")
Back to Journals » Clinical Ophthalmology » Volume 18
Comparison of Visual and Refractive Outcomes of Keratorefractive Lenticule Extraction for Compound Myopic Astigmatism Between VisuMax and VISUMAX 800
Authors Varman A, Varman A, Balakumar D
Received 22 August 2024
Accepted for publication 26 November 2024
Published 30 November 2024 Volume 2024:18 Pages 3557—3566
DOI https://doi.org/10.2147/OPTH.S492552
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Aadithreya Varman, Arulmozhi Varman, Dinesh Balakumar
Uma Eye Clinic, Chennai, India
Correspondence: Aadithreya Varman, Uma Eye Clinic, O Block, No. 995, 2 nd Avenue, Annanagar, Chennai, 600040, India, Email [email protected]
Purpose: To evaluate the visual outcomes of keratorefractive lenticule extraction using a new version of a femtosecond laser platform with semi-automated cyclotorsion compensation in comparison to the previous generation without cyclotorsion control.
Methods: This was an ambispective study of consecutive eyes treated by SMILE with the VisuMax and VISUMAX 800 femtosecond lasers at the Uma Eye clinic, Chennai, India between June 2022 and July 2023. Inclusion criteria were myopia up to − 10 D and astigmatism between 1.5 D and 5 D. Data was retrospectively collected from patients that underwent SMILE using the VisuMax without cyclotorsion compensation and prospectively collected from patients undergoing SMILE using the VISUMAX 800 with Oculign and Centralign software aids.
Results: Data was collected from a total of 220 eyes that underwent routine SMILE; 115 eyes with VisuMax (VM500 group) and 105 eyes with VISUMAX 800 (VM800 group). The mean attempted spherical equivalent was − 4.82± 2.16 D in the VM500 group and − 4.80± 2.24 in the VM800 group. At the 3-month postoperative visit, 94% of eyes in the VM500 group and 98% of eyes in the VM800 group had an UDVA of 20/20 or better. Accuracy of the SEQ showed that 71% of eyes were within ± 0.50 D and 100% were within ± 1.00 D of target in the VM500 group and 96% of eyes were within ± 0.50 D and 100% were within ± 1.00 D of target in the VM800 group. There were no reported cases of suction loss or any other intraoperative complication in either group.
Conclusion: SMILE with the VisuMax and VISUMAX 800 provided excellent visual and refractive outcomes for subjects with myopic astigmatism. The VISUMAX 800, using Oculign and Centralign aids, demonstrated better accuracy when correcting cylinder greater than 2 D compared to the VisuMax without using manual cyclotorsion compensation.
Keywords: small-incision lenticule extraction, VISUMAX 800, astigmatism
Introduction
Small-incision lenticule extraction (SMILE), a keratorefractive lenticule extraction (KLEx) procedure, is an established treatment modality. SMILE has been performed using the VisuMax femtosecond laser (Carl Zeiss Meditec AG, Jena, Germany) since 2011 with long-term data on safety and efficacy outcomes for myopia and myopic astigmatism.1–4
One feature lacking on the original VisuMax is cyclotorsion compensation, which may compromise the outcomes when treating patients with high astigmatism.5,6 Previous studies have described manual compensation techniques to overcome this pitfall and have shown excellent results.7,8 However, the techniques to compensate for cyclotorsion, especially in the hands of novice SMILE surgeons, may lead to operator errors such as inaccurate alignment of the reference corneal marks with the eyepiece reticule and possible suction loss if rotation of the contact glass is not performed in a gentle manner.9
The VISUMAX 800 femtosecond laser (Carl Zeiss Meditec AG, Jena, Germany) is the latest upgrade to the SMILE platform. The major hardware improvement is an increased pulse frequency of 2 MHz which ensures a faster laser application time. Lenticule creation time with the VISUMAX 800 is between 8 and 10 seconds, compared to 22 to 30 seconds with the VisuMax. Cyclotorsion compensation has been addressed on the VISUMAX 800 with the addition of OcuLign software. After docking and suction activation, OcuLign allows the surgeon to twist the joystick on the laser arm in a clockwise or anticlockwise manner to align the cylinder treatment to the appropriate axis. In addition to Oculign, the VISUMAX 800 also has CentraLign software which allows the (x,y) coordinates of the corneal vertex to be entered during treatment planning. CentraLign then displays the corneal vertex coordinates, and the surgeon is guided by visual overlays on the treatment monitor to align the treatment on the visual axis. Recent studies of SMILE with VISUMAX 800 showed the procedure to be safe and effective for treating myopia with astigmatism with equivalent results to the VisuMax when manual compensatory protocols were used.10,11
The objective of this study was to evaluate the visual and refractive outcomes of treating myopic astigmatism with SMILE using the new VISUMAX 800 platform with cyclotorsion compensation (OcuLign) and centration (CentraLign) in comparison to SMILE using VisuMax 500 without any manual compensatory protocols.
