")
Back to Journals » Clinical Ophthalmology » Volume 19
Comparison of Normal Tension Glaucoma and Preperimetric Glaucoma and Changes in Medication Use: A Multicenter Survey in Japan
Authors Inoue K, Kunimatsu-Sanuki S, Tomita G , Ishida K
Received 17 January 2025
Accepted for publication 8 May 2025
Published 5 June 2025 Volume 2025:19 Pages 1805—1816
DOI https://doi.org/10.2147/OPTH.S518111
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Kenji Inoue,1 Shiho Kunimatsu-Sanuki,2 Goji Tomita,1,3 Kyoko Ishida3
1Inouye Eye Hospital, Chiyoda-Ku, Tokyo, Japan; 2Nishikasai Inouye Eye Hospital, Edogawa-Ku, Tokyo, Japan; 3Department of Ophthalmology, Toho University Ohashi Medical Center, Meguro-Ku, Tokyo, Japan
Correspondence: Kenji Inoue, Inouye Eye Hospital, 4-3 Kanda-surugadai, Chiyoda-Ku, Tokyo, 101-0062, Japan, Tel +813-3295-0911, Fax +813-3295-0917, Email [email protected]
Purpose: This study aimed to compare clinical characteristics and treatment patterns between patients with normal tension glaucoma (NTG) and preperimetric glaucoma (PPG), assess medication trends over time, and benchmark these against a 2020 study to inform treatment strategies.
Materials and Methods: During March 10– 16, 2024, 6323 outpatients diagnosed with glaucoma or ocular hypertension were enrolled in a survey conducted across 82 private practices. We compared patient characteristics and medication usage between those with NTG and PPG.
Results: Among the enrolled patients, 2882 were diagnosed with NTG, and 344 were diagnosed with PPG. The average age was significantly lower in the PPG group (60.2 ± 14.3 years) than in the NTG group (69.0 ± 12.9 years, P < 0.0001). The average number of medications used was significantly higher for the NTG group (1.7 ± 1.1 drugs) than for the PPG group (0.4 ± 0.7 drugs; P < 0.0001). Monotherapy was used in 1473 patients with NTG and 96 patients with PPG. The most prescribed medications were prostanoid FP receptor agonist (FP agonists) (61.6% and 47.9% for NTG and PPG, respectively), β-adrenergic blockers (β-blockers) (18.3% and 27.1% for NTG and PPG, respectively), and prostanoid EP2 receptor agonist (EP2 agonists) (12.4% and 14.6% for NTG and PPG, respectively). FP agonist prescriptions were significantly more common in patients with NTG than in patients with PPG (P < 0.05). β-blockers and ion channel opener prescriptions were significantly more common in patients with PPG than in patients with NTG (P < 0.05). FP/β fixed-combination eye drops were the most prescribed treatment for both groups. These were used in 399 patients with NTG and 10 patients with PPG.
Conclusion: NTG was more prevalent than PPG in this population. Patients with PPG were significantly younger and required fewer medications compared to those with NTG.
