")
Back to Journals » Clinical Ophthalmology » Volume 19
Comparing the Effectiveness of Propensity Score-Matched Ab Interno Trabeculotomy Between Two Types of Trabecular Hooks
Authors Nakagawa S , Totsuka K, Chen YN, Okinaga K, Takamoto M, Ishii K
Received 3 October 2024
Accepted for publication 17 February 2025
Published 21 February 2025 Volume 2025:19 Pages 663—671
DOI https://doi.org/10.2147/OPTH.S498940
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Suguru Nakagawa, Kiyohito Totsuka, Yi-Ning Chen, Kimiko Okinaga, Mitsuko Takamoto, Kiyoshi Ishii
Department of Ophthalmology, Saitama Red Cross Hospital, Saitama, Japan
Correspondence: Suguru Nakagawa, Department of Ophthalmology, Saitama Red Cross Hospital, Saitama, Japan, Tel +81-48-852-1111, Email [email protected]
Purpose: This retrospective study compares the surgical outcomes of ab interno trabeculotomy using the Kahook Dual Blade (KDB) and Tanito microhook (TMH) combined with cataract surgery.
Patients and Methods: Twenty-four eyes from 19 and 17 patients with glaucoma in the KDB and TMH groups, respectively, were included. Background factors were matched for medication score and disease type using propensity scores.
Results: Preoperative age, sex, intraocular pressure (IOP), medication scores, and disease type were comparable between the groups. The intraoperative incision range was lower in the KDB than TMH group. The postoperative medication scores and IOPs were 2.7± 1.6 mmHg and 14.5 ± 2.8 mmHg in the KDB group, and 2.0± 1.8 and 13.8 ± 3.4 mmHg in the TMH group, respectively. There were no significant differences between the groups regarding changes in medication scores, IOP reduction rate, or survival 6 months postoperatively. Postoperative IOP changes were significantly associated with preoperative IOP in both groups, and trabeculotomy range in the KDB group. There were no significant between-group differences regarding the incidence of postoperative complications, excluding a higher incidence of hyphema in the TMH group.
Conclusion: Surgical outcomes for ab interno trabeculotomy using the KDB and TMH were not significantly different. There was no significant difference in the occurrence of postoperative complications, except hyphema, which may reflect the difference in the incision range of trabeculotomy between the hooks. Finally, in the KDB group, where narrow incisions range up to just over one quadrant, the trabeculotomy incision range correlated with IOP.
Plain Language Summary: Glaucoma is a leading cause of vision loss. Controlling intraocular pressure (IOP) is crucial to slow the disease. We performed a type of minimally invasive glaucoma surgery called ab interno trabeculotomy using two different hooks—the Kahook Dual Blade and Tanito microhook—combined with cataract surgery. We compared how effectively they lowered IOP and reduced the need for glaucoma medications. Both hooks achieved similar IOP reductions; however, wider incisions may lead to an increased risk of hyphema. Furthermore, the range of trabeculotomy incisions up to just over one quadrant may correlate with IOP. This information may help people with glaucoma and cataracts make informed surgical decisions.
Keywords: ab interno trabeculotomy, Kahook dual blade, minimally invasive glaucoma surgery, propensity score, Tanito ab interno microhook
Introduction
Glaucoma is a leading cause of blindness worldwide.1 Intraocular pressure (IOP) is the only modifiable factor that halts glaucoma progression and should be adequately controlled to prevent visual field deterioration.2–9 As the population ages, procedures that address both cataracts and glaucoma are increasingly important; minimally invasive glaucoma surgery (MIGS) has rapidly evolved to fulfill this need.10
Ab interno trabeculotomy incises the inner trabecular meshwork (TM) and Schlemm’s canal (SC) to facilitate aqueous outflow.11–15 Two commonly used instruments are the Kahook Dual Blade (KDB) and Tanito microhook (TMH).14,15 Retrospective comparisons can be biased regarding differences in baseline IOP, medication use, or glaucoma types; to mitigate this bias, we used propensity score matching to balance medication scores and glaucoma types between the two treatment groups. We aimed to compare the short-term surgical outcomes of ab interno trabeculotomy with KDB vs TMH in patients who underwent concurrent cataract surgery after matching the background factors of medication score and glaucoma types.
