")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 17
Comprehensive Insights into the Economic Burden of Rheumatoid Arthritis in Latin America: A Systematic Literature Review of Regional Perspectives
Authors Maldonado-Restrepo AI, Acelas-Gonzalez GE , Rodríguez-Vargas GS , Rodriguez-Linares P , Gonzalez-Rodriguez JL, Rojas-Villarraga A , Santos-Moreno P
Received 2 October 2024
Accepted for publication 10 March 2025
Published 17 April 2025 Volume 2025:17 Pages 349—373
DOI https://doi.org/10.2147/CEOR.S498994
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xing Lin Feng
Angela Isabel Maldonado-Restrepo,1 Gabriel E Acelas-Gonzalez,2 Gabriel-Santiago Rodríguez-Vargas,3,4 Pedro Rodriguez-Linares,3 Javier-Leonardo Gonzalez-Rodriguez,1 Adriana Rojas-Villarraga,5 Pedro Santos-Moreno6
1School of Management and Business, Research Group Management and Business, Universidad del Rosario, Bogotá, Colombia; 2Research Vicerectory, Fundación Universitaria de Ciencias de la Salud – FUCS, Bogotá, Colombia; 3Research Department, Biomab – Center for Rheumatoid Arthritis, Bogotá, Colombia; 4Department Internal Medicine, Universidad del Bosque, Bogotá, Colombia; 5Research Institute, Fundación Universitaria de Ciencias de la Salud – FUCS, Bogotá, Colombia; 6Scientific Direction, Biomab – Center for Rheumatoid Arthritis, Bogotá, Colombia
Correspondence: Angela Isabel Maldonado-Restrepo, Universidad del Rosario, Bogotá, Colombia, 200th Street. North Highway. Module B, Tel +57 3102711396, Email [email protected]
Purpose: Rheumatoid arthritis (RA) affects approximately 0.3 to 1.2% of the world’s population. The objective of this study was to identify the existing literature on economic evaluations of RA in Latin America.
Patients and Methods: Studies of economic evaluations of patients with RA from 2000 to 2023 were analyzed using the databases PubMed, Scopus, Web of Science, Embase, Cochrane, and the Virtual Health Library following Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. Study quality was assessed using the Joanna Briggs Institute (JBI) tool, and qualitative analysis was done (following SwiM guidelines).
Results: A total of 851 articles were identified. Following the application of inclusion criteria to titles and abstracts, 117 articles were initially considered eligible. Of these, 42 were excluded due to population or outcome-based errors, leaving 27 articles and 48 abstracts for analysis. Duplicates were removed prior to this process. The included studies involved various designs: cross-sectional, longitudinal, prospective, and retrospective. Brazil accounted for the highest proportion of publications (33.3%), followed by Colombia and Mexico, each contributing 26%. Most economic studies focused on cost analysis (86%), while cost-effectiveness studies and cost-utility studies represented 7.4% and 3.3%, respectively. Predominant perspectives included third-party payer 26%, insurers 14.8%, social providers 7.4%, and mixed providers 3.7%. In terms of publications of abstracts, Colombia leaded at 35.4%. The predominant perspective was that of the provider 66.6%, including the general perspective (37.5%), private (34.3%), public (22%), and mixed (6.2%) and the perspective of third-party payers (33.3%).
Conclusion: Economic evaluations of rheumatoid arthritis in Latin America remain limited, with most studies focusing on cost analysis. Brazil, Colombia, and Mexico lead in publications, primarily from a provider perspective. Greater emphasis on cost-effectiveness and broader economic evaluations is needed to guide health policy in the region.
