")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 17
Comparative Cost Analysis for Direct Medical Costs of Protocol Administration of Non-Small Cell Lung Cancer Treatment Regimens in Curative Intent: A Micro-Costing Study in Jordan
Authors Madae'en SS , Salem AA, Ararawi NS, Ramzi EJ, Aloueedat RF, Saabenh AM, Allouzi DA, Abuoudeh RH, Hnaif OE, Musa LM, Alshdaifat SH, Al-Tanashat AJ, Almasa'afeh HY, Abuallaban SM
Received 30 January 2025
Accepted for publication 20 June 2025
Published 12 July 2025 Volume 2025:17 Pages 455—471
DOI https://doi.org/10.2147/CEOR.S520119
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Samer Hamidi
Saba S Madae’en,1 Ahmed A Salem,2 Naila S Ararawi,3 Ezaldeen J Ramzi,3 Roa’a F Aloueedat,3 Abdullah M Saabenh,3 Diala A Allouzi,3 Reem H Abuoudeh,3 Osama E Hnaif,3 Leen M Musa,3 Salma H Alshdaifat,3 Ahmad J Al-Tanashat,3 Hala Y Almasa’afeh,3 Salma M Abuallaban3
1Department of Clinical Pharmacy and Pharmacy Practice, Faculty of Pharmaceutical Sciences, The Hashemite University, Zarqa, Jordan; 2Department of Anatomy, Physiology and Biochemistry, Faculty of Medicine, The Hashemite University, Zarqa, Jordan; 3Faculty of Medicine, Hashemite University, Zarqa, Jordan
Correspondence: Saba S Madae’en, Department of Clinical Pharmacy and Pharmacy Practice, Faculty of Pharmaceutical Sciences, the Hashemite University, Zarqa, Jordan, Email [email protected]
Background: Non-small cell lung cancer (NSCLC) treatment costs significantly impact healthcare systems. This study analyzes direct costs and cost drivers of perioperative and adjuvant systemic treatments for stage I–II NSCLC from Jordanian healthcare providers’ perspective using micro-costing methodology.
Methods: We employed micro-costing to analyze direct medical expenses including drug acquisition, preparation, administration, pre/post-medications, diagnostics, labor, and wastage costs for perioperative regimens used in stage I–II NSCLC. International guidelines defined therapeutic regimens, while drug prices were extracted from Jordan Food and Drug Administration’s database. Published data and surveys quantified micro-costs.
Results: Among 26 assessed regimens (2 targeted therapy, 10 chemotherapy, 10 chemo-immunotherapy, 4 immunotherapy), targeted/immunotherapy agents significantly increased costs. Chemotherapy regimen cost differences ranged from $633.68 (squamous) to $1,763.91 (non-squamous) per cycle. Antineoplastic agents were primary cost drivers, highest for Durvalumab (98.72% of cycle cost). Laboratory costs comprised up to 50.73% in chemotherapy and 7.24% in immunotherapy regimens. Wastage contributed up to 10.36% of total cycle costs. Average administration cost was $35 per cycle. Maximum cycle costs were: targeted therapy (Osimertinib) $7,206.44, immunotherapy (Durvalumab) $9,057.71, immune-chemotherapy (Durvalumab-Carboplatin-Pemetrexed) $11,358.43, and chemotherapy (Carboplatin-Pemetrexed) $2,300.72.
Conclusion: Our results highlight the substantial economic impact and cost variability among treatment regimens. This variability presents opportunities for cost reduction through careful selection of therapeutically equivalent regimens based on pricing and toxicity profiles. The findings emphasize the need for comprehensive and precise cost analysis to inform healthcare policies and clinical practices. Future research should focus on cost-effectiveness analyses of these expensive agents to ensure value for money, support evidence-based decision-making, and strengthen price negotiations with suppliers.
Keywords: chemotherapy, targeted therapy, immunotherapy, cost analysis, non-small cell lung cancer, sensitivity analysis, direct medical cost, administration cost, wastage cost
Introduction
Lung cancer is the leading cause of cancer-related death globally, ranking first among men and second among women.1 Individuals with advanced stages at presentation have a significantly lower survival rate. The projected average five-year survival rate is acceptable for early-stage disease but poor for locally advanced and metastatic disease, with significant geographical differences.2 Non-small cell lung cancer (NSCLC) accounts for around 85% of all lung cancer cases. Curative therapies, such as surgery, radiation therapy, or chemotherapy, are commonly utilized in the management of stage I–II NSCLC.3 Beside the relatively high mortality rate, lung cancer has a great financial and economic impact on employers, insurance companies, governments, patients and their families, and the community, particularly in developing nations.4
In Jordan, the incidence rate of lung cancer has significantly increased, with 650 new cases reported in 2022 compared to 371 new cases in 2012.5 This increase places a significant strain on oncology services. Treatment for NSCLC has evolved with a high use of targeted and immune treatments, resulting in improving survival outcomes and low toxicity.6 However, this has also led to a dramatic rise in the cost of these treatments, rising concern worldwide regarding the accessibility and affordability of these treatments, particularly in low- and middle-income countries.7
Early-stage NSCLC constitutes 12.35% of overall lung cancer cases in Jordan.8 Understanding the financial implications of evidence-based decisions for treating early-stage NSCLC is critical as healthcare systems face resource constraints. Like many other countries throughout the world, Jordan has seen an increase in the financial burden connected with lung cancer. The key causes for this increase in Jordan are an increase in cancer incidence and the rising cost of cutting-edge lung cancer therapies and technology.9 This is especially true for lung cancer, as the need for advanced diagnostic equipment and new targeted and immunotherapy agents drastically burdens both public and private healthcare resources,10 which necessitates the conduct of cost-effectiveness studies grounded in comprehensive cost analysis.
Chemo-, immuno-, and targeted therapy are used perioperatively in curative-intent early-stage NSCLC. In patients who are not candidates for immunotherapy, chemotherapy is used basically as an adjuvant or neoadjuvant therapy, while immunotherapy can be used in combination with chemotherapy as neoadjuvant therapy or as a single therapy adjuvant in patients who are candidates for immunotherapy. Targeted therapy can be used as adjuvant treatment in selected NSCLC patients with driver mutations. Immunotherapy and targeted therapy in early-stage NSCLC improved patients’ survival.11,12 For example, a study on Osimertinib, a third-generation EGFR inhibitor, found that it significantly prolonged disease-free survival and overall survival rates in adults with stage IB-IIIA NSCLC compared to placebo in the pivotal ADAURA trial when used as adjuvant therapy.13,14 Another study conducted by Forde et al defined the role of a Nivolumab-chemotherapy combination regimen in comparison to chemotherapy alone in the neoadjuvant setting in early-stage NSCLC. Median event-free survival improved from 20.8 months with chemotherapy alone to 31.6 months with Nivolumab, and the pathological complete response improved from 2.2% to 24%.15 These results, among others, emphasize the importance of studying the cost-effectiveness of these novel agents, as their elevated expenses present a considerable burden, particularly in resource-limited settings such as Jordan. These studies are needed to guarantee that these treatments deliver value for money and warrant the necessity for sustainable healthcare solutions.
