 4, 4 being the worst), fluid turnover per case, surge incidence and intra-operative complications were assessed.
Results: Intra-operatively, the mean chamber stability score was significantly better for the Quatera 700 in both the soft and dense cataract groups compared to the other two machines (p < 0.001). Total Phaco Time (TPT) with Quatera 700 was significantly lower compared to Signature Pro, while it was comparable with Centurion for both the soft and dense cataract groups. The mean fluid turnover was significantly lower for the Quatera 700 in the dense cataract group (p = 0.04) and so was the combined phaco and I/A time (p = 0.01) when compared with Signature Pro. One eye operated with Signature Pro and 2 eyes operated with Centurion had PCR due to surge. The mean corneal clarity scores on POD-1 and specular counts at 2 weeks and 6 months were comparable.
Conclusion: The new Quatera 700 system resulted in lesser TPT, fluid turnover and phaco + I/A time than Signature Pro, while its performance was comparable to Centurion for these parameters. Moreover, the surgeon graded intra-operative chamber stability scoring was highest, when compared to the other two systems.
Ctri Registration Number: CTRI/2022/01/039296.
Keywords: Quatera 700, Quattro pump, phacoemulsification
Introduction
Over the past 50 years, phaco machines have undergone numerous incremental upgrades that have improved the safety and efficacy of cataract surgery. With constant improvements and upgrades, most of the modern phacoemulsification systems available today offer advanced fluidics, IOP control, and excellent anterior chamber stability, resulting in reduced surgical times and lower rates of intra-operative complications. These advantages help in translating into better postoperative outcomes and patient satisfaction.
The Centurion (Alcon Surgicals, Fort Worth, TX, USA), introduced in 2013, combines multiple intelligent phaco technologies and other key features including the Active Fluidics, Balanced Energy and Applied Integration. Active Fluidics is an automated system that optimizes anterior chamber stability by allowing surgeons to proactively set and maintain a target IOP during cataract removal.1–3 Balanced Energy enhances phaco efficiency through OZil Intelligent Phaco (IP) and the Intrepid Balanced tip probe. Occlusion surge is touted to be minimal because of programming and the 150µm ABS opening drilled into the phaco tip, due to which total occlusion never occurs.4–7
The WhiteStar Signature Pro (Johnson and Johnson Vision, North Jacksonville, FL) system, on the other hand, offers proactive IOP management with automatic occlusion sensing. Additionally, it monitors vacuum levels throughout the case, optimizes power settings for enhanced control and improved efficiency, anticipates pressure changes and proactively responds to occlusion breaks, and protects the chamber during post-occlusion surge.8,9 It offers on-demand fluidics with peristaltic, venturi or combination pump capabilities. Ultrasound with the Ellips FX handpiece balances power and control.9
In line with these advancements, a new phacoemulsification system “Quatera 700” has been recently developed by Carl Zeiss Meditec, Jena, Germany. The system has a unique ZEISS Patented QUATTRO Pump that operates via four syringe-like membranes that directly control infusion and aspiration. Integrated sensors measure real-time irrigation and aspiration flow, and the pump synchronizes irrigation and aspiration while accounting for incision leakage to maintain the stability of the chamber, independent of vacuum or IOP level.10 The new system also has two other unique features “Power on demand (POD)” and an “Advanced power modulation (APM)”, both essentially aiming at reducing the effective phaco time and total phaco energy used during the surgery. The console is also integrated with the IOL Master 700 and the operating microscope ARTEVO 800 to provide a complete surgical cockpit.
With this background, the present study was conducted to evaluate the performance of the new Quatera 700 phacoemulsification system in terms of intra-operative safety and surgical efficiency and compare the same with Centurion and Signature Pro phacoemulsification systems. The study also compared the efficiency of these machines for emulsifying different grades of cataract by a single experienced phaco surgeon.
Study Design & Methodology
This prospective, randomized, comparative study was approved by the Institutional Ethics Committee of Nethradhama Superspeciality Eye Hospital, Bangalore and was conducted as per the tenets of declaration of Helsinki. Informed consent was obtained from all patients participating in the study. The following criteria were considered for the eligibility of the patients for inclusion in the study.
