")
Back to Journals » Journal of Inflammation Research » Volume 17
Comparative Efficacy and Safety of Ustekinumab and Secukinumab in the Treatment of Generalized Pustular Psoriasis: A 48-Week Retrospective Cohort Study with Genetic Background Analysis
Authors Ruan SF, Su X, Xiao Z, Zhang Y, Lin T, Luo R, Xiang N, Cheng B, Gong T, Ji C
Received 5 April 2024
Accepted for publication 13 September 2024
Published 24 September 2024 Volume 2024:17 Pages 6707—6721
DOI https://doi.org/10.2147/JIR.S472338
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tara Strutt
Shi-Fan Ruan,1– 3,* Xinhong Su,1,2,* Zhixun Xiao,1,2,* Yihua Zhang,1,2,* Tingting Lin,1,2 Renwei Luo,1,2 Niu Xiang,1,2 Bo Cheng,1– 3 Ting Gong,4 Chao Ji1– 3
1Department of Dermatology, The First Affiliated Hospital of Fujian Medical University, Fuzhou, Fujian, 350000, People’s Republic of China; 2Key Laboratory of Skin Cancer of Fujian Higher Education Institutions, Fuzhou, Fujian, 350000, People’s Republic of China; 3Fujian Provincial Clinical Research Center for Immune Skin Diseases, Fuzhou, Fujian, 350000, People’s Republic of China; 4Central Laboratory, The First Affiliated Hospital of Fujian Medical University, Fuzhou, Fujian, 350000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ting Gong, Central Laboratory, The First Affiliated Hospital of Fujian Medical University, 20 Chazhong Road, Fuzhou, Fujian, 350000, People’s Republic of China, Email [email protected] Chao Ji, Department of Dermatology, The First Affiliated Hospital of Fujian Medical University, 20 Chazhong Road, Fuzhou, Fujian, 350000, People’s Republic of China, Email [email protected]
Purpose: Recent studies have shown that novel biologics may provide significant clinical benefits for patients with generalized pustular psoriasis (GPP). Ustekinumab and secukinumab have been approved in Japan for GPP treatment in adult patients. However, the differences in efficacy and safety of these two drugs in GPP are not known.
Aim: Based on the genetic background, we aimed to compare the efficacy and safety of secukinumab and ustekinumab in patients with GPP.
Methods: Patients with moderate to severe GPP who were treated with ustekinumab/secukinumab at our department from July 2019 to May 2022 were included in this study and followed up for 48 weeks. The difference in efficacy between ustekinumab and secukinumab was evaluated by assessing changes in body temperature, laboratory indices, recovery of skin lesions, and changes in quality of life. Additionally, we collected patients’ saliva for genotyping and explored the effect of CARD14 genetic mutations on clinical efficacy.
Results: A total of 65 patients (32 adults and 33 children) with moderate to severe GPP were included in this study. 31 patients received ustekinumab therapy, and 34 patients were treated with secukinumab. Secukinumab demonstrated superiority to ustekinumab, as evidenced by a higher GPPASI 90 response at week 2. Additionally, the efficacy of ustekinumab and secukinumab was found to be independent of the presence of the CARD14 mutation.
Conclusion: Secukinumab is superior to ustekinumab in rapidly clearing the skin and improving health-related quality of life. Moreover, the responses to ustekinumab/secukinumab in patients were not influenced by CARD14 gene mutations.
Keywords: generalized pustular psoriasis, secukinumab, ustekinumab, clinical efficacy, safety, gene mutations
Introduction
Generalized pustular psoriasis (GPP) is a chronic and recurrent systemic inflammatory disease characterized by the sudden and extensive eruption of superficial sterile pustules, accompanied by fever, discomfort, and fatigue. GPP onset often occurs in people aged 40–50 years, and patients with onset in childhood are often associated with genetic mutations.1 The estimated global prevalence of GPP is 0.27–4.6 per 10,000 people, and it is more common in women. GPP is much less common in the pediatric population, accounting for 0.6% to 7% of all psoriasis cases.2,3 The mechanism of this disease remains unclear, and some genetic factors are thought to be involved in the development of GPP, including mutations in IL36RN, CARD14, AP1S3, TNIP1, SERPINA3, and MPO.4 Recent case reports have shown that genetic risk factors do not impact treatment efficiency.5–7
The treatment of GPP is challenging due to the recurrent course of the disease. Currently, traditional drugs such as acitretin, methotrexate, and cyclosporine are used as first-line treatment options for pediatric and adult GPP and may also be effective. However, side effects such as hyperlipidemia, premature epiphyseal closure, severe teratogenic effects, and abnormal liver and kidney function are of great concern for patients.2,8 Therefore, they are not ideal long-term treatment options for GPP patients. Recent studies have shown that novel biologics may provide significant clinical benefits for patients with GPP. In a recent nationwide retrospective cohort study with 1516 GPP patients included in Japan, Miyachi et al stated that biological therapy for GPP showed favorable outcomes, including fewer comorbidities, lower in-hospital mortality, and morbidity compared to other treatments.9
The current studies demonstrate innate and adaptive immune responses functioning in tandem in GPP.8 The innate immunity driven by the interleukin (IL) −1/IL-36-chemokine-neutrophil axis plays a crucial role in the pathogenesis of GPP. Innate inflammation cooperates with the adaptive immune response induced by the IL-23/IL-17 axis, leading to a progressive cycle of inflammation.1 Biological therapies that target IL-36, along with cytokines in the IL-23/IL-17 axis, are employed in the treatment of GPP. This includes drugs like spesolimab, an antagonist of the IL-36 receptor, ustekinumab, a selective inhibitor of IL-12/23p40, and secukinumab, characterized by its inhibition of IL-17A. Currently, spesolimab has been on the market for a short time, and there is no long-term real-world data available yet. In China, ustekinumab and secukinumab have emerged as new options for clinical doctors to treat GPP in recent years. There are few real-world studies on the long-term efficacy and safety of ustekinumab and secukinumab in the treatment of GPP, and long-term follow-up data of adult patients are limited to Japanese Phase III clinical trial studies.10,11 Arakawa A et al showed that GPP responded well to ustekinumab treatment irrespective of the presence or absence of IL36RN mutations.12 Previous studies by our team have demonstrated that secukinumab provides high and sustained clinical benefits in children with GPP and is well tolerated by pediatric patients with GPP.13 Similar conclusions were also drawn by Miao C et al, where GPP systemic inflammation and skin symptoms rapidly improved with the treatment of secukinumab.14 However, the differences in efficacy and safety of the two drugs in GPP are not yet fully understood. In this study, we aim to report the difference in efficacy between an IL-17A inhibitor and an IL-12/23p40 inhibitor in GPP. We also sought to test whether CARD14 gene mutations, one of the major genes mutated in GPP, predispose GPP patients to respond differently to ustekinumab and secukinumab.