Treatment costs for NSCLC can vary significantly depending on several factors, including the cost of the drug regimen. Standard cytotoxic chemotherapy is generally less expensive than immunotherapy and targeted medications. There is a paucity of research on micro-costing in the Middle East and North Africa region (MENA); none of the studies that specifically address the cost analysis of lung cancer therapy have been conducted in Jordan. Understanding these costs is critical for healthcare providers to make evidence-based decisions, particularly in resource-constrained settings. Many hidden costs are not taken into consideration when choosing protocols for reimbursement and procurement and even bargaining the price with supplier. We aimed to conduct a comprehensive micro-costing analysis to assess and compare the direct costs and key cost drivers related to perioperative regimens that are used to manage early-stage NSCLC from the perspective of the Jordanian healthcare providers. We were able to capture the cost components of administration, treatment, labs, investigations, and waste using this method, which allowed us to break down costs at a granular level in compliance with international treatment protocols.
Methods and Materials
We collected data on the direct medical expenses related to the acquisition, preparation, and administration of preoperative and adjuvant regimens employed in stage I–II NSCLC from NCCN and NHS guidelines (based on tertiary cancer centres in the UK).16–18 Due to the absence of a standardized national NSCLC treatment protocol in Jordan, and given that local protocols generally align with international guidelines, we opted to follow NCCN and UK NHS protocols. This choice ensures consistency with global clinical practice and aligns with local tertiary center practices. We utilized a micro-costing approach from Jordanian healthcare provider’s viewpoint. This required enumerating and pricing each input used in the treatment of a certain patient.19
We calculated the cycle cost of the selected regimens used in neoadjuvant and adjuvant settings in patients stage I–II NSCLC. We divided cycle costs into six main categories. (1) targeted, immuno- and chemotherapy agents’ costs; (2) pre- and post-medication costs; (3) preparation and administration costs (4) laboratory test costs; (5) monitoring radiological diagnostic and lab test costs and (6) waste costs. Adverse events management costs and indirect costs were excluded from this analysis. We followed aforementioned guidelines for administration and doses, radiological diagnostics and lab tests. In July 2024, we collected the prices for each drug from the Jordan Food and Drug Agency’s drug pricing database, found in Supplementary Table 1, with the Jordan Dinar serving as the wholesale purchasing cost.20 All costs were converted at the average 2024 currency rate of JD 1.0 = US$ 1.41.21 This study adhered to the Consolidated Health Economic Evaluation Reporting (CHEERS) Standards guideline for economic evaluations in 2022.22 Because we used publicly available data and this study is not classified as human participation research under the Declaration of Helsinki no informed consent was required. This study was conducted under the umbrella of an approved study by the institutional Review Board in Hashemite University (2400486).
Drug Regimens
The selection of the regimens followed the latest guidelines from NCCN (version:6.2024) and a tertiary NHS cancer center in the UK.17,18 They were classified as adjuvant and neoadjuvant regimens. Table 1 shows the employed regimens, doses per cycle, number of cycles, and the cost components for each regimen.
 |
Table 1 Direct Medical Cost Components per Cycle for Perioperative NSCLC Treatment Regimens |
Drug Costs
The protocol established the targeted, immuno-and chemotherapy regimen, pre- and post-medications, doses, frequency, duration, and number of cycles. We employed either the average male body surface area of 1.7 m2 (70 kg), mg/kg, AUC 5, or the fixed dose specified in the protocol. We determined the cost of targeted, immuno-, and chemotherapy drugs, as well as pre- and post-medications for each regimen in the treatment protocol, using the JFDA wholesale price in 2024.20 We computed the cost of one dose by using the average price of the best-fitting vials on the market, as local clinical practice would choose the best combination of available vial sizes to meet the required dose. To reduce potential waste, we carefully selected the best-fitting available vials, considering all vial sizes accessible for purchase in Jordan. For the sensitivity analysis, we used the highest and lowest market prices to compute drug cycle costs within those ranges. When there was only one drug brand available, we utilized the price as the base, lower, and upper values.
Lab and Diagnostic Test Costs
We used the aforementioned protocol from tertiary NHS cancer center in the UK to specify all laboratory, diagnostic, and monitoring tests, including CT, chest X-rays (CXR), or ECG, used for monitoring. We priced all items based on a university hospital price list (King Abdullah University Hospital).23 The private sector prices are used for upper and lower values when applicable.24
Wastage Costs
In our study, the baseline scenario implies a certain level of waste, as the vials are not reused once opened. We evaluated the cost of drug waste by calculating the milligram difference between the best available vial size combination on the market and the required dose for each patient, as specified in the aforementioned protocol. We then multiplied the net wastage in mg by the cost per mg.
Cost of Drug Administration
The drug administration cost estimates include venipuncture, preparation, administration, and monitoring of antineoplastic agent’s infusion in an outpatient clinic. We consulted oncology pharmacists from Jordan University Hospital and Jordanian Royal Medical Services and agreed on the time required for preparation, and dispensing of various regimens, as well as the time required by nursing personnel to monitor patients every hour. Physician fees were included. Overhead costs were not included as the employed method calculates the direct medical cost for administration protocol. The cost of the IV set infusion equipment used in the session was provided by Jordan University Hospital on July,2024.25 The IV set infusion comprises a cannula and IV start kit (antiseptic wipes, gauze, and plaster), excluding the cost of pump usage.
Labor Costs
Nursing and pharmacy time was calculated by multiplying the time spent on drug preparation, dispensing, drug administration, and monitoring by the nurse or pharmacist’s hourly compensation. The average salaries for nurses and pharmacists were derived from Hammad et al’s study, which incorporated financial records from across different Jordan’s healthcare sectors, Health Professional Association, and Jordan civil service bureau. Their methodology included gathering staff salary data directly from HR departments with employee validation, providing dependable baseline costs for healthcare professionals in Jordan, adjusted for inflation rate.26
Physician Fees
We calculated specialist physician fees using the published average wage for physicians.26 We considered the average number of beds or chairs used in oncology clinics from two tertiary institutions (JUH and JRMS). We calculated the total fees by multiplying the average interval for each regimen by the hourly physician fees.
