")
Back to Journals » Journal of Pain Research » Volume 17
Compound Probiotics Improve Neuropathic Pain Prognosis in a Murine Model of Chronic Constriction Injury
Authors Wang X, Chen Y, Qian S , Kong J, Su Z, Wang Q, Liao L
Received 10 July 2024
Accepted for publication 19 November 2024
Published 11 December 2024 Volume 2024:17 Pages 4213—4221
DOI https://doi.org/10.2147/JPR.S486259
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Wendy Imlach
Xiaomei Wang,1,2 Yinsheng Chen,3 Shuwen Qian,4 Jia Kong,2 Zehua Su,5 Qingxiu Wang,3,* Lijun Liao5,*
1Department of Anesthesiology and Surgical Intensive Care Unit, Xinhua Hospital, School of Medicine, Shanghai Jiaotong University, Shanghai, People’s Republic of China; 2Department of Anesthesiology Management, Shanghai East Hospital, School of Medicine, Tongji University, Shanghai, People’s Republic of China; 3Shanghai East Hospital Clinical Medical College, Nanjing Medical University, Shanghai, People’s Republic of China; 4Department of Anesthesiology and Pain Management, Yangpu Hospital, School of Medicine, Tongji University, Shanghai, People’s Republic of China; 5Department of Pain Management, Shanghai East Hospital, School of Medicine, Tongji University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qingxiu Wang, Shanghai East Hospital Clinical Medical College, Nanjing Medical University, No. 1800, YunTai Road, Shanghai, 200123, People’s Republic of China, Tel +86 13310054121, Email [email protected] Lijun Liao, Department of Pain Management, Shanghai East Hospital, School of Medicine, Tongji University, No. 1800, YunTai Road, Shanghai, 200123, People’s Republic of China, Tel +86 13817428913, Email [email protected]
Purpose: Compound probiotics have been reported to ameliorate imbalances in the intestinal flora that may play a critical role in neuropathic pain. This study aimed to investigate the efficacy of compound probiotic treatment on neuropathic pain.
Methods: Thirty mice were randomly divided into three groups: 1) sham group, 2) mouse with chronic constrictive injury (CCI), and 3) probiotic gavage with CCI (CCI+Prob). The degree of pain and gait recovery was assessed by Mechanical withdrawal threshold (MWT), thermal withdrawal latency (TWL), and mouse footprints. The degree of atrophy of the gastrocnemius muscle was assessed by muscle weight, hematoxylin and eosin (H&E) staining. Gut microbiota were analyzed by 16S ribosomal RNA sequencing (16SrRNA).
Results: Four weeks after surgery, TWL and MWT assessment showed significant increases in the CCI+Prob group compared with the CCI group (P < 0.01). Gait analysis results as well as gastrocnemius muscle weight showed a significant improvement in the CCI+Prob group compared with the CCI group. Measurement of alpha diversity showed a significant increase in the CCI group compared with the sham group, but this increase was attenuated by probiotic intervention in the CCI+Prob group. Although the CCI group had significantly decreased levels of Akkermansia and significantly increased levels of Ruminococcaceae, probiotic treatment reversed these changes.
Conclusion: Compound probiotics treatment can improve the pain and muscle atrophy in mice with CCI-induced neuropathic pain. The improvement of symptoms is associated with changes in the composition of gut microbiota.
Keywords: probiotics, neuropathic pain, gut microbiota, muscle atrophy, Akkermansia, Ruminococcaceae
Introduction
Neuropathic pain can occur within the case of a lesion or disease of the somatosensory nervous system1,2 and has the key manifestations of hyperalgesia, spontaneous pain, and psychiatric comorbidities, which in turn enhance pain perception.3 Neuropathic pain may also directly and indirectly affect muscle function via activity restriction and immobility.4 This pain impairs physical, mental, and emotional function, which can significantly reduce quality of life. A multidisciplinary approach toward treatment combining pharmacological interventions, such as antidepressants, antiepileptics, or opioids, with physical or cognitive interventions is now advocated.5,6 Nevertheless, epidemiological surveys have shown that a significant number of patients do not receive appropriate treatment.7,8 The recurrent nature of refractory pain and the adverse effects stemming from the prolonged use of opioids are well known. It is imperative to account for the potential risks associated with long-term opioid consumption and consider the use of other gentler and more effective strategies for treating intractable pain and related symptoms.