Materials and Methods
Study Design and Patients
This is a retrospective study of adult and pediatric patients with GPP. We obtained data for 65 patients (33 children, 32 adults) who were admitted to the Department of Dermatology in the First Affiliated Hospital of Fujian Medical University because of GPP between July 2019 and May 2022. 31 (15 children, 16 adults) of these patients were treated with ustekinumab while 34 (18 children, 16 adults) were treated with secukinumab. All patients were followed for 48 weeks.
Diagnostic Criteria
Patients corresponded to all four features according to Japanese guidelines for the management and treatment of GPP.10
Inclusion Criteria
Exclusion Criteria
Genotyping
Genomic DNA was isolated from human saliva collected using the ORAcollect•DNA OCR-100 kit. The DNA quality control and genotyping were carried out at the WeGene Clinical Laboratory in Shenzhen. To identify mutations in IL36RN, CARD14, AP1S3, and MPO, targeted re-sequencing was performed using the Illumina Infinium Chinese Genotyping Array BeadChip: Illumina WeGene V3 Arrays. Genotyping was performed by the Illumina iScan System, following the manufacturer’s instructions.
Treatment
Before treatment, patients underwent routine blood and urine tests, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), liver and kidney function tests, tuberculous infection of T cells spot tests, hepatitis B virus marker tests, chest CT scans, etc. After exclusion of relevant contraindications, patients received subcutaneous ustekinumab/secukinumab therapy. During the treatment period, patients received either ustekinumab at weeks 0, 4, 16, and every 12 weeks thereafter until week 48, or secukinumab at weeks 0, 1, 2, 3, and 4, and every 4 weeks thereafter until week 48. The dose of ustekinumab/secukinumab was referenced to the dose used for moderate to severe plaque psoriasis. The single dose of ustekinumab was 45 mg for adult subjects weighing ≤ 100 kg, and 90 mg for subjects weighing > 100 kg. The ustekinumab dosage for pediatric patients was 0.75 mg/kg for patients weighing < 60 kg; 45 mg for pediatric patients weighing 60 kg to 100 kg; and 90 mg for pediatric patients weighing > 100 kg. The secukinumab dosage was 300mg for adult humans. Pediatric patients received a dose based on their weight category (<50 kg, ≥50 kg): patients weighing < 50 kg received 75 mg, those weighing ≥50 kg received 150 mg. All subjects were thoroughly counseled, and consent was obtained prior to commencing any therapy.
Assessment of Efficacy
The efficacy was assessed based on three aspects: changes in body temperature and laboratory indices, improvement of skin lesions, and changes in quality of life.
Body temperatures were recorded every day during hospitalization. White blood cell (WBC) count, CRP levels, and serum albumin were measured using standard methodologies by local laboratory at baseline before first treatment and at week 1, 2, 3, and 4.
Efficacy analyses were performed based on the scores of Generalized Pustular Psoriasis Area and Severity Index (GPPASI) and Generalized Pustular Psoriasis Physician Global Assessment (GPPGA) at week 0, 2, 4, 12, 24, and 48. Specific assessment methods have been described previously and were evaluated as described previously.13
At weeks 0, 4, 12, and 24, adult patients completed the Dermatology Life Quality Index (DLQI) and the Medical Outcomes Study 36-item Short-Form Health Survey (SF-36), and pediatric patients completed the Children’s Dermatology Life Quality Index (CDLQI) and the Pediatric Quality of Life Inventory (PedsQL) with the assistance of a physician or parents.
The DLQI is a widely used indicator to assess the quality of life (QoL) of people with psoriasis and consists of 10 questions covering six domains of health-related quality of life (HRQoL): symptoms and feelings, daily activities, leisure, work and school, personal relationships, and treatment. Each question was rated as follows: “not at all” = 0; “a little” = 1; “a lot” = 2; “very much” = 3. Possible total score ranged from 0 to 30, with a lower score indicating better HRQoL. The CDLQI is the pediatric version of the DLQI replacing the questions with a full-color cartoon version that is easier for pediatric patients to understand. DLQI / CDLQI 0 or 1 indicates that the disease has no effect on the patient’s QoL.