Total Cost
Total cost was computed by adding targeted-, immuno-chemotherapy drug, pre-post medicines, labs, monitoring tests, and drug administration charges per cycle, as per protocol. The aforementioned protocols outline the number of cycles and the treatment intervals for adjuvant targeting and immunotherapy administration. The following equations formula were utilized:


Statistical and Sensitivity Analyses
Data were analysed using Microsoft Excel (Version 2024).27 Statistical measures included medians and ranges for cost components. Cost variations were expressed as percentages of base case values. In our sensitivity analysis, we evaluated the impact of price fluctuations on overall cycle costs across different perioperative regimens to provide comprehensive cost implications. Total cycle cost was calculated across a range of likely values derived from upper and lower market pricing values for all cost components. The disparity between the upper and lower ranges was calculated as a percentage to assess the cost variation in the market by subtracting the lower value from the upper value, dividing the result by the lower value, and multiplying by 100.
Results
Cost analysis of 26 perioperative systemic therapy regimens for stage I–II NSCLC in Jordan revealed substantial cost variations. These differences were notable between patients eligible for immune checkpoint inhibitors/targeted therapy versus those who were not, as well as among therapeutically equivalent or near-equivalent chemotherapy regimens. Among patients who are not candidates for immune check point inhibitors/targeted therapies, Cisplatin-Pemetrexed had the highest median cycle cost ($2,191.94) for non-squamous histology, while Cisplatin-Etoposide had the lowest cycle cost ($428.03). For squamous histology, the median cycle cost of Cisplatin-Gemcitabine ($551.35) was 9.82% lower than the Cisplatin-Docetaxel ($605.52). For other recommended regimens, Pemetrexed-Carboplatin showed the highest median cycle cost ($2300.72), while Carboplatin-Gemcitabine (AUC5/1250 mg) had the lowest ($582.22). Among therapeutically equivalent or near-equivalent chemotherapy regimens, the cost differential representing the gap between highest and lowest per-cycle regimen costs, was $633.68 for squamous carcinoma and $1,763.91 for non-squamous carcinoma.
Immunotherapy carries the highest cycle cost among the available treatment options. For instance, Durvalumab had the highest median cycle cost ($9,057.71), followed by Pembrolizumab ($8,512.32). For oral targeted therapy, Osimertinib had the highest cycle cost ($7,206.44), followed by Alectinib ($5,955.54). Combination regimens further increased costs, with Durvalumab-Carboplatin-Pemetrexed regimen reaching $11,358.43 per cycle and Durvalumab-Cisplatin-Pemetrexed at $11,249.65. Adding immunotherapy to chemotherapy regimens significantly increased costs. For example, combining Durvalumab with Cisplatin-Gemcitabine raised the cycle cost from $551.35 to $9,609.06 (a 17.4-fold increase). Similarly, adding Pembrolizumab to the Cisplatin-Gemcitabine regimen increased costs from $551.35 to $9,063.67 (a 16.4-fold increase). It is noteworthy that adding immunotherapy to Pemetrexed-containing regimens, while still resulting in dramatic cost increases, showed lower fold-increases compared to non-Pemetrexed regimens, due to the already high inherent cost of Pemetrexed. Adding Nivolumab to Cisplatin-Pemetrexed increased the cycle cost from $2,191.94 to $8,767.05, representing a 4-fold increase. Similarly, combining Durvalumab with Carboplatin-Pemetrexed raised the cycle cost from $2,300.72 to $11,358.43, a 4.9-fold increase. These substantial multipliers highlight the significant financial impact of adding immunotherapy to chemotherapy backbones, even when the base regimens already carry relatively high costs.
Moreover, adding Nivolumab to standard chemotherapy regimens also substantially increased costs. The Cisplatin-Gemcitabine-Nivolumab regimen cost $8,767.05 per cycle compared to $551.35 for Cisplatin-Gemcitabine alone (a 15.9-fold increase). The Cisplatin-Pemetrexed-Nivolumab regimen’s cycle price increased from $2,191.94 to $8,767.05 (a 4-fold increase). When comparing immunotherapy agents, Durvalumab substantially increased costs compared to Nivolumab when added to the same chemotherapy backbone, with differences ranging from 1.3-fold to 1.4-fold. For example, Cisplatin-Pemetrexed-Durvalumab costs $11,249.65 while Cisplatin-Pemetrexed-Nivolumab regimen’s cycle price is $8,767.05.
The primary cost driver across regimens was the expense of antineoplastic agents. Targeted and immunotherapy drugs account for the highest percentage of the overall cycle cost, with Durvalumab accounting for 98.72% and Osimertinib accounting for 97.10%. These agents incur significantly lower costs for other cycle components compared to chemotherapy regimens. For instance, in the case of Alectinib, pre- and post-drugs, labs, diagnostics, and administration costs comprise only 3.56% ($211.97) of the overall cycle cost ($5,955.54). In contrast, for the chemotherapy regimen of Cisplatin-Etoposide, the chemotherapy cost constitutes only 19.76% ($84.6) of the total cycle cost ($428.03). Chemotherapy costs in other regimens range from 38.99% in Gemcitabine-Carboplatin($582.22) to 75.93% in Carboplatin-Pemetrexed ($2,300.72)of the total cycle cost. In combined immuno-chemotherapy regimens, costs range from 87.38% in Cisplatin-Gemcitabine-Nivolumab($7,130.94) to 96.05% in Durvalumab-Cisplatin-Gemcitabine ($9,609.06). This emphasizes the necessity of considering costs alongside treatment effectiveness when evaluating these agents, as they have significant financial implications for all healthcare stakeholders.
Laboratory test costs were the second-largest cost contributor, ranging from $73.32 to $390.57 per cycle for targeted and immunotherapy regimens and accounting for up to 7.24% of the total cycle cost. Among the chemotherapy regimens, The Etoposide-Cisplatin regimen incurred the highest lab test cost ($217.14), accounting for 50.73% of its overall cycle cost ($428.03). On the other hand, the Cisplatin-Vinorelbine regimen (cycles 2 and 3) incurred the lowest lab cost per cycle ($71.91), indicating a significant decrease from the first cycle’s lab test cost of $169.2. Incorporating immunotherapy into a chemotherapy regimen significantly increases laboratory test costs. For instance, adding Pembrolizumab to a Cisplatin-Pemetrexed regimen increases them from $128.31 to $518.88 (a 4-fold increase), while adding Durvalumab to Cisplatin-Gemcitabine increases them from $104.34 to $ 201.63 (a 1.9-fold increase). This, however, only accounts for 2.1% and 5.46% of the total cycle cost, respectively. The high total cycle cost for both regimens explains this. The other regimens required laboratory tests that cost between $104.34 and $217.14, as shown in Table 1.