Methods
This was an ambispective, non-randomized, single site study evaluating subjects that underwent routine SMILE with VisuMax or VISUMAX 800 for myopic astigmatism. Data was collected from patients that were treated by a single experience surgeon (A.V). at the Uma Eye Clinic, Chennai, Tamil Nadu, India between June 2022 and July 2023. VISUMAX 800 data was collected prospectively, and Institutional Review Board approval was obtained from Uma eye clinic ethics committee (Ref Number: ECO-2018-0190). Informed consent was collected from all patients prior to enrolling in the study. VisuMax data was retrospectively collected from eyes that met the same inclusion criteria and were treated during the same time period. The data was exempt from full Review Board approval due to the de-identified and retrospective nature of the study. All portions of this study were conducted according to the Declaration of Helsinki and any applicable local and national laws.
Patients
The inclusion criteria were subjects found suitable for routine SMILE, at least 18 years of age, myopia up to −10 D, cylinder between 1.5 and 5 D, preoperative corrected distance visual acuity of 20/25 or better, and a minimum central corneal thickness of 480 μm. Exclusion criteria were ocular pathology, history of previous ocular surgery or trauma, and irregular astigmatism. Patients diagnosed with dry eye were treated accordingly prior to treatment.
Surgical Protocol
VisuMax Group (VM500 Group)
Docking and laser application were performed following the directions for use, with no additional techniques incorporated to compensate for cyclotorsion or treatment centration. Once supine on the laser bed, the subject was asked to locate and focus on the green fixation light and docking was continued until full suction was complete. The procedure was completed without rotating the contact glass to compensate for cyclotorsion.
VISUMAX 800 Group (VM800 Group)
Prior to treatment and with the subject seated upright at the slit-lamp, limbal marking was performed on the horizontal axis at 0° and 180° using a dye permitting transmission of infrared radiation (Viscot surgical skin marker 1436; Viscot Medical, East Hanover, NJ). Following the marking on the horizontal axis, the slit-lamp beam was rotated and the eye was marked again at 90°. Once supine on the laser bed, CentraLign software was used to ensure centration during docking. After docking and suction activation, the joystick on the laser arm was rotated clockwise or counter-clockwise to align the laser reticule to the limbal markings and then treatment was applied.
Laser Settings
All laser parameters were the same between the VM500 and VM800 groups including a total pulse energy of 130 nJ, lenticule diameter of 6.5 mm, cap diameter of 7.00 mm, and intended cap thickness between 120 and 140 µm. The spot distance was 4.5 μm and the track distance was 4.5 μm. The small incision was 2.5 mm in length and positioned at 120° with an angle of 40°.