Keywords: economic burden, Latin America, rheumatoid arthritis
Introduction
The success of a health system is closely related to the type and risk of diseases present in a population, which directly impacts health care expenditure (HCE). Defined by the OECD (Organization for Economic Cooperation and Development), HCE represents the total resources allocated to health care goods and services, including treatment, rehabilitation, medical services, equipment, public health, and system administration. 1
High HCE is particularly evident in the case of high-cost or in some countries also known as catastrophic diseases. These diseases, as defined by the Pan American Health Organization (PAHO), are characterized by high costs, severe health impacts, and unsustainable household financing. Examples include chronic non-communicable diseases such as cancer, chronic kidney disease, and autoimmune diseases, which account for a significant portion of health care resources and impose a substantial financial burden on governments, health systems, and households.2 Among autoimmune diseases, rheumatoid arthritis (RA) stands out due to its significant impact on functional abilities of individuals and health systems. Affecting approximately 1% of the population, predominantly women, RA requires specialized treatment and generates considerable economic and social costs.3,4 These include direct medical expenses, labor-related costs (absenteeism, presenteeism, and unemployment), and broader social costs that challenge the sustainability of health and economic systems.5
A key measure to assess the burden of disease is disability-adjusted life years (DALYs), which quantify the years lost due to disability, illness, or premature death. In 2019, DALYs for RA in Latin America were highest in Mexico (0.30%), followed by Venezuela (0.24%), Colombia (0.21%), and Brazil and Argentina (both at 0.16%).6,7 The disease’s burden is compounded by comorbidities such as osteoporosis, hypertension, dyslipidemia, Sjögren’s syndrome, diabetes, renal disease, and cardiovascular disease, which significantly increase the cost of care8. It is common for a small percentage of the population to consume most of the available resources, in other words, 20 to 30% of the population may use 70% of the resources expended.9
The financial impact of RA is amplified by the introduction of costly pharmacological treatments, particularly biological drugs. While these drugs have improved disease management, they have substantially increased direct medical costs, including hospitalizations, outpatient visits and surgeries. In countries like Brazil, Argentina, Mexico, and Colombia, approximately 65% of HCE for RA is attributed to direct medical and non-medical costs, while indirect costs account for about 30%. These expenses can represent up to 50% of household income and tend to rise as the disease progresses7.
Socioeconomic disparities and differences in healthcare systems across regions significantly impact the economic burden of RA. The shortage of rheumatologists, particularly in rural areas, and the lack of primary care referral systems hinder early diagnosis and treatment.10 Additionally, limited access to conventional synthetic Disease-Modifying Antirheumatic Drugs (csDMARDs) and the low coverage of biological drugs (less than 10% in half of the countries) in public healthcare systems exacerbate the situation10. Factors such as low socioeconomic status and cultural barriers in rural and indigenous communities further restrict access to adequate care, increasing disability and worsening health outcomes.11
While studies on the economic evaluation of RA exist in Latin America and the Caribbean, the evidence remains limited, with most focusing primarily on direct and/or indirect costs. This highlights the need for more comprehensive economic evaluations to better understand the impact of RA in the region. Given the fragmented nature of the available literature and the lack of a complete synthesis, this study aims to conduct a systematic review to identify and analyze the main economic evaluations of RA in Latin America from 2000 to 2023, contributing to the knowledge base and informing public health decision-making.
Material and Methods
Search Strategy
This systematic review was registered in PROSPERO (Registration number: CRD42023459439). The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines were followed with no language limitations. The search strategy was done using the Patient, Intervention, Comparison, and Outcome (PICO) framework. All of the articles published in the PUBMED - SCOPUS - EMBASE - Cochrane Library - Web of Science and Virtual Health Library (VHL) databases from January 1, 2000, to December 31, 2023 were identified. (Supplementary data 1).
Selection Criteria
All studies involving economic evaluations of RA or direct costs that met the following inclusion criteria were included: 1. Case-control studies, cross-sectional or analytical prevalence design, cohort studies, controlled clinical trials (“CCT”), preclinical trials, simulation-modeling studies, conference abstracts, conference summaries, nursing clinic costing studies. 2. Studies of the populations of Latin American countries belonging to the Economic Commission for the Americas and the Caribbean (CELAC): Antigua and Barbuda, Argentina, Bahamas, Barbados, Belize, Bolivia, Brazil, Colombia, Costa Rica, Cuba, Chile, Dominica, Dominican Republic, Ecuador, Salvador, Grenada, Guatemala, Guyana, Haiti, Honduras, Jamaica, Mexico, Nicaragua, Panama, Paraguay, Peru, St. Kitts and Nevis, St. Vincent and the Grenadines, St. Lucia, Suriname, Trinidad and Tobago, Uruguay, and Venezuela. Brazil is included because it is a Latin American power.
Exclusion Criteria: 1. Letters to the editor, systematic or narrative reviews, case reports, or case series. 2. Studies that included patients with Juvenile Arthritis.
Article Selection
Using the Rayyan application, all searches were imported from the databases.12 Duplicates were subsequently removed; the studies were reviewed by title and abstract and were included or excluded based on the inclusion criteria. The articles were divided into 2 sections. They were distributed between 2 pairs of authors who reviewed the two sections initially by title and abstract. After that they exchanged sections to review the full text of those eligible in search of further data. Inconsistencies were resolved for each pair of reviewers by a third reviewer who led a joint review and helped reach a consensus.