Humans harbor trillions of microorganisms, most of which reside in microbial communities within the gastrointestinal tract. Previous studies have verified the role of gut microbiota in maintaining host health by modulating intestinal permeability, digestion, metabolism, and immune response.9–12 However, most studies have focused on conditions such as cancer, malnutrition, and age-related diseases.13–15
Gut microbial composition is dynamic and can be affected by the host’s diet, lifestyle, hygiene, and use of antibiotics. The relationship between gut microbiota and pain has been described in the last years, specifically in alleviating abdominal pain.16 In recent years, growing evidence suggests that gut microbiota plays a role in both acute and chronic pain17–19 The findings have also shown the potential effectiveness of probiotics in the treatment of inflammatory diseases.20–22 It works primarily by modulating the immune system.23–25 We know that pain and inflammation are closely related. The inflammatory response plays a pivotal role in the transition of the pain process. A study using an in vitro model of sensitive neuron reported that paclitaxel (PTX)-induced neuropathic pain could be counteracted by administration of a high-concentration probiotic formulation.21 Despite the possibility of modulating gut flora–pain interactions with probiotics, no studies have evaluated the prognosis of compound probiotics in neuropathic pain. Therefore, in the present study, we described for the first time the effect of compound probiotics on pain threshold, degree of muscle atrophy, and gait using the CCI mouse model and conducted a preliminary exploration of possible mechanisms.
Material and Methods
Animals
Adult male C57BL/6J mice weighing 22–25 g were obtained from the Animal Experiment Center Institute of Regenerative Medicine, Shanghai East Hospital. All animals were raised in a 12:12 h light-to-dark cycle with ad libitum access to food and water. To ensure the reliability of the experiment two pain-hypersensitive mice and two hypalgesic mice were excluded from each group.
CCI Modeling
The CCI model was developed as described by Bennett in 1988.26 Each mouse was anesthetized by intraperitoneal injection of 5% chloral hydrate (0.1 mL/10 g). The sciatic nerve was bluntly separated and surrounded with 4–0 sutures made with 2 light ligation loops in 1 mm intervals and tightened until the thigh muscles twitched. The mice were randomly assigned to three groups: CCI with normal saline gavage group (CCI group), CCI with probiotic gavage group (CCI+Prob group), and a sham group that underwent the same procedure without sciatic nerve ligation (sham group).
Compound Probiotics
Probiotics were purchased from Wuhan Senlan Biological Company, China, containing the following 15 trains: Bifidobacterium animalis ssp. Lactis HN019, Bifidobacterium bifidum Bb06, Bifidobacterium animalis ssp. lactis BB-12, Bifidobacterium animalis ssp. lactis Bi07, Bifidobacterium longum R175, Bifidobacterium animalis B94, Lactobacillus rhamnosus GG, Lactobacillus casei LC11, Lactobacillus helveticus R52, Lactobacillus paracasei Lpc37, Lactobacillus plantarum R1012, Lactobacillus reuteri HA188, Lactobacillus rhamnosus R11, Lactobacillus acidophilus NCFM, and Streptococcus thermophiles St21. Each gram contained 10 billion viable colony-forming units (CFUs). According to dose translation from animal to human,27 each mouse in the CCI+Prob group was administered 2.5 ×107CFU/g/day. To avoid loss of active cultures, the probiotic powder was stored at 4°C and kept away from heat and light. The probiotic mixture was added to saline to make a probiotic suspension, and administered through intragastric gavage.
Thermal Withdrawal Latency Test
A plantar algometer (Tes7370, Ugo Basile, Comerio, Italy) was used to measure the TWL of the injured limb by detection of infrared irradiation on the plantar surface of the mouse paw. Three independent measurements were performed for each mouse with 30-s intervals. Latency was defined as the average interval duration of three measurements before the mouse licked a hind paw or withdrew. A threshold time of 22 seconds was set to prevent tissue damage.
Mechanical Withdrawal Threshold Test
Before the assessment of the MWT, mice were placed on metal grids and acclimated for 30 min, avoiding the stress resulting from the test conditions. While the mice were quiet, Von Frey fibers were used to vertically stimulate the operative paws of the mice for 4–6 s with a 30-s interval. When foot withdrawal or foot licking was observed, it was regarded as a positive reaction and recorded as “X”, whereas no reaction was recorded as “O”. The order of stimulation intensity of fiber silk was 0.4, 0.6, 1, 2, 4, 6, 8, 10, and 15 g, Stimulation intensity was started at 2 g and decreased when a positive response occurred and increased if no response occurred. Measurements were applied six times, and the final mechanical pain threshold was recorded against the threshold table.