Due to common adverse events associated with chemotherapy agents’ administration, the pre- and post-drug costs per cycle form the highest percentage of total cycle costs, whereas targeted and immunotherapy treatments have significantly lower pre- and post-drug costs. The highest pre- and post-medication cost per cycle was $159.33 for the Cisplatin-Vinorelbine regimen (cycle 1)($921.06) and $94.18 for the Cisplatin-Etoposide regimen($428.03), while this cost comprised between 2 and 22% of the total cycle cost for the other regimens. On the other hand, targeted and immunotherapy had the lowest pre- and post-drugs costs per cycle owing to a reduced incidence of adverse events linked to their administration, primarily attributable to the steroids drugs that used for rash management. Alectinib, Osimertinib, and Pembrolizumab had the lowest costs ($1.41), followed by Atezolizumab ($2.82). The remaining regimens range between these values, as observed in Table 1.
The cost of radiological diagnostic and monitoring tests, such as chest x-rays and CT scans, for many of the regimens ranged from $105.75 to $121.26, constituting up to 20.92% of the overall cycle cost for certain regimens. Table 1 displays the radiological diagnostic costs for these regimens. In terms of drug administration costs, they range from 0.01 to 24.84% of the overall cycle cost assuming patients do not require hospitalization. The number of days within each cycle led to the highest cost of Cisplatin-Vinorelbine cycle 1 ($228.75) as it is administered for 8 consecutive days in cycle1, while Osimertinib and Alectinib, which are targeted oral agents, incurred the lowest costs at $1.88, attributed solely to dispensing costs. The other regimens had generally low administration costs ranging from $10 to $52.
Notably, the expenditures for several regimens fluctuated from cycle to cycle, with the first cycle incurring the highest cost. The highest difference, 74.87%, was for the Cisplatin-Vinorelbine regimen between cycles one and two as the number of days and doses of this regimen vary from the first cycle to the subsequent cycles. The Cisplatin-Docetaxel regimen showed price fluctuations in different percentages between cycles, with cycles two and three showing a 37% decrease from the base case cycle cost and cycle four showing a 23% decrease in cost. That cost reduction is attributable to lab tests cost. Some regimens showed marginal reduction in the cycle’s costs, such as Pemetrexed-Carboplatin and Durvalumab-Gemcitabine-Pemetrexed, with a cost decrease of 5.7% for either, while Atezolizumab showed a cost decrease of 5.2%. Furthermore, other regimens using Nivolumab alongside chemotherapy demonstrated relative cost reductions of 1–2.5%. On the other hand, other regimens, like Cisplatin-Gemcitabine and Carboplatin-Paclitaxel, exhibited more consistent pricing. Table 2 demonstrates the difference between the first and subsequent cycle costs.
 |
Table 2 Comparative Analysis of Cycle Costs for Perioperative NSCLC Treatment Regimens (USD) |
Drug waste contributed significantly to costs in certain chemo- and immunotherapy-containing regimens. Nivolumab incurred the highest wastage costs at $452.61 per cycle (7% of total cycle cost), while other immunotherapies (Pembrolizumab, Atezolizumab, and Durvalumab) and oral-targeted therapies (Osimertinib and Alectinib) showed no wastage. Among chemotherapy regimens, Carboplatin-Pemetrexed and Cisplatin-Pemetrexed had the highest wastage costs at $238.29 (10.4% of total cycle cost) and $225.60 (10.3% of total cycle cost), respectively. Adding Nivolumab to chemotherapy regimens further increased wastage costs—for example, the Pemetrexed-Cisplatin-Nivolumab regimen had wastage costs of $678.21 (7.5% of total cycle cost), representing a 201% increase in wastage costs compared to the chemotherapy regimen alone ($225.60). Even the regimens with minimal wastage still contribute to overall costs. For example, Carboplatin-Paclitaxel had a comparatively small wastage cost of $36.27, representing 1.2% of its $881.25 overall cycle cost, yet this still amounts to a meaningful expense when calculated across multiple treatment cycles and patients. These waste cost estimates are conservative, based on average BSA calculations, and may underrepresent actual clinical practice. Table 1 presents the waste expense in US dollars per cycle, while Figure 1 shows the percentage of waste cost relative to total cycle cost for each regimen.
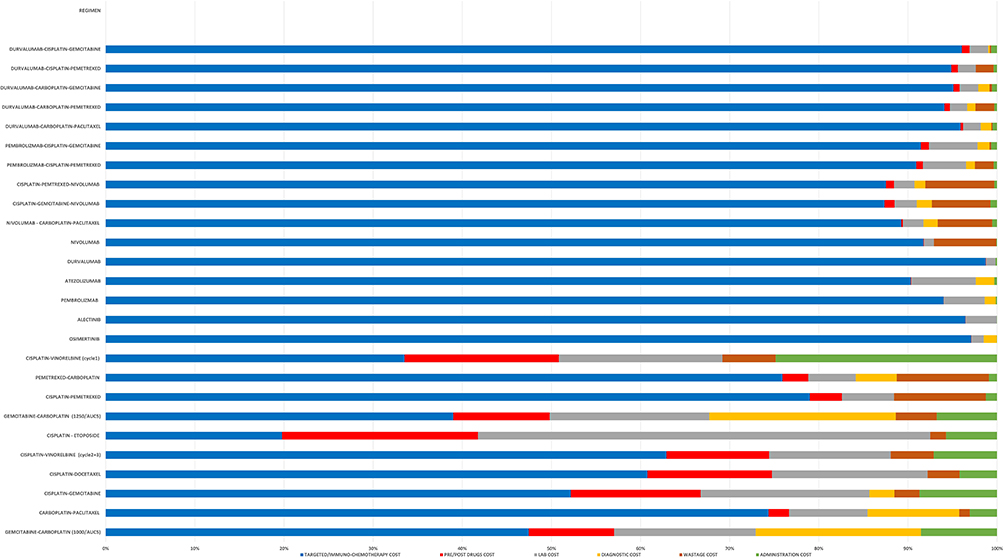 |
Figure 1 Percentage Distribution of Cycle Cost Components for Perioperative NSCLC Treatment Regimens. |
In Table 2 out of the 26 regimens assessed, 2 include targeted therapy, 10 consist of chemotherapy, 10 combine chemotherapy with immunotherapy, and 4 consist entirely of immunotherapy. The total cost per protocol for various treatment regimens varies significantly, with targeted therapies exhibiting the highest costs. In the adjuvant setting for a duration of up to three years, the cost of Osimertinib is $259,431.84, whereas Alectinib costs $142,932.96 for a two-year period. The annual cost per protocol for adjuvant systemic therapy in patients eligible for immune checkpoint inhibitors is $144,709.44 when utilizing Pembrolizumab, while the expense for 13 cycles of Nivolumab amounts to $84,212.44; furthermore, Durvalumab incurs a cost of $108,692.52 for the same duration. Adding Durvalumab to Carboplatin-Gemcitabine resulted in the lowest cost among other platinum-doublet regimens ($38,452.41), whereas its combination with Carboplatin-Pemetrexed incurred a total cost of $45,078.88. Overall, total perioperative costs per protocol for Durvalumab maintenance combined with platinum-doublet regimens range from $147,144.93 to $153,771.40. These costs highlight the financial burden associated with different treatment protocols, emphasizing the need for cost-effective strategies in cancer treatment. Finally, the total cost per chemotherapy protocol aligned closely with the cost per cycle, with the Cisplatin-Etoposide regimen being the least expensive at $856.06 and the Pemetrexed-Carboplatin regimen having the highest cost at $8,809.46.