The SF-36 is a frequently used self-reported measure of health that is widely used to evaluate the effectiveness of clinical trials related to psoriasis. This scale consists of 9 dimensions, namely Physical Functioning (PF), Role-Physical (RP), Bodily Pain (BP), General Health (GH), Vitality (VT), Social Functioning (SF), Role-Emotional (RE), Mental Health (MH), and Reported Health Transition (HT). Each dimension is directly transformed into a 0–100 scale on the assumption that each question carries equal weight. The Physical Component Summary (PCS) is the mean of four dimensions: PF, RP, BP, and GH. The Mental Component Summary (MCS) is the mean of four dimensions: VT, SF, RE, and MH. The higher the score, the better the HRQoL.
The PedsQL consists of 23 items and encompasses the core domains of physical health and psychosocial health (including social functioning, school functioning, emotional functioning). Possible PedsQL total score, physical health summary score, and psychosocial health summary score range from 0 to 100, with higher scores indicating better HRQoL. Three age-specific versions of the PedsQLTM 4.0 Generic Core Scales were administered: 5 to 7, 8 to 12, and 13 to 18 years of age. All patients completed the questionnaire independently.
Assessment of Safety
Patients were also asked to report all adverse events (AEs) during follow-up.
Clinical Outcomes
Statistical Analysis
All data were expressed as mean ± standard deviation (SD), frequency (percentage), and median (interquartile ranges). The t-test was used to compare two groups conforming to normal distributions, and the Mann–Whitney U-test was used to compare skewed distributions. Fisher exact test was used to compare GPPASI75/90/100 and DLQI 0/1 responses between treatments; analysis of covariance was used for absolute change from baseline in subjects’ assessment of body temperature, laboratory indices, PedsQL total score, and SF-36. Multivariate analysis of variance (MANOVA) was used to assess the statistical significance of the differences in cytokine levels before and after treatment. P value < 0.05 was considered statistically significant. All statistical analyses were performed by SPSS (version 22.0; IBM, Armonk, NY) and GraphPad Prism 9.1 (GraphPad Software Inc., La Jolla, CA, USA).
Results
Study Patients
The study protocol and participants’ disposition in this study are shown in Figure 1. A total of 65 patients were enrolled in this study. Among them, 31 (47.69%) patients received ustekinumab therapy, with 15 of them being children and 16 being adults. The remaining 34 (52.31%) patients were treated with secukinumab, with 18 being children and 16 being adults. No dropouts occurred during the follow-up period. The age of the patients ranged from 2 to 83 years, with a mean age of 36.00±18.97 in the ustekinumab group and 22.92±21.07 in the secukinumab group. Of all patients, 47.69% (31 out of 65 patients) had been diagnosed with psoriasis vulgaris (PV) prior to GPP. The mean GPPASI score in the patients of the two groups was 25.16±7.64 and 25.97±8.32, respectively. All patients had a total GPPGA score of 3 or more, indicating moderate to severe disease and reflecting that the enrolled patients were in the acute phase of GPP. None of the subjects received any other treatment, including phototherapy or topical therapy, while using ustekinumab/secukinumab. The baseline characteristics of all subjects are shown in Table 1.
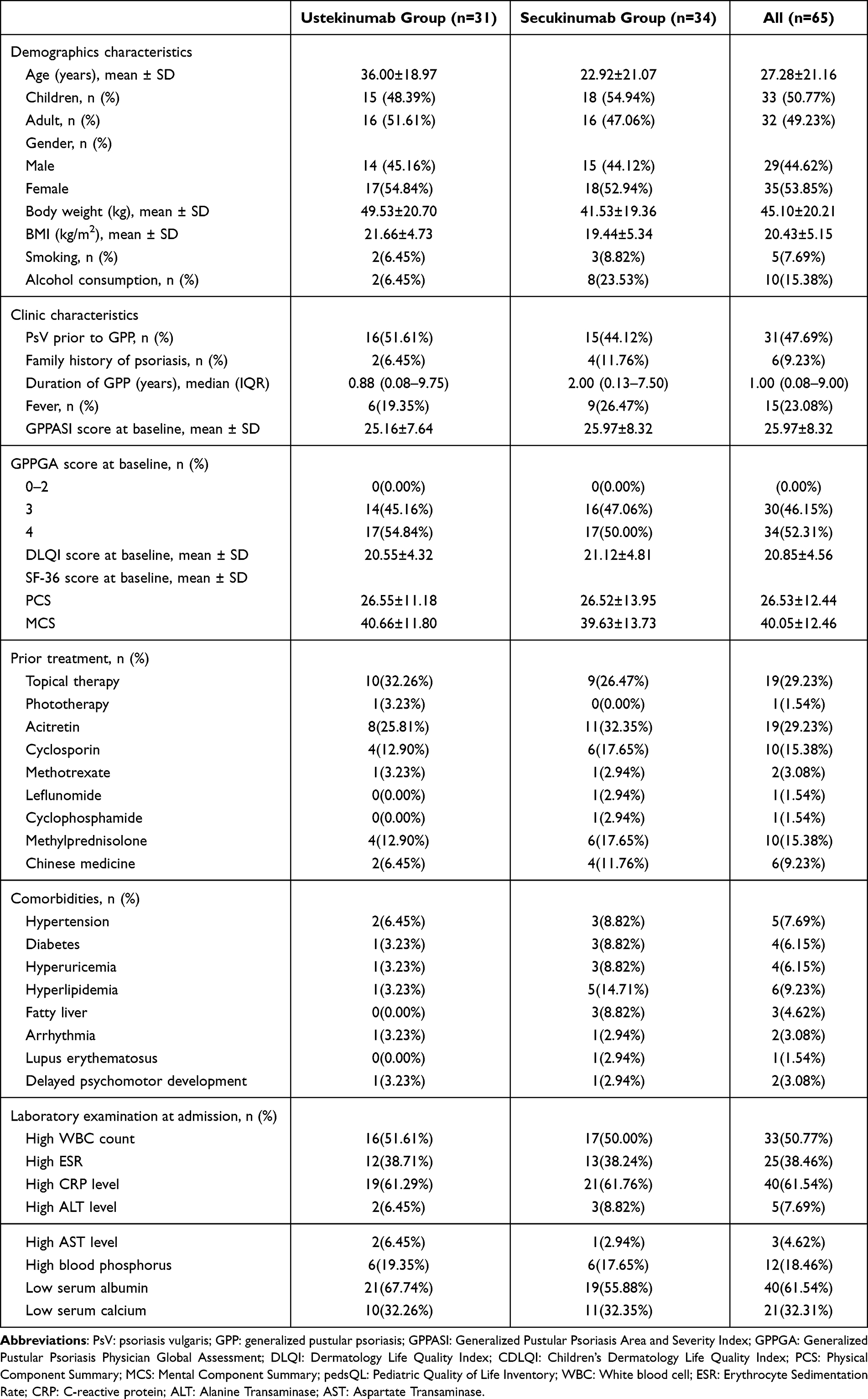 |
Table 1 Patient Demographics and Baseline Disease Characteristics |
 |
Figure 1 Study protocol. Two independent cohorts were enrolled in this study. |
Clinical Responses with Secukinumab Occurred Earlier and Were Greater Than Those with Ustekinumab Throughout the 48-Week Treatment Period
Subjects in the secukinumab group reported faster improvement in temperature, WBC, CRP, and serum albumin compared to the ustekinumab group (Figure 2). Most patients’ temperature returned to normalcy within 7 days after treatment (Figure 2A). WBC counts restored in both groups in the first week (Figure 2B). No marked difference was observed in CRP levels between the two groups before treatment (P>0.05). The CRP levels of the two groups of patients decreased noticeably after treatment, and the decrease in the secukinumab group was more significant (P=0.005) (Figure 2C). Serum albumin was significantly elevated and returned to normal levels in both groups by week 2 after treatment. From baseline to week 3, the increase in serum albumin was more pronounced in the secukinumab group compared to the ustekinumab group (at week 1, P=0.041; at week 2, P<0.0001; at week 3, P<0.0001) (Figure 2D).