Materials and Methods
This study was conducted as part of the “Clinical Study on Induced Astigmatism and Postoperative Outcomes of Minimally Invasive Glaucoma Surgery” research protocol approved by the Institutional Review Board of our hospital, and complied with the tenets of the Declaration of Helsinki. The Ethics Committee waived the need for informed consent for the use of patient’s medical record data in accordance with the provisions of the “Guidelines for Epidemiological Research” issued by the Japanese government. However, the protocol was posted on our hospital’s website to inform the study participants. Only anonymized data were used for the statistical analyses.
Participants
A total of 94 eyes of 62 Japanese patients with glaucoma who underwent ab interno trabeculotomy with KDB or TMH combined with cataract surgery by an ophthalmologist between January 2018 and December 2019 at Saitama Red Cross Hospital and were followed up for ≥6 months were selected. Patients with a history of glaucoma surgery or significant ocular disease were excluded. Propensity score matching was performed among the two groups using logistic regression analysis, and each patient was matched 1:1 based on their preoperative medication score and disease type; the caliper coefficient was set to 0.2. We performed surgery on patients whose progression was not controlled with medication alone and whose cataracts were observed concurrently. These patients were indicated for ab interno trabeculotomy, rather than trabeculectomy, due to their target IOP being in the mid-teens, alongside considerations for their age and other background factors.
Surgical Technique
All patients underwent ultrasonic phacoemulsification using the INFINITY Vision System (Alcon Surgical, Fort Worth, TX, USA) and acrylic intraocular lens insertion through a corneal incision. Trabeculotomy was performed after cataract surgery under gonioscopy (IPRISM; Glaucos Corp., Laguna Hills, CA, USA); KDB or TMH were selected at the surgeon’s discretion. In the KDB group, the KDB was introduced into the anterior chamber, where its pointed tip was engaged with the TM until the heel settled within SC. Subsequently, the KDB was advanced for approximately 3–6 clock hours (nasal and inferior quadrants), and the TM was excised.
A microhook was inserted into the anterior chamber through the corneal incision in the TMH group. Afterward, the tip of the microhook was inserted into SC and moved circumferentially. After 3–8 clock hours (nasal and inferior and temporal quadrants), the inner wall of SC and TM were incised. Postoperatively, antibiotics (moxifloxacin), a corticosteroid (betamethasone sodium phosphate), and miotic medication (pilocarpine hydrochloride) were administered four times daily as eye drops. The drug doses were tapered during the postoperative period. Finally, the surgeon’s recommendation resulted in the readministration of IOP-lowering medications.
Statistical Analysis
The primary endpoints were changes in IOP and medication scores over time, with observation time points at 1, 3 (±2 weeks), and 6 (±4 weeks) months postoperatively. Additionally, the baseline IOP was the final IOP measured preoperatively. Regarding the medication score analysis, the concomitant medication and oral acetazolamide were assigned “2” and “1”, respectively. The routine use of postoperative miotic medications was not considered for IOP reduction.
Baseline clinical numerical factors and postoperative numerical values were compared between the KDB and TMH groups using a linear mixed model, with each patient as a random effect. Linear mixed models were used to adjust for the hierarchical structure of data modeling by grouping measurements in subjects to reduce possible bias from including data from both eyes in one patient.16 Furthermore, the associations between the rate of IOP reduction and preoperative IOP, medication scores, and the extent of trabeculotomy incision were examined using a linear mixed model. Kaplan–Meier survival analysis and Log rank tests were performed to determine whether an IOP reduction of <20%, IOP of >18 mmHg, or additional glaucoma surgery were defined as failures.
All statistical analyses were performed using EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan),17 a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria). Data are reported as the mean ± standard deviation, and statistical significance was set at p<0.05.
