")
Back to Journals » Clinical Ophthalmology » Volume 18
Comparison of Visual Performance Between Mix-and-Match and Bilateral Implantation of Rotationally Asymmetric Multifocal Intraocular Lenses
Authors Liu D, Li H , Zheng S, Sun J, Bai H, Wu X
Received 1 September 2024
Accepted for publication 4 November 2024
Published 18 November 2024 Volume 2024:18 Pages 3289—3295
DOI https://doi.org/10.2147/OPTH.S487162
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Dongle Liu,1– 3 Honglei Li,1– 3 Simeng Zheng,1– 3 Jiajun Sun,1– 3 Huiran Bai,1– 3 Xiaoming Wu1– 3
1Eye Institute of Shandong First Medical University, Qingdao Eye Hospital of Shandong First Medical University, Qingdao, People’s Republic of China; 2State Key Laboratory Cultivation Base, Shandong Provincial Key Laboratory of Ophthalmology, Qingdao, People’s Republic of China; 3School of Ophthalmology, Shandong First Medical University, Qingdao, People’s Republic of China
Correspondence: Xiaoming Wu, Eye Institute of Shandong First Medical University, Qingdao Eye Hospital of Shandong First Medical University, 5 Yanerdao Road, Qingdao, 266000, People’s Republic of China, Email [email protected]
Objective: To evaluate and compare the clinical outcomes of rotationally asymmetric multifocal intraocular lenses (IOLs) in a mix-and-match approach or bilateral implantation.
Methods: In this prospective study, patients were split into two groups based on the types of IOLs implanted. The mix group received mix-and-match implantation of a LENTIS Mplus LS-313 +1.50D IOL in the dominant eye and a LENTIS Mplus LS-313 +3.0D IOL in the fellow eye. The bilateral group received bilateral implantation of LENTIS Mplus LS-313 +3.00D IOLs. A three-month follow-up was performed after the surgery. Binocular visual acuity at various distances, subjective refraction and defocus curves were assessed. Subjective questionnaires included the overall satisfaction, a self-assessment of visual quality, spectacle independence, and presence of photic phenomena were completed.
Results: The study was completed by 52 patients in total (25 mix-and-match, 27 bilateral). The mean binocular uncorrected intermediate visual acuity in the mix group and the bilateral group were 0.10 ± 0.12 logMAR and 0.23 ± 0.14 logMAR, respectively, demonstrating a significant difference (P = 0.005). The mix group performed better in intermediate vision (range: − 1.00 to − 2.00 D) than the bilateral group (all P< 0.05), according to binocular defocus curves. About 92.0% of patients in the mix group did not need spectacles for intermediate distance vision compared to 59.26% in the bilateral group (P = 0.0001).
Conclusion: The mix-and-match implantation of the +1.50D and +3.00D rotationally asymmetric multifocal IOLs provided good binocular visual outcomes and resulted in better intermediate vision than bilateral implantation of +3.00D IOLs.
Keywords: multifocal intraocular lenses, mix-and-match, visual outcomes
Introduction
The use of multifocal intraocular lenses (IOLs) is becoming increasingly widespread and has become a significant alternative for refractive cataract surgery with the advancement of IOL materials, technology, and advanced optics, as well as the improvement of patients’ criteria for visual quality.1 Multifocal IOLs are specifically engineered to offer clear vision across multiple distances—near, intermediate, and far—unlike monofocal IOLs, which are designed to focus on a single distance. The primary objective of multifocal IOLs is to enhance overall visual acuity, enabling patients to see well at varying distances simultaneously.2 Since its introduction, the Lentis Mplus LS-313 series (Oculentis GmbH, Berlin, Germany) has set the standard for rotationally asymmetric multifocal IOLs. Its unique design has consistently delivered satisfactory visual outcomes, making it a benchmark in the field.3–6
The rotationally asymmetric multifocal IOL is designed with an optic that combines an inferior segmental near addition with an aspheric distance vision zone, offering a seamless transition between these two zones.7 The near addition options are +3.00, +2.00, or +1.50 diopters (D), selected by the surgeon based on the patient’s needs and expectations. It was formerly common to implant both eyes with multifocal IOLs that had the same near addition power. Mixed implantation has been studied in the past, and previous research has mostly focused on diffractive multifocal IOLs or extended depth of focus (EDOF) IOLs.8–12 There was few research on blended implantation with rotationally asymmetric multifocal IOLs.5 Although trifocal IOLs provide good visual acuity at near, intermediate, and far distances,1,2 our study focuses on evaluating the outcomes of the mix-and-match approach with the IOLs selected, offering an alternative strategy for achieving visual acuity at varying distances.