Measurement of Murine Footprints
The experimental design was based on a previous study by Wertman et al,28 which took advantage of natural mouse behavior and affinity for small, dark places. Mice were placed on a tunnel 5 cm in width, 10 cm in height, and 100 cm in length. The soles of the mice were evenly dipped in ink before they walked across smooth white paper within a tunnel. Footsteps that were consistently clearly spaced and non-smudged were used for analysis.
Tissue Collection
After behavioral testing was conducted on day 28 post-surgery, the mice were sacrificed by an overdose of sevoflurane. The gastrocnemius muscle on the operated side of the mouse was removed and fixed in 4% paraformaldehyde, dehydrated, embedded in paraffin wax, and serially sectioned at 6 mm for immunofluorescent and hematoxylin and eosin (H&E) staining.
Statistical Analysis
All data are presented as the mean ± standard deviation. Data were analyzed by one-way analysis of variance followed by the Bonferroni multiple comparison post-hoc test using GraphPad Prism Software version 6.0 (Boston, MA, USA). A P value <0.05 was considered an indication of statistical significance.
Results
Compound Probiotics Improve Pain and Gait in Neuropathic Murine Model
One week after surgery, compound probiotics or normal saline was administered by intragastric gavage for three consecutive weeks according to the requirements of the group. The MWT and TWL of each group were assessed before surgery and at 1, 2, 3, and 4 weeks after surgery. All the results showed that the MWT and TWL of the CCI and CCI+Prob groups had significantly decreased 1 week after CCI surgery (P<0.05). Compared with those of the CCI group, the MWT and TWL of the CCI+Prob Group had significantly increased after 3 weeks of gavage (P<0.01; Figure 1A and B). The weight of the surgery groups all showed a decrease, but the prob group tended to increase compared with the CCI group, although the difference between them did not reach statistical significance (Figure 1C).
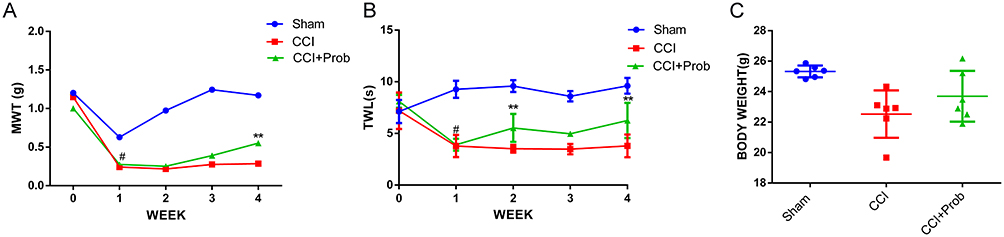 |
Figure 1 Comparison of mechanical withdrawal threshold (A), thermal withdrawal latency (B), and body weight (C) of sham, CCI, and CCI+Prob groups before and after surgery. Values were measured 0, 1, 2, 3, and 4 weeks after surgery. #P < 0.05 0 vs 1 week for mechanical withdrawal threshold and thermal withdrawal latency; **P < 0.01 CCI vs CCI+Prob group. |
Gait analysis of the right hind paw revealed that both the shape and clarity of the footprints of the CCI and CCI+Prob groups significantly differed from those of the sham group (Figure 2A). The clarity of the footprints of the CCI+Prob group was relatively improved compared with that of the CCI group, suggesting that the CCI+Prob group had a stronger grip on the ground. The analysis revealed no significant change in the toe length of the surgical paws of the three groups (P > 0.05; Figure 2B), The CCI+Prob group displayed a significantly increased toe spreading length (P < 0.05; Figure 2C) and stride length (P < 0.05; Figure 2D) compared with the CCI group.