 |
Figure 2 Changes in body temperature (A), WBC count (B), CRP level (C), and serum albumin level (D) after 4 weeks of ustekinumab/secukinumab treatment. All data presented in the figure are the median (interquartile ranges). Analysis of covariance was used for absolute change from baseline in subjects’ assessment of body temperature, WBC count, CRP level, and serum albumin level. P values <0.05 were considered statistically significant. *P <0.05, **P<0.01, ****P<0.0001. |
The main result was the proportion of patients in each group who achieved GPPASI 75, GPPASI 90, and GPPASI 100 at each time point (Figure 3). Our results showed that a significantly greater proportion of patients in the secukinumab group achieved a GPPASI 75 response at week 1 (14 [41.18%] of 34 patients vs 3 [9.68%] of 31 patients), and week 2 (25 [73.53%] of 34 patients vs 16 [51.61%] of 31 patients) than did those in the ustekinumab group (treatment difference was 31.50 percentage points at week 1, 95% CI 1.67–25.78, P<0.001; treatment difference was 21.92 percentage points at week 2, 95% CI 0.92–7.35, P=0.047) (Figure 3A). We found consistent results, with 12 (35%) of 34 patients in the secukinumab group versus 2 (6.45%) of 31 patients in the ustekinumab group achieving a GPPASI 90 response at week 2 (treatment difference was 28.55 percentage points, 95% CI 1.60–39.03, P=0.012) (Figure 3B). The proportions of patients achieving GPPASI 75/90 responses were similar between the ustekinumab and secukinumab groups after week 4. During the 48-week follow-up period, the proportions of patients with a GPPASI 100 response in the ustekinumab group were lower than those in the secukinumab group, but there was no statistically significant difference (Figure 3C). In the ustekinumab group, the mean time of disappearance of pustules was 4.26±1.41 days, while in the secukinumab group, it was 3.00±1.23 days. The difference between the two groups was statistically significant (P=0.0003) (Figure 3D). Representative patient photographs showing disease progression before and after the biological therapy were shown in Figure 4.
 |
Figure 3 Proportions of patients achieving clinical response over time in the ustekinumab (n=31) and secukinumab (n=34) groups. Proportion of patients achieving at least 75% improvement from baseline in GPPASI (A), a 90% improvement in GPPASI (B), and a 100% improvement in GPPASI (C) in both groups. (D) Time of pustular disappearance. Data presented are the mean values±SD. *P < 0.05, **P < 0.01, ***P < 0.001, ****P < 0.0001. |
 |
Figure 4 Clinical photographs of pediatric patients and an adult patient with GPP, along with their GPPASI score at baseline (week 0), week 2, week 24, and week 48 with the treatment of ustekinumab/secukinumab. Patient 1 was an 8-year-old pediatric patient with GPP treated with ustekinumab. Patient 2 was a 33-year-old adult patient with GPP treated with secukinumab. |
GPP is well known to adversely affect the overall quality of life. In our study, we assessed the quality of life in patients using DLQI/CDLQI, PedsQL, and SF-36 (Table 2). During the 48-week follow-up period, the proportions of patients with a CDLQI/DLQI 0/1 response in the ustekinumab group were lower than those in the secukinumab group, but there was no statistically significant difference. The PedsQL total score improved gradually over time in both groups. No marked difference was observed in PedsQL total scores in both groups before treatment (P > 0.05). The PedsQL total score of the two groups of patients at week 2 increased noticeably, and the increase in the secukinumab group was more significant (P = 0.005). Similar findings were found in SF-36 scores of adult patients as PedsQL. In terms of SF-36 PCS, the improvement was more obvious in the secukinumab group compared with the ustekinumab group at week 2 (P = 0.022). Improvements in PedsQL total scores and SF-36 PCS were not significantly different between the two groups at other time points. In conclusion, secukinumab reversed HRQoL more rapidly in pediatric and adult GPP patients compared to ustekinumab.