Analysis of the Jordanian Cancer Registry data from 2022 identified 650 lung cancer patients, with NSCLC accounting for 553 cases (85%). Of these NSCLC cases, 68 patients (12.35%) were diagnosed in early stages.8 Molecular profiling data indicates that 14.7% of early-stage patients possess EGFR mutations that qualify them for targeted therapy. PD-L1 expression analysis shows that 20–30% of early-stage patients express high levels (≥50%), making them eligible for immunotherapy, while an additional 10–20% with lower PD-L1 expression levels may also qualify for treatment. Taking into account a 5–10% overlap between targeted therapy and immunotherapy eligible populations, approximately 45–65% of early-stage NSCLC patients in Jordan are candidates for either immunotherapy or targeted therapy.28,29 An estimated 69% of NSCLC patients receive at least one recommended course of chemotherapy. Among these patients, 25–30% have squamous carcinoma, while 70–75% have non-squamous carcinoma.30
Sensitivity Analysis
The low and high cases represent the maximum and minimum prices of all cycle components observed in the market, enabling wide-ranging inferences as presented in Supplementary text 1, while the base case reflects the median cost per cycle for each regimen. Single-brand regimens, such as Osimertinib, Alectinib, Durvalumab, and Atezolizumab, exhibited minimal price variation due to limited market competition. Conversely, regimens such as Gemcitabine-Carboplatin and Carboplatin-Paclitaxel demonstrated substantial cost variability, with Carboplatin-Paclitaxel expenses ranging widely from $473.26 to $1,385.50 per cycle and Gemcitabine-Carboplatin costs fluctuating considerably from $428.99 to $1,139.93, highlighting the extensive variation in potential treatment costs. This wide range of price fluctuations is largely attributed to market competition and vial size availability. These findings underscore the importance of cost predictability in treatment planning, as significant cost variability could adversely impact healthcare budgets and patient affordability. Range estimates of cost components for cancer treatment regimens, including lower and upper bounds for each component for sensitivity analysis, and best case with lower total cost and worst case with highest total cost as well as expressed variation as a percentage from base case are presented in supplementary Table 2.
Discussion
This study presents the first comprehensive micro-costing analysis of 26 perioperative and adjuvant regimens for stage I–II NSCLC in Jordan, addressing a key gap in the absence of previous studies in Jordan and the Middle East. We provided a detailed breakdown of direct medical costs including pharmacist and nursing labor, medication preparation, dispensing, and administration, antineoplastic agents, pre- and post-medications, and laboratory and radiological monitoring. Cost analysis serves as a fundamental part of health economics by identifying, measuring, and valuing healthcare resource utilization. While reliable cost information is essential for economic evaluation, micro-costing stands out as the most precise method for cost estimation.19 This methodology uncovered typically hidden costs often underestimated and revealing notable variations in cost components across different treatment regimens. Our micro-costing analysis revealed antineoplastic drugs as the primary cost driver of total cycle costs, significantly impacting on the overall financial burden of cancer care. The rapid introduction of novel cancer therapies has led to increased healthcare expenditures globally, with cancer drugs accounting for up to 30% of total hospital expenditure in the European Union.31,32 This impact is particularly notable in Jordan, where healthcare expenditure represents 7.29% of GDP, with pharmaceutical costs comprising 24.82% of total healthcare spending.33 Supporting this trend, data from the King Hussein Cancer Center shows pharmacy expenditure increased by 63% between 2005 and 2008, driven by novel cancer therapies.9
Beyond drug acquisition costs, our findings revealed significant additional financial burdens in NSCLC treatment regimens. These treatments require extensive laboratory monitoring, with diagnostic costs comprising up to one-half of total expenses in some chemotherapy and combined regimens, underscoring the need for strategies that optimize resource utilization. Drug wastage emerged as another substantial yet frequently overlooked cost factor in cancer care. While traditional cost evaluations typically presume complete utilization of all prescribed drugs without accounting for wastage,34 our analysis demonstrated that wastage costs constitute a significant portion of total cycle expenses, even when employing careful dose calculations based on average male body surface area and optimal vial size selection. Clinical settings may experience even higher wastage due to patient body surface area variations, limited suitable vial sizes accessibility at specific institution, dose modifications, treatment discontinuations, and toxicity-related adjustments. Although our initial analysis suggested negligible waste for oral targeted therapies, research by Lam et al indicates these medications can incur waste of 1.78% (SD, ±2.21%) of total cycle costs,35 approximating $123 per cycle in our study context. To accurately assess and address this economic impact, healthcare institutions must consider all cost components when assessing new therapeutic options to determine cost drivers and ensure sustainable resource allocation. Furthermore, implementing cost-saving strategies through targeted mitigation approaches in cancer care delivery can significantly reduce expenditures. These strategies include: establishing institutional policies for vial sharing or dose rounding to align with available vial sizes; centralizing drug preparation processes; consolidating administration days for drugs with substantial wastage potential, such as Nivolumab; and systematically collecting real-world data on wastage, particularly for expensive medications. When implemented methodically, these approaches can substantially decrease unnecessary costs while preserving treatment efficacy and quality of care.36
These cost considerations become particularly relevant in the context of emerging therapeutic advances for early-stage NSCLC. The high recurrence rate after surgery, affecting approximately 30% of stage I patients,37 has highlighted the need for improved adjuvant treatment approaches.38 While traditional adjuvant or neoadjuvant chemotherapy only improves 5-year survival by 5–10%,39 newer targeted therapies and immunotherapies have demonstrated significant improvements in survival outcomes, as evidenced by multiple landmark trials.12,15,40–43
However, these therapeutic advances pose significant economic challenges when scaled to a population level. Treatment costs vary substantially, with targeted therapy expenditures ranging from $142,932.96 to $259,431.84 per course, particularly in extended protocols such as 24-month Alectinib and 36-month Osimertinib regimens. When extrapolated to Jordan’s NSCLC population, the financial implications are profound: total expenditure ranges from $1.4 to $2.6 million USD for targeted therapy-eligible patients and $0.6 to $3.7 million USD for immunotherapy candidates. Even conventional chemotherapy carries significant costs, ranging from $26,465-$56,881 for squamous carcinoma to $56,496-$308,331 for non-squamous carcinoma.