Postoperative
After surgery, all subjects received a topical antibiotic/steroid combination eye drop for one week, followed by steroid drops alone for four weeks. Topical lubricants were used as needed. All subjects were evaluated immediately after treatment and at 1-day, 1-week, 1-month, and 3-months postoperatively. Uncorrected distance vision (UDVA), corrected distance visual acuity (CDVA), aberrometry, and topography were evaluated at the 3-month postoperative visit.
Statistical Analysis
Normality of the data was checked using Shapiro–Wilk’s test. Comparison of treatment outcomes between groups was performed using unpaired Student’s t-test for data that followed normal distribution and Mann Whitney U-test for data that were not in normal distribution. Data analysis was done using IBM SPSS software version 25. Visual and refractive outcomes analysis was performed according to the Standard Graphs for Reporting Refractive Surgery12 and vector analysis was performed using the Alpins method13 and Assort software (ASSORT Pty. Ltd., Victoria, Australia).
Results
Data was collected from a total of 220 eyes that underwent routine SMILE with VisuMax or VISUMAX 800 at the Uma Eye Clinic between June 2022 and July 2023. The preoperative patient demographics can be seen in Table 1. Of the 220 eyes, 115 (52.5%) were treated using the VisuMax (VM500 group) and 105 (47.5%) using the VISUMAX 800 (VM800 group). The two groups were further divided into low cylinder and high cylinder cohorts based on the preoperative astigmatism values. Eyes with ≤ 2.00 D were classified as low cylinder and eyes with > 2.00 D were classified as high cylinder. Demographics for the low cylinder and high cylinder cohort can be seen in Supplemental Tables 1A and B, respectively.
 |
Table 1 Patient Demographics |
Efficacy and Predictability
Figures 1 and 2 show the Nine Standard Graphs for Reporting Refractive Surgery for all eyes within the VM500 group and the VM800 group, respectively. The UDVA in the VM500 group was 20/20 or better in 94% of eyes compared to 100% with a preoperative CDVA of 20/20 or better (Figure 1A). The UDVA in the VM800 group was 20/20 or better in 98% of eyes compared to 98% with a preoperative CDVA of 20/20 or better (Figure 2A). The mean postoperative manifest refraction spherical equivalent (SEQ) was −0.32±0.20 D in the VM500 group and −0.27±0.22 in the VM800 group. Accuracy of the SEQ showed that 71% of eyes were within ±0.50 D and 100% were within ±1.00 D of target in the VM500 group (Figure 1E) and 96% of eyes were within ±0.50 D and 100% were within ±1.00 D of target in the VM800 group (Figure 2E).
 |
Figure 1 Standard graphs for reporting refractive surgery showing the 3-month postoperative outcomes after small-incision lenticule extraction using the VisuMax 500 femtosecond laser. (A) Cumulative Snellen visual acuity (20/× or better) comparing postoperative (postop) uncorrected distance visual acuity (UDVA) with preoperative (preop) corrected distance visual acuity (CDVA). (B) Comparison of pre operative CDVA with post operative UDVA. (C) Change in corrected distance visual acuity (CDVA) compared to preoperative. (D) Attempted versus achieved spherical equivalent of refraction. (E) Spherical