Results
Overall, 24 eyes each from 19 and 17 patients with glaucoma in the KDB and TMH group, respectively, were included in the final analysis. Five surgeons performed trabeculotomy with KDB, while three performed surgery with TMH. Table 1 presents the patient background of each group. The preoperative age of the KDB and TMH groups was 70.0 ± 7.4 years and 71.8 ± 11.2 years, respectively, with no significant difference (p=0.54, linear mixed model). The male/female ratio was 15/9 and 16/8 eyes in the KDB and TMH groups, respectively, with no significant difference between groups (p=1.000, generalized linear mixed model). Preoperative medication scores were 4.3 ± 1.2 and 4.5 ± 2.4 in the KDB and TMH groups, respectively (p=0.97, linear mixed model). Preoperative IOP was 19.7 ± 4.7 mmHg and 20.1 ± 7.3 mmHg in the KDB and TMH groups, respectively (p=0.83, linear mixed model). Glaucoma types included 15 primary open-angle glaucoma (POAG), three normal-tension glaucoma (NTG), three pseudoexfoliative glaucoma (PXG), one secondary open-angle glaucoma (SOAG), and two chronic angle closure glaucoma (CACG) cases in the KDB group; and 12 POAG, three NTG, six PXG, one SOAG, and two CACG cases in the TMH group, with no significant difference in prevalence between the two groups (p=0.999, generalized linear mixed model). Furthermore, the intraoperative incision range was significantly lower in the KDB (117.9° ± 24.5°) than TMH (177.5° ± 59.4°; p<0.001, linear mixed model) group.
 |
Table 1 Background Demographics |
Tables 2 and 3 present the changes in IOP and medication scores, respectively. The decrease in IOP from baseline was significant at all time points in both groups (KDB: p<0.001, TMH: p<0.005; Table 2). Similarly, the reduction in medication scores from baseline was significant at all time points in both groups (KDB: p<0.001, TMH: p<0.001; Table 3). However, the change in the IOP reduction rate and medication score from baseline at each time point did not significantly differ between the two groups (linear mixed model).
 |
Table 2 Changes in IOP Over Time |
 |
Table 3 Changes in Medication Score Over Time |
As shown in Table 4, preoperative IOP was significantly associated with the IOP reduction rate in the KDB and TMH groups (coefficients: 3.1 and 3.0, p<0.001 and p<0.001, respectively; linear mixed model). Additionally, the incision range of trabeculotomy was significantly associated with the IOP reduction rate in the KDB group (coefficient: 0.47, p<0.001; linear mixed model), but not in the TMH group (Table 4).
 |
Table 4 Association Between the Percent Change in Intraocular Pressure and Selected Variables |
Based on the Kaplan–Meier survival curve analysis, the probabilities of complete success in the KDB and TMH groups were 62.5% and 58.3%, respectively, at 6 months postoperatively, with no significant between-group difference (p=0.99; Table 5, Figure 1).
 |
Table 5 Survival Rate |
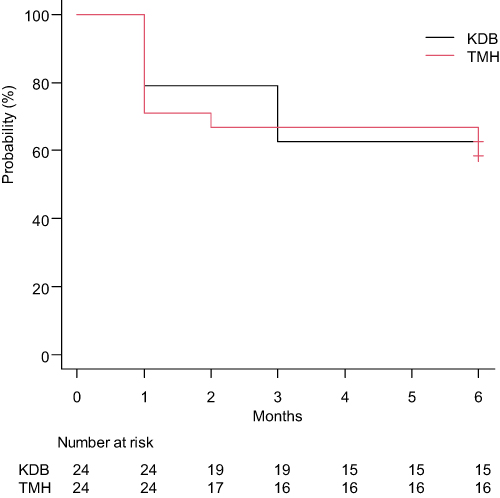 |
Figure 1 Success rate of intraocular pressure control after ab interno trabeculotomy using the KDB or TMH according to survival curve analysis. Surgery failure was defined as an intraocular pressure decrease of <20%, intraocular pressure of >18 mmHg, and additional glaucoma surgery. Black: KDB group; red: TMH group. Abbreviations: KDB, Kahook Dual Blade; TMH, Tanito microhook. |
Table 6 presents the postoperative complications. IOP elevations >25 mmHg were observed in three eyes each in the KDB and TMH groups. Additional filtration surgery was required in one and four eyes in the KDB and TMH groups, respectively. No significant differences were observed between the two types of hooks. Layered anterior chamber hemorrhages were significantly more frequently observed in the TMH than KDB group (4 vs 14 eyes, p=0.00006; generalized linear mixed model).
