")
Back to Journals » Clinical Ophthalmology » Volume 19
Comparison of IMO vifa24plus(1-2) and Humphrey Field Analyzer 24-2
Authors Takagi Y, Asano R, Yamashita K, Sakai Y, Yokoyama S, Ichikawa K, Ichikawa K
Received 12 November 2024
Accepted for publication 23 January 2025
Published 30 January 2025 Volume 2025:19 Pages 301—307
DOI https://doi.org/10.2147/OPTH.S506059
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yuki Takagi,1,2 Ryo Asano,1,3 Kanna Yamashita,2 Yukihiro Sakai,2 Sho Yokoyama,1 Kei Ichikawa,2 Kazuo Ichikawa2
1Department of Ophthalmology, Japan Community Healthcare Organization Chukyo Hospital, Nagoya, Aichi, Japan; 2Chukyo Eye Clinic, Nagoya, Aichi, Japan; 3Asano Eye Clinic, Nagoya, Aichi, Japan
Correspondence: Yuki Takagi, Department of Ophthalmology, Japan Community Healthcare Organization Chukyo Hospital, 1-1-10 Sanjo Minami-ku, Nagoya, Aichi, Japan, Tel +81-52-691-7151, Fax +81-52-692-5220, Email [email protected]
Purpose: This study aimed to compare the results of the IMO vifa 24plus(1– 2) and HFA 24– 2 visual field tests.
Patients and Methods: We included 52 patients (104 eyes) with glaucoma who visited Chukyo Eye Clinic between June 2023 and March 2024. On the same day, the HFA 24– 2 test using the Swedish Interactive Threshold Algorithm Standard and the IMO vifa 24plus(1– 2) test using the Ambient Interactive Zippy Estimated strategy were performed. A Wilcoxon signed-rank test was used to compare fixation, false positives, false negatives, and total test time for both eyes between the HFA and IMO vifa tests. Only eyes with reliable test results were selected, and the visual field index (VFI), mean deviation (MD), and pattern standard deviation (PSD) were examined using Spearman’s rank correlation coefficient and the Wilcoxon signed-rank test.
Results: The test times for the HFA 24– 2 and IMO vifa 24plus(1– 2) were 716.83± 118.80 and 628.75± 142.70 s, respectively, with the IMO vifa being significantly shorter (P< 0.001). For fixation, the results were 15.85± 16.57% and 11.09± 15.20%, with significantly better fixation in the IMO vifa (P< 0.0001). False positives and negatives were 4.52± 5.19 / 4.14± 6.85% and 4.97± 7.99 / 5.47± 7.86%, respectively, with no significant differences, though the IMO vifa showed a slightly higher trend (P=0.980, 0.056). In eyes with reliable results, the HFA 24– 2 and IMO vifa 24plus(1– 2) outcomes were as follows: MD (− 6.45± 7.23, − 6.85± 7.35, P=0.724), PSD (7.13± 4.75, 7.49± 4.87, P=0.061), VFI (80.86± 21.61, 80.86± 21.74, P=0.644). The Spearman rank correlation coefficients between the HFA 24– 2 and IMO vifa 24plus(1– 2) were MD: 0.938, PSD: 0.949, VFI: 0.932 (all P< 0.001).
Conclusion: The IMO vifa demonstrates a very high correlation with HFA and allows for a shorter examination time. Fixation errors are significantly improved compared to HFA, while there is no significant difference in false positives or false negatives.
Keywords: glaucoma, visual field test, IMO vifa 24plus(1-2), HFA 24-2
Introduction
Glaucoma is known to be one of the diseases that can lead to blindness,1 and it is expected to increase globally in the future.2 Visual field tests are essential in the diagnosis and treatment of glaucoma.3 Visual field tests are divided into dynamic visual field tests, which use the Goldmann perimeter and static visual field analyzers, with the Humphrey Field Analyzer (HFA) (Carl Zeiss Meditec, Dublin, CA, USA) being a representative example. HFA is a primary tool for functional testing;4 however, in Japan, other static perimeters, such as OCTOPUS (HAAG-STREIT, Köniz, Switzerland), AP7700 (Kowa, Nagoya, Japan), and IMO/IMO visual function analyzer (IMO-vifa) (CREWT Medical Systems, Tokyo, Japan) are also commonly used.