Inclusion Criteria
Patients of either sex aged between 40–75 years, diagnosed with nuclear or cortico-nuclear cataract of grade I–IV according to the Lens Opacity Classification System III (LOCS III)11 scale, suitable to undergo phacoemulsification with foldable Intraocular Lens (IOL) implantation within an IOL power range of +16 to +24 D and willing and able to sign a written informed consent document were recruited.
Exclusion Criteria
LOCS-III Nuclear sclerosis grade 4+, mature and intumescent, morgagnian, posterior polar, uveitic cataracts, traumatic and subluxated cataracts, poorly dilating pupils, corneal ectatic diseases, corneal scars, corneal degenerations, endothelial cell counts <2000 cells/mm2, previous intraocular surgery, severe optic nerve and retinal disorders, immunocompromised states or systemic conditions potentially increasing the operative risk or confound the result of the investigation.
Primary end points evaluated were chamber stability at various parameters (AFR, vacuum and IOP), incidence of surge and fluid turnover per case. Secondary end points were total phaco time (TPT), total surgical time (incision to closure), and time taken for phacoemulsification and I/A (starting at the beginning of the phaco to the ending of irrigation and aspiration before IOL implantation), and incidence of intra-operative complications.
A total of 180 non-consecutive eyes (unilateral/bilateral) satisfying the eligibility criteria, with grades of nucleus colour (NC) and nucleus opalescence (NO) LOCS III, were distributed into the following two categories – grade 1–2, and grade 3–4. Eyes were randomized using computer generated random numbers to receive operation with either of the three phaco machines. Thus, the distribution and number of eyes operated in each study group was as follows:
Quatera 700: 60 eyes (n = 30 eyes each of grades 1–2 and 3–4)
Centurion: 60 eyes (n = 30 eyes each of grades 1–2 and 3–4)
Signature Pro: 60 eyes (n = 30 eyes each of grades 1–2 and 3–4)
Pre-operative assessment included visual acuity with ETDRS chart at 4m, slit-lamp examination, dilated fundus examination, intraocular pressure (IOP) recording by non-contact tonometry (NCT), optical biometry using IOL Master 700 (Carl Zeiss Meditec, Jena, Germany), specular microscopy (Tomey, Japan), and macular OCT (Optovue, Fremont, USA).
All surgeries were performed under topical anaesthesia using a 2.2 mm temporal clear corneal approach, following a standard surgical technique.12 All IOLs were implanted under balanced salt solution.
Details of the intra-operative surgical mode, parameters and specifications of the phaco tips used for the three phaco systems in the study are provided in Table 1. At the end of each surgical procedure, total phaco time (min), fluid turnover/case (cc), total surgical time (incision to closure), combined phaco and I/A time (min), chamber stability and incidence of surge were noted. The operating surgeon assessed the chamber stability using a grading system provided in Table 1. Complications such as posterior capsule rupture, zonular dialysis, nucleus or fragment drop, vitreous loss, wound burn etc. were also recorded. For measurement of fluid utilized per case, the priming fluid was first discarded from the drainage bag before the start of each case. Immediately after the surgery, the drainage bag was removed from the consumable assembly, and the aspirate was carefully emptied into a measuring beaker. The upper fluid level was noted by a single observer, who was masked for the phaco machine used.
 |
Table 1 Details of the Intra-Operative Surgical Mode, Parameters and Specifications of the Phaco Tips Used for the Three Phaco Systems and Chamber Stability Grading System Used in the Study |
Post-operative examinations were conducted on 1st day, 2 weeks and 6 months post-op and data was recorded for intraocular pressure (NCT), corneal clarity (using a standard grading system),13 anterior chamber reaction (Sun classification)14 and IOL position on post-op day 1. Uncorrected distance visual acuity (UDVA), corrected distance visual acuity (CDVA), NCT, corneal clarity, anterior chamber reaction, IOL position, CCT and endothelial cell density (ECD) were recorded on future visits.
Statistical Analysis
Data was analyzed for all the surgical parameters evaluated in the study, individually as well as compared between the three cohorts of the patients operated using the three study machines. Statistical analysis was performed using the Data analysis tool pack available in Microsoft Excel. Continuous variables were compared using the t-test and ANOVA or the Mann–Whitney and Kruskal–Wallis tests depending upon the distribution of the data. A p-value of ≤0.05 was considered statistically significant.