 |
Table 6 Postoperative Complications |
Discussion
This study compared the surgical outcomes following ab interno trabeculotomy using KDB and TMH (both in 24 eyes). Additionally, the eyes were matched for preoperative medication scores and disease-type background factors using propensity scores. No significant differences were observed in preoperative age, IOP, sex, medication scores, disease type, IOP reduction rate, change in medication scores, or survival between the two groups.
Maheshwari et al18 conducted a prospective, randomized, interventional study comparing TMH and phacoemulsification alone. They reported that 12 months postoperatively, the preoperative IOP in the TMH group decreased from 26.5 mmHg to 12.5 mmHg, while the preoperative IOP in the phacoemulsification alone group decreased from 25.3 mmHg to 20.0 mmHg. Omoto et al19,20 and Aoki et al21 recently reported significant reductions in the postoperative IOP and use of IOP-lowering medications after phacoemulsification and aspiration of the lens with trabeculotomy using KDB or TMH; no significant differences were observed in IOP reduction at the 6- or 12-month follow-up between the two techniques. In our study, IOP significantly decreased from 19.7 mmHg to 14.5 mmHg, and from 20.1 mmHg to 13.8 mmHg in the KDB and TMH groups, respectively, at 6 months postoperatively; however, no significant difference was observed in the IOP reduction rate or changes in medication scores between the two groups. A recent study reported an IOP of 15–16 mmHg at 6 months postoperatively following trabeculotomy with TMH (median medication score of 5).22 The postoperative IOP values in our study were comparable with those reported in previous studies.
Furthermore, the baseline medication scores were higher in both groups in our study compared with those previously reported (2.423 and 1.3524 in the KDB and TMH groups in previous studies, compared with 4.24 and 4.27 in Omoto’s study,20 and 4.3 and 4.5, in this study, respectively). The medication scores decreased significantly compared with baseline and remained under good control for ≥6 months, with no significant difference between the two groups.
Our study demonstrated that the higher the preoperative IOP, the greater the change in postoperative IOP in both the KDB and TMH groups (Table 4). This aligns with several previous studies that used trabeculotomy;25–28 therefore, our study results indicate that the magnitude of IOP reduction would be greater in eyes with a higher preoperative IOP.
In this study, no significant difference in survival at 6 months postoperatively was observed between the two groups. Aoki et al21 reported that at 12 months postoperatively, the criteria (20% reduction in preoperative IOP and IOP >20 mmHg) were 71.8% and 62.2% in the TMH and KDB groups, respectively, with no significant difference between the two groups regarding survival. Additionally, Iwasaki et al29 studied patients with POAG and PXG and reported long-term outcomes in the KDB group; they reported a survival rate of 62.4% at 12 months for the criteria (20% reduction in preoperative IOP, IOP >18 mmHg, or additional glaucoma surgery). Okada et al30 reported survival rates of 70.4% and 48.2% at 12 months in the TMH and KDB groups, respectively, while Tanito et al31 reported a standard survival rate of 44.6% at 12 months postoperatively for 560 eyes in the TMH group (including 28% with TMH ab interno trabeculotomy alone without cataract surgery). Therefore, we believe that our results are justified based on survival rates in both groups.