The IMO is a head-mounted perimeter and has a different design compared to stationary perimeters, such as the HFA. The IMO is a visual field analyzer known for its ability to perform tests with both eyes open and without occlusion. It has shown a high correlation with the visual field test results of the HFA and can be conducted in a shorter time than the HFA.5–8 Additionally, it can perform a binocular random single-eye test, which allows simultaneous testing of the visual fields of both eyes by presenting visual targets randomly to the left or right under binocular open conditions. This test condition is reported to have high reproducibility, similar to the monocular testing performed with the HFA.9 In the binocular random single-eye test, the subject cannot identify the eye being tested, suggesting its potential usefulness in diagnosing psychogenic visual field defects and malingering.10,11
The IMO vifa (Figure 1) is an improved model of the IMO, featuring a design where VR goggle-like equipment is mounted in a stationary position. This modified setup requires the patient to lean slightly forward to look into the device for visual field testing. The ability to perform visual field testing under binocular open conditions, as well as perform the binocular random single-eye test, has been retained. A report on the IMO vifa compared the IMO vifa 24–2 Ambient Interactive Zippy Estimated (AIZE)-Rapid with the HFA 24–2 Swedish Interactive Threshold Algorithm (SITA)-Faster, finding a high correlation in mean deviation (MD) values and a shorter testing time with the IMO vifa.8 However, no reports have compared fixation, false positives, or false negatives between the IMO vifa and HFA tests.
 |
Figure 1 Appearance of IMO vifa. The IMO vifa is a VR goggle-like stationary device where the examinee leans slightly forward to look into the equipment for testing. |
In both the IMO and IMO vifa, a testing condition called 24plus(1–2) has been developed, which adds test points within the central 10°, similar to the 24–2c in the HFA. A study comparing the IMO 24plus(1–2) with the HFA 30–2 reported a high correlation in outcomes, such as MD values.7 however, there are no previous reports comparing the IMO vifa 24plus(1–2) with the HFA. Additionally, even including the IMO, there have been no reports comparing 24plus(1–2) with 24–2. Therefore, we conducted a comparative study of the IMO vifa 24plus(1–2) and HFA 24–2.
Materials and Methods
Participants
This cross-sectional study included patients who visited the glaucoma clinic at Chukyo Eye Clinic between June 2023 and March 2024. The study was approved by the Ethics Committee of Chukyo Eye Clinic (approval no.: 20230530052) and conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants after providing an explanation in writing.
Participants were aged ≥20 years, with a history of multiple visual field tests, diagnosed with glaucoma or preperimetric glaucoma. The diagnosis of glaucoma and preperimetric glaucoma was made based on the following criteria: glaucomatous optic nerve changes observed on fundus photography and optical coherence tomography (Cirrus, Carl Zeiss Meditec, Dublin, CA, USA), including a horizontal C/D ratio of ≥0.7, notching of the rim, a rim width of ≤0.1, and defects in the retinal nerve fiber layer. Cases were classified as glaucoma if they exhibited corresponding glaucomatous visual field defects in the 24–2 SITA Standard using the HFA. The severity of glaucoma was classified as follows: preperimetric glaucoma with no visual field defects, mild glaucoma with an MD value greater than −4 dB, moderate glaucoma with an MD value between −4 and −12 dB, and severe glaucoma with an MD value less than −12 dB. No exclusion criteria were applied based on disease stage, glaucoma type, refractive error, or corrected visual acuity, although cases with other diseases causing visual field abnormalities (such as optic neuritis, retinal disease, intracranial disease, or psychogenic disorders) were excluded.
Visual Field Tests
Visual field testing was performed on consenting patients on the same day using the HFA 24–2 SITA Standard and the IMO vifa 24plus(1–2) AIZE. For the HFA test, the non-tested eye was covered, and monocular visual field testing was performed. For the IMO vifa 24plus(1–2), the binocular random single-eye test was performed under binocular open conditions, without covering either eye.
Statistical Analysis
First, a Wilcoxon signed-rank test was performed across all cases to compare fixation, false positives, false negatives, and the total testing time for both eyes between the HFA and IMO vifa. Next, cases with fixation loss >20%, false positives, or false negatives >33% were excluded as unreliable visual field tests. For the remaining cases, the visual field index (VFI), MD values, pattern standard deviation (PSD), and foveal threshold (FT) were analyzed using Spearman’s rank correlation coefficient and the Wilcoxon signed-rank test. VFI, MD, and PSD values were analyzed using Bland–Altman analysis. Additionally, a power analysis was conducted for the primary outcome measures, including MD, PSD, VFI, FT, testing time, false positive rate, and false negative rate, using a paired sample t-test design. All statistical analyses were performed using SPSS (version 29.0; IBM Corp., Armonk, NY, USA), with a significance level of P<0.05.