equivalent refractive accuracy. (F) Stability of post op spherical equivalent of refraction. (G) Distribution of refractive astigmatism pre and post op. (H): Comparison of Target induced astigmatism with surgically induced astigmatism. (I) Distribution of angle of error of refractive astigmatism. Abbreviations: D, Diopters; UDVA, Uncorrected Distance Visual Acuity; CDVA, Corrected Distance Visual Acuity; SEQ, Spherical Equivalent; SIA, Surgically Induced Astigmatism; TIA, Target Induced Astigmatism. |
 |
Figure 2 Standard graphs for reporting refractive surgery showing the 3-month postoperative outcomes after small-incision lenticule extraction using the VISUMAX 800 femtosecond laser. (A) Cumulative Snellen visual acuity (20/× or better) comparing postoperative (postop) uncorrected distance visual acuity (UDVA) with preoperative (preop) corrected distance visual acuity (CDVA). (B) Comparison of pre operative CDVA with post operative UDVA. (C) Change in corrected distance visual acuity (CDVA) compared to preoperative. (D) Attempted versus achieved spherical equivalent refraction. (E) Spherical equivalent refractive accuracy. (F) Stability of post op spherical equivalent of refraction. (G) Distribution of refractive astigmatism pre and post op. (H) Comparison of Target induced astigmatism with surgically induced astigmatism. (I) Distribution of angle of error of refractive astigmatism. Abbreviations: D, Diopters; UDVA, Uncorrected Distance Visual Acuity; CDVA, Corrected Distance Visual Acuity; SEQ, Spherical Equivalent; SIA, Surgically Induced Astigmatism; TIA, Target Induced Astigmatism. |
The mean manifest refraction cylinder was −0.27±0.31 D in the VM500 group and −0.14±0.29 D in the VM800 group. Accuracy of the cylinder correction showed that 82.5% of eyes had ≤ 0.50 D and 98% had ≤ 1.00 D of refractive astigmatism in the VM500 group (Figure 1G) and 92% of eyes had ≤ 0.50 D and 100% had ≤ 1.00 D of refractive astigmatism in the VM800 group (Figure 2G). Further analysis of mean postoperative cylinder for all eyes can be found in Table 2, the low cylinder in Table 3 and high cylinder sub-cohort in Table 4.
 |
Table 2 Refractive Outcomes at the 3-Month Postoperative Visit (All Eyes) |
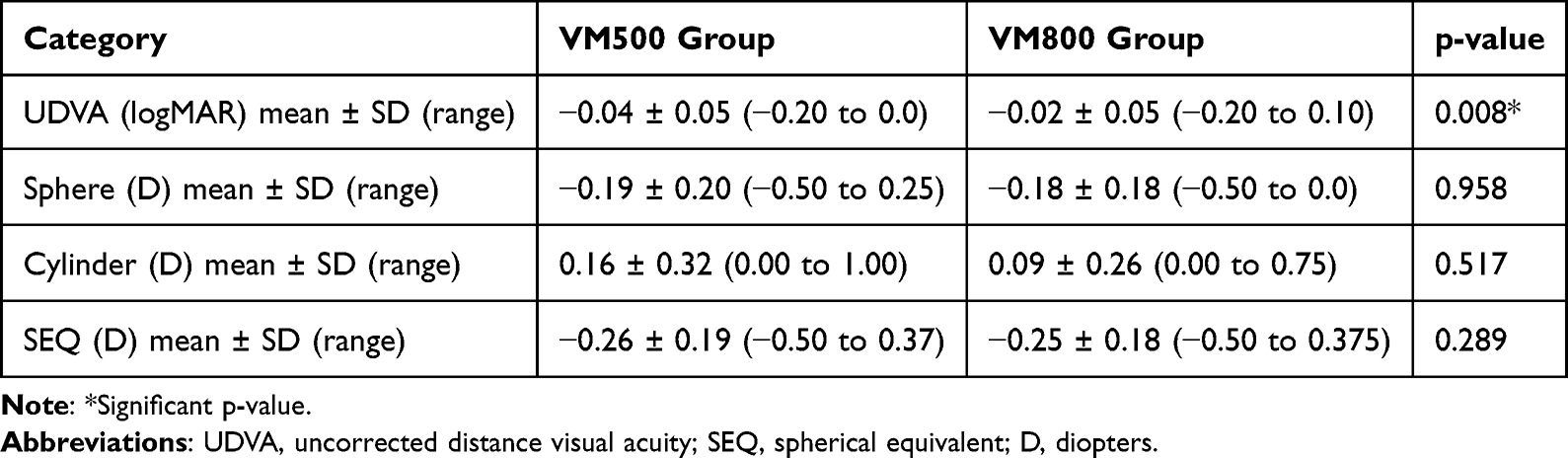 |
Table 3 Refractive Outcomes at the 3-Month Postoperative Visit (Low Cylinder Cohort) |
 |
Table 4 Refractive Outcomes at the 3-Month Postoperative Visit (High Cylinder Cohort) |
Astigmatism Analysis
Analysis of the angle of error (AoE) revealed differences between the two groups. In the VM500 group, 18% of eyes exhibited an AoE exceeding 5°, with a range of 5° to 35° (Figure 1I). Conversely, only 5% of eyes in the VM800 group had an AoE greater than 5°, and all were within 15° (Figure 2I). Additional astigmatism outcomes were reported according to the quad polar maps as seen in Figures 3 and 4 for the VM500 group and VM800 group, respectively. The target induced astigmatism vector (TIA) mean was 2.16 Axis 178 in the VM500 group and 1.89 Axis 179 in the VM800 group. The difference vector (DV) mean was 0.17 Axis 1 in the VM500 group compared to 0.15 Axis 0 in the VM800 group. The correction index (CI) arithmetic mean was 0.95 in the VM500 group and 0.98 in the VM800 group.