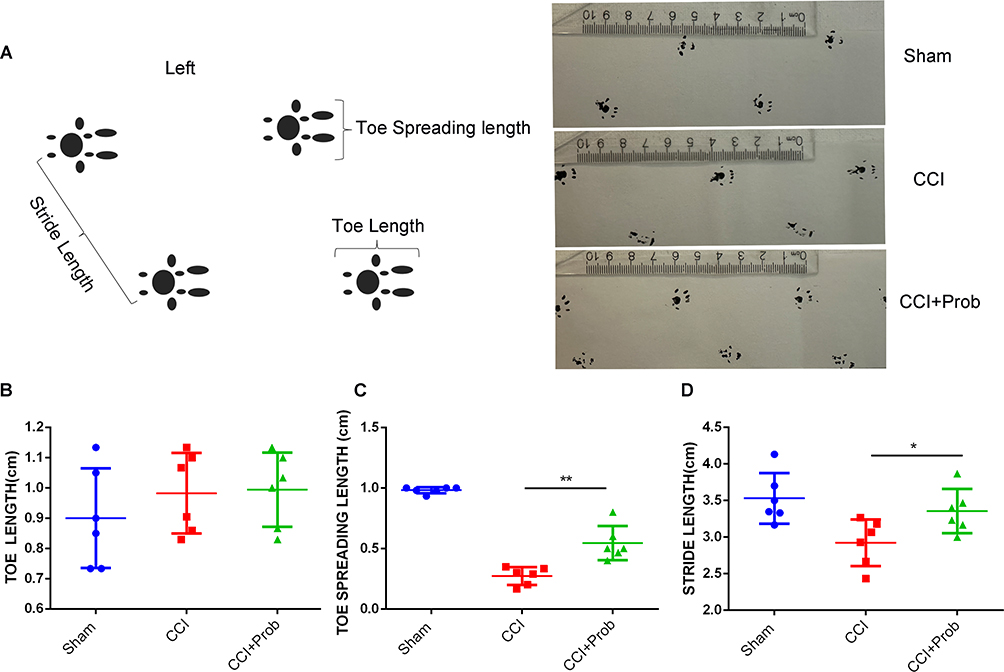 |
Figure 2 (A) Gait analysis results. (B) No changes were detected in the toe-spreading length of the surgical paw in the sham, CCI, or CCI+Prob group. (C and D) CCI+Prob group displayed a significantly increased toe-spreading and stride length compared with the CCI group. *P < 0.05 CCI vs CCI+Prob group; **P < 0.01 CCI vs CCI+Prob group. |
Compound Probiotic Treatment Improves CCI-Induced Neuromuscular Atrophy
The gastrocnemius muscle is one of the main muscles innervated by the sciatic nerve that showed varying degrees of atrophy after sciatic nerve ligation. The atrophy of the gastrocnemius muscle on the surgical side of the mice was significantly improved in the CCI+Prob group (P<0.05; Figure 3A). Comparison of H&E-stained transverse sections of the gastrocnemius muscle revealed a high number of muscle fibers with centrally located nuclei in the CCI group, a primary pathological sign of muscular dystrophy. The muscle fibers of CCI mice were smaller compared with those of the other two groups, and smaller muscle fibers were more commonly distributed in the muscles of CCI mice. Such phenomenon improved in the CCI+Prob group (Figure 3B). We observed that the weight of the gastrocnemius muscle was reduced in both the CCI group and the CCI+Prob group compared to the sham group. However, the weight of the gastrocnemius muscle was significantly increased in the CCI+Prob group than in the CCI group. (P<0.05; Figure 3C).
 |
Figure 3 (A) Gross morphology of gastrocnemius muscle. (B) Gastrocnemius muscle cross section from hematoxylin and eosin stain. (C) CCI+Prob group displays a significant increase in gastrocnemius muscle weight. *P < 0.05 CCI vs CCI+Prob group. |
Intestinal Flora Diversity is Altered with CCI-Induced Neuropathic Pain
Using 16S rRNA gene sequencing to measure microbial populations, we detected structural differences in the microbial composition of the feces of the three groups (Figure 4A). The Linear Discriminant Analysis Effect Size (LEfSe) tool was used to analyze the data, which shows a range of discriminating biomarkers across all taxonomic levels. We can identify those taxa of different levels were differentially abundant in the three groups (Figure 4B). Using the Shannon index to analyze the alpha diversity, which refers to the diversity of bacteria or species, we observed a significant increase in the CCI group compared with the sham group (Figure 4C). Furthermore, we found a clear downward trend in the diversity of the CCI+Prob group despite detecting no significant differences between the CCI and CCI+Prob groups.