Keywords: normal-tension glaucoma, preperimetric glaucoma, medication, multicenter survey, monotherapy
Introduction
The fifth edition of the Guidelines for the Clinical Practice of Glaucoma defines preperimetric glaucoma (PPG) as
A condition involving abnormalities suggestive of glaucoma, such as glaucomatous optic nerve head and retinal nerve fiber defects on ophthalmoscopy and optical coherence tomography, but no visual field defects are seen on conventional automated static perimetry test.1
Structural and electrophysiological differences between PPG and normal eyes or normal tension glaucoma (NTG) have been frequently reported.2–5 However, reports on treatment approaches for PPG are limited.6,7
Since 2007, we have conducted multicenter surveys of patients with glaucoma to better understand their treatment.8–10 The sixth survey, conducted in 2024, introduced PPG as a glaucoma subtype for the first time. Previous surveys focused on examining differences in the clinical characteristics and treatment conditions of patients with primary open-angle glaucoma (POAG) and NTG.8 However, with the inclusion of PPG as a target disease subtype, we analyzed differences in the clinical profiles of patients with NTG and PPG. Additionally, the treatment status of patients with NTG was compared with findings from a previous survey.8
Materials and Methods
Institutions employing ophthalmologists previously affiliated with the Inouye Eye Hospital Group, as well as institutions collaborating with our hospital, were invited to participate in the survey. The survey was conducted across 82 participating institutions (Table 1) during March 10–16, 2024. All outpatients diagnosed with glaucoma or ocular hypertension during this study period were included. The total number of patients was 6323 (one eye each). Diagnoses and treatments were performed at the discretion of the attending physician, in accordance with the fifth edition of the Guidelines for the Clinical Practice of Glaucoma.1 The investigation included the affected eye of patients with unilateral glaucoma or ocular hypertension and included the right eye for bilateral cases. The right eye was selected owing to the multicenter nature of the study, which reduced the burden of randomization on the attending physicians. The study protocol was approved by the Ethics Committee of Inouye Eye Hospital (approval number: 202402-1) and adhered to the tenets of the Declaration of Helsinki. The committee waived the requirement for written informed consent owing to the study’s retrospective design. However, the institutions provided the study information to participants, and the participants had the opportunity to opt out of the study.
 |
Table 1 The 82 Institutions Participating in the 2024 Survey |
The survey was conducted using a questionnaire (Figure 1). The questionnaires were distributed to each participating institution in advance. Patient data, including age, sex, diagnosis, number and type of medications used, and history of laser treatment or surgery for glaucoma at the time of consultation, were collected from medical records. Data aggregation was performed at the Inouye Eye Hospital. From aggregated data, age, sex, and previous history of surgery for glaucoma or laser treatment of patients with NTG and PPG were compared. Similarly, the number of drugs used and the breakdown of single- and two-medication use was compared. Additionally, data from the NTG group, including the number of cases, sex, age, and history of surgery for glaucoma or laser treatment, were compared with findings from the previous survey conducted in 2020.8 Historical data were derived from results obtained from the Fifth survey, performed during March 8–14, 2020.8 Seventy-eight institutes participated in that survey, including 5303 patients (one eye each).
 |
Figure 1 Sixth multicenter survey of patients with glaucoma. Abbreviations: POAG, primary open-angle glaucoma; NTG, normal-tension glaucoma; PPG, preperimetric glaucoma; PACG, primary angle closure glaucoma; LI, laser iridotomy; SLT, selective laser trabeculoplasty; CAI, carbonic anhydrase inhibitor; ROCK inhibitor, Rho-associated coiled-coil kinase. |
NTG was defined as
A subtype of POAG (broad) in which the intraocular pressure (IOP) always remains within the statistically determined normal range during the developmental process of glaucomatous optic neuropathy.1
PPG was defined as described in the Introduction:
A condition in which the patient has abnormalities suggestive of glaucoma, such as glaucomatous optic nerve papillae or retinal nerve fiber deficits on fundoscopy or optical coherence tomography, but no visual field defects on conventional automated static perimetry testing.1
Fixed-combination eye drops were analyzed as two medications. Drugs were collected under their generic names.
For statistical analyses, the χ2 and Fisher’s exact tests were used to compare glaucoma subtypes and medication usage. Fisher’s exact test was used to analyze sex and patient history of surgery and laser treatment, while the Mann–Whitney U-test was used to compare age and number of medications. Yate’s continuity correction was applied to the χ2 test where appropriate. All statistical analyses were performed using IBM SPSS Statistics for Windows version 22 (IBM Corp., Armonk, NY, USA). Statistical significance was set at P-value < 0.05.