Quality Assessment
The quality of the studies was evaluated using the “The Joanna Briggs Institute (JBI) Critical Appraisal tools for use in Systematic Reviews Checklist tool.13 Four reviewers working in pairs used the JBI checklist that consists of 11 questions to investigate the methodological quality of economic studies. Each question was assigned a “yes”, “no” or “unclear” weighting. Each pair of reviewers evaluated the articles and conference abstracts. Disagreements were resolved through a joint review with a third reviewer. The score limits for the methodological quality of the studies and conference abstracts were defined as a total score > 6 with all studies being considered. Agreement levels were evaluated by calculating the mean difference and standard deviation. What was evident in both cases was that the ratings of the different reviewers tended to be clustered near the mean. (Supplementary data 2 and 3).
Analysis
To condense the information, doing a synthesis without meta-analysis was proposed as a qualitative analysis of the data and not a quantitative analysis given the heterogeneity of all the articles by following the SWIM “Synthesis without meta-analysis” guide.14 General and specific tables were established for reporting the information, and the data was recorded in Word and Excel. The results of the costs of the selected articles and abstracts were converted into US dollars as of 2023 using the exchange rates representative of the year of each study and the year-to-year values of inflation up to 2023. This was done by creating tables using Excel formulas for each country. (Supplementary data 4).
Ethics Approval and Informed Consent
This study was conducted in accordance with the principles of the Declaration of Helsinki and approved by the Research Ethics Committee on Human Beings, Fundación Universitaria de Ciencias de la Salud – FUCS, Bogota, Colombia (Record 0317–2021, June 1st, 2021). In Colombia, this study does not require any informed consent, because there is no patient contact, and it is considered without risk. Therefore, it does not require informed consent. Nevertheless, an authorization for the use and analysis of the data was taken from each patient.
Results
The search strategy identified 851 articles. After these initially selected studies were reviewed, duplicates were eliminated, and they were checked for compliance with inclusion criteria, 117 articles were considered eligible for the study. Of these, 42 were eliminated because they corresponded to the wrong population or outcome thus leaving a total of 27 articles15–41 and 4842–88 conference abstracts included which we decided to evaluate in order to do the proposed qualitative analysis. (Figure 1).
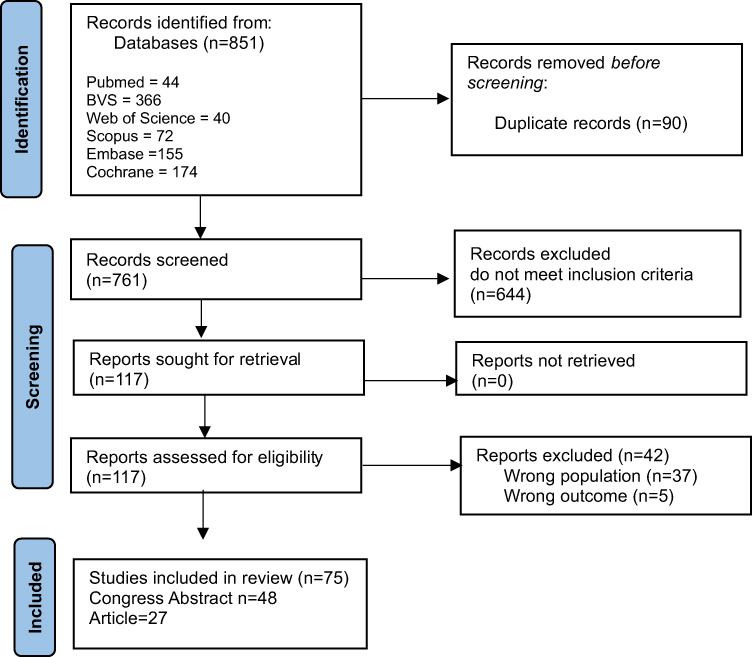 |
Figure 1 Identification of studies via databases and registries. |
General Characteristics of the Articles
Of the 27 articles reviewed, there is a yearly publication frequency starting in 2003. The years which the most publications were reported in 2008, 2011, 2021, and 2023. The distribution of articles published by country gives the highest number of articles to Brazil with nine, followed by Colombia and Mexico with seven each. Three articles were found to have been published by countries collaborating with each other. The first was published jointly by Brazil, Mexico, Colombia, and Argentina. The second was published by Mexico and Puerto Rico and the third was a study by the BRICS countries (Brazil, Russia, China, India and South Africa) while Argentina reported a single article of its own. Regarding the population characteristics, the age range in which the studies were carried out was adults between 45 and 60 years of age. With respect to gender, the majority of the articles published related to women. Regarding the time horizon, which refers to the number of years over which resource consumption was quantified, these studies found a range between 1 and 27 years. Regarding study design, cross-sectional, longitudinal, prospective and retrospective studies were found. The perspective from which the economic evaluations were made was from that of the third-party payer 26%, from the insurer 14.8%, from the social perspective 7.4%, and from mixed providers 3.7%. The rest did not report. Inclusion criteria included: adults of both sexes who were in the official databases of each of the countries or provider entities. Moreover, only one article was found that reported the use of 13 clinical trials. The predominant economic evaluation is cost analysis 86%, followed by cost-effectiveness studies (CE) 7.4%, and cost-utility (CU) with 3.3%; 3.3% did not report. (Table 1).