In this prospective study, patients who received a mix-and-match approach with rotationally asymmetric multifocal IOLs (+1.50 D in dominant eye and +3.00 D in non-dominant eye) were compared to those who received bilateral implantation with rotationally asymmetric multifocal IOLs +3.00 D.
Patients and Methods
Study Design
This study was a single-center, prospective, contralateral trial that adhered to the ethical standards outlined in the Helsinki Declaration. It received approval from the Ethics Committee of Qingdao Eye Hospital (approval number QYLS 201906). Written informed consent was obtained from all patients who underwent uncomplicated bilateral cataract surgeries between June 2021 and July 2023.
Inclusion criteria: patients who had an uneventful cataract surgery and a preoperative corneal astigmatism of less than 1.00 D, patients planning to complete bilateral cataract surgery within 2 weeks, and 4mm pupil diameter higher-order aberration <0.3μm. Exclusion criteria: dry eye, corneal diseases, glaucoma, progressive retinopathy, and any other ocular diseases that can affect the surgical outcomes.
The characterization and price of both mix-and-match and bilateral IOL implantation methods were explained to each patient. The patients were divided into two groups based on their voluntary choice of implantation method. Mix-and-match and bilateral IOL implantation methods were used to split patients into two groups. Mix-and-match patients received the LENTIS Mplus IOL with a +1.50 D in the dominant eye and a +3.00 D in the non-dominant eye. In the bilateral group, the LENTIS Mplus IOL +3.00 D addition was bilaterally implanted.
Preoperative Assessment
Ophthalmological examination included uncorrected distance visual acuity (UDVA), subjective refraction, corneal endothelial counts, optical coherence tomography, slit-lamp, and fundus examination. Optical biometric device (OA-2000, Tomey Co., Japan) was used to measure ocular biometric parameters. The IOL power was calculated by Barrett Universal II formula. Both eyes were targeted for emmetropia.
IOLs
The aspheric hyperopic and posterior fan-shaped near vision zones of the LENTIS Mplus LS-313 are included in a single-piece foldable biconvex acrylic IOL. It is designed with a plate support. The overall diameter is 12 mm, with optics measuring 6 mm. LENTIS Mplus LS-313MF30 improves near vision by +3.00 D, whereas LENTIS Mplus LS-313MF15 improves intermediate vision by +1.50 D.
Surgical Procedure
All cataract surgeries were carried out by a highly experienced surgeon, Xiaoming Wu, utilizing the Infiniti Vision System (The Alcon Laboratories, Inc). The procedures adhered to a standardized suture-less phacoemulsification technique, which started with a 2.2-mm clear temporal corneal incision and a 5.5-mm continuous curvilinear capsulorhexis. Following this, a LENTIS Mplus LS-313 IOL was implanted into the capsular bag, with the near addition segment precisely positioned inferiorly.
Postoperative Assessment
Three months after surgery, monocular UDVA and corrected distance visual acuity (CDVA) and binocular uncorrected visual acuity were evaluated at three distances: far (5 m), intermediate (66 cm), and near (40 cm). The assessments included subjective refraction, defocus curves, and subjective questionnaires. Defocus curves were obtained by measuring visual acuity under photopic conditions at a 5 m distance, using lenses added in 0.5 D increments from −4.0 to +1.0 D.
The subjective questionnaires addressed overall satisfaction, self-perceived visual quality, and the degree of spectacle independence for near, intermediate, and far vision. They also assessed the presence of photic phenomena, such as glare, halos, and starbursts. Overall satisfaction was rated on a scale from 5 to 0 (very satisfied, satisfied, neither satisfied nor dissatisfied, unsatisfied, very unsatisfied). The self-assessment of visual quality, both during the day and at night, was scored on a scale from 0 (worst) to 10 (best).
Statistical Analysis
SPSS (version 22.0; SPSS Inc., Chicago, IL) was used for statistical analysis. Chi-square tests were employed to analyze categorical data. The Student’s t-test was applied to compare variables that met the assumptions of normal distribution and equal variance. In cases where the data did not meet these assumptions, the Mann–Whitney U-test was used for comparison. All statistical tests were considered significant if the P value was less than 0.05.