 |
Figure 3 Vector analysis of refractive cylinder showing target induced astigmatism (TIA), surgically induced astigmatism (SIA), difference vector (DV), and correction index (CI) after small-incision lenticule extraction using the VisuMax 500 femtosecond laser. |
 |
Figure 4 Vector analysis of refractive cylinder showing target induced astigmatism (TIA), surgically induced astigmatism (SIA), difference vector (DV), and correction index (CI) after small-incision lenticule extraction using the VISUMAX 800 femtosecond laser. |
Safety
Corrected distance visual acuity (CDVA) and surgical complications were evaluated for safety considerations. Postoperative CDVA was compared against preoperative CDVA for both groups as can be seen in Figures 1C and 2C. Three eyes in each group lost one line of vision. No eyes in either group lost two or more lines of CDVA. There were no intraoperative complications such as suction loss, retained lenticule fragments, incision tears, or improper plane dissection reported for either group.
Discussion
While manual cyclotorsion compensation on the VisuMax femtosecond laser has been adopted by many surgeons, it is not used by everyone. In addition, it can be difficult for novice users, takes time to master, and has been reported to lead to loss of suction if rotation of the contact glass is not performed in a gentle manner.9 Therefore it was important to compare the VM500 group results, without compensation, to the VM800 group that underwent treatment with the VISUMAX 800 using the latest upgrades, especially when evaluating astigmatism outcomes.
The current study results show excellent visual and refractive outcomes with both the VisuMax (without the use of cyclotorsion compensation or centration aids) and the newer VISUMAX 800 using the upgraded Oculign and Centralign features. Both groups showed an excellent mean postoperative SEQ. A high percentage of eyes, 94% in the VM500 group, and 98% in the VM800 group achieved an UDVA of 20/20. In addition, 71% of eyes in the VM500 group and 95% of eyes in the VM800 group were within ±0.50 D of intended target.
The efficacy of SMILE with VisuMax in the correction of myopia and myopic astigmatism is well established. However, there are a number of reports that show a trend of undercorrection of cylinder when treating above 2 D.14–16 In the current VM500 group, with no cyclotorsion compensation, 82% of eyes had ≤ 0.50 D of refractive astigmatism with a similar undercorrection seen as seen in the other studies for eyes requiring ≥ 2.00 D of treatment.
To treat astigmatism more accurately with SMILE, there have been a number of techniques described to manually compensate for the cyclotorsion. Ganesh et al,7 described marking the limbus at 0° and 180°, which could serve as reference marks for identifying cyclotorsion when the patient was placed in the supine position. Once docking and suction activation is complete, the surgeon is required to manually rotate the contact glass to align the reference marks with the horizontal and vertical axis which is visible when looking through the auxiliary screen. Jun et al,8 described a triple centration technique of marking two points at the horizontal meridian 7 mm apart, and one mark bisecting the first Purkinje image. Wang et al,17 described a similar methods of cyclotorsion compensation and reported slightly better outcomes when treating patients with high cylinders when compared to a control group without incorporating manual compensation.