Results
A total of 180 non-consecutive eyes from 151 patients were recruited for the study. Table 2 shows the group-wise comparison of the pre-operative demographic data of all the patients who participated in the study. For both the cataract groups, the parameters of age, axial length, anterior chamber depth, steep and flat keratometry and IOL power were comparable, without any significant differences (p > 0.05) for all parameters. Table 3 and 4 demonstrate the comparison of intra-operative parameters of anterior chamber stability scores, total phaco time (TPT), fluid turnover per case, total surgical time, combined phaco and I/A time and intra-operative complications of Quatera 700 versus Signature Pro (Table 3) and Quatera 700 versus Centurion (Table 4).
 |
Table 2 Group-Wise Comparison of the Pre-Operative Demographic Data of All the Patients Who Participated in the Study |
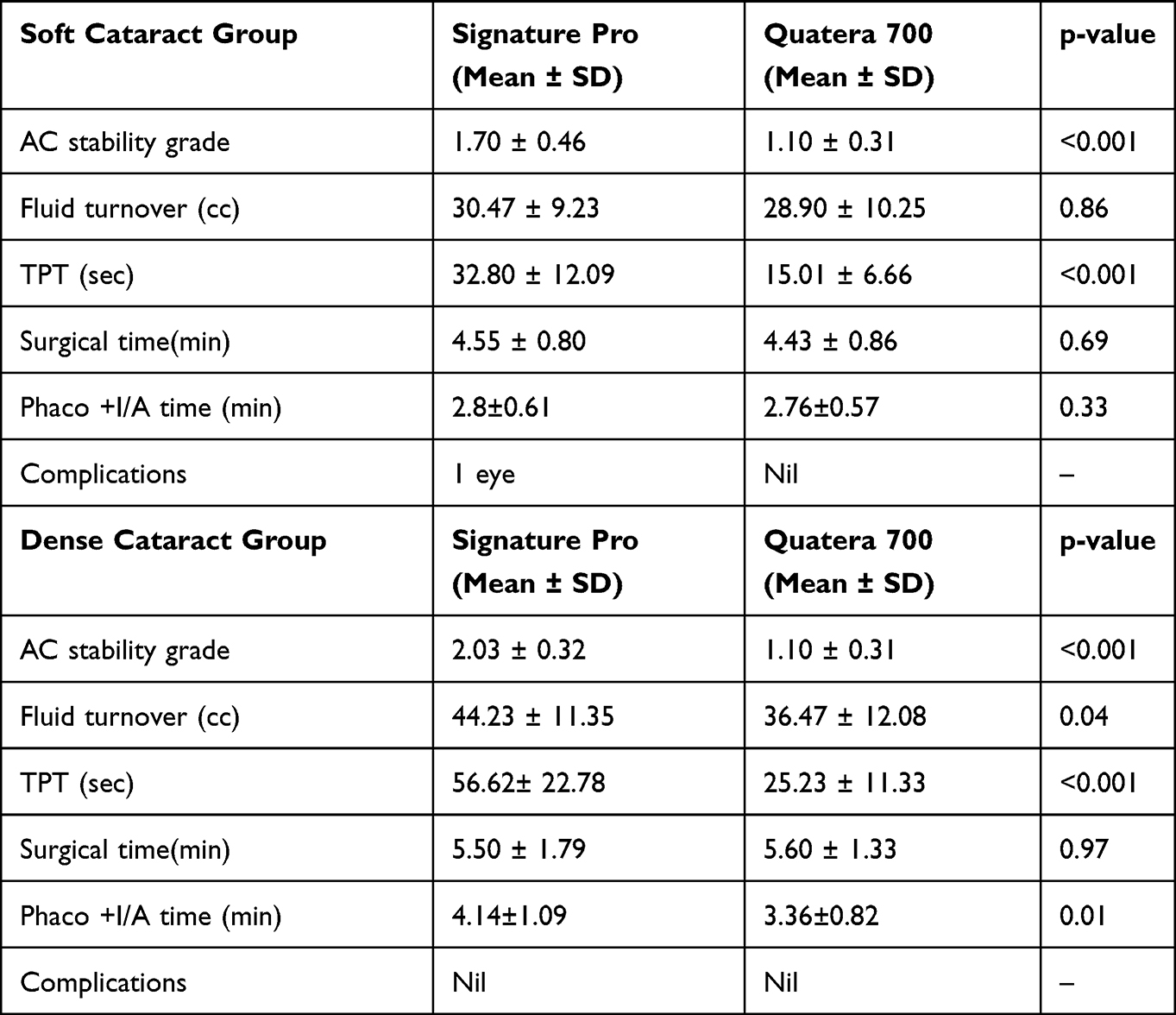 |
Table 3 Comparison of Intra-Operative Anterior Chamber Stability Scores, Total Phaco Time (TPT), Fluid Turnover per Case, Surgical Time, and Complications Between Quatera 700 and Signature Pro Study Groups |
 |
Table 4 Comparison of Intra-Operative Anterior Chamber Stability Scores, Total Phaco Time (TPT), Fluid Turnover per Case, Surgical Time, and Complications Between Quatera 700 and Centurion Study Groups |
Soft Cataract Group (Quatera-700 versus Signature Pro), Table 3
The mean anterior chamber stability grade was significantly better in the Quatera 700 (1.10 ± 0.31), versus the Signature-Pro (1.70 ± 0.31), p < 0.001. The total phaco time (TPT) for the Quatera 700 was 15.01 ± 6.66 sec, which was significantly lower than the Signature Pro (32.80 ± 12.09) sec, p < 0.001. The fluid turnover/case was comparable, with no significant differences between the groups, p = 0.86. Similarly, the total surgical time and the combined phaco and I/A time was comparable between Quatera 700 and Signature Pro machines, p = 0.69 and 0.33, respectively.
Dense Cataract Group (Quatera-700 versus Signature Pro),Table 3