Results
The study included 52 participants (104 eyes). Twenty-five patients received the LENTIS Mplus LS-313 +3.00/+1.50D in the mix group, while 27 patients were bilaterally implanted with the LENTIS Mplus LS-313 +3.00 in the bilateral group. Table 1 provides an overview of the demographic and preoperative clinical characteristics for each group. There were no statistically significant differences between the two groups in terms of sex, age, preoperative UDVA, axial length, corneal astigmatism, corneal endothelial cell count, anterior chamber angle, or IOL power.
 |
Table 1 Preoperative Patient Demographics |
Three-month post-surgery, the visual acuity and refractive outcomes are presented in Table 2. There were no significant differences in monocular UDVA and CDVA between the two groups (all P > 0.05). No statistically significant differences were observed between the groups in binocular UDVA, CDVA, and uncorrected near visual acuity (UNVA) (all P > 0.05). However, the mix group demonstrated better binocular uncorrected intermediate visual acuity (UIVA) compared to the bilateral group (0.10 ± 0.12 vs 0.23 ± 0.14 logMAR, P = 0.005).
 |
Table 2 Refractive Outcomes and Binocular Visual Acuities 3 Months After IOL Implantation |
The binocular defocus curve revealed consistent performance from far to near distances, with the mix group showing superior visual acuity at −1D, −1.5D, and −2D compared to the bilateral group (P = 0.01, 0.008, and 0.012, respectively). Figure 1
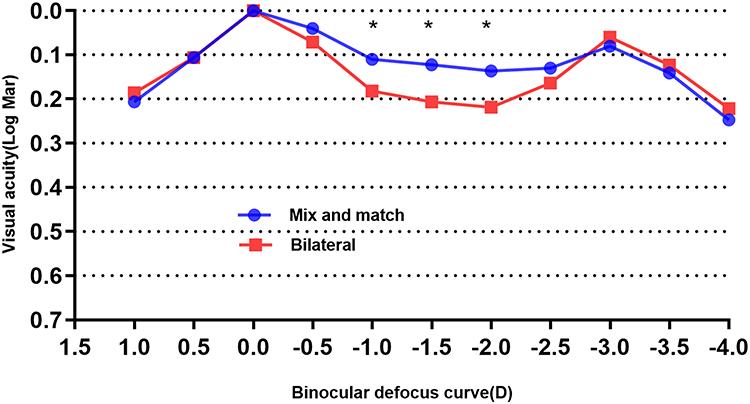 |
Figure 1 Binocular defocus curve 3 months after cataract surgery between the 2 groups. (*P<0.05). |
There were no significant differences in over satisfaction, a self-assessment of visual quality, or the percentage of visual disturbances between the two groups. (all P > 0.05) In the mix group, 96.0% of patients did not require spectacles for far distance vision, similar to 96.3% in the bilateral group. For intermediate distance vision, 92.0% of patients in the mix group did not need spectacles, compared to 59.26% in the bilateral group (P = 0.0001). Regarding near distance vision, 92.0% of patients in the mix group did not need spectacles, compared to 96.3% in the bilateral group. Table 3
 |
Table 3 Subjective Evaluation by Questionnaires 3 Months After IOL Implantation |
Discussion
Many bifocal IOLs offer excellent visual acuity for both distant and near vision or for distant and intermediate vision.1 However, due to the growing necessity for distant, intermediate and near vision for activities in different life scenarios, many patients now seek to have both far, intermediate, and near vision at the same time in the case of implantation of bifocal IOLs. Given the variety of IOL options available for patients seeking presbyopia correction, surgeons face the challenge of selecting IOLs that offer the best combination of spectacle independence, minimal photic phenomena and high patient satisfaction.12 To overcome this challenge of bifocal IOLs, an innovative way for achieving good vision in all three focus areas on a two-focus basis was devised in the 1990s, known as the mix-and-match method.13
The mix-and-match method is based on the assumption that hyperopia results in a clear high contrast image in the dominant eye, while myopia results in a sharp high contrast image in the non-dominant eye, resulting in binocular superposition, or binocular vision with a higher visual sensitivity than monocular vision.14 Previously published research shown that the mix-and-match strategy was used with diffractive multifocal IOLs or IOLs with an expanded depth of focus.8–12 It was reported that implanting ReSTOR +2.50 D IOLs in a combination of ReSTOR +3.00 D diffractive bifocal IOLs produced near vision that was on par with that of bilaterally implanting ReSTOR +2.50 D diffractive bifocal IOLs in a prospective, randomized parallel-group investigation.8 Tarib et al10 reported patients implanted bilaterally with an EDOF IOL AT LARA 829MP showed good levels of satisfaction and visual quality, while patients implanted with a mix-and-match of an EDOF IOL and a diffractive trifocal IOL AT Lisa tri 839MP had better near visual acuity. Wendelstein et al12 used mix-and-match approach with a spherical monofocal IOL in the dominant eye and an EDOF IOL in the non-dominant eye, concluding that this method provides excellent distance vision, improved intermediate and near vision, and high patient satisfaction. Despite this, only a few clinical studies have looked at the mix-and-match method using rotationally asymmetric multifocal IOLs.