Results
Results of This Survey: Comparison of Clinical Characteristics between NTG and PPG
Comparison of Patient Characteristics between the NTG and PPG Groups
The overall survey data (Table 2) included 2882 patients with NTG (45.6%), 2090 patients with POAG (33.1%), 492 secondary patients with glaucoma (7.8%), 344 patients with PPG (5.4%), and 280 patients with ocular hypertension (4.4%). There were 1191 men and 1691 women in the NTG group and 140 men and 204 women in the PPG group, with no significant difference in sex distribution between the two groups (P = 0.91). The mean age was 69.0 ± 12.9 years (mean ± standard deviation) and 60.2 ± 14.3 years in the NTG and PPG groups, respectively, and patients with PPG were significantly younger (P < 0.0001). The percentage of patients with history of laser treatment was significantly higher in the NTG group (2.1%; 61 patients) than in the PPG group (0.0%; 0 patients) (P < 0.0001). Similarly, 109 patients with NTG (3.8%) had a history of surgery, compared to 0 patient with PPG (P < 0.0001).
 |
Table 2 Comparison of Characteristics between Patients with NTG and PPG |
Comparison of Medications between the NTG and PPG Groups
The average number of medications used was significantly higher in the NTG group (1.7 ± 1.1) than in the PPG group (0.4 ± 0.7, P < 0.0001). PPG was significantly more common among patients using no medication (P < 0.0001), whereas NTG was significantly more common among those requiring 1–7 medications (P < 0.0001) (Figure 2).
 |
Figure 2 Comparison of medications between the NTG and PPG groups. χ2 test, Fisher’s direct method **P < 0.001. |
Monotherapy Medication Use in the NTG and PPG Groups
FP receptor agonists (FP agonists) were the most used monotherapy for both NTG and PPG, with significantly higher usage in patients with NTG (61.6%, 907 patients) than in patients with PPG (47.9%, 46 patients) (P < 0.05) (Figure 3). β-Blockers were the second most frequently used medication, with significantly higher usage in patients with NTG (18.3%, 270 patients) than in patients with PPG (27.1%, 26 patients) (P < 0.05). Other ion channel openers were prescribed in 34 patients with NTG (2.3%) and 7 patients with PPG (7.3%), with significantly greater usage in patients with PPG (P < 0.01). Other medications were comparable between the two groups.
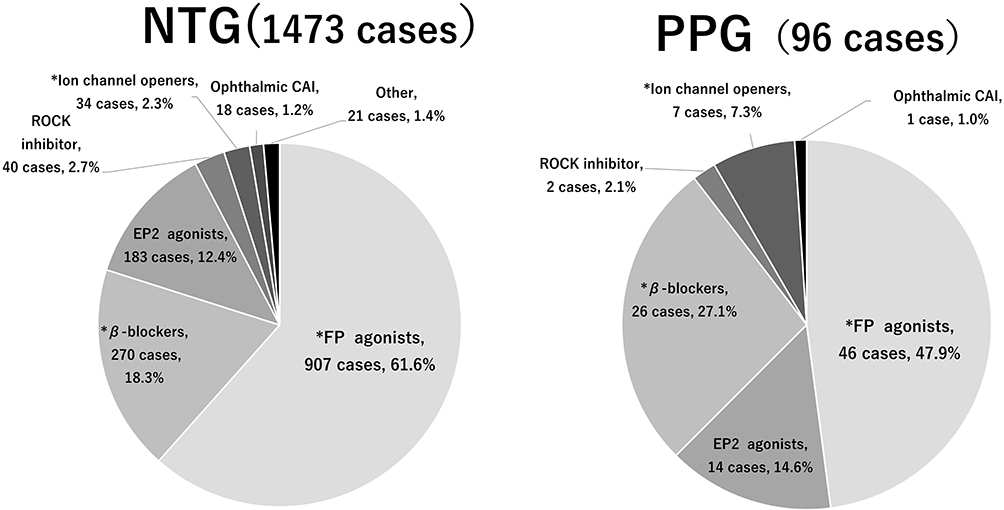 |
Figure 3 Monotherapy drugs used in patients with NTG and PPG. χ2 test, Fisher’s direct method *P < 0.05. Abbreviations: FP agonists, FP receptor agonists; EP2 agonists, EP2 receptor agonists; CAI, carbonic anhydrase inhibitor; ROCK inhibitor, Rho-associated coiled-coil kinase. |
Comparison of Drugs Used as Monotherapy in the NTG and PPG Groups
Latanoprost, an FP agonist, was the most used medication in the NTG group (40.8%, 601 patients) and PPG group (33.3%, 32 patients) (Figure 4). Tafluprost, another FP agonist, was the second most common medication in the NTG group (13.8%, 203 patients), while omidenepag isopropyl, an EP2 receptor agonist (EP2 agonist), was the second most common medication in the PPG group (14.6%, 14 patients). Patients with PPG (18.8%, 18 patients) had significantly greater usage of long-acting carteolol hydrochloride, a β-blocker, than patients with NTG (10.8%, 159 patients) (P < 0.01).