Similar to the soft cataract group, the mean anterior chamber stability score in the dense cataract group also was significantly better for the Quatera 700 (1.10 ± 0.31), compared to the Signature Pro (2.03 ± 0.32), p < 0.001. Likewise, the total phaco time (TPT) was lower in the Quatera-700 (25.23 ± 11.33 sec) versus the Signature Pro (56.62 ± 22.78 sec), the difference being statistically significant, p < 0.001. Regarding the fluid turnover/ case, it was significantly lower for the Quatera 700 group, p = 0.04. The mean surgical time was comparable, with no significant differences noted amongst both the machine groups, p = 0.97. However, the average combined phaco and I/A time was significantly lower for the Quatera 700 (3.36 ± 0.82 min) when compared to the Signature Pro (4.14 ± 1.09), p = 0.01, Table 3.
Soft Cataract Group (Quatera-700 versus Centurion),Table 4
The mean anterior chamber stability grade was significantly better in the Quatera 700 (1.10 ± 0.31), versus the Centurion (2.23 ± 0.50), p < 0.001. However, the total phaco time (TPT) for the Quatera 700 (15.01 ± 6.66 sec) was comparable to that of Centurion (15.36 ± 7.72) sec, p = 0.92. The fluid turnover/case was comparable, with no significant differences between the groups, p = 0.16. Similarly, the total surgical time and the combined phaco and I/A time was comparable between Quatera 700 and Centurion machines, p = 0.45 and 0.77, respectively.
Dense Cataract Group (Quatera-700 versus Centurion),Table 4
Similar to the soft cataract group, the mean anterior chamber stability score in the dense cataract group was significantly better for the Quatera 700 (1.10 ±0.31), compared to the Centurion (2.20 ± 0.55), p < 0.001. The total phaco time (TPT) in the Quatera 700 group was (25.23 ± 11.33 sec) versus the Centurion (31.83 ± 16.82 sec), the difference being statistically insignificant, p = 0.08. Regarding the fluid turnover/ case, it was also comparable for both the groups, p = 0.81. The mean surgical time, as well as the average combined phaco and I/A time was comparable too, with no significant differences noted amongst both the machine groups, p = 0.92 (mean surgical time), and p = 0.12 (phaco + I/A time).
Intra-op Complications
In the soft cataract group, one eye each operated with the Signature Pro and Centurion machines, had posterior capsule rupture (PCR), due to inadvertent surge noted intra-operatively. On the other hand, one eye in the dense cataract group, operated with the Centurion system had PCR, again attributed to sudden intra-operative surge. No eye in the Quatera 700 system encountered PCR due to inadvertent chamber shallowing.