 |
Table 1 General Characteristics of Included Articles |
Description of Findings by Country with the Most Published Articles (Table 2)
Brazil
These articles are written by a variety of authors. There is no single author who stands out in the frequency of their writing. Of the articles selected, 44.4% report the perspective from which the analysis was done the third-party payer’s perspective accounted for 22.2% while another 22.2% focused on the insurer’s perspective. In relation to the sources of information, 66.6% obtained it through the application of surveys and SF-36 questionnaires on Health Status (Short-Form) and HAQ (Health Assessment Questionnaire). The other 33.4% use the national database of the hospital and outpatient health information system. Regarding the type of analysis, 100% were found to use linear and logistic regression measurements with probabilistic matching. As for evaluation methodologies, 22.2% used decision tree, and Markov models while only 11.1% applied micro-costing methodologies. In terms of intervention technology, 44.5% reported using Biologic DMARDS (bDMARDs) among which the most frequent were anti-tumor necrosis factor (Anti-TNF) agents: Adalimumab (ADA), Infliximab (INF), Etanercept (ETA). Cost analysis, in turn, was the predominant method in 88.8% of the articles. A sensitivity analysis was done under certain specific conditions in 33.3% of the studies to assess the values of independent variables attributable to a dependent variable. Of these, 22.2% identified changes in the percentage effectiveness of Methotrexate (MTX) and changes in cost-effectiveness when Golimumab (GOL) was applied. Another 11.1%, given the country’s economic situation, estimated the indirect cost based on individual and population data. The remaining 66.7% did not report any sensitivity analysis.
 |
Table 2 Specific Characteristics in Economic Evaluations of the Brazilian and Colombian Articles |
The results, in turn, were calculated with the exchange rates presented by the articles and brought forward to the year 2023 while factoring in the country’s annual inflation. The average annual cost of RA medication for 2002 was US$161.36 dollars/patient, the average direct cost per patient was US$370.36 dollars/year, and the average direct non-medical cost was US$32.68 dollars.19 As of November 2023, the annual cost of RA medication was US$921.85 dollars/patient, the average direct cost per patient was US$2115.34 dollars/year, and the average direct non-medical cost was US$190.92 dollars. A study in 2008 reported, with a time horizon of 1 year, the cost based on a model of treatment cycles in line with the medication used and the transition time between each cycle as follows: US$382 (cycle 1), US$1561 (cycle 2), US$1826 (cycle 3), US$2149.8 (cycle 4), US$30,182 (cycle 5).21 These values would have been US$2639.03 (cycle 1), US$10,784.09 (cycle 2), US$12,614.82 (cycle 3), US$14,851.7 (cycle 4), US$20,8510.76 (cycle 5) as of 2023. Another study mentioned that the direct medical cost in 2013 was $981,886 which is equivalent to an average of $9532 dollars per patient/year with a time horizon of 2 years.28 This value in direct medical costs would be US$4,518,198.25 as of 2023, which is equivalent to an average of US$43,862.05 dollars per patient/year. The total expenditure for inpatient and outpatient medical treatment of RA with a time horizon of 5 years was reported to be $7,979,738 in 2016.20 As of 2023, this cost could have amounted to US$17,724,939.4. Last of all, the cost of GOL in 2021 was US$30,480.69 of ETA US$33,458.42, and of ADA US$35,615 over a 5-year follow-up period. This was based on maintaining similar profitability but differences in cost. This impacted the economic model due to the prices agreed upon with the manufacturers and affected the incremental profit for them.35 The cost of GOL in 2023 would have been US$30,662.18, ETA US$33,657, and ADA US$35,827.9 for 5 years of follow-up while maintaining a similar profit. A 2023 article mentioned that ADA 40 mg and ETA 50 mg had the greatest impact on financial expenditure since they accounted for 68.3% of the expenditures on biological drugs. The average annual expenditure was US$93 million. RA, with seropositive rheumatoid factor accounted for 45.5% of the expenditures, followed by RA with seronegative rheumatoid factor at 22.5%.40
Therefore, in Brazil, the direct medical cost of RA treatment would probably range from US$2115.34 dollars per patient/year to US$43,862 dollars per patient/year, depending on the phase of treatment the patient is in and bearing in mind the fact that Brazil is considered the country with the second most depreciated currency in Latin America for 2023.