Notably, our analysis revealed substantial cost differentials between therapeutically equivalent regimens highlight an opportunity for policymakers and clinicians to implement cost-conscious prescribing practices that could significantly reduce financial burden without compromising treatment efficacy. Moreover, potential cost-saving opportunities through careful selection among therapeutically equivalent or near-equivalent regimens, with cost differentials of $633.68 and $1,763.91 per cycle for squamous and non-squamous carcinoma, respectively. To address these significant economic variations, healthcare systems must adopt comprehensive clinical protocols and policy mechanism to optimize healthcare expenditure. Recommended cost-containment strategies include: standardizing treatment protocols that prioritize cost-effective options where clinical outcomes are comparable; integrating electronic decision support tools that present cost information alongside efficacy data at the point of prescribing; carefully selecting patients for targeted therapies through suitable molecular biomarker testing; implementing value-based pricing models for high-cost drugs, potentially linking payment to clinical outcomes alongside cost-effectiveness analysis.; and developing clear regulatory pathways for biosimilar adoption. These strategies would help Jordan balance access to innovative therapies with healthcare system sustainability while providing powerful evidence for future policy decisions.
This substantial financial burden is particularly concerning given Jordan’s current approach to oncology drug formulary inclusion, which lacks alignment with standard cost-effectiveness analysis practices.44 This misalignment underscores two urgent needs: conducting economic evaluations to ensure value for money and determining mutation prevalence in Jordanian NSCLC patients to accurately estimate treatment-eligible populations. These strategic interventions can help optimize resource allocation while maintaining quality cancer care.
The contextualization of our findings within existing literature presents several methodological challenges. The absence of prior NSCLC treatment cost studies in Jordan, coupled with the lack of comparative micro-costing analyses in other disease areas, restricts direct comparisons. This knowledge gap is particularly pronounced in low- and middle-income countries, especially within the MENA region, where health economic research remains scarce. A global bibliometric analysis by Pitt et al revealed that the MENA region contributed only 2% of health economic evaluations,45 while Zrubka et al’s comprehensive review through 2019 found that merely 5.7% of regional economic evaluations addressed neoplasms, with none examining perioperative NSCLC regimens.46 Meaningful cross-study comparisons are further hindered by heterogeneity in methodological approaches and the absence of standardized guidelines compounded by diversity of healthcare systems and economic classifications. Nevertheless, our findings align with those of Nadeem et al regarding the substantial cost impact of novel therapeutic agents and relative proportional costs of some treatment regimens, despite differences in economic conditions and healthcare structures between study populations.47
The critical importance of such locally relevant cost analyses is underscored by the limitations of existing global cost estimates. While a systematic review reported a global median cancer treatment administration cost of $142 per hour, this figure primarily reflects high-income country data and may not represent costs in diverse healthcare contexts.48 Our analysis addresses this gap by providing Jordan-specific data, revealing an average administration cost of $35.06 per cycle in the outpatient setting - notably excluding indirect costs and equipment expenses, suggesting actual costs may be higher. These findings emphasize the need for comprehensive, context-specific economic evaluations to guide resource allocation and policy decisions in cancer care delivery.
To the best of our knowledge, this study represents the first application of micro-costing methodology to analyze NSCLC treatment costs in Jordan. Our comprehensive analysis of 26 perioperative and adjuvant regimens establishes crucial benchmarks for the country’s healthcare system. The micro-costing approach revealed several important insights: components beyond antineoplastic agents constitute a substantial portion of total cycle costs; significant cost-saving opportunities exist through selection between therapeutically equivalent or near-equivalent regimens; and targeted mitigation strategies for reducing drug wastage and optimizing vial size selection could yield substantial savings and improved immuno-chemotherapy management strategies. These findings are particularly valuable given Jordan’s unique healthcare context, where drug pricing and system structures create distinct cost patterns that differ from global norms.
Several limitations warrant consideration when interpreting our findings. First, while local protocols generally align with international guidelines with minor deviations, we opted for NCCN and UK NHS protocols due to the absence of a standardized national NSCLC treatment protocol in Jordan. This approach ensures consistency with global clinical practice while aligning with local tertiary center practices. We recommend conducting a multi-center validation study to quantify how protocol variations impact overall treatment costs across different Jordanian clinical settings, thereby enhancing the generalizability of our findings within the national healthcare system. Second, our use of publicly available wholesale prices may not reflect real-world costs, excluding potential supplier discounts and pricing variations across healthcare settings. Third, cost extrapolations based on average adult male parameters may not accurately represent the Jordanian cancer patient population. Fourth, our analysis excludes indirect medical and societal costs, as well as expenses associated with managing treatment-related adverse events, which could significantly impact total treatment costs. Further studies that estimate these indirect costs and the economic burden of adverse events would provide a more reliable assessment of the treatment’s overall economic impact.
In conclusion, this micro-costing analysis of stage I–II NSCLC treatment in Jordan reveals significant variations in direct medical costs across 26 perioperative and adjuvant regimens. Our findings highlight antineoplastic drugs as the primary cost driver, particularly in targeted and immunotherapy regimens. The identification of other cost drivers and wastage factors establishes essential benchmarks for comparing the financial burden of different treatment regimens. This suggests that comparing therapeutically equivalent or near-equivalent regimens could help lower costs, along with conducting studies using real-world data to estimate the prevalence of Jordanian patients eligible for targeted or immunotherapies and their clinical outcomes.