Post-Operative Outcomes
The mean corneal clarity scores on post-operative day 1 showed clearer corneas in the eyes operated with the Quatera 700 for both the cataract groups, with the average score being least (better) compared to the other two machines. However, the difference was not statistically significant, p = 0.87 for soft cataract and 0.36 for the dense cataract group, Figure 1. The anterior chamber inflammation score was also comparable and not significantly different between the three groups of phaco machines for both grades of cataracts, p-value = 1, Figure 2.
 |
Figure 1 Mean corneal clarity scores on post-operative day 1, for eyes operated with the three machines in the study. |
 |
Figure 2 Anterior chamber inflammation scores on post-operative day 1, for eyes operated with the three machines in the study. |
Two weeks post-operatively, the mean values of IOP, CCT, endothelial cell density, UDVA and CDVA were comparable across the three machines, for both the soft and dense cataract groups, without any significant differences between the 3 machines, p > 0.05, (Table 5).
 |
Table 5 Comparison of Post-Operative IOP, CCT, Endothelial Cell Density, UDVA and CDVA Across the Three Machines Groups |
The % ECD loss at 6 months post-op, compared to pre-op in the soft cataract group was 11.9%, 11.4% and 10.8% for the Signature Pro, Centurion and Quatera 700 study groups, respectively, without any significant differences, p-value = 0.72. In the dense cataract group, these values were 14.5%, 14.6% and 14.1% for the Signature Pro, Centurion and Quatera 700 study groups respectively, again, with no significant differences between groups, p-value = 0.95, Supplemental file 1. Similar to 2 weeks outcome, the UDVA and CDVA, was not significantly different between the 3 machines across both the varieties of cataract grades, (Table 5).
Discussion
One of the observations which was consistent across both the soft and hard cataract groups was a significantly better anterior chamber stability score, as graded by the surgeon with Quatera 700, when compared to the Centurion and Signature-Pro machines. Even though it was a subjective grading, however, it may be considered valid, as the operating surgeon is a highly skilled phaco surgeon who has performed over 100,000 phaco surgeries using different phaco systems, and thus is experienced enough to detect minor variations in the chamber stability.
This may be attributed to the patented Quattro pump incorporated in the Quatera 700 system, which is a synchronized fluid exchange system that directly measures and simultaneously controls both infusion and aspiration volumes in real-time. It also actively compensates for incision leakage volume.15 Supplementary Video 1, shows surgical video of an eye operated using the Quatera 700 system demonstrating excellent chamber stability, especially during the final stages of phacoemulsification. Note that the pupillary margin is stable, with minimal fluctuations. On the other hand, eyes operated with Signature Pro and Centurion systems show visible fluctuations of the pupillary margin during the phacoemulsification of the last fragment, Supplementary Video 2, & Supplementary Video 3, respectively. This may also have potentially translated into better intra-operative safety in this group, as no eye operated with the Quatera 700 encountered any significant capsule-related complications such as posterior capsule rupture due to post occlusion surge or chamber shallowing.
In a study by Sharif-Kashani et al, who compared and quantified occlusion break surge of different phacoemulsification systems at vacuum pressures between 200 and 600 mmHg, the authors observed that occlusion break surge increased with increasing aspiration vacuum for all phacoemulsification systems, with the largest surge areas observed at 600 mmHg, the surge areas being: WhiteStar Signature, 4.8 ± 0.45 mmHg∙second; Infiniti, 4.1 ± 0.37 mmHg∙second; Centurion Active Fluidics, 1.3 ± 0.15 mmHg∙second; and Centurion gravity fluidics, 1.4 ± 0.12 mmHg∙second. Thus, across the aspiration vacuum pressure range tested, White star Signature had the highest surge followed by Infiniti, while Centurion produced substantially less occlusion break surge with both the gravity and Active Fluidics settings.16 Even at the highest pre-set aspiration vacuum level (600 mmHg) and lowest Active Fluidics irrigation fluid pressure (IOP target 40 mmHg, equivalent to 54 cm H2O), Centurion achieved decreased surge area compared with the gravity fluidics of Infiniti and WhiteStar Signature at 90 cm H2O. This was likely due to the lower-compliance fluidics of Centurion compared with the other systems tested.16 This may explain better chamber stability observed with Centurion compared to the Signature Pro, observed in the study. However, at each pre-set aspiration vacuum pressure tested, occlusion break surge area with Centurion Active Fluidics predictably increased with decreasing target IOP settings. At 600 mmHg, the surge areas were 1.3 ± 0.1, 2.1 ± 0.37, 2.7 ± 0.21 and 3.6 ± 0.37 mmHg.sec with target IOPs of 65, 55, 50 and 40 mmHg, respectively. In the present study, the surgeon used a vacuum setting of 700mm Hg and a relatively low and physiological target IOP of 40 mmHg with the Centurion system, which may explain the two cases of posterior capsule ruptures due to possible occlusion breaks, as evident from the observations of the above study.