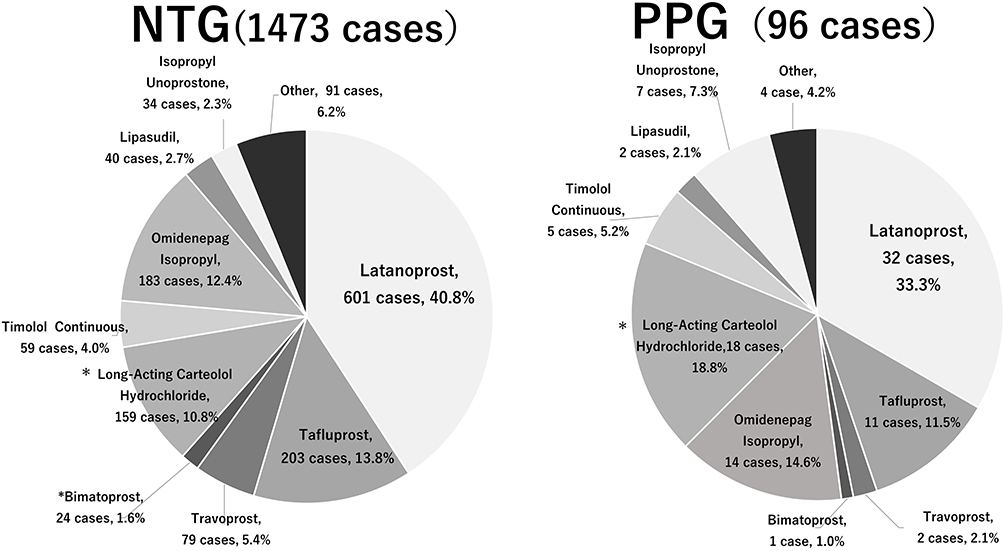 |
Figure 4 Comparison of monotherapy drug use in patients with NTG and PPG. χ2 test, Fisher’s direct method *P < 0.05. |
Two-Medication Use in the NTG and PPG Groups
For both groups, FP/β fixed-combination eye drops were the most prescribed treatment (NTG: 399 patients, 59.4%; PPG: 10 patients, 71.4%) (Figure 5), followed by an FP agonist with a β-blocker (NTG: 61 patients, 9.1%; PPG: 2 patients, 14.3%) and an FP agonist with a carbonic anhydrase inhibitor (CAI) in the NTG group (45 patients, 6.7%) and CAI/β fixed-combination eye drops (NTG: 44 patients, 6.5%; PPG: 2 patients, 14.3%), but there were no significant differences between the two groups.
 |
Figure 5 Two-drug usage in patients with NTG and PPG. Abbreviations: FP/β, FP receptor agonists/β-blocker; CAI/β, carbonic anhydrase inhibitor/β-blocker; α2, α-2-adrenergic agonist; β, β-blocker; CAI, carbonic anhydrase inhibitor; FP, FP receptor agonists. |
Three-, Four-, or Five-Medication Use in the NTG Group
Among patients with NTG who used three medications, the most common medications were CAI/β fixed-combination eye drops + FP agonist (81 patients, 22.5%), followed by FP/β fixed-combination eye drops + ophthalmic CAI (67 patients, 18.6%) and FP/β fixed-combination eye drops + α2-adrenergic agonist (α2 agonist; 52 patients, 14.4%).