Similar to the excellent outcomes that have been reported on the VisuMax, recent studies on the outcomes after SMILE with the VISUMAX 800 by Reinstein et al,10 and Saad et al,18 showed that 91% and 92.8% of eyes achieved UDVA of 20/20 or better, respectively. In addition, both studies showed accurate cylinder outcomes with Reinstein et al,10 reporting 85% of eyes with ≤ 0.50 D of astigmatism and Saad et al,18 reporting 94.1% of eyes with ≤ 0.50 D. In the current population, the preoperative mean cylinder was greater than in Reinstein study (−0.98 D compared to −2.54 D) but still showed similar results for the VM800 group with 92% of eyes achieving ≤ 0.50 D of residual astigmatism.
A comparison of astigmatism outcomes in the current population found statistically significant differences in the correction of myopic astigmatism between the VM500 group and the VM800 group. In this study, eyes treated on the VM800 group had more accurate outcomes in the treatment of cylinder in comparison to the VM500 group (Table 2). Analysis of the angle of error (AoE) revealed differences between the two groups. In the VM500 group, 18% of eyes exhibited an AoE exceeding 5°, with a range of 5° to 35°. Conversely, only 5% of eyes in the VM800 had an AoE greater than 5°, and all were within 15°. The difference in spread of AoE was likely due to not using any cyclotorsion compensation techniques in the VM500 group. While the correction index (CI) is slightly better in the VM800 group as one may expect, the results are similar and are not likely clinically significant. Further evaluation of similar graphs based on level of preoperative astigmatism may show a greater difference between the groups. The mean magnitude of the difference vector (DV) was 0.15 D Ax 0 in the VM800 group and 0.17 D Ax 1 in the VM500 group. Although the arithmetic mean of the DV was slightly lower in the VM500 group (0.21 D) compared to the VM800 group (0.24 D), this difference was likely due to random error and is not clinically significant. As with the CI, further analysis based on magnitude of preoperative astigmatism may yield more concrete answers.
As noted in Table 3, the difference between cylinder outcomes was not significant when evaluating eyes with low cylinder (≤ 2 D). However, the difference between the two groups seemed to be amplified in the high cylinder subgroup which showed greater statistical significance in comparison to the low cylinder subgroup, indicating greater benefit when correcting more than 2 D of cylinder (Table 4). The improved accuracy of cylinder correction in the VM800 group seemed to correlate with a better UDVA when compared to the VM500 group. However, this difference was minimal. These results also match the conclusion of a meta-analysis performed by Yang et al19 that found a slight advantage of cyclotorsion compensation in SMILE when compared to control groups where no cyclotorsion compensation was performed.
The current study yielded outcomes comparable to those reported by Reinstein et al.10 Although our cohort exhibited higher target-induced astigmatism (TIA) and surgically induced astigmatism (SIA), vector analysis parameters were similar between the two studies. Notably, the current study demonstrated a marginally lower difference vector (DV) in the VM800 group (0.24 ± 0.22) compared to the Reinstein study (0.38 ± 0.28). The summated vector mean was comparable across both studies (0.15 Ax 0 in our study vs 0.26 Ax 12 reported by Reinstein.
In addition to evaluating visual outcomes, intraoperative and postoperative complication were also monitored for the VM500 and VM800 groups. As previously mentioned, the VISUMAX 800 uses a 2 MHz frequency. One possible advantage of the increase in lenticule creation speed, is a decrease incidence of suction loss. In a previous study on suction loss with the VisuMax, the incidence was reported to be 0.5%, with 65% of the cases occurring after the 10 seconds of creation of the lenticule interface.20 Therefore, it was hypothesized that there could be a significant reduction in suction loss with the VISUMAX 800 when compared to its predecessor. In the current study, there were no reported cases of suction loss in either the VM500 group (115 eyes) or the VM800 group (105 eyes). Additional large population VISUMAX 800 outcomes studies will help further evaluate the possibility of a reduction in reported cases of suction loss.