 |
Table 2 Health-Related Quality of Life End Points |
CARD14 Mutation Did Not Affect the Therapeutic Efficiency of Ustekinumab and Secukinumab
In our study, all patients were tested for mutations in the IL36RN, CARD14, AP1S3, and MPO genes. Of these patients, 44.62% were found to have gene mutations, while 55.38% did not. The mutated sites identified in pediatric and adult patients were distributed in CARD14 (29 [44.61%] of 65 patients) and IL36RN (1 [1.54%] of 65 patients). No mutations in the AP1S3 and MPO genes were detected. The most commonly detected genetic mutation was the CARD14 mutation, accounting for 48.39% (15 of 31 patients) in the ustekinumab group and 41.18% (14 of 34 patients) in the secukinumab group. Therefore, we focused on the impact of CARD14 gene mutations on the clinical response (Figure 5). To determine whether CARD14 gene mutation was independently associated with the response to ustekinumab/secukinumab, we analyzed patients with or without CARD14 mutations and observed that patients with CARD14 mutations did not have higher response rates than those without mutations in terms of GPPASI 90 at weeks 2, 4, 12, 24, and 48, suggesting that CARD14 gene mutation was not associated with a good clinical response to ustekinumab/secukinumab (Figure 5A and B). We also found that CARD14 mutation does not affect the difference in efficacy between ustekinumab and secukinumab in the treatment of GPP (Figure 5C and D). The proportion of patients achieving a GPPASI 90 response at week 2 was higher in the secukinumab group than in the ustekinumab group, regardless of the presence or absence of the CARD14 gene mutation (CARD14 positive: 6 [46.15%] of 13 patients vs 2 [12.50%] of 16 patients, P=0.03; CARD14 negative: 5 [28.57%] of 21 patients vs 0 [0%] of 15 patients, P=0.92). The efficacy of ustekinumab/secukinumab, regardless of the presence of the CARD14 mutation, suggests that the IL-23/IL-17A pathway may play a pathogenic role among patients with GPP who have different genetic backgrounds, including those without gene mutations. Two-way ANOVA was employed to assess the effects of CARD14 gene mutations and medications, as well as interaction effects (CARD14 gene mutation x medication). The P-value for interaction was not significant at week 1, 2, 4, 12, 24, and 48 (all P>0.05). These results show that CARD14 mutation does not affect the therapeutic efficiency of ustekinumab and secukinumab.
 |
Figure 5 (A and B) Proportions of patients in the CARD14 positive and CARD14 negative groups who achieved GPPASI 90 with ustekinumab/secukinumab treatment. (C and D) Proportions of patients in the ustekinumab and secukinumab groups who achieved GPPASI 90 with CARD14 positive or negative status. *P < 0.05. |
Ustekinumab and Secukinumab Have a Good Safety Profile for Pediatric and Adult Patients with GPP
During the follow-up, no new or unexpected safety signals were observed (Table 3). AEs were similar in extent and severity to those previously observed in each treatment group. The proportions of patients with any AEs were comparable between the ustekinumab and secukinumab groups (32.26% vs 38.24%, respectively). There was a high incidence of skin-related adverse reactions in both groups, including 6 cases of eczema-like dermatitis, 3 cases of injection site reactions, and 1 case of urticaria.