Rosenquist et al32 reported a gradual decrease in aqueous humor outflow resistance with increasing degrees of incision based on observations in human enucleated eyes; 30°, 120°, and 360° incisions resulted in 30%, 60%, and 71% decreases in IOP, respectively. However, the question of whether IOP decreases gradually with an increasing degree of incision remains controversial. For example, Manabe et al33 examined the effect of the degree of incision (between 150° and 360°) on postoperative IOP and found no significant association. No significant difference in IOP reduction was observed between the 180° and 360° incisions,34 or between the one- and two-quadrant incisions.22 In our study, the KDB and TMH incisions were made at 117.9° ± 24.5°, and a wider angle of 177.5° ± 59.4°, respectively. No significant differences were observed in the postoperative IOP reduction rates or changes in medication scores between the two groups, indicating that a reduction in the incisional area does not affect the postoperative IOP. The rate of IOP reduction did not correlate with the range of trabeculotomy incision in the TMH group; however, the range of trabeculotomy incision (coefficient: 0.47, p=0.001; linear mixed model) significantly correlated with the rate of IOP reduction in the KDB group. Therefore, this finding, combined with those of previous reports, implies that for narrower incisions up to just over one quadrant, the incision range of trabeculotomy correlates with IOP. However, the range of trabeculotomy incision does not correlate with postoperative IOP changes for incisions over one quadrant.
Safety was adequate in both groups in our study; however, the incidence of hyphema in trabeculotomy has been reported to range from 17–50%.22,23,25,26 A previous study reported a significant difference in the frequency of postoperative hyphema between 180° and 360° SC incisions.33 The incidence of hyphema in the KDB and TMH groups was 16.7% and 58.3%, respectively (Table 6), probably owing to the larger incisional extent in the TMH than KDB group.22,26
This study included one (4.2%) and four (16.7%) patients in the KDB and TMH groups, respectively, who underwent additional filtration procedures owing to failure. One patient in the KDB group required an additional filtration procedure 24 months postoperatively, and each patient in the TMH group required additional filtration procedures at 1, 2, 4, and 11 months postoperatively, respectively. Iwasaki et al29 reported that 4.1% of patients in the KDB group required additional glaucoma surgery during a mean follow-up of 31.3 ± 14.8 months. Furthermore, several patients in the TMH group required additional filtration surgery. Unfortunately, the number of participants was reduced owing to the use of propensity scores, and risk factors could not be assessed. However, given the lack of a significant difference in the rate of postoperative IOP reduction, additional surgery may be required in the KDB group if the follow-up period is extended.
This study had several limitations. First, the retrospective nature of our work and discretionary use of KDB or TMH could introduce bias; however, propensity score matching mitigates some of this concern. Second, propensity score matching was employed, thus reducing the number of available cases and potentially introducing variability compared with studies with larger sample sizes. While propensity score matching adjusts for known confounders—those variables deliberately chosen by the authors—it does not mitigate the impact of unknown confounding factors. Third, even after matching the types of disease, there were three more patients with PXG in the TMH group and three fewer patients with POAG; thus, the types of disease did not match perfectly. We performed a subgroup analysis of eyes with PXG and POAG; IOP reduction at 6 months postoperatively was more pronounced in the PXG (KDB: 43%, TMH: 41%) than POAG (KDB: 23%, TMH: 6%, Supplementary Table 1) group, and changes in medication scores at 6 months postoperatively were more pronounced in the PXG (KDB: −3.0, TMH: −4.2) than POAG (KDB: −1.5, TMH: −1.0, Supplementary Table 2) group. These findings align with previous reports suggesting that the PXG group demonstrates a stronger lotomy effect and greater IOP reduction.35,36 However, the small sample size in this study necessitates caution in interpreting these results. The disparity in effects between the PXG and POAG groups within the KDB and TMH subgroups may have influenced the observed outcomes; thus, further prospective randomized clinical trials are necessary to comprehensively address these limitations.
Despite these limitations, our study contributes valuable comparative data on KDB and TMH devices under real-world practice conditions. A recent randomized controlled trial has shown the benefits of combining TMH with phacoemulsification over phacoemulsification alone.18 Thus, future studies with longer follow-up and larger cohorts may clarify whether incision extent should be optimized for individual patient risk profiles.