One limitation of the study is the relatively short follow up period. However previous literature on long-term follow up of patients treated with SMILE using the VisuMax for myopia and myopic astigmatism have shown stable results.21,22 It is reasonable to expect the same stability when treating using the VISUMAX 800. However, future studies with long term follow up are required to verify this claim. A second limitation of the study is the retrospective nature of the data collection used for the VM500 group. As part of standard practice, a strict preoperative, operative, and postoperative protocol is followed for all patients that are treated at the clinic and therefore minimizes any inherent differences between data regardless of if it was collected in a prospective or retrospective manner. However, it is not lost on the authors that there may be unseen differences in patient responses that are out the clinicians control when the subject knows they are enrolled in a prospective study.
As part of the current study, it was important to evaluate the refractive outcomes without using any cyclotorsion compensation technique in the VM500 group to properly evaluate the inherent benefits of the VISUMAX 800. This may be of particular interest for new or novice surgeons starting on the VisuMax or the VISUMAX 800 and further studies should be performed to analyze any potential benefits that these new features may have in the learning curve for new surgeons and surgeons who may not be comfortable performing the manual cyclotorsion techniques required with the VisuMax femtosecond laser.
In conclusion, both platforms provided excellent visual outcomes. However, the new platform for KLEx with VISUMAX 800 provided more accurate refractive cylinder outcomes in the treatment of myopic astigmatism by incorporating a mechanism of semi-automated cyclotorsion compensation and treatment centration in comparison to the VisuMax when manual protocols are not used. Further investigations with a larger dataset of treated eyes and longer follow-up will be needed to gauge the magnitude of difference between the two technologies.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Reinstein DZ, Archer TJ, Vida RS, Carp GI, Reinstein JFR, McAlinden C. Objective and subjective quality of vision after SMILE for high myopia and astigmatism. J Refract Surg. 2022;38:404–413. doi:10.3928/1081597X-20220516-03
2. Blum M, Lauer AS, Kunert KS, Sekundo W. 10-year results of small incision lenticule extraction. J Refract Surg. 2019;35:618–623.
3. Damgaard IB, Sejersen H, Ivarsen A, Hjortdal J. 7-year results of SMILE for high myopia: visual and refractive outcomes and aberrations. J Refract Surg. 2021;37:654–661. doi:10.3928/1081597X-20210712-02
4. Chen P, Ye Y, Yu N, Zhang X, Zhuang J, Yu K. Correction of astigmatism with SMILE with axis alignment: 6-month results from 622 eyes. J Refract Surg. 2019;35:138–145. doi:10.3928/1081597X-20190124-02
5. Chow SSW, Chow LLW, Lee CZ, Chan TCY. Astigmatism correction using SMILE. Asia Pac J Ophthalmol. 2019;8:391–396. doi:10.1097/01.APO.0000580140.74826.f5
6. Khalifa MA, Ghoneim AM, Shaheen MS, Piñero DP. Vector analysis of astigmatic changes after small-incision lenticule extraction and wavefront-guided laser in situ keratomileusis. J Cataract Refract Surg. 2017;43:819–824. doi:10.1016/j.jcrs.2017.03.033
7. Ganesh S, Brar S, Pawar A. Results of intraoperative manual cyclotorsion compensation for myopic astigmatism in patients undergoing small incision lenticule extraction (SMILE). J Refract Surg. 2017;33:506–512. doi:10.3928/1081597X-20170328-01