Results
This study included 52 patients (104 eyes), comprising 23 males and 29 females. The clinical characteristics of the patients are presented in Table 1.
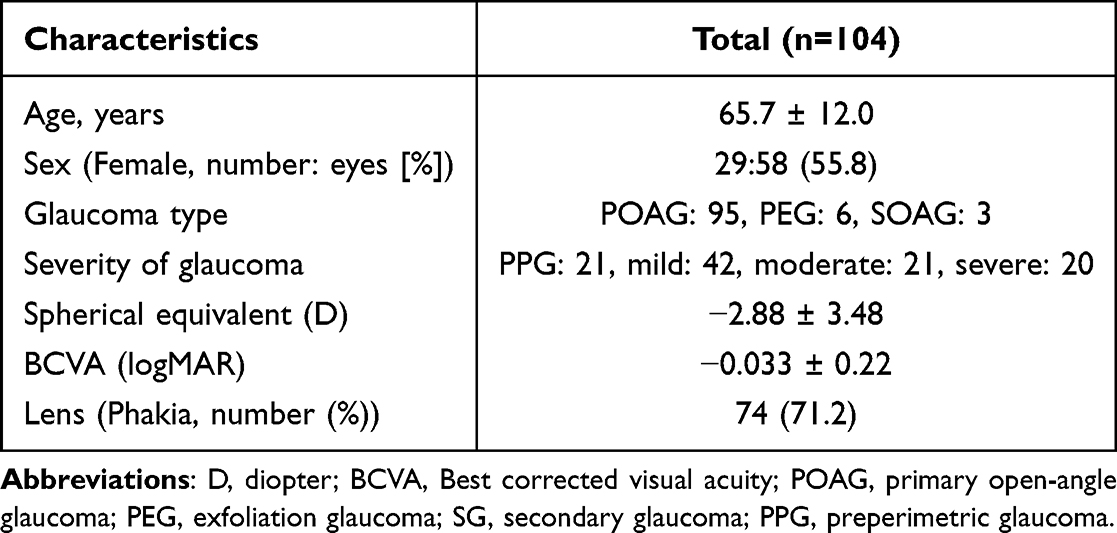 |
Table 1 Clinical Characteristics of All Cases |
The measurement time for both eyes for HFA 24–2 was significantly longer than that of IMO vifa24plus(1–2) (716.83±118.80 s vs 628.75±142.70 s; P<0.001). IMO vifa demonstrated significantly higher fixation values than HFA 24–2 (15.85±16.57% vs 11.09±15.20%; P<0.0001) (Table 2). The HFA 24–2 had false positive and false negative rates of 4.52±5.19% and 4.14±6.85%, respectively, while the IMO VIFA 24plus(1–2) had rates of 4.97±7.99% and 5.47±7.86%. No significant differences were observed between the groups (P=0.980 and 0.056).
 |
Table 2 Comparison Between IMO Vifa 24plus(1–2) and Humphrey Field Analyzer 24–2 for All Cases |
Forty cases (63 eyes) with reliable visual field test results were selected (Table 3). The results of the HFA 24–2 and IMO vifa 24plus(1–2) were as follows: MD (−6.45±7.23, −6.85±7.35, P=0.724), PSD (7.13±4.75, 7.49±4.87, P=0.061), VFI (80.86±21.61, 80.86±21.74, P=0.644), and FT (34.53±4.57, 30.51±9.24, P<0.001). The Spearman rank correlation coefficients between HFA 24–2 and IMO vifa 24plus(1–2) were as follows: MD: 0.938, PSD: 0.949, VFI: 0.932 (all P<0.001), and FT: 0.536 (P<0.001) (Table 4). Scatter plots for MD, PSD, and VFI between HFA 24–2 and IMO vifa 24plus(1–2) (Figure 2A–C) and the results of the Bland–Altman analysis (Figure 3A–C) showed no significant fixed or proportional bias.