Recent study by Fanney et al, evaluated and compared peak surge and surge duration time after occlusion break, incision leakage compensation, and passive vacuum for Quatera 700 and Centurion phacoemulsification systems in an experimental study, in which Quatera 700 demonstrated slightly higher surge peak values and notably shorter surge duration times after occlusion break than Centurion.17 Quatera 700 also demonstrated better incision leakage compensation and lower passive vacuum than Centurion, suggesting good safety and chamber maintenance, even at higher parameters, thus supporting findings of our study.
The Advanced Power Modulation (APM™) is an ultrasound modulation that combines the burst and the pulse patterns in each modulation cycle, thus aiding in chopping techniques by impaling the nucleus with the power of the burst and removing the quadrants with the speed of the pulse.18–20 The use of APM, along with relatively higher settings of vacuum used in the vacuum mode of the machine, may have resulted in comparatively less total phaco time, TPT (time spent in foot pedal position 3) with the Quatera 700 system due to faster and more efficient chopping and emulsification of the nucleus achieved compared to the Signature Pro. Moreover, it was possible to emulsify the entire nucleus using nil or minimal phaco energy in some cases of softer grades of cataracts, using only the high vacuum settings with the Quatera 700. The TPT, however, was comparable with Centurion, probably due to the favourable effects of the torsional phacoemulsification available with this machine.
EPT or effective phaco time parameter was not evaluated in the present study between the 3 machine groups. This is because a direct reading of EPT was not available on the graphic user interface of Centurion machine at the end of the case. Even though, effective phaco time (EPT) can be considered as the product of phaco time multiplied by the average phaco power,21 the manual calculation of the same may result in conflicting results due to the differences in the basic modes of ultrasound delivery utilized by the 3 machines. The Quatera 700 uses the longitudinal phaco, while the WhiteStar Signature-Pro Ellipse FX system is based on a combination of longitudinal and transversal phaco.7,22 On the other hand, the Centurion system utilizes the torsional mode phacoemulsification with the OZil® Intelligent Phaco software that produces side-to-side rotary oscillations of the phaco tip, along with longitudinal ultrasound pulses which are activated at certain pre-set vacuum % levels during occlusion/pre-occlusion.23,24 Apart from the differences in the modes of ultrasound delivery, the three machines also differ in their ultrasound frequencies, potentially affecting the EPT.25,26 In general, the metrics of ultrasound phaco emulsification such as percentage phaco power, EPT, CDE (Cumulative Dissipated Energy) etc., remain proprietary and unique to each machine, and manufacturers may use different algorithms to calculate these parameters. Hence, direct comparison among different machines remains fraught with difficulty. However, with regard to the total phaco time (TPT), Quatera 700 was comparable to the Centurion for both soft and dense grades, and significantly better than the Signature Pro. This may be due to the higher parameters used in the Quatera-700 group which were well supported by the Quattro pump, and allowed for faster emulsification of the nucleus fragments potentially reducing the wastage of energy required to attract the fragments to the tip.
In terms of the average fluid turnover/case, Quatera 700 group showed the lower fluid consumption compared to the Signature Pro in the dense cataract group, which may be due to the comparatively less combined phaco and I/A time observed in Quatera-700 compared to the other two machine groups. The use of vacuum mode27,28 with a high vacuum setting of 700 mm Hg, along with a flared tip29 would result in better holdability and faster chopping of the nuclear fragments, thus reducing the time taken for phacoemulsification and thus the aspirate.