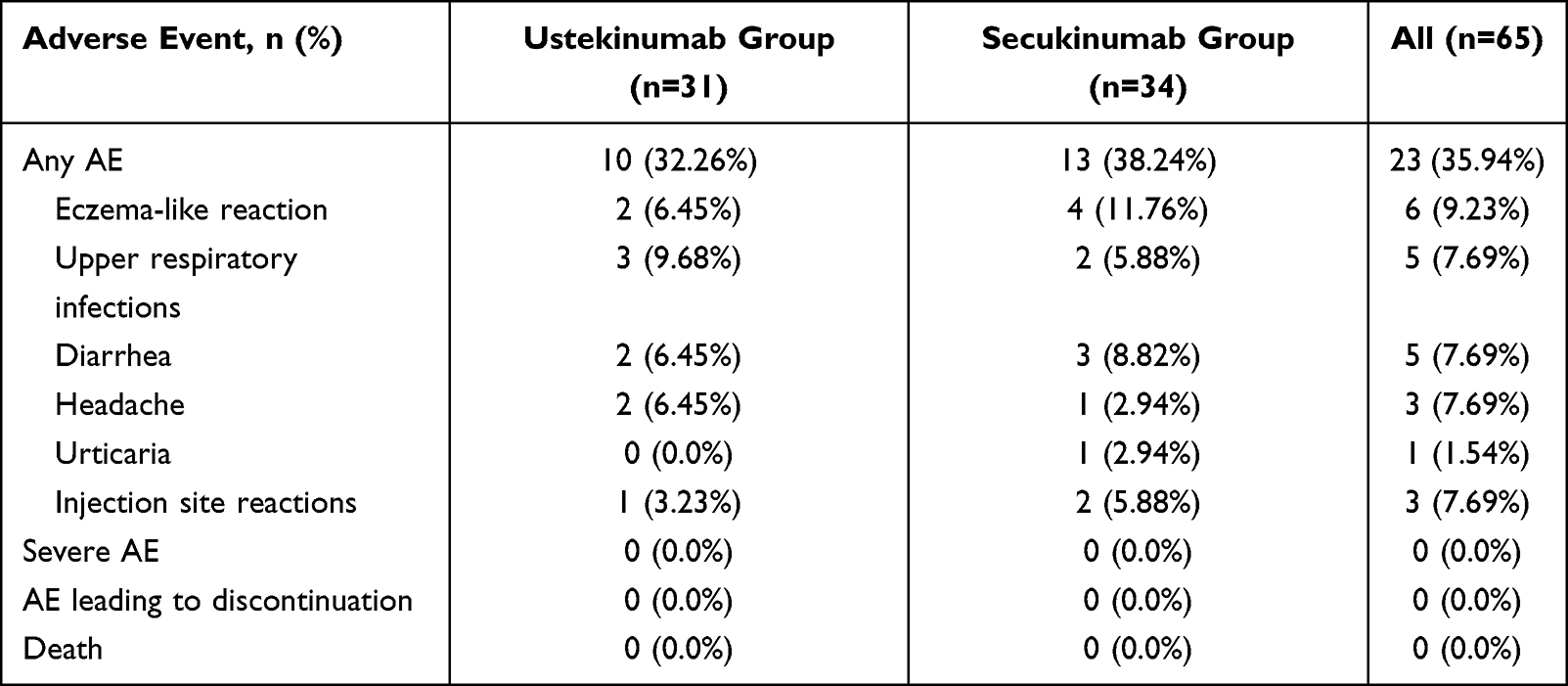 |
Table 3 Overview of Adverse Events Up to Week 48 |
Discussion
GPP is a recurrent and severe multi-systemic inflammatory disease. Patients with GPP may experience frequent flares, resulting in a significant decrease in their quality of life.15,16 Conventional drugs are not suitable for long-term maintenance treatment, and most patients experience a relapse of the disease even after medication is administered. Biologics may be one of the first-line treatment options for GPP. In this study, we present a substantial amount of comparative efficacy and safety data on two biological agents used in the treatment of patients with GPP. We reported on 33 children and 32 adults with GPP who received either ustekinumab or secukinumab monotherapy. The patients were followed for up to 48 weeks.
We found that both ustekinumab and secukinumab effectively reversed the systemic inflammation and skin symptoms of GPP, with sustained improvement observed for up to 48 weeks. The majority of patients achieved a GPPASI 100 response and maintained it until week 48. Additionally, our study demonstrated that secukinumab acted rapidly, as a significantly higher proportion of patients receiving secukinumab achieved efficacy responses at week 1 and 2 compared to those receiving ustekinumab. The pustule clearance time was also shorter in the secukinumab group compared to the ustekinumab group, with most patients experiencing complete pustule disappearance within 72 hours after the first injection of secukinumab, while it took 1 week for patients using ustekinumab. This difference in response may be attributed to IL-17A, a known potent neutrophil chemotactic factor.17 IL-17A has a strong ability to recruit neutrophils and induce the release of neutrophil chemoattractants (eg, CXCL1, CXCL8) from keratinocytes.18 The use of IL-17A inhibitors directly reduces the release of neutrophil chemokines, preventing the accumulation of neutrophils in the epidermis and the formation of Kogoj’s spongiform pustules. In contrast, IL-12/23 inhibitors indirectly affect IL-17A production by inhibiting IL-23, which subsequently prevents neutrophil aggregation in the epidermis. Furthermore, several studies have shown that the neutrophil/IL-36 axis plays a central role in the development of skin inflammation in GPP.19 In psoriatic lesions, IL-17A initiates the IL-36 amplification cycle, resulting in active IL-36 cytokines that act synergistically with IL-17A.20 IL-17A inhibitors interfere with the IL-36 cytokine family members in keratinocytes, affecting several inflammatory processes, including keratinocyte differentiation into a psoriatic phenotype.17 Therefore, clinical responses with secukinumab occurred earlier than those with ustekinumab. Our study suggests that pediatric patients with GPP had a good response to ustekinumab or secukinumab monotherapy. Compared to children treated with ustekinumab, children receiving secukinumab experienced a shorter time to improve systemic symptoms and achieve complete clearance of lesions. However, due to the exploratory nature of this study, further research and clinical trials are needed to determine the optimal dosage, injection frequency, and overall treatment course of ustekinumab/secukinumab in pediatric patients with GPP.
With the shift in the medical pattern to a biopsychosocial model, researchers have introduced the concept of HRQoL. Assessment of improvement in quality of life during the treatment of chronic diseases is an important indicator of treatment effectiveness. Adult patients with GPP were severely affected in terms of PF and RP. Due to the extensive lesions and systemic symptoms, patients were often unable to perform daily work or even basic activities (such as walking, climbing stairs, bathing, dressing, etc). At the same time, the patient’s SF and RE were significantly affected. Patients’ work and daily activities were prevented by the negative emotions brought about by this disease. In the current study, we also found that GPP had a negative impact on physical and psychosocial development in children and caused major social and economic burdens on patients, families, and health care systems. During the acute phase of GPP, pediatric patients were usually suffered from intense physical discomfort which affected their physical activities (eg, running, sports exercise, bathing, etc). They reported feeling frustrated, helpless, and scared and had trouble sleeping. Due to the frequent disease recurrence, some patients had to suspend or leave school, which significantly affected their academic and social activities. Moreover, since treatment often requires the involvement of caregivers, the QoL of the family members may also be impaired.21,22 Our results showed that ustekinumab and secukinumab can significantly improve HRQoL of pediatric and adult patients with GPP. 86.15% of patients reached a CDLQI/DLQI score of “0 or 1” at week 48. Consistent with its clinical efficacy, secukinumab also achieved significantly faster improvement in subject-reported symptoms and HRQoL, compared with ustekinumab.