 |
Table 3 Clinical Characteristics of Eyes With High Confidence |
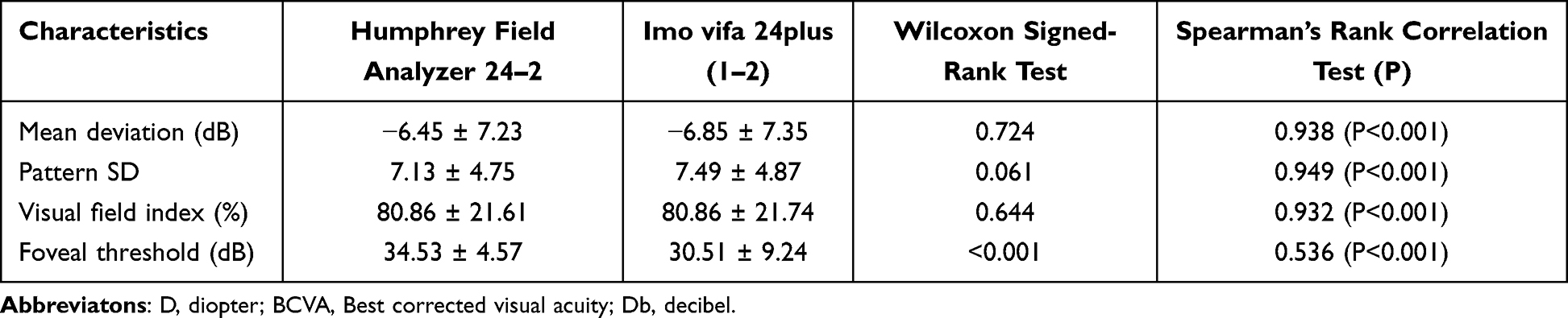 |
Table 4 Comparison of the Imo Vifa 24plus(1–2) and the Humphrey Field Analyzer 24–2 for Eyes With Good Confidence |
 |
Figure 2 Scatter plots comparing IMO vifa and HFA. (A) MD (r=0.938, P<0.001), (B) PSD (r=0.949, P<0.001) and (C) VFI (r=0.932, P<0.001) each showed a significantly positive and strong correlation. |
 |
Figure 3 Bland–Altman diagram with mean difference and agreement limits (including 95% of all difference values). (A) MD, (B) PSD, and (C) VFI did not show any clear fixed or proportional bias. |
The calculated effect sizes (Cohen’s d) and corresponding statistical power values were as follows: MD: effect size = 0.055, power = 8.6%; PSD: effect size = 0.076, power = 11.9%; VFI: effect size = 0.0, power = 5.0%; FT: effect size = 0.88, power = 100%; testing time: effect size = 0.74, power = 100%; false positive rate: effect size = 0.087, power = 14.1%; false negative rate: effect size = 0.194, power = 50.1%.
Discussion
Several studies have compared the visual field test results of the HFA with those of the IMO and IMO vifa.5–9 Although test conditions and equipment vary, all reports indicate significantly shorter testing times with the IMO and IMO vifa. However, in these studies, the number of test points was matched between the HFA and IMO/IMO vifa. For example, previous studies compared the HFA 30–2 (78 test points) with IMO 24plus(1–2) (78 test points) 7 and the HFA 24–2 (54 test points) with IMO vifa 24–2,8 reporting a 30–40% reduction in test time with the IMO/IMO vifa. This reduction is attributed to the AIZE algorithm, unique to IMO. In our study, the IMO vifa 24plus(1–2) had 78 test points compared to 54 in the HFA 24–2, resulting in a condition with more test points for the IMO vifa. Despite this, visual field testing with the IMO vifa still completed significantly faster, approximately 12% shorter. Although this time reduction is lower than that in previous reports,7,8 the results suggest that the IMO/IMO vifa can still achieve shorter test durations, even with more test points than the HFA, possibly due to the AIZE algorithm.