 |
Figure 4 Differential profiles of gut microbiota among three study groups. (A) Taxonomic composition of gut microbiota. (B) Taxa identified by LEfSe as biomarkers of samples from the Sham group, CCI group, and the Prob group (cutoffs were LDA ≥ 4 and p-value ≤ 0.05) (C) Shannon index, an α-diversity indicator, of gut microbiota. |
Using the DESeq2 method to further analyze the results of pairwise comparisons, we found that the level of phylum Verrucomicrobia significantly decreased while the level of family Ruminococcaceae significantly increased in the CCI group. However, probiotic treatment reversed the CCI-induced changes in the relative abundance of Verrucomicrobia and Ruminococcaceae in the CCI+Probiotics group (Table 1). We also observed this phenomenon in the relative abundance of Akkermansia, which is the only genus of bacteria in the phylum Verrucomicrobiota known to be in the gut.
 |
Table 1 Changes at Different Levels in Gut Microbiota |
Discussion
Patients with neuropathic pain accompanied by muscle atrophy experience a decline in muscle strength, gait speed, and athletic ability, negatively impacting their quality of life. The results of our comparison of footprint clarity, stride length and toe-spreading length in three groups of mice indicate that compound probiotic treatment can attenuate nociceptive hypersensitivity in a CCI-induced neuropathic pain model. We found that the gait of the mice who had undergone probiotic treatment was closer to that of healthy mice than the mice that had not undergone probiotic treatment, suggesting that the probiotic treatment had improved lameness in the CCI group. These findings are consistent with previous findings that muscle wasting and dysfunction can be delayed by intervening in the microbe–muscle axis with probiotic treatment.29–31
To compare the changes in gut microbiota in the three experimental groups, we measured the alpha diversity, an indicator of bacterial diversity, using the Shannon index. We found that the relative abundance of microbiota in the CCI group was higher than that of the sham group, as well as that the improvement of symptoms in the CCI+Prob group was accompanied by a reduction in changes in the gut microbiota. Interestingly, we also observed that probiotic treatment reversed the reduction in levels of Akkermansia, bacteria associated with inflammatory diseases and metabolic disorders that can convert mucin to short-chain fatty acids (SCFAs) that may mediate immunoregulatory effects.32–34 Akkermansia adheres to the mucus layer to strengthen intestinal barrier function to protect epithelial cells from microbial attacks.35 Moreover, it acts as a nutrient providing energy for microorganism growth. Experiments on hamsters provided evidence that Akkermansia provides a competitive advantage during stressful events, such as fasting and malnutrition.36 A similar significant trend regarding an increase in levels of Akkermansia has been reported in the context of immune-based diseases.37,38
The family Ruminococcaceae acts as a key component of the microbiota in humans by maintaining homeostasis of the gut microenvironment. Although we found that levels of Ruminococcaceae significantly increased in the CCI group, this increase was reversed by probiotic treatment. Most studies have found higher levels of Ruminococcaceae in healthy controls, and only some studies reported mixed results, such as that increased levels of Ruminococcaceae correlate with longer Parkinson’s disease duration.39 A case study reported that Ruminococcaceae levels increased significantly and progressively with improvement in bipolar depression symptomology.40 Nevertheless, few studies have examined the relationship between disease and Ruminococcaceae levels despite their fluctuations possibly being related to specific diseases. As the development and progression of CCI-induced neuropathic diseases could be associated with levels of Akkermansia and Ruminococcaceae, they could serve as the pathological foundations of muscle atrophy and nociceptive hypersensitivity in disease progression and may even serve as therapeutic targets or markers.
Probiotics appear to act as antioxidants, namely the production of antioxidant enzymes and metabolites like lactate.41,42 In addition, probiotics inhibit the TLR4/NF-κB pathway activated by gut-derived lipopolysaccharide and reduce the production of inflammatory factors.43 Studies have shown that reactive oxygen species as well as inflammatory responses play an important role in neuropathic pain and are involved in central sensitization.44,45 Therefore, we speculate that the antioxidant properties of probiotics and the reduction of inflammatory factor production may also be one of the mechanisms in alleviating symptoms of neuropathic pain.