Given the scarcity of economic evaluations in low- and middle-income countries, particularly in Jordan, this comparative cost analysis study establishes a crucial foundation for future cost-effectiveness research. While our investigation provides comprehensive cost data, it does not estimate how various regimens might increase life expectancy or quality-adjusted life years (QALYs). Future studies should aim to integrate these cost findings with clinical outcome data to determine the true value of different treatment options. Additional research priorities include patient-level data analysis, evaluation of real-world practice variations, and assessment of costs associated with managing adverse events. These investigations will enhance our understanding of the full economic value of different treatment regimens, thereby supporting evidence-based decision-making in optimizing cancer care delivery in resource-limited settings.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. World Health Organization. Cancer; 2022. Available from: https://www.who.int/news-room/fact-sheets/detail/cancer.
2. Redondo-Sánchez D, Petrova D, Rodríguez-Barranco M, Fernández-Navarro P, Jiménez-Moleón JJ, Sánchez MJ. Socio-economic inequalities in lung cancer outcomes: an overview of systematic reviews. Cancers. 2022;14(2):398. doi:10.3390/cancers14020398
3. Relli V, Trerotola M, Guerra E, Alberti S. Abandoning the notion of non-small cell lung cancer. Trends Mol Med. 2019;25(7):585–594. doi:10.1016/j.molmed.2019.04.012
4. Yousefi M, Jalilian H, Heydari S, Seyednejad F, Mir N. Cost of lung cancer: a systematic review. Value Health Reg Issues. 2023;33(1):17–26. doi:10.1016/j.vhri.2022.07.007
5. Ministry of Health. Home page. Published n.d. Available from: https://moh.gov.jo/ebv4.0/root_storage/ar/eb_list_page/%D8%A7%D9%84%D8%AA%D9%82%D8%B1%D9%8A%D8%B1_%D8%A7%D9%84%D8%B3%D9%86%D9%88%D9%8A_%D9%84%D8%A7%D8%B5%D8%A7%D8%A8%D8%A7%D8%AA_%D8%A7%D9%84%D8%B3%D8%B1%D8%B7%D8%A7%D9%86_%D8%A7%D9%84%D9%85%D8%B3%D8%AC%D9%84%D8%A9_%D9%81%D9%8A_%D8%A7%D9%84%D8%A7%D8%B1%D8%AF%D9%86_%D9%84%D8%B9%D8%A7%D9%85_2022.pdf.
6. Liu SY, Zheng MM, Pan Y, Liu SY, Li Y, Wu YL. Emerging evidence and treatment paradigm of non-small cell lung cancer. J Hematol Oncol. 2023;16(1):1–24. doi:10.1186/s13045-023-01436-2
7. Metreau E, Young KE, Eapen SG. World bank country classifications by income level for 2024-2025. World Bank Blogs; Published January 13, 2025. Available from: https://blogs.worldbank.org/en/opendata/world-bank-country-classifications-by-income-level-for-2024-2025.
8. Ministry of Health, Noncommunicable disease directorate. Cancer incidence rate. Unpublished internal data. 2024.
9. Treish I, Al Rabayah A, Jaddoua S, Tuffaha H. Impact of a new cost-effectiveness threshold implementation on cancer formulary decisions in Jordan. PharmacoEconomics - Open. 2021;6(2):137–145. doi:10.1007/s41669-021-00293-4
10. Mansour R, Abdel-Razeq H, Al-Hussaini M, et al. Systemic barriers to optimal cancer care in resource-limited countries: Jordanian healthcare as an example. Cancers. 2024;16(6):1117. doi:10.3390/cancers16061117
11. Schneider BJ, Ismaila N, Aerts J, et al. Lung cancer surveillance after definitive curative-intent therapy: ASCO guideline. J Clin Oncol. 2019;38(7):753–766. doi:10.1200/jco.19.02748
12. Lazzari C, Spagnolo CC, Ciappina G, et al. Immunotherapy in early-stage non-small cell lung cancer (NSCLC): current evidence and perspectives. Curr Oncol. 2023;30(4):3684–3696. doi:10.3390/curroncol30040280
13. Tsuboi M, Herbst RS, John T, et al. Overall survival with osimertinib in resected EGFR-mutated NSCLC. N Engl J Med. 2023;389(2):137–147. doi:10.1056/nejmoa2304594
14. Herbst RS, Wu Y-L, John T, et al. Adjuvant Osimertinib for resected EGFR-mutated stage IB-IIIA non–small-cell lung cancer: updated results from the phase III randomized ADAURA trial. J Clin Oncol. 2023;41(10):1830–1840. doi:10.1200/jco.22.02186
15. Forde PM, Spicer J, Lu S, et al. Neoadjuvant nivolumab plus chemotherapy in resectable lung cancer. N Engl J Med. 2022;386(21):1973–1985. doi:10.1056/nejmoa2202170
16. National Comprehensive Cancer Network (NCCN). Guidelines detail. Available from: https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1450.
17. Clatter bridge cancer CEn. Clatterbridge. Available from: https://www.clatterbridgecc.nhs.uk/professionals/clinical-guidance.
18. National Health Services. Chemotherapy protocols: lung. Available from: https://www.uhs.nhs.uk/health-professionals/chemotherapy-protocols/lung.
19. Xu X, Lazar CM, Ruger JP. Micro-costing in health and medicine: a critical appraisal. Health Econ Rev. 2021;11(1):1–8. doi:10.1186/s13561-020-00298-5
20. Jordan Food and Drug Administration (JFDA). Wholesale price information. Available from: https://www.jfda.jo.
21. XE.com. XE currency converter; 2024. Available from: https://www.xe.com.
22. Husereau D, Drummond M, Augustovski F, et al. Consolidated Health Economic Evaluation Reporting Standards (CHEERS) 2022 explanation and elaboration: a report of the ISPOR CHEERS II good practices task force. Value Health. 2022;25(1):10–31. doi:10.1016/j.jval.2021.10.008
23. King Abdullah University Hospital, Financial Department. Unit cost records. Unpublished internal data. 2024.
24. Jordan Unilabs. Price list for medical lab tests in Jordan. Available from: https://unilabs.jo/ar.
25. Jordan University Hospital, Financial Department. Unit cost records for an IV set infusion. Unpublished internal data. 2024.