In the present study, there was no significant difference between the IMO vifa and HFA in terms of false positives and negatives, although the IMO vifa showed slightly higher results. Previous studies comparing the HFA and IMO reported significantly higher false positives and negatives with the IMO;7 our study demonstrated a similar trend, though without significant differences. Although the same criteria for false positives and negatives are applied to both the IMO and IMO vifa, no significant difference was observed when compared with the HFA in the present study. One possible explanation for this is the difference in equipment design between the IMO and IMO vifa. The IMO vifa allows visual field testing by looking into VR goggle-like equipment in a slightly forward-leaning position, with contact only around the eyes. In contrast, the IMO is head-mounted, covering from the face to the top of the head, resulting in a larger contact area and a weight of 1.8 kg, which applies pressure to the patient’s head. Thus, the IMO vifa possibly provides less sense of pressure and less burden during testing, which may affect the rate of false positives and negatives. However, as there is no direct comparison between the IMO and IMO vifa, further study is required to investigate this impact.
In the present study, the rate of fixation loss during visual field testing with the IMO vifa was significantly lower compared to the HFA. Previous studies reported either no significant difference in fixation loss7 or a significant reduction in fixation loss with the IMO.12 The presence of eye-tracking functionality in both the IMO and IMO vifa may contribute to the reduced fixation loss observed compared to the HFA. Additionally, since the study used the IMO,7 the difference in equipment design between the IMO and IMO vifa may also be a contributing factor.
Previous studies comparing HFA 30–2 with IMO 30–2 and HFA 24–2 with IMO 24–2 have all demonstrated a high correlation in MD and VFI.5,6 Another study comparing IMO vifa 24–2 with HFA 24–2 also demonstrated a high correlation with no significant differences.8 Our study compared HFA 24–2 with IMO vifa 24plus(1–2), which differs in conditions from previous studies; however, MD and VFI still showed a high correlation, similar to previous findings. These results suggest that, although the IMO vifa has a different design from the IMO, it still shows a high correlation with the HFA, similar to the IMO.
The 24plus(1–2) test condition includes additional test points within the central 10° compared to 24–2; nevertheless, the present study demonstrated a high correlation with no significant differences. Bland–Altman analysis also indicated no fixed or proportional bias. Although conditions differ, a comparison of HFA 30–2 and IMO 24plus(1–2) similarly showed no significant differences.7 Thus, the impact of the additional test points within the central 10° in the 24plus(1–2) condition on MD and VFI is possibly limited.
For PSD, previous studies reported significant differences.8 Although our study did not find significant differences, the difference between HFA and IMO vifa for PSD tended to be greater than that for MD or VFI. Therefore, while our study used the 24plus(1–2) condition, unlike previous studies, the tendency for a larger difference in PSD with IMO vifa may still be observed. The lack of significance in our study could be due to the smaller sample size compared to previous studies. However, as other studies did not mention PSD,5–7 further research is required to evaluate the impact of differences between the IMO and IMO vifa, as well as between 24–2 and 24plus(1–2), on PSD.
In the present study, the correlation for the FT was moderate, unlike that of MD, and showed a significant difference compared to the HFA. Previous studies also reported a significant difference.8 This may be due to the open binocular condition used with the IMO and IMO vifa and the impact of the binocular random single-eye test. Several reports indicate that binocular open conditions and the binocular random single-eye test differ in sensitivity compared to monocular occlusion and single-eye testing.13–16 In particular, Kumagai et al classified eyes into Better Eye and Worse Eye groups based on visual acuity and FT and compared the visual sensitivity at the fovea and central four points between the monocular test and binocular random single-eye test using the IMO.14 Their results showed that in the Better Eye group, visual sensitivity was better in the binocular random single-eye test than in the monocular test, while it was worse in the Worse Eye group. Thus, the central visual field, particularly the FT, may be more influenced by the open binocular condition and the binocular random single-eye test. Based on these previous reports and our study’s findings, it can be inferred that, despite differences in device design, both the IMO and IMO vifa are similarly affected by the open binocular condition and the sensitivity influence of the binocular random single-eye test. Therefore, in cases where there is a significant discrepancy in FT between the HFA and IMO vifa, the open binocular condition and the binocular random single-eye test may be unsuitable It is recommended to conduct the test with monocular occlusion or to consider using a conventional visual field analyzer such as the HFA.
A limitation of this study is the relatively small sample size of 104 eyes. Although the power analysis demonstrated sufficient statistical power for several primary outcomes, some variables, such as MD and PSD, exhibited lower power. This limitation highlights the need for further studies with larger sample sizes to ensure robust conclusions for all measured parameters. Additionally, a direct comparison between the IMO and IMO vifa was not performed. Therefore, to evaluate the impact of device design alone, a direct comparison under standardized conditions would be necessary.