In recent years, variants of IL36RN, CARD14, AP1S3, and MPO genes have been identified as causative or contributing to genetic defects in a proportion of patients affected by GPP.23 Mutations in the IL36RN and CARD14 genes are likely to be the main molecular genetic basis defect in patients with GPP.1,2 However, in our data, the most detected genetic mutation was the CARD14 mutation. Gain-of-function mutations in the CARD14 gene cause enhanced NF-κB activation in keratinocytes and upregulation of a subset of psoriasis-associated genes, particularly the chemokine CCL20 and IL-8 genes.24 We compared the clinical efficacy of ustekinumab or secukinumab in 29 GPP patients with CARD14 mutations and 36 patients without mutations. The observation that ustekinumab and secukinumab demonstrated efficacy in patients with and without CARD14 genetic mutations suggests that the IL-23/IL-17A immune pathway plays a key role in GPP pathogenesis, regardless of the presence of genetic alterations. This immune pathway serves as a bridge between innate and adaptive immunity, involving the activation of IL-36 and promoting the chemotaxis and aggregation of inflammatory cells (eg, neutrophils) at sites of inflammation.8
No new or unexpected safety signals were identified for ustekinumab and secukinumab during the 48-week treatment period. Secukinumab exhibited a safety profile similar to that of ustekinumab and consistent with that seen in secukinumab pivotal phase III trials. In the phase III clinical trial, secukinumab was well tolerated for GPP patients, and no deaths were reported. Common adverse reactions included nasopharyngitis, urticaria, diabetes mellitus, and arthralgia.11 In this study, it is worth noting that the incidence of eczema-like reactions was as high as 9.23% (6 out of 65 patients). Interestingly, 5 of these patients had a history of atopic and/or allergic diseases. We speculated that targeting Th1 cytokines would induce a Th2-dominated immune response, resulting in the eczema-like phenotype.25 In a recent study, the authors suggested that patients with a prior history of atopy (atopic dermatitis, asthma, or allergic rhinitis) seem to be more likely to experience such adverse events. Therefore, dermatologists should pay more attention to patients with a special medical history when using biological agents.26 Other adverse reactions included upper respiratory infections, diarrhea, headache, and injection site reactions. However, these adverse reactions did not lead to the discontinuation of ustekinumab/secukinumab. In general, our study confirms that ustekinumab and secukinumab are safe and effective medications for long-term use in both adult and child patients with GPP.
Taken together, our study confirms the superiority of secukinumab over ustekinumab in achieving rapid skin clearing among both adult and pediatric patients with GPP. Furthermore, we found that CARD14 mutation did not impact the therapeutic efficacy of either ustekinumab or secukinumab. Secukinumab also demonstrated superiority over ustekinumab in improving patients’ health-related quality of life. Additionally, the safety profile of secukinumab observed over the 48-week period was comparable to that of ustekinumab and consistent with previous findings.
Conclusion
Potential limitations include the retrospective nature of the data, single-center nature, lack of a control group, and small sample size. Our study highlights the efficacy and safety of ustekinumab/secukinumab treatment in adult and pediatric patients with GPP and hence deserves replication in larger sample size and future randomized controlled trials.
Ethics Approval and Consent to Participate
The population study was carried out following the principles stated in the Declaration of Helsinki and received approval from the Ethics Committee of the First Affiliated Hospital of Fujian Medical University, Fuzhou, China, in accordance with Chinese law (no. [2022]007). Written informed consent was obtained from patients/participants to participate in this study. In this study, informed consent was obtained from the parents or legal guardians of all patients under the age of 18.
Funding
This work was supported by grants from the National Natural Science Foundation of China (No.82373469), the Joint Funds for the Innovation of Science and Technology, Fujian Province (No.2021Y9150), and the Startup Fund for Scientific Research of Fujian Medical University (No.2022QH2027).
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Gooderham MJ, Van Voorhees AS, Lebwohl MG. An update on generalized pustular psoriasis. Expert Rev Clin Immunol. 2019;15(9):907–919. doi:10.1080/1744666X.2019.1648209
2. Hoegler KM, John AM, Handler MZ, Schwartz RA. Generalized pustular psoriasis: a review and update on treatment. J Eur Acad Dermatol Venereol. 2018;32(10):1645–1651. doi:10.1111/jdv.14949
3. Boehner A, Navarini AA, Eyerich K. Generalized pustular psoriasis - A model disease for specific targeted immunotherapy, systematic review. Exp Dermatol. 2018;27(10):1067–1077. doi:10.1111/exd.13699
4. Takeichi T, Akiyama M. Generalized pustular psoriasis: clinical management and update on autoinflammatory aspects. Am J Clin Dermatol. 2020;21(2):227–236. doi:10.1007/s40257-019-00492-0
5. Albela H, Begum S, Leong KF. Successful treatment of paediatric generalized pustular psoriasis with secukinumab: a case series. J Dermatol Treat. 2022;33(3):1769–1773. doi:10.1080/09546634.2021.1899111
6. Sun ZL, Liu ZL, Xu YY, Zhang XL, Zhang CL, Guan X. Successful treatment of generalized pustular psoriasis with secukinumab: a report of two cases. Chin Med J. 2020;133(24):3015–3016 doi:10.1097/CM9.0000000000001244.