26. Hammad EA, Alabbadi I, Taissir F, et al. Hospital unit costs in Jordan: insights from a country facing competing health demands and striving for universal health coverage. Health Eco Rev. 2022;12(1). doi:10.1186/s13561-022-00356-0
27. Microsoft Corporation. Microsoft Excel 2024 [computer software]. Redmond, WA: Microsoft Corporation; 2024.
28. Obeidat N, Awidi A, Ababneh N, et al. Frequency of epidermal growth factor receptor mutations in Jordanian lung adenocarcinoma patients at diagnosis. J Cancer Res Ther. 2016;12(2):616. doi:10.4103/0973-1482.147711
29. Kerr KM, Thunnissen E, Dafni U, et al. A retrospective cohort study of PD-L1 prevalence, molecular associations and clinical outcomes in patients with NSCLC: results from the European Thoracic Oncology Platform (ETOP) Lungscape project. Lung Cancer. 2019;131(March):95–103. doi:10.1016/j.lungcan.2019.03.012
30. Jacob S, Hovey E, Ng W, Vinod S, Delaney GP, Barton MB. Estimation of an optimal chemotherapy utilization rate for lung cancer: an evidence-based benchmark for cancer care. Lung Cancer. 2010;69(3):307–314. doi:10.1016/j.lungcan.2009.11.017
31. Smith TJ, Hillner BE, Kelly RJ. Reducing the cost of cancer care: how to bend the curve downward. Am Soc Clin Oncol Educ Book. 2012;32:e46–e51. doi:10.14694/edbook_am.2012.32.183
32. Van Harten WH, Wind A, De Paoli P, Saghatchian M, Oberst S. Actual costs of cancer drugs in 15 European countries. Lancet Oncol. 2015;17(1):18–20. doi:10.1016/s1470-2045(15)00486-6
33. World Bank Open Data. World bank open data. Available from: https://data.worldbank.org/indicator/SH.XPD.CHEX.GD.ZS?locations=JO.
34. Meropol NJ, Schulman KA. Cost of cancer care: issues and implications. J Clin Oncol. 2007;25(2):180–186. doi:10.1200/jco.2006.09.6081
35. Lam M, Olivier T, Haslam A, Tuia J, Prasad V. Cost of drug wastage from dose modification and discontinuation of oral anticancer drugs. JAMA Oncol. 2023;9(9):1238. doi:10.1001/jamaoncol.2023.2306
36. Hess LM, Cui ZL, Li XI, Oton AB, Shortenhaus S, Watson IA. Drug wastage and costs to the healthcare system in the care of patients with non-small cell lung cancer in the United States. J Med Econ. 2018;21(8):755–761. doi:10.1080/13696998.2018.1467918
37. Goldstraw P, Crowley J, Chansky K, et al. The IASLC lung cancer staging project: proposals for the revision of the TNM stage groupings in the forthcoming (Seventh) edition of the TNM classification of malignant tumours. J Thorac Oncol. 2007;2(8):706–714. doi:10.1097/jto.0b013e31812f3c1a
38. Kauffmann-Guerrero D. Adjuvant TKI treatment of EGFR-mutant lung cancer—already ripe for decision? Trans Lung Cancer Res. 2020;9(4):964–966. doi:10.21037/tlcr.2020.04.13
39. Kris MG, Gaspar LE, Chaft JE, et al. Adjuvant systemic therapy and adjuvant radiation therapy for stage I to IIIA completely resected non–small-cell lung cancers: American society of clinical oncology/cancer care Ontario clinical practice guideline update. J Clin Oncol. 2017;35(25):2960–2974. doi:10.1200/JCO.2017.72.4401
40. Wakelee HA, Altorki NK, Zhou C, et al. IMpower010: primary results of a phase III global study of atezolizumab versus best supportive care after adjuvant chemotherapy in resected stage IB-IIIA non-small cell lung cancer (NSCLC). J Clin Oncol. 2021;39(15_suppl):8500. doi:10.1200/jco.2021.39.15_suppl.8500
41. Wu YL, Tsuboi M, He J, et al. Osimertinib in resected EGFR-mutated non-small-cell lung cancer. N Engl J Med. 2020;383(18):1711–1723. doi:10.1056/nejmoa2027071
42. Heymach JV, Harpole D, Mitsudomi T, et al. Perioperative durvalumab for resectable non–small-cell lung cancer. N Engl J Med. 2023;389(18):1672–1684. doi:10.1056/nejmoa2304875
43. Spigel DR, Faivre-Finn C, Gray JE, et al. Five-year survival outcomes from the PACIFIC trial: durvalumab after chemoradiotherapy in stage III non-small-cell lung cancer. J Clin Oncol. 2022;40(12):1301–1311. doi:10.1200/jco.21.01308
44. Alabbadi I, Almomani E, Alshazili M. Drug selection for formulary inclusion: an exploratory case study of oncology medicines in Jordan. Value Health Reg Issues. 2020;21:211–221. doi:10.1016/j.vhri.2019.12.004
45. Pitt C, Vassall A, Teerawattananon Y, et al. Foreword: health economic evaluations in low- and middle-income countries: methodological issues and challenges for priority setting. Health Econ. 2016;25(S1):1–5. doi:10.1002/hec.3319
46. Zrubka Z, Rashdan O, Gulácsi L. Health economic publications from the Middle East and North Africa region: a scoping review of the volume and methods of research. Glob J Qual Saf Health Care. 2020;3(2):44–54. doi:10.36401/jqsh-20-4
47. Nadeem H, Jayakrishnan TT, Rajeev R, et al. ReCAP: cost differential of chemotherapy for solid tumors. J Oncol Pract. 2016;12(3):251. doi:10.1200/jop.2015.006700
48. Sohi GK, Levy J, Delibasic V, et al. The cost of chemotherapy administration: a systematic review and meta-analysis. Eur J Health Econ. 2021;22(4):605–620. doi:10.1007/s10198-021-01278-0
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Nanoparticles for Chemoimmunotherapy Against Triple-Negative Breast Cancer
Liu S, Li J, Gu L, Wu K, Xing H
International Journal of Nanomedicine 2022, 17:5209-5227
Published Date: 7 November 2022
The Path to Personalized Treatment in KRAS-Mutant Non-Small Cell Lung Cancer: A Review of Targeted Therapies and Immunotherapy
Shu CL, Liu YL
Cancer Management and Research 2022, 14:3485-3492
Published Date: 16 December 2022
Breast Cancer: An Overview of Current Therapeutic Strategies, Challenge, and Perspectives
Wang J, Wu SG
Breast Cancer: Targets and Therapy 2023, 15:721-730
Published Date: 20 October 2023
Roles of SPOCK1 in the Formation Mechanisms and Treatment of Non-Small-Cell Lung Cancer and Brain Metastases from Lung Cancer
Zhang X, Zhang X, Yin H, Li Q, Fan B, Jiang B, Xie A, Guo D, Hao H, Zhang B
OncoTargets and Therapy 2025, 18:35-47
Published Date: 16 January 2025
Diagnosis, Prognosis, and Treatment of Triple-Negative Breast Cancer: A Review
Jie H, Ma W, Huang C
Breast Cancer: Targets and Therapy 2025, 17:265-274
Published Date: 17 March 2025