Conclusion
The IMO vifa demonstrates a very high correlation with HFA and permits a shorter examination time. The fixation errors are significantly improved compared to HFA, while there is no significant difference in false positives or false negatives. Additionally, although the IMO vifa 24plus(1–2) has more test points than the HFA 24–2, it still allows for shorter testing times.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grants from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
Dr Kazuo Ichikawa reports personal fees from Carl Zeiss Meditec, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Weinreb RN, Aung T, Medeiros FA. The pathophysiology and treatment of glaucoma: a review. JAMA. 2014;311(18):1901–1911. doi:10.1001/jama.2014.3192
2. Tham YC, Li X, Wong TY, Quigley HA, Aung T, Cheng CY. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081–2090. doi:10.1016/j.ophtha.2014.05.013
3. Heijl A, Leske MC, Bengtsson B, et al. Measuring visual field progression in the early manifest glaucoma trial. Acta Ophthalmol Scand. 2003;81(3):286–293. doi:10.1034/j.1600-0420.2003.00070.x
4. Johnson CA, Wall M, Thompson HS. A history of perimetry and visual field testing. Optom Vis Sci. 2011;88:E8–E15.
5. Matsumoto C, Yamao S, Nomoto H, et al. Visual Field Testing with Head-Mounted Perimeter ‘imo’. PLoS One. 2016;11:e0161974.
6. Nakai Y, Bessho K, Shono Y, Taoka K, Nakai Y. Comparison of imo and Humphrey field analyzer perimeters in glaucomatous eyes. Int J Ophthalmol. 2021;14(12):1882–1887. doi:10.18240/ijo.2021.12.11
7. Kimura T, Matsumoto C, Nomoto H. Comparison of head-mounted perimeter (imo®) and Humphrey Field Analyzer. Clin Ophthalmol. 2019;13:501–513. doi:10.2147/OPTH.S190995
8. Nishida T, Eslani M, Weinreb RN, et al. Perimetric comparison between the IMOvifa and Humphrey Field analyzer. J Glaucoma. 2023;32(2):85–92. doi:10.1097/IJG.0000000000002134
9. Toyokuni H, Sakamoto M, Ueda K, Kurimoto T, Yamada-Nakanishi Y, Nakamura M. Test-retest repeatability of the imo binocular random single-eye test and Humphrey monocular test in patients with glaucoma. Jpn J Ophthalmol. 2023;67(5):578–589. doi:10.1007/s10384-023-01007-5
10. Goseki T, Ishikawa H, Shoji N. Bilateral concurrent eye examination with a head-mounted perimeter for diagnosing functional visual loss. Neuro-ophthalmology. 2016;40(6):281–285. doi:10.1080/01658107.2016.1220593
11. Takagi Y, Yokoyama S, Yokoyama Y, Hozumi K, Kaga T. A case of functional visual loss diagnosed through bilateral randomized visual field testing with a trick method. Am J Ophthalmol Case Rep. 2023;32:101877. doi:10.1016/j.ajoc.2023.101877
12. Goukon H, Hirasawa K, Kasahara M, Matsumura K, Shoji N. Comparison of Humphrey Field Analyzer and imo visual field test results in patients with glaucoma and pseudo-fixation loss. PLoS One. 2019;14:e0224711.
13. Mine I, Shoji T, Kumagai T, Yoshikawa Y, Kosaka A, Shinoda K. Central visual field sensitivity with and without background light given to the nontested fellow eye in glaucoma patients. J Glaucoma. 2021;30(6):537–544. doi:10.1097/IJG.0000000000001764
14. Kumagai T, Shoji T, Yoshikawa Y, et al. Comparison of central visual sensitivity between monocular and binocular testing in advanced glaucoma patients using imo perimetry. Br J Ophthalmol. 2020;104(11):1258–1534. doi:10.1136/bjophthalmol-2019-315251
15. Wakayama A, Matsumoto C, Ayato Y, Shimomura Y. Comparison of monocular sensitivities measured with and without occlusion using the head-mounted perimeter imo. PLoS One. 2019;14:e0210691.
16. Wakayama A, Nomoto H, Chiba Y, Matsumoto C, Kusaka S. Effect of sensitivity disparity between the two eyes on pointwise monocular sensitivity under binocular viewing in patients with glaucoma. J Glaucoma. 2021;30(1):37–43. doi:10.1097/IJG.0000000000001675
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.