In our CCI-induced neuropathic pain murine model, we observed changes in gut microbiota that we attempted to modify with compound probiotics to treat the neuropathic pain. The most significant limitation of our study was the limited period of observation. Despite this limitation, our findings strongly suggest that targeting the gut microbiota might be a novel treatment for neuropathic pain or even a means of alleviating skeletal muscle atrophy. The potential role of compound probiotics should be examined within the context of the interaction of significant factors in pain development and management. Further studies are needed to explore how changes in gut microbiota can be used to improve disease symptoms in neuropathic pain.
Conclusion
Our findings provide evidence that compound probiotic treatment provides some degree of relief from neuropathic pain and its associated symptoms, supporting previous observations that probiotic treatment could be a means of managing inflammation-related pain symptoms. We also provide evidence that changes in the composition of gut microflora are associated with the development of neuropathic pain. Among the microflora for which we detected changes in levels, we observed that Akkermansia and Ruminococcaceae were related to disease progression, suggesting that they could be utilized as targets for treatment or as markers for disease progression.
Abbreviations
CCI, chronic constrictive injury; Prob, probiotics; TWL, thermal withdrawal latency; MWT, mechanical withdrawal threshold; H&E, hematoxylin and eosin; 16SrRNA, 16S ribosomal RNA sequencing; CFUs, colony-forming units; LEfSe, Linear Discriminant Analysis Effect Size.
Data Sharing Statement
Data supporting the findings of this study are available from the corresponding author on request.
Ethics Approval
All ethical principles are considered in this commentary. All ethical principles are considered in all experimental procedures. All procedures were conducted in compliance with the Animal Experiment Regulations of Tongji University Experimental Animal Center, the Animal Experiment Committee Regulations, and the Animal Experiment Approval Provisions (Approval Nos: TJBB03124102).
Acknowledgments
We thank all the authors of the papers mentioned in the references.We also would like to thank Wuhan Senlan Biological Company for providing the compound probiotics.
Funding
This work was supported by Shanghai’s 2023 “Technology Innovation Action Plan” medical innovation research project (23Y11908300), the National Natural Science Foundation of China (82202401, 8217010632), Important Weak Subject Construction Project of Shanghai Pudong New Area Health Commission (Grant No. PWZbr2022-01), Pudong New Area Peak-Plateau Discipline Construction: Clinical Medicine New Quality Specific Department(Specific Disease) Project 2024-PWXZ-023.
Disclosure
The authors declare that they have no competing interests.
References
1. Finnerup NB, Attal N, Haroutounian S, et al. Pharmacotherapy for neuropathic pain in adults: a systematic review and meta-analysis. Lancet Neurol. 2015;14(2):162–173. doi:10.1016/s1474-4422(14)70251-0
2. Gierthmühlen J, Baron R. Neuropathic pain. Semin Neurol. 2016;36(5):462–468. doi:10.1055/s-0036-1584950
3. Finnerup NB, Kuner R, Jensen TS. Neuropathic pain: from mechanisms to treatment. Physiol Rev. 2021;101(1):259–301. doi:10.1152/physrev.00045.2019
4. Moes JR, Holden JE. Characterizing activity and muscle atrophy changes in rats with neuropathic pain: a pilot study. Biol Res Nurs. 2014;16(1):16–22. doi:10.1177/1099800413502722
5. Maleki MS, Zamani Z, Amiri R, et al. Pregabalin in patients with post-traumatic peripheral neuropathic pain: a meta-analysis of randomized controlled trials. Pain Pract. 2023;23(6):595–602. doi:10.1111/papr.13221