Conclusion
Ab interno trabeculotomy using KDB or TMH yields significant and similar reductions in IOP and medication scores at 6 months when combined with cataract surgery. Wider incisions may lead to an increased risk of hyphema. Furthermore, as in the KDB group in our study, the extent of trabeculotomy incision up to just over one quadrant may correlate with IOP.
Abbreviations
CACG, chronic angle closure glaucoma; IOP, Intraocular pressure; KDB, Kahook Dual Blade; MIGS, minimally invasive glaucoma surgery; NTG, normal-tension glaucoma; POAG, primary open-angle glaucoma; PXG, pseudoexfoliative glaucoma; SC, Schlemm’s canal; SOAG, secondary open-angle glaucoma; TM, trabecular meshwork; TMH, Tanito microhook.
Data Sharing Statement
The datasets analyzed during the study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Institutional Review Board of our hospital and complied with the tenets of the Declaration of Helsinki. The Ethics Committee waived the need for informed consent for the use of patients’ medical data in accordance with the provisions of the “Guidelines for Epidemiological Research” issued by the Japanese government; however, the protocol was posted on our hospital’s website to inform the study participants.
Acknowledgments
We thank Editage (www.editage.com) for English language editing.
Author Contributions
All authors made a significant contribution to the work reported—whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas—took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Japan Society for the Promotion of Science (JSPS) KAKENHI, Grant Number 19 K18837 (SN). The funding body played no role in the study’s design, data collection, analysis, interpretation, or manuscript writing.
Disclosure
The authors have no relevant financial or non-financial interests to disclose for this work.
References
1. Jayaram H, Kolko M, Friedman DS, Gazzard G. Glaucoma: now and beyond. Lancet. 2023;402(10414):1788–1801. doi:10.1016/S0140-6736(23)01289-8
2. Garway-Heath DF, Crabb DP, Bunce C, et al. Latanoprost for open-angle glaucoma (UKGTS): a randomised, multicentre, placebo-controlled trial. Lancet. 2015;385(9975):1295–1304. doi:10.1016/S0140-6736(14)62111-5
3. Musch DC, Gillespie BW, Lichter PR, Niziol LM, Janz NK, Investigators CS. Visual field progression in the collaborative initial glaucoma treatment study the impact of treatment and other baseline factors. Ophthalmology. 2009;116(2):200–207. doi:10.1016/j.ophtha.2008.08.051
4. Jay J, Murray S. Early trabeculectomy versus conventional management in primary open angle glaucoma. Br J Ophthalmol. 1988;72(12):881–889. doi:10.1136/bjo.72.12.881
5. Holmin C, Thorburn W, Krakau C. Treatment versus no treatment in chronic open angle glaucoma. Acta Ophthalmol. 1988;66(2):170–173. doi:10.1111/j.1755-3768.1988.tb04006.x
6. Heijl A, Leske MC, Bengtsson B, et al. Reduction of intraocular pressure and glaucoma progression: results from the early manifest glaucoma trial. Arch Ophthalmol. 2002;120(10):1268–1279. doi:10.1001/archopht.120.10.1268
7. Chauhan BC, Mikelberg FS, Balaszi AG, et al. Canadian glaucoma study: 2. risk factors for the progression of open-angle glaucoma. Arch Ophthalmol. 2008;126(8):1030–1036. doi:10.1001/archopht.126.8.1030
8. European Glaucoma Prevention Study (EGPS) Group; Miglior S, Pfeiffer N. Predictive factors for open-angle glaucoma among patients with ocular hypertension in the European glaucoma prevention study. Ophthalmology. 2007;114(1):3–9.