Vargas et al5 used a mix-and-match strategy to implant the LS-313MF30(+3.00D) in the non-dominant eye and the LS-313MF15(+1.50 D) in the dominant eye to achieve adequate distance, intermediate, and near vision while maintaining acceptable contrast sensitivity and patients’ satisfaction. However, this study only focused on the mix-and-match method of rotationally asymmetric multifocal IOLs and did not compare with other methods or IOLs. This method has not been thoroughly compared to traditional bilateral symmetric implantations. Mix-and-match rotationally asymmetric multifocal IOLs (LENTIS Mplus LS-313 +3.00 and +1.50 D) have been compared to bilateral multifocal lenses (LENTIS Mplus LS-313 +3.00D) in terms of visual performance in this study. This study’s findings revealed that the mix-and-match group had better intermediate-distance binocular vision than the bilateral group.
The mix-and-match group had a considerably lower binocular UIVA (0.10 ± 0.12 LogMAR) than the bilateral group (0.23 ± 0.14 LogMAR), demonstrating that mix-and-match refractive rotationally asymmetric multifocal IOLs produce better UIVA than bilateral multifocal IOLs. Both groups had satisfactory binocular UDVA, CDVA, and UNVA following IOL implantation, which was consistent with previous research.5,15 As a result, both the mix group and the bilateral group obtained remarkable distant and near visual outcomes, as well as functional restoration following cataract surgery. Due to the better binocular UIVA, the mix group had a much higher rate of intermediate spectacle independence (92.0%) than the bilateral group (59.26%).
The defocus curve is a valuable technique for evaluating multifocal intraocular lens visual performance.16 Similar to Vargas et al’s5 findings, we found that the mix group achieved good distance, intermediate, and near vision for the mix-and-match method’s beneficial summation effect and that the mix group’s intermediate vision was superior to the bilateral group, as demonstrated by the binocular defocus curve between the two groups.
Subjective questionnaires are often evaluated as important results to determine the patient’s subjective feelings.17 Both the mix-and-match and bilateral groups achieved a superior overall satisfaction and a greater independence from distant and near spectacles. As previously stated, the mix-and-match group’s superior intermediate vision contributed to the considerable difference in intermediate spectacle independence between the two groups.
The study has the following limitations: the follow-up time was brief; therefore, long-term follow-up of beyond 3 months is needed to consider neuroadaptation. Second, the patients who were included were not randomly assigned; rather, they were divided according to their personal preferences. A randomized study is regarded as the most appropriate method for removing patient bias. Finally, we did not perform contrast sensitivity tests. We should investigate contrast sensitivity in a future study due to the scarcity of current research circumstances.
Conclusion
Mix-and-match implantation of the +1.50D and +3.00D rotationally asymmetric multifocal IOLs provided better intermediate vision than bilateral implantation of +3.00D IOLs.
Institutional Review Board Statement
The study adhered to the guidelines of the Declaration of Helsinki and received approval from the Ethics Committee of Qingdao Eye Hospital of Shandong First Medical University, with the approval number QYLS 2019(06).
Data Sharing Statement
Further enquiries can be directed to the corresponding author.
Funding
No funding was received for this article.
Disclosure
The author declares no conflicts of interest about this study.