6. Tai LW, Yeung SC, Cheung CW. Enriched environment and effects on neuropathic pain: experimental findings and mechanisms. Pain Pract. 2018;18(8):1068–1082. doi:10.1111/papr.12706
7. Andrew Moore R. What works for whom? Determining the efficacy and harm of treatments for pain. Pain. 2013;154 Suppl 1:S77-s86. doi:10.1016/j.pain.2013.03.024
8. Ghazisaeidi S, Muley MM, Salter MW. Neuropathic pain: mechanisms, sex differences, and potential therapies for a global problem. Annu Rev Pharmacol Toxicol. 2023;63:565–583. doi:10.1146/annurev-pharmtox-051421-112259
9. Sánchez B, Delgado S, Blanco-Míguez A, Lourenço A, Gueimonde M, Margolles A. Probiotics, gut microbiota, and their influence on host health and disease. Mol Nutr Food Res. 2017;61(1). doi:10.1002/mnfr.201600240
10. Sommer F, Bäckhed F. The gut microbiota--masters of host development and physiology. Nat Rev Microbiol. 2013;11(4):227–238. doi:10.1038/nrmicro2974
11. Li XV, Leonardi I, Iliev ID. Gut mycobiota in immunity and inflammatory disease. Immunity. 2019;50(6):1365–1379. doi:10.1016/j.immuni.2019.05.023
12. Perler BK, Friedman ES, Wu GD. The Role of the Gut Microbiota in the Relationship Between Diet and Human Health. Annu Rev Physiol. 2023;85:449–468. doi:10.1146/annurev-physiol-031522-092054
13. Chen LH, Huang SY, Huang KC, et al. Lactobacillus paracasei PS23 decelerated age-related muscle loss by ensuring mitochondrial function in SAMP8 mice. Aging. 2019;11(2):756–770. doi:10.18632/aging.101782
14. Wong CC, Yu J. Gut microbiota in colorectal cancer development and therapy. Nat Rev Clin Oncol. 2023;20(7):429–452. doi:10.1038/s41571-023-00766-x
15. Bauer KC, York EM, Cirstea MS, et al. Gut microbes shape microglia and cognitive function during malnutrition. Glia. 2022;70(5):820–841. doi:10.1002/glia.24139
16. Rousseaux C, Thuru X, Gelot A, et al. Lactobacillus acidophilus modulates intestinal pain and induces opioid and cannabinoid receptors. Nature Med. 2007;13(1):35–37. doi:10.1038/nm1521
17. Santoni M, Miccini F, Battelli N. Gut microbiota, immunity and pain. Immunol Lett. 2021;229:44–47. doi:10.1016/j.imlet.2020.11.010
18. Liu L, Wu Q, Chen Y, et al. Gut microbiota in chronic pain: novel insights into mechanisms and promising therapeutic strategies. Int Immunopharmacol. 2023;115:109685. doi:10.1016/j.intimp.2023.109685
19. Manske S. The microbiome’s role in chronic pain and inflammation. Integr Med. 2024;23(4):10–15.
20. Huang J, Zhang C, Wang J, Guo Q, Zou W. Oral Lactobacillus reuteri LR06 or Bifidobacterium BL5b supplement do not produce analgesic effects on neuropathic and inflammatory pain in rats. Brain Behav. 2019;9(4):e01260. doi:10.1002/brb3.1260
21. Castelli V, Palumbo P, d’Angelo M, et al. Probiotic DSF counteracts chemotherapy induced neuropathic pain. Oncotarget. 2018;9(46):27998–28008. doi:10.18632/oncotarget.25524
22. Ticinesi A, Nouvenne A, Cerundolo N, et al. Gut microbiota, muscle mass and function in aging: a focus on physical frailty and Sarcopenia. Nutrients. 2019;11(7):1633. doi:10.3390/nu11071633
23. Hegazy SK, El-Bedewy MM. Effect of probiotics on pro-inflammatory cytokines and NF-kappaB activation in ulcerative colitis. World J Gastroenterol. 2010;16(33):4145–4151. doi:10.3748/wjg.v16.i33.4145
24. Cristofori F, Dargenio VN, Dargenio C, Miniello VL, Barone M, Francavilla R. Anti-inflammatory and immunomodulatory effects of probiotics in gut inflammation: a door to the body. Front Immunol. 2021;12:578386. doi:10.3389/fimmu.2021.578386
25. Ng SC, Hart AL, Kamm MA, Stagg AJ, Knight SC. Mechanisms of action of probiotics: recent advances. Inflammatory Bowel Dis. 2009;15(2):300–310. doi:10.1002/ibd.20602
26. Bennett GJ, Xie YK. A peripheral mononeuropathy in rat that produces disorders of pain sensation like those seen in man. Pain. 1988;33(1):87–107. doi:10.1016/0304-3959(88)90209-6