9. Gordon MO, Beiser JA, Brandt JD, et al. The ocular hypertension treatment study: baseline factors that predict the onset of primary open-angle glaucoma. Arch Ophthalmol. 2002;120(6):714–720. doi:10.1001/archopht.120.6.714
10. Francis BA, Singh K, Lin SC, et al. Novel glaucoma procedures: a report by the American Academy of Ophthalmology. Ophthalmology. 2011;118(7):1466–1480. doi:10.1016/j.ophtha.2011.03.028
11. Tanihara H, Negi A, Akimoto M, et al. Surgical effects of trabeculotomy ab externo on adult eyes with primary open angle glaucoma and pseudoexfoliation syndrome. Arch Ophthalmol. 1993;111(12):1653–1661. doi:10.1001/archopht.1993.01090120075025
12. Honjo M, Tanihara H, Negi A, et al. Trabeculotomy ab externo, cataract extraction, and intraocular lens implantation: preliminary report. J Cataract Refract Surg. 1996;22(5):601–606. doi:10.1016/S0886-3350(96)80017-4
13. Tanito M, Ohira A, Chihara E. Surgical outcome of combined trabeculotomy and cataract surgery. J Glaucoma. 2001;10(4):302–308. doi:10.1097/00061198-200108000-00010
14. Tanito M, Sano I, Ikeda Y, Fujihara E. Short‐term results of microhook ab interno trabeculotomy, a novel minimally invasive glaucoma surgery in Japanese eyes: initial case series. Acta Ophthalmol. 2017;95(5):e354–e360. doi:10.1111/aos.13288
15. Greenwood MD, Seibold LK, Radcliffe NM, et al. Goniotomy with a single-use dual blade: short-term results. J Cataract Refract Surg. 2017;43(9):1197–1201. doi:10.1016/j.jcrs.2017.06.046
16. Baayen RH, Davidson DJ, Bates DM. Mixed-effects modeling with crossed random effects for subjects and items. J Mem Lang. 2008;59(4):390–412. doi:10.1016/j.jml.2007.12.005
17. Kanda Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013;48(3):452–458. doi:10.1038/bmt.2012.244
18. Maheshwari D, Grover DS, Ramakrishnan R, Pillai MR, Chautani D, Kader MA. Early outcomes of combined phacoemulsification and ab interno tanito microhook trabeculotomy in open-angle glaucoma. Ophthalmol Glaucoma. 2024;7(2):123–130. doi:10.1016/j.ogla.2023.10.007
19. Omoto T, Fujishiro T, Asano-Shimizu K, et al. Comparison of the short-term effectiveness and safety profile of ab interno combined trabeculotomy using 2 types of trabecular hooks. Jpn J Ophthalmol. 2020;64(4):407–413. doi:10.1007/s10384-020-00750-3
20. Omoto T, Fujishiro T, Asano-Shimizu K, et al. Comparison of 12-month surgical outcomes of ab interno trabeculotomy with phacoemulsification between spatula-shaped and dual-blade microhooks. Jpn J Ophthalmol. 2021;65(3):402–408. doi:10.1007/s10384-020-00806-4
21. Aoki R, Hirooka K, Goda E, et al. Comparison of surgical outcomes between microhook ab interno trabeculotomy and goniotomy with the Kahook dual blade in combination with phacoemulsification: a retrospective, comparative case series. Adv Ther. 2021;38(1):329–336. doi:10.1007/s12325-020-01543-3
22. Mori S, Murai Y, Ueda K, et al. Comparison of efficacy and early surgery‐related complications between one‐quadrant and two‐quadrant microhook ab interno trabeculotomy: a propensity score matched study. Acta Ophthalmol. 2021;99(8):898–903. doi:10.1111/aos.14787
23. Tanito M, Ikeda Y, Fujihara E. Effectiveness and safety of combined cataract surgery and microhook ab interno trabeculotomy in Japanese eyes with glaucoma: report of an initial case series. Jpn J Ophthalmol. 2017;61(6):457–464. doi:10.1007/s10384-017-0531-z