8. Jun I, Kang DSY, Reinstein DZ, et al. Clinical outcomes of SMILE with a triple centration technique and corneal wavefront-guided transepithelial PRK in high astigmatism. J Refract Surg. 2018;34:156–163. doi:10.3928/1081597X-20180104-03
9. Chuckpaiwong V, Chansue E, Lekhanont K, Tanehsakdi M, Jongkhajornpong P, Nonpassopon M. 12-month outcomes of small incision lenticule extraction with proper head positioning but no reference marking for the correction of astigmatism. J Refract Surg. 2023;39:683–692. doi:10.3928/1081597X-20230824-01
10. Reinstein DZ, Archer TJ, Potter JG, Gupta R, Wiltfang R. Refractive and visual outcomes of SMILE for compound myopic astigmatism with the VISUMAX 800. J Refract Surg. 2023;39:294–301. doi:10.3928/1081597X-20230301-02
11. Yoo TK, Kim D, Kim JS, et al. Comparison of early visual outcomes after SMILE using VISUMAX 800 and VISUMAX 500 for myopia: a retrospective matched case-control study. Sci Rep. 2024;14:11989. doi:10.1038/s41598-024-62354-y
12. Reinstein DZ, Archer TJ, Randleman JB. JRS standard for reporting astigmatism outcomes of refractive surgery. J Refract Surg. 2014;30:654–659. doi:10.3928/1081597X-20140903-01
13. Alpins NA. A new method of analyzing vectors for changes in astigmatism. J Cataract Refract Surg. 1993;19:524–533. doi:10.1016/S0886-3350(13)80617-7
14. Pérez-Izquierdo R, Rodríguez-Vallejo M, Matamoros A, et al. Influence of preoperative astigmatism type and magnitude on the effectiveness of SMILE correction. J Refract Surg. 2019;35:40–47. doi:10.3928/1081597X-20181127-01
15. Zhong Y, Li M, Han T, Fu D, Zhou X. Four-year outcomes of small incision lenticule extraction (SMILE) to correct high myopic astigmatism. Br J Ophthalmol. 2021;105:27–31. doi:10.1136/bjophthalmol-2019-315619
16. Ivarsen A, Hjortdal J. Correction of myopic astigmatism with small incision lenticule extraction. J Refract Surg. 2014;30:240–247. doi:10.3928/1081597X-20140320-02
17. Wang B, Wang Y, Zhang J. Comparison of astigmatic correction with and without limbal marking during small-incision lenticule extraction. J Cataract Refract Surg. 2022;48:924–928. doi:10.1097/j.jcrs.0000000000000889
18. Saad A, Klabe K, Kirca M, Kretz FAT, Auffarth G, Breyer DRH. Refractive outcomes of small lenticule extraction (SMILE) Pro® with a 2 MHz femtosecond laser. Int Ophthalmol. 2024;44:52. doi:10.1007/s10792-024-02915-2
19. Yang X, Liu Y, Xiao K, et al. Effect of cyclotorsion compensation in small incision lenticule extraction surgery for the correction of myopic astigmatism: a systematic review and meta-analysis. Ophthalmol Ther. 2024;13:1271–1288. doi:10.1007/s40123-024-00921-2
20. Reinstein DZ, Archer TJ, Vida RS, Carp GI. Suction stability management in small incision lenticule extraction: incidence and outcomes of suction loss in 4000 consecutive procedures. Acta Ophthalmol. 2020;98:e72–e80. doi:10.1111/aos.14215
21. Lang M, Cao KW, Liu T, Zhu Y, Ye J. Five-year results of refractive outcomes and vision-related quality of life after SMILE for the correction of high myopia. Int J Ophthalmol. 2021;14:1365–1370. doi:10.18240/ijo.2021.09.11
22. Ağca A, Tülü B, Yaşa D, Yıldırım Y, Yıldız BK, Demirok A. Long-term (5 years) follow-up of small-incision lenticule extraction in mild-to-moderate myopia. J Cataract Refract Surg. 2019;45:421–426. doi:10.1016/j.jcrs.2018.11.010
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.