References
1. Alio JL, Plaza-Puche AB, Fernandez-Buenaga R, et al. Multifocal intraocular lenses: an overview. Surv Ophthalmol. 2017;62(5):611–634. doi:10.1016/j.survophthal.2017.03.005
2. Rampat R, Gatinel D. Multifocal and extended depth-of-focus intraocular lenses in 2020. Ophthalmology. 2021;128(11):e164–e185. doi:10.1016/j.ophtha.2020.09.026
3. Nuzzi R, Tripoli F, Ghilardi A. Evaluation of the effects of multifocal intraocular lens oculentis LENTIS Mplus LS-313 MF30 on visual performance in patients affected by bilateral cataract and treated with phacoemulsification. J Ophthalmol. 2022;2022:1315480. doi:10.1155/2022/1315480
4. Alvarez-Garcia MT, Rivera-Ruiz E, Alio JL, et al. Long-term prevalence of opacification of a hydrophylic acrylic rotationally asymmetric refractive multifocal intraocular lens. J Refract Surg. 2024;40(2):e98–e107. doi:10.3928/1081597X-20240115-01
5. Vargas V, Ferreira R, Alio Del Barrio JL, et al. Visual outcomes, patient satisfaction, and light distortion analysis after blended implantation of rotationally asymmetric multifocal intraocular lenses. J Refract Surg. 2020;36(12):796–803. doi:10.3928/1081597X-20200902-01
6. Li H, Liu D, Gao H, et al. Visual performance following bilateral implantation of refractive rotationally asymmetric bifocal intraocular lens (LS-313 MF30) or apodized diffractive bifocal intraocular lens (ReSTOR SN6AD1). Ther Clin Risk Manage. 2021;17:917–926. doi:10.2147/TCRM.S325287
7. Moore JE, McNeely RN, Pazo EE, et al. Rotationally asymmetric multifocal intraocular lenses: preoperative considerations and postoperative outcomes. Curr Opin Ophthalmol. 2017;28(1):9–15. doi:10.1097/ICU.0000000000000339
8. Nuijts RM, Jonker SM, Kaufer RA, et al. Bilateral implantation of +2.5 D multifocal intraocular lens and contralateral implantation of +2.5 D and +3.0 D multifocal intraocular lenses: clinical outcomes. J Cataract Refract Surg. 2016;42(2):194–202. doi:10.1016/j.jcrs.2016.02.009
9. Bilbao-Calabuig R, Gonzalez-Lopez F, Amparo F, et al. Comparison between mix-and-match implantation of bifocal intraocular lenses and bilateral implantation of trifocal intraocular lenses. J Refract Surg. 2016;32(10):659–663. doi:10.3928/1081597X-20160630-01
10. Tarib I, Kasier I, Herbers C, et al. Comparison of visual outcomes and patient satisfaction after bilateral implantation of an EDOF IOL and a mix-and-match approach. J Refract Surg. 2019;35(7):408–416. doi:10.3928/1081597X-20190417-02
11. Hammond MD, Potvin R. Visual outcomes, visual quality and patient satisfaction: comparing a blended bifocal approach to bilateral extended depth of focus intraocular lens implantation. Clin Ophthalmol. 2019;13:2325–2332. doi:10.2147/OPTH.S232800
12. Wendelstein JA, Casazza M, Reifeltshammer S, et al. Unilateral intraindividual comparison and bilateral performance of a monofocal spherical and diffractive extended depth of field intraocular lens mix-and-match approach. Clin Exp Ophthalmol. 2024;52(1):31–41. doi:10.1111/ceo.14315
13. Jacobi KW, Eisenmann D. Asymmetrische Mehrzonenlinsen - ein neues Konzept multifokaler Intraokularlinsen [Asymmetric multizone lenses--a new concept in multifocal intraocular lenses]. Klinische Monatsblatter fur Augenheilkunde. 1993;202(4):309–314. doi:10.1055/s-2008-1045597 German
14. Campbell FW, Green DG. Monocular versus binocular visual acuity. Nature. 1965;208(5006):191–192. doi:10.1038/208191a0
15. Alio JL, Plaza-Puche AB, Pinero DP, et al. Comparative analysis of the clinical outcomes with 2 multifocal intraocular lens models with rotational asymmetry. J Cataract Refract Surg. 2011;37(9):1605–1614. doi:10.1016/j.jcrs.2011.03.054
16. Vargas V, Radner W, Allan BD, et al. Methods for the study of near, intermediate vision, and accommodation: an overview of subjective and objective approaches. Surv Ophthalmol. 2019;64(1):90–100. doi:10.1016/j.survophthal.2018.08.003
17. Grzybowski A, Kanclerz P, Muzyka-Wozniak M. Methods for evaluating quality of life and vision in patients undergoing lens refractive surgery. Graefes Arch Clin Exp Ophthalmol. 2019;257(6):1091–1099. doi:10.1007/s00417-019-04270-w
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.