24. ElMallah MK, Seibold LK, Kahook MY, et al. 12-month retrospective comparison of kahook dual blade excisional goniotomy with istent trabecular bypass device implantation in glaucomatous eyes at the time of cataract surgery. Adv Ther. 2019;36(9):2515–2527. doi:10.1007/s12325-019-01025-1
25. Sato T, Kawaji T, Hirata A, Mizoguchi T. 360-degree suture trabeculotomy ab interno with phacoemulsification in open-angle glaucoma and coexisting cataract: a pilot study. BMJ Open Ophthalmol. 2018;3(1):e000159. doi:10.1136/bmjophth-2018-000159
26. Okada N, Hirooka K, Onoe H, Murakami Y, Okumichi H, Kiuchi Y. Comparison of efficacy between 120° and 180° Schlemm’s canal incision microhook ab interno trabeculotomy. J Clin Med. 2021;10(14):3181. doi:10.3390/jcm10143181
27. Tanito M, Sugihara K, Tsutsui A, Hara K, Manabe K, Matsuoka Y. Effects of preoperative intraocular pressure level on surgical results of microhook ab interno trabeculotomy. J Clin Med. 2021;10(15):3327. doi:10.3390/jcm10153327
28. Asaoka R, Nakakura S, Mochizuki T, et al. Which is more effective and safer? Comparison of propensity score-matched microhook ab interno trabeculotomy and iStent inject. Ophthalmol Ther. 2023;12(5):2757–2768. doi:10.1007/s40123-023-00777-y
29. Iwasaki K, Kakimoto H, Orii Y, Arimura S, Takamura Y, Inatani M. Long-term outcomes of a Kahook dual blade procedure combined with phacoemulsification in Japanese patients with open-angle glaucoma. J Clin Med. 2022;11(5):1354. doi:10.3390/jcm11051354
30. Okada N, Hirooka K, Onoe H, Okumichi H, Kiuchi Y. Comparison of mid-term outcomes between microhook ab interno trabeculotomy and goniotomy with the Kahook dual blade. J Clin Med. 2023;12(2):558. doi:10.3390/jcm12020558
31. Tanito M, Sugihara K, Tsutsui A, Hara K, Manabe K, Matsuoka Y. Midterm results of microhook ab interno trabeculotomy in initial 560 eyes with glaucoma. J Clin Med. 2021;10(4):814. doi:10.3390/jcm10040814
32. Rosenquist R, Epstein D, Melamed S, Johnson M, Grant WM. Outflow resistance of enucleated human eyes at two different perfusion pressures and different extents of trabeculotomy. Curr Eye Res. 1989;8(12):1233–1240. doi:10.3109/02713688909013902
33. Manabe SI, Sawaguchi S, Hayashi K. The effect of the extent of the incision in the Schlemm canal on the surgical outcomes of suture trabeculotomy for open-angle glaucoma. Jpn J Ophthalmol. 2017;61(1):99–104. doi:10.1007/s10384-016-0487-4
34. Sato T, Kawaji T. 12-month randomised trial of 360° and 180° Schlemm’s canal incisions in suture trabeculotomy ab interno for open-angle glaucoma. Br J Ophthalmol. 2021;105(8):1094–1098. doi:10.1136/bjophthalmol-2020-316624
35. Ting JL, Damji KF, Stiles MC; Trabectome Study Group. Ab interno trabeculectomy: outcomes in exfoliation versus primary open-angle glaucoma. J Cataract Refract Surg. 2012;38(2):315–323. doi:10.1016/j.jcrs.2011.08.043
36. Tanito M, Matsuo M. Ab-interno trabeculotomy-related glaucoma surgeries. Taiwan J Ophthalmol. 2019;9(2):67–71. doi:10.4103/tjo.tjo_38_19
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Kahook Dual Blade versus Trabectome (KVT): Comparing Outcomes in Combination with Cataract Surgery
Fliney GD, Kim E, Sarwana M, Wong S, Tai TYT, Liu J, Sarrafpour S, Chadha N, Teng CC
Clinical Ophthalmology 2023, 17:145-154
Published Date: 10 January 2023