Among patients who used four medications, the most common medications were FP/β fixed-combination eye drops + CAI/α2 fixed-combination eye drops (66 patients, 41.3%), followed by FP agonist + CAI/β fixed-combination eye drops + α2 agonist (21 patients, 13.1%) and FP/β fixed-combination eye drops + Rho-associated coiled-coil kinase (ROCK)/α2 fixed-combination eye drops (13 patients, 8.1%).
Among those using five medications, the most common was FP/β fixed-combination eye drops + CAI/α2 fixed-combination eye drops + ROCK (38 patients, 55.1%), followed by FP agonist + CAI/β fixed-combination eye drops + ROCK/α2 fixed-combination eye drops (11 patients, 15.9%).
Comparison of the Current and Previous Surveys on NTG
Comparison of Background Characteristics between the Current and Previous Surveys (2024 vs 2020) in Patients with NTG
The current survey (2024) included 2882 patients with NTG (45.6%), representing a significant decrease from the 2710 patients (51.1%) in the previous survey (P < 0.0001) (Table 3). The sex distribution was comparable (1191 men and 1691 women in this survey and 1116 men and 1594 women in the previous survey, P = 0.92). The average age in this survey was 69.0 ± 12.9 years, significantly older than the average age of 67.5 ± 13.4 years in the previous survey (P < 0.0001). The number of patients with a history of laser treatment was significantly higher in the present survey (61 patients, 2.1%) than in the previous survey (28 patients, 1.0%) (P < 0.01). Similarly, the number of patients with a history of surgery was significantly higher in the present survey (109 patients, 3.8%) than in the previous survey (30 patients, 1.1%) (P < 0.0001). The average number of medications used was 1.7 ± 1.1 in this survey and 1.6 ± 1.0 in the previous survey, with the average number of medications being significantly higher in this survey (P < 0.0001).
 |
Table 3 Comparison of Patient Characteristics between the Previous and Current Studies on Patients with NTG (2020 vs 2024) |
Comparison of Monotherapy Use between the Present and Previous Surveys (2024 vs 2020) in Patients with NTG
The proportion of patients with NTG was similar between the two surveys (P = 0.06), with 1473 patients (51.1%) in this survey and 1452 patients (53.6%) in the previous survey (Figure 6). EP2 agonists were used in 183 patients (12.4%) in this survey compared with 80 patients (5.5%) in the previous survey, whereas ROCK inhibitors were used in 40 patients (2.7%) in this survey and four patients (0.3%) in the previous survey, each significantly higher in this survey (P < 0.0001). By contrast, the use of FP agonists significantly decreased from 961 patients (66.2%) in the previous survey to 907 patients (61.6%) in this survey (P < 0.05). Similarly, the use of β-blockers significantly declined from 328 patients (22.6%) in the previous survey to 270 (18.3%) in this survey, while the use of α2 agonists also significantly declined from 59 (4.1%) in the previous survey to 7 (0.5%) in this survey (P < 0.05).
 |
Figure 6 Comparison of single-drug usage between the current and previous surveys for patients with NTG. χ2 test, Fisher’s direct method *P < 0.05, **P < 0.001. Abbreviations: FP agonists, FP receptor agonists; EP2 agonists, EP2 receptor agonists; ROCK inhibitor, Rho-associated coiled-coil kinase; α2 agonist, α2 adrenergic agonist; CAI, carbonic anhydrase inhibitor; α2, α-2-adrenergic agonist. |
Comparison of Patients with NTG Using Two Medications in the Present and Previous Surveys (2024 vs 2020)
The proportion of patients with NTG in this survey (23.3%; 672 patients) was significantly higher than that in the previous survey (24.2%; 657 patients) (P < 0.01) (Figure 7). FP/β fixed-combination eye drops were used in 59.4% of patients in this survey compared to 46.1% in the previous survey, with a significant increase in this survey (P < 0.01). The proportion of fixed-combination eye drops used was 71.0% in this survey compared to 54.5% in the previous survey, with a significant increase in this survey (P < 0.0001).