7. Gabeff R, Safar R, Leducq S, et al. Successful therapy with secukinumab in a patient with generalized pustular psoriasis carrying homozygous IL36RN p.His32Arg mutation. Int J Dermatol. 2019;58(1):e16–e17. doi:10.1111/ijd.14293
8. Samotij D, Szczęch J, Reich A. Generalized pustular psoriasis: divergence of innate and adaptive immunity. Int J Mol Sci. 2021;22(16):9048. doi:10.3390/ijms22169048
9. Miyachi H, Konishi T, Kumazawa R, et al. Treatments and outcomes of generalized pustular psoriasis: a cohort of 1516 patients in a nationwide inpatient database in Japan. J Am Acad Dermatol. 2022;86(6):1266–1274. doi:10.1016/j.jaad.2021.06.008
10. Fujita H, Terui T, Hayama K, et al. Japanese guidelines for the management and treatment of generalized pustular psoriasis: the new pathogenesis and treatment of GPP. J Dermatol. 2018;45(11):1235–1270. doi:10.1111/1346-8138.14523
11. Imafuku S, Honma M, Okubo Y, et al. Efficacy and safety of secukinumab in patients with generalized pustular psoriasis: a 52-week analysis from phase III open-label multicenter Japanese study. J Dermatol. 2016;43(9):1011–1017. doi:10.1111/1346-8138.13306
12. Arakawa A, Ruzicka T, Prinz JC. therapeutic efficacy of interleukin 12/interleukin 23 blockade in generalized pustular psoriasis regardless of IL36RN mutation status. JAMA Dermatol. 2016;152(7):825–828. doi:10.1001/jamadermatol.2016.0751
13. Ruan SF, Zhang LL, Liu Z, et al. Real-world data on the clinical use of secukinumab in pediatric generalized pustular psoriasis: a 48-week retrospective study. J Am Acad Dermatol. 2023;88(1):243–246. doi:10.1016/j.jaad.2022.04.064
14. Miao C, Chen Y, Wang Z, Xiang X, Liu Y, Xu Z. Real-world data on the use of secukinumab and Acitretin in pediatric generalized pustular psoriasis. J Dermatol. 2023;50(2):258–261. doi:10.1111/1346-8138.16551
15. Wang WM, Jin HZ. Biologics in the treatment of pustular psoriasis. Expert Opin Drug Saf. 2020;19(8):969–980. doi:10.1080/14740338.2020.1785427
16. Saikaly SK, Mattes M. Biologics and pediatric generalized pustular psoriasis: an emerging therapeutic trend. Cureus. 2016;8(6):e652. doi:10.7759/cureus.652
17. Plachouri KM, Chourdakis V, Georgiou S. The role of IL-17 and IL-17 receptor inhibitors in the management of generalized pustular psoriasis. Drugs Today. 2019;55(9):587–593. doi:10.1358/dot.2019.55.9.3020159
18. Reich K, Papp KA, Matheson RT, et al. Evidence that a neutrophil-keratinocyte crosstalk is an early target of IL-17A inhibition in psoriasis. Exp Dermatol. 2015;24(7):529–535. doi:10.1111/exd.12710
19. Johnston A, Xing X, Wolterink L, et al. IL-1 and IL-36 are dominant cytokines in generalized pustular psoriasis. J Allergy Clin Immunol. 2017;140(1):109–120. doi:10.1016/j.jaci.2016.08.056
20. Pfaff CM, Marquardt Y, Fietkau K, Baron JM, Lüscher B. The psoriasis-associated IL-17A induces and cooperates with IL-36 cytokines to control keratinocyte differentiation and function. Sci Rep. 2017;7(1):15631. doi:10.1038/s41598-017-15892-7
21. Lin VW. Tough-skinned kids: identifying psychosocial effects of psoriasis and helping pediatric patients and families cope. J Pediatr Nurs. 2012;27(5):563–572. doi:10.1016/j.pedn.2011.10.003
22. Salman A, Yucelten AD, Sarac E, Saricam MH, Perdahli-Fis N. Impact of psoriasis in the quality of life of children, adolescents and their families: a cross-sectional study. An Bras Dermatol. 2018;93(6):819–823. doi:10.1590/abd1806-4841.20186981
23. Zhou J, Luo Q, Cheng Y, Wen X, Liu J. An update on genetic basis of generalized pustular psoriasis (Review). Int J Mol Med. 2021;47(6). doi:10.3892/ijmm.2021.4951
24. Trai NN, Van Em D, Van BT, et al. Correlation of IL36RN and CARD14 mutations with clinical manifestations and laboratory findings in patients with generalised pustular psoriasis. Indian J Dermatol Venereol Leprol. 2023;89(3):378–384. doi:10.25259/IJDVL_1054_2021
25. Napolitano M, Megna M, Fabbrocini G, et al. Eczematous eruption during anti-interleukin 17 treatment of psoriasis: an emerging condition. Br J Dermatol. 2019;181(3):604–606. doi:10.1111/bjd.17779
26. Al-Janabi A, Foulkes AC, Mason K, Smith CH, Griffiths CEM, Warren RB. Phenotypic switch to eczema in patients receiving biologics for plaque psoriasis: a systematic review. J Eur Acad Dermatol Venereol. 2020;34(7):1440–1448. doi:10.1111/jdv.16246
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.