The mean endothelial cell loss at 6 months when compared to pre-op and post-op visual outcomes were no different amongst the three study groups, showing that all the three systems had similar endothelial safety and resulted in satisfactory clinical outcomes. No significant differences between torsional and conventional mode phacoemulsification were observed for post-op endothelial cell loss, as suggested by previously publishes studies.30,31
In conclusion, the new Quatera 700 phaco system resulted in superior intra-operative chamber stability, lowest total phaco time and better safety compared to the Centurion and Signature Pro systems across both the soft and dense cataract grades, suggesting the potential benefit of the patented Quattro pump; thus enhancing the intra-operative safety and efficiency. More data and future comparative studies with different machines are suggested to verify these preliminary results. Also, longer follow-ups are required to evaluate the long-term effects of the new system on endothelial cell density compared to other systems.
Data Sharing Statement
The complete patient data Excel sheet of the recruited subjects can be made available by requesting Dr. Chandan Latha, ethics committee in charge Nethradhama Superspeciality Eye Hospital, Bangalore. She can be accessed at [email protected]
Disclosure
Dr. Sri Ganesh, Dr. Sheetal Brar and Dr. Supriya Sriganesh are consultants to Carl Zeiss Meditec. The study was investigator-led and was supported by Carl Zeiss Meditec. company. The authors report no other conflicts of interest in this work.
References
1. Aravena C, Dyk DW, Thorne A, Fanney D, Miller KM. Aqueous volume loss associated with occlusion break surge in phacoemulsifiers from 4 different manufacturers. J Cataract Refract Surg. 44(7):884–888.
2. Jirásková N, Stepanov A. Our experience with active sentry and centurion ozil handpieces. Cesk Slov Oftalmol, 77 1 18–21 doi: 10.31348/2021/1.
3. Dasgupta S, Mehra R. Comparative studies between longitudinal and torsional modes in phacoemulsification, using active fluidics technology along with the intrepid balanced tip. Indian J Ophtha. 2018;66(10):1417. doi:10.4103/ijo.IJO_7_18
4. Sun YX, Cao R, Liu ZY, et al. Comparisons of the energy efficiency and intraocular safety of two torsional phacoemulsification tips. BMC Ophtha. 2022;22(1):1–8. doi:10.1186/s12886-021-02233-6
5. Sabur H, Eroglu SA, Azarsiz SS. Efficacy of balanced torsional phacoemulsification tip for cataract surgery. J Curr Ophtha. 2022;34(1):74. doi:10.4103/joco.joco_105_21
6. Demircan S, Ataş M, Göktaş E, Başkan B. Comparison of 45-degree Kelman and 45-degree balanced phaco tip designs in torsional microcoaxial phacoemulsification. Int J Ophthalmol. 8(6):1168–1172. doi:10.3980/j.issn.2222-3959.2015.06.16.
7. Tognetto D, Cecchini P, Leon P, Di Nicola M, Ravalico G. Stroke dynamics and frequency of 3 phacoemulsification machines. J Cataract Refract Surg. 38(2):333–342.
8. Tognetto D, D’Aloisio R, Cecchini P, Di Nicola M, Di Martino G. Comparative clinical study of Whitestar Signature phacoemulsification system with standard and Ellips FX handpieces. Intl Ophthalmol. 2018;38(4):1697–1702. doi:10.1007/s10792-017-0649-5
9. Kim YN, Lee JA, Kim JY, Kim MJ, Tchah HW. Clinical Effects of an Improved Pump Reaction Rate and Automatic Occlusion Sensing System in Phacoemulsification. J Korean Ophthalmol Soc. 59(11):1017–1023.
10. https://www.zeiss.com/meditec/en/products/phaco-vitrectomy-lensfragmentation/zeiss-quatera-700.html.
11. LT C, Wolfe JK, Singer DM, et al. The Lens Opacities Classification System III. The Longitudinal Study of Cataract Study Group. Arch Ophthalmol. 1993;111(6):831–836. doi:10.1001/archopht.1993.01090060119035.
12. Ganesh S, Brar S, Rp N, Rathod D. Clinical Outcomes, Contrast Sensitivity, Reading Performance and Patient Satisfaction Following Bilateral Implantation of AT LARA 829MP EDoF IOLs. Clin Ophthalmol. 15:4247–4257. doi: 10.2147/OPTH.S331860.
13. Strauss G, Newsom RB, Surka J. Corneal grading system for post-operative assessment of manual small incision cataract surgery (MSICS. South Afr Ophthalmol J. 2020;15(2):1.