 |
Figure 7 Comparison of two-drug usage between the current and previous surveys for patients with NTG. χ2 test, Fisher’s direct method *P < 0.05. Abbreviations: FP/β, FP receptor agonists/β-blocker; CAI/β, carbonic anhydrase inhibitor/β-blocker; β/α2, β-blocker/α2 agonist; FP, FP receptor agonists; β, β-blocker; CAI, carbonic anhydrase inhibitor; FP+β, FP+CAI, FP+α2, a single drug combination. |
Comparison of Patients with NTG Using Three or More Medications in the Present and Previous Surveys (2024 vs 2020)
Among patients using three, four, or five medications, the proportion of fixed-combination eye drops used significantly increased in this survey compared with that in the previous survey. Specifically, the proportions were 93.3%, 96.9%, and 100.0% for three, four, and five medications in this survey, respectively, compared to 82.5%, 89.0%, and 88.9% in the previous survey (P < 0.0001 for three medications; P < 0.05 for four and five medications). In this survey, two fixed-combination eye drops were used in 50.6% of patients using four medications and in 76.8% of patients using five medications.
Discussion
Regarding the treatment of PPG, the fifth edition of the Guidelines for Glaucoma Practice recommends that
The initiation of treatment for PPG with normal IOP should be considered alongside careful clinical follow-up and evaluation of risk factors.1
Reports have also described the use of eye drops in treating PPG.6,7 One study investigated glaucoma progression in 127 patients with PPG, with 127 eyes treated with eye drops for over 5 years.6 Glaucoma progression occurred in 72 eyes (56.7%), with risk factors including optic papillary hemorrhage and percentage reduction in IOP. Another study observed 71 eyes of 71 patients with PPG for an average of 6.8 years after initiating eye drop treatment.7 Glaucoma progression occurred in 41 eyes (57.7%), with 30 eyes showing retinal nerve fiber layer thinning, 19 developing visual field defect appearance, and 8 having duplication. Risk factors for progression were optic papillary hemorrhage and IOP reduction rate of less than 20%.
In this survey, patients with PPG were significantly younger than patients with NTG, suggesting that PPG may progress to NTG over time. The number of medications used was significantly lower in PPG than in NTG. This is because treatment initiation in PPG is typically considered intermittently, based on careful follow-up and evaluation of risk factors, as mentioned above. Consequently, fewer medications are administered.
In patients with monotherapy use, the drugs used were similar, but FP agonists were significantly more common in NTG, while β-blockers and ion channel openers were significantly more common in PPG, possibly as a result of more IOP reduction in NTG and more safety considerations (“appearance of adverse effects”) in PPG. In patients using two medications, FP/β fixed-combination eye drops and FP agonist + β-blocker were more common in both NTG and PPG, in that order. The increased use of fixed-combination eye drops is likely owing to their availability in a single bottle, which simplifies adherence, similar to monotherapy. The use of FP agonists + β-blockers may include many cases of continuous use before the availability of fixed combination eye drops. In NTG, the use of FP agonists + β-blockers is comparable to that in the previous survey in 2020,8 suggesting a decrease in the number of new patients with this treatment.
When the differences in patients with NTG between this and the previous survey were examined, the proportion of patients with NTG decreased significantly in this survey. Other primary angle-closure glaucoma also decreased significantly. By contrast, the proportion of patients with POAG significantly increased. When PPG was combined with POAG in the broader definition of glaucoma, the proportion rose significantly, from 82.1% in the previous survey to 84.1% in this survey (P < 0.01). Despite expectations that heightened awareness of early glaucoma detection would increase NTG diagnoses, the opposite trend was observed. This discrepancy may be owing to the inclusion of PPG as a distinct disease category in this survey, shifting some previously classified patients with NTG into the PPG category. The patients with NTG were significantly older in this survey. Although increased awareness of early glaucoma detection was expected to result in younger patients with NTG, the opposite was observed. This could be attributed to an aging population and the tendency of patients to seek long-term care. The number of laser treatment and surgery cases was significantly higher in this survey, possibly owing to the widespread use of laser trabeculoplasty and micro-invasive (minimally invasive) glaucoma surgery. The number of medications used also increased significantly in this survey. Over the 4 years since the previous survey, several new fixed-combination eye drops have become available, including brimonidine tartrate hydrochloride/brinzolamide hydrochloride eye drops (CAI/α2 combination eye drops; launched in June 2020) and brimonidine tartrate hydrochloride/ripasudil hydrochloride combination eye drops (ROCK/α2 combination eye drops; launched in December 2022), increasing the number of medications. The increased variety of fixed-combination eye drops appears to have contributed to their growing usage. Monotherapy use of ROCK inhibitors, introduced in December 2014, and EP2 agonists, launched in December 2018, showed significant increases in this survey, likely reflecting their broader adoption over time. Conversely, the use of FP agonists, β-blockers, and α2 agonists decreased significantly, possibly owing to the rising preference for newer alternatives.