27. Reagan-Shaw S, Nihal M, Ahmad N. Dose translation from animal to human studies revisited. FASEB J. 2008;22(3):659–661. doi:10.1096/fj.07-9574LSF
28. Wertman V, Gromova A, La Spada AR, Cortes CJ. Low-cost gait analysis for behavioral phenotyping of mouse models of neuromuscular disease. J Visualized Exp. 2019;(149). doi:10.3791/59878
29. Bindels LB, Delzenne NM. Muscle wasting: the gut microbiota as a new therapeutic target? Int J Biochem Cell Biol. 2013;45(10):2186–2190. doi:10.1016/j.biocel.2013.06.021
30. Liu W, Zhou Y, Sun H, et al. Goat milk improves glucose homeostasis via enhancement of hepatic and skeletal muscle AMP-activated protein kinase activation and modulation of gut microbiota in streptozocin-induced diabetic rats. Mol Nutr Food Res. 2021;65(6):e2000888. doi:10.1002/mnfr.202000888
31. Lahiri S, Kim H, Garcia-Perez I, et al. The gut microbiota influences skeletal muscle mass and function in mice. Sci trans med. 2019;11(502). doi:10.1126/scitranslmed.aan5662
32. Derrien M, Belzer C, de Vos WM. Akkermansia muciniphila and its role in regulating host functions. Microb Pathogenesis. 2017;106:171–181. doi:10.1016/j.micpath.2016.02.005
33. Huck O, Mulhall H, Rubin G, et al. Akkermansia muciniphila reduces Porphyromonas gingivalis-induced inflammation and periodontal bone destruction. J Clin Periodontol. 2020;47(2):202–212. doi:10.1111/jcpe.13214
34. Zhang T, Li Q, Cheng L, Buch H, Zhang F. Akkermansia muciniphila is a promising probiotic. Microb Biotechnol. 2019;12(6):1109–1125. doi:10.1111/1751-7915.13410
35. Hänninen A, Toivonen R, Pöysti S, et al. Akkermansia muciniphila induces gut microbiota remodelling and controls islet autoimmunity in NOD mice. Gut. 2018;67(8):1445–1453. doi:10.1136/gutjnl-2017-314508
36. Sonoyama K, Fujiwara R, Takemura N, et al. Response of gut microbiota to fasting and hibernation in Syrian hamsters. Appl Environ Microbiol. 2009;75(20):6451–6456. doi:10.1128/aem.00692-09
37. Peng L, Gao X, Nie L, et al. Astragalin attenuates Dextran Sulfate Sodium (DSS)-induced acute experimental colitis by alleviating gut microbiota dysbiosis and inhibiting NF-κB activation in mice. Front Immunol. 2020;11:2058. doi:10.3389/fimmu.2020.02058
38. Routy B, Le Chatelier E, Derosa L, et al. Gut microbiome influences efficacy of PD-1-based immunotherapy against epithelial tumors. Science. 2018;359:6371):91–7. doi:10.1126/science.aan3706
39. Hill-Burns EM, Debelius JW, Morton JT, et al. Parkinson’s disease and Parkinson’s disease medications have distinct signatures of the gut microbiome. Mov Disord. 2017;32(5):739–749. doi:10.1002/mds.26942
40. Jiang HY, Xu LL, Zhang X, Zhang Z, Ruan B. The microbiome in bipolar depression: a longitudinal study of one pair of monozygotic twins. Bipolar disord. 2019;21(1):93–97. doi:10.1111/bdi.12736
41. Azcárate-Peril MA, Sikes M, Bruno-Bárcena JM. The intestinal microbiota, gastrointestinal environment and colorectal cancer: a putative role for probiotics in prevention of colorectal cancer? Am J Physiol Gastrointest Liver Physiol. 2011;301(3):G401–24. doi:10.1152/ajpgi.00110.2011
42. Wang Y, Wu Y, Wang Y, et al. Antioxidant properties of probiotic bacteria. Nutrients. 2017;9(5):521. doi:10.3390/nu9050521
43. Liu Q, Tian H, Kang Y, et al. Probiotics alleviate autoimmune hepatitis in mice through modulation of gut microbiota and intestinal permeability. J Nutr Biochem. 2021;98:108863. doi:10.1016/j.jnutbio.2021.108863
44. Gao X, Kim HK, Mo Chung J, Chung K. Reactive oxygen species (ROS) are involved in enhancement of NMDA-receptor phosphorylation in animal models of pain. Pain. 2007;131(3):262–271. doi:10.1016/j.pain.2007.01.011
45. Pottorf TS, Rotterman TM, McCallum WM, Haley-Johnson ZA, Alvarez FJ. The role of microglia in neuroinflammation of the spinal cord after peripheral nerve injury. Cells. 2022;11(13). doi:10.3390/cells11132083
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.