14. Jabs DA, Nussenblatt RB, Rosenbaum JT; Standardization of Uveitis Nomenclature (SUN) Working Group. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol. 2005;140(3):509–516. doi:10.1016/j.ajo.2005.03.057.
15. Quatera white paper.
16. Sharif-Kashani P, Fanney D, Injev V, Richard G, Druchkiv V, Steinberg J. Comparison of occlusion break responses and vacuum rise times of phacoemulsification systems. BMC Ophtha. 2014;14(1):1–7. doi:10.1186/1471-2415-14-1
17. Fanney D, Layser GS, AR K, Kübler C, Seibel BS, Seibel BS. Experimental study comparing 2 different phacoemulsification systems with intraocular pressure control during steady-state flow and occlusion break surge events. J Cataract Refract Surg. 49(9):976–981. doi: 10.1097/j.jcrs.0000000000001242.
18. Talal A New phaco technology minimizing the effective phaco time: the VISALIS 500 Family APM™ ultrasound modulation. White Paper, 2013.
19. Körber N A new concept of faster and more balanced cataract surgery: the VISALIS 500 Family APM™ ultrasound modulation. White Paper, 2013.
20. Prasad N Phaco efficiency of a new ultrasound modulation APM™ (advanced power modulation) in hard nuclei. White Paper, 2014.
21. Alió JL, Soria F, Abdou AA, Peña-García P, Fernández-Buenaga R, Javaloy J. Comparative outcomes of bimanual MICS and 2.2-mm coaxial phacoemulsification assisted by femtosecond technology. J Refract Surg. 2014;30(1):34–40. doi:10.3928/1081597X-20131217-04.
22. Assil KK, Harris L, Cecka J. Transverse vs torsional ultrasound: prospective randomized contralaterally controlled study comparing two phacoemulsification-system handpieces. Clin Ophthalmol. 9:1405–1411. doi: 10.2147/OPTH.S86660.
23. Leon P, Umari I, Mangogna A, Zanei A, Tognetto D. An evaluation of intraoperative and postoperative outcomes of torsional mode versus longitudinal ultrasound mode phacoemulsification: a meta-analysis. Interna J Ophtha. 2016;9(6):890. doi:10.18240/ijo.2016.06.18
24. Salman SH, Mourad MS, ElGhazawy RM, Rihan RA. Comparative study of conventional versus torsional phacoemulsification in management of hard nucleus. J Egypt Ophthalmol Soc. 114(1):1.
25. Dewan T, Malik PK, Tomar P. Comparison of effective phacoemulsification time and corneal endothelial cell loss using three different ultrasound frequencies: a randomized controlled trial. Indian J Ophthalmol. 2022;70(4):1180–1185. doi:10.4103/ijo.IJO_2163_21.
26. Pacifico RL. Ultrasonic energy in phacoemulsification: mechanical cutting and cavitation. J Cataract Refract Surg. 1994;20(3):338–341. doi:10.1016/s0886-3350(13)80587-1.
27. Patrício MS, Almeida AC, Rodrigues MP, Guedes ME, Ferreira TB. Correlation between cataract grading by Scheimpflug imaging and phaco time in phacoemulsification using peristaltic and venturi pumps. European J Ophtha. 2013;23(6):789–792. doi:10.5301/ejo.5000293
28. Hida WT, de Medeiros AL, de Araújo Rolim AG, et al. Prospective randomized comparative study between venturi and peristaltic pumps in WhiteStar Signature® phacoemulsification machine. Clinical Ophthalm. 2019;13:49.
29. McNeill JI. Flared phacoemulsification tips to decrease ultrasound time and energy in cataract surgery. J Cataract Refract Surg. 2001;27(9):1433–1436. doi:10.1016/s0886-3350(01)00789-1.
30. Reuschel A, Bogatsch H, Barth T, Wiedemann R. Comparison of endothelial changes and power settings between torsional and longitudinal phacoemulsification. J Cata Ref Surg. 2010;36(11):1855–1861. doi:10.1016/j.jcrs.2010.06.060
31. Kim D-H, Wee W-R, Lee J-H, Kim M-K. The comparison between torsional and conventional mode phacoemulsification in moderate and hard cataracts. Korean J Ophtha. 2010;24(6):336–340. doi:10.3341/kjo.2010.24.6.336
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.