The use of FP/β fixed-combination eye drops significantly increased among patients requiring two medications for NTG. Fixed-combination eye drops, which consolidate multiple treatments into a single bottle, are gaining popularity owing to their convenience. Additionally, this survey revealed a significant increase in the use of four or five medications. Among patients requiring three or more medications, a significant increase was noted in the proportion of fixed-compound eye drops used. This may be owing to the launch of the two aforementioned fixed-combination eye drops without β-blockers, CAI/α2 fixed-combination eye drops and ROCK/α2 fixed-combination eye drops, during the 4-year period of 2020–2024.
This study had several limitations that should be considered. First, this was a cross-sectional study that aimed to investigate differences in treatment patterns between NTG and PPG. We did not consider differences in the duration of treatment, course, or follow-up. Furthermore, systemic risk factors such as hypertension and diabetes were not assessed. Second, because the study population was different from that in the previous study, case-by-case follow-up was not possible. Finally, the study was based on the situation in Japan, and the drugs available in other countries may differ; therefore, the results may need to be verified in different countries.
Conclusion
The drugs used in this survey were significantly more common in NTG than in PPG. While the breakdown of monotherapy medications was similar, significantly more FP agonists were used in NTG, and β-blockers and ion channel openers were more frequently used in PPG. The use of two medications was nearly equivalent between NTG and PPG. As new eye drops with new mechanisms of action are expected to emerge, the increasing complexity of pharmacotherapy underscores the importance of regularly conducting multicenter surveys to better understand the current state of glaucoma pharmacotherapy. In addition, we clarified that PPG and NTG differ in terms of age, type of drug administered, and number of medications and evaluated these trends in comparison with the 2020 study, providing a benchmark for routine treatment strategies.
Abbreviations
PPG, preperimetric glaucoma; NTG, normal tension glaucoma; POAG, primary open-angle glaucoma; IOP, intraocular pressure; FP agonists, prostanoid FP receptor agonist; β-blockers, β-adrenergic blockers; EP2 agonists, prostanoid EP2 receptor (selective) agonist; FP/β, FP receptor agonists /β-blocker; CAI/β, carbonic anhydrase inhibitor/β-blocker; CAI/α2, carbonic anhydrase inhibitor/α-2-adrenergic agonist; α2/β, α-2-adrenergic agonist/β-blocker; ROCK/α2, Rho-associated coiled-coil kinase/α-2-adrenergic agonist.
Data Sharing Statement
The participants’ data that support the findings of this study are available for 5 years after publication from the corresponding author, Kenji Inoue, upon reasonable request by e-mail.
Ethics Approval and Informed Consent
The study protocol was approved by the Ethics Committee of Inouye Eye Hospital (approval number: 202402–1) and adhered to the tenets of the Declaration of Helsinki. The committee waived the requirement for written informed consent owing to the study’s retrospective design. However, the institutions provided the study information to participants, and the participants had the opportunity to opt out of the study.
Consent for Publication
A copy of the signed agreement to the journal editorial office will be provided upon request.
Acknowledgments
We would like to thank the doctors at the 82 participating institutions for collecting the data for this survey.
Author Contributions
All authors made a significant contribution to the work reported, including in the conception, study design, execution, acquisition of data, analysis and interpretation; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Disclosure
K. Inoue reports receiving grants from Santen Pharmaceutical Co., Ltd., TEIJIN PHARMA LIMITED, and ONO PHARMACEUTICAL CO., LTD., as well as lecture fees from Senju Pharmaceutical Co., Ltd., Otsuka Pharmaceutical Co., Ltd., Kowa Pharmaceutical Co., Ltd., Santen Pharmaceutical Co., Ltd., Allergan Japan, K.K., Novartis Pharma K.K., CHUGAI PHARMACEUTICAL CO., LTD., Viatris, Inc., and Rohto Nitten Co. S. Kunimatsu-Sanuki received lecture fees from Santen Pharmaceutical Co., Ltd., Novartis Pharma K.K., Senju Pharmaceutical Co., Ltd., Otsuka Pharmaceutical Co., Ltd., Nitto Medic Co., Ltd., Viatris Inc., ROHTO Nitten Co., Ltd., and Kowa Pharmaceutical Co., Ltd.
G. Tomita received lecture fees from Senju Pharmaceutical Co., Ltd., Nitto Medic Co., Ltd., and Viatris Inc. K. Ishida reports lecture fees from Santen Pharmaceutical Co., Ltd., Senju Pharmaceutical Co., Ltd., Otsuka Pharmaceutical Co., Ltd., Kowa Pharmaceutical Co., Ltd., Nitto Medic Co., Ltd., and Glaukos Corporation. The authors declare no other conflicts of interest in this work.
References
1. Kiuchi Y, Inoue T, Shoji N, Nakamura M, Tanito M; Glaucoma Guideline Preparation Committee, Japan Glaucoma Society. The Japan Glaucoma Society guidelines for glaucoma 5th edition. Jpn J Ophthalmol. 2023;67(2):189–254. doi:10.1007/s10384-022-00970-9
2. Omodaka K, Horii T, Takahashi S, et al. 3D evaluation of the lamina cribrosa with swept-source optical coherence tomography in normal tension glaucoma. PLoS One. 2015;10(4):e0122347. doi:10.1371/journal.pone.0122347
3. Kim SB, Lee EJ, Han JC, Kee C. Comparison of peripapillary vessel density between preperimetric and perimetric glaucoma evaluated by OCT-angiography. PLoS One. 2017;12(8):e0184297. doi:10.1371/journal.pone.0184297
4. Jung KI, Jeon S, Shin DY, Lee J, Park CK. Pattern electroretinograms in preperimetric and perimetric glaucoma. Am J Ophthalmol. 2020;215:118–126. doi:10.1016/j.ajo.2020.02.008
5. Mehta B, Ranjan S, Sharma V, et al. The discriminatory ability of ganglion cell inner plexiform layer complex thickness in patients with preperimetric glaucoma. J Curr Ophthalmol. 2023;35(3):231–237. doi:10.4103/joco.joco_124_27
6. Kim KE, Jeoung JW, Kim DM, Ahn SJ, Park KH, Kim SH. Long-term follow-up in preperimetric open-angle glaucoma: progression rates and associated factors. Am J Ophthalmol. 2015;159(1):160–8.e1. doi:10.1016/j.ajo.2014.10.010
7. Jeong JH, Park KH, Jeoung JW, Kim DM. Preperimetric normal tension glaucoma study: long-term clinical course and effect of therapeutic lowering of intraocular pressure. Acta Ophthalmol. 2014;92(3):e185–e193. doi:10.1111/aos.12277
8. Piao H, Inoue K, Inoue J, et al. Multicenter survey study of glaucoma in 2020: normal-tension glaucoma and primary open angle glaucoma. Atarashii Ganka. 2021;38:945–950. Japanese.
9. Nakai Y, Inoue K, Moriyama R, et al. Current status of glaucoma therapy at private practices and a private ophthalmology hospital. Atarashii Ganka. 2008;25:1581–1585. Japanese.
10. Inoue K, Komori R, Kunimatsu-Sanuki S, Ishida K, Tomita G. Frequency of use of fixed-combination eye drops by patients with glaucoma at multiple private practices in Japan. Clin Ophthalmol. 2022;16:557–565. doi:10.2147/OPTH.S345944
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.