Colombia
Between (Santos-Moreno) and (Quintana G) there is a tie for first place in publications, corresponding to 66.6%. A total of 85.7% of the articles written in Colombia report the perspective from which the analysis was carried out. Thus, this country is the one that most frequently reports this data. Ninety-six percent do so from a third-party payer perspective and 4% from a social perspective. Seventy-one percent used medical records as a source of information and the rest used historical cost databases. As for the method of analysis, 71% used scenario simulations by means of Markov models. Another 14.5%, in turn, used the macro-costing methodology. The other 14.5% followed the recommendations of the Economic Evaluation Guide issued by the Colombian Institute for Health Technology Assessment (IETS in Spanish). Fifty percent of the articles mention procedures related to disease stage, bDMARDs, and csDMARDs. The evaluation that prevails in 100% of the studies is cost evaluations. Colombia as a country reports a sensitivity analysis less than any other at only 14.2% and does so when bDMARDs such as ADA, ETA or INF are used.
Thus, the results were calculated with the exchange rates presented by the articles and carried forward to the 2023 exchange rate while factoring in the country’s annual inflation and highlighting the following: A study in 2004 reported the total costs of medical treatment of early RA in the different therapeutic approaches; Approach 1. US$728, Approach 2. US$779.3, Approach 3. US$860.9, Approach 4. US$1383.2; laboratory test costs among the 5 institutions range from US76 to US204.16 The total costs of medical treatment of early RA for the different therapeutic approaches in the year 2023 would be as follows: Approach 1. US$1256.34, Approach 2. US$1344.87, Approach 3. US$1485.69, Approach 4. US$2387.05; laboratory test costs among the 5 institutions range from US$131.16 to US$352. The average cost of caring for a patient in the first year with mildly active disease in 2008 was US$1689, with moderate activity US$1805, and with 36 severe activity US$23,441 when using anti-TNF. 25 The average cost of caring for a patient in the first year with a mildly active disease in 2023 would have been US$1529, with moderate activity US$1634.05, and with severe activity US$21,220 when using anti-TNF.23 Costs in 2017 were found to average US$8996.9 ± US$2172 per RA patient per year.36 As of 2023, the annual average is likely to be US$8466.55 ± US$2044.17. Finally, a last study in 2021 reported that the total cost of conventional diagnosis in a patient with seronegative RA was estimated to be US$59.20 and that the cost of a proposed new alternative diagnostic model including more imaging was US$269.57. However, although the proposed diagnostic alternative is a priori five times more expensive, there is a savings in one-year treatment costs of US$1570.75520 due to ruling out RA in 74% of the cases using the new alternative. The cost, in turn, of treating a patient over one year of follow-up was US$5419.3 (range US$5125.8 - US$5787.7). However, the highest cost was related to pharmacological treatment (US$5332.6). Therefore, increasing the number of patients in remission and with low disease activity would result in a cost saving of US$223,874/year and US$231.3 per patient.38 The total diagnostic cost as of 2023 would have been US$ 67.15. Follow-up for a seronegative patient could cost an average of US$ 6146.36. The pharmacological treatment was about US$ 6047.69. The savings in cost from the increase in the number of patients in remission and with low activity were about US$253.88 dollars/year and US$262.35 dollars/patient. In this regard, it is clear that the trend of inflation in 2021 had an impact on raising prices and, for previous years, there is evidence of a drop in prices due to low inflation.
Other Countries (Table 3)
Mexico
The authors of these articles are varied. There is no one author who predominates in the frequency of the writing of these articles. Only 42.8% of the selected articles report an analysis perspective. Of these, 28.5% correspond to the insurer’s perspective and 14.36% to the provider’s perspective. As for the sources of information, like Brazil, 71.4% are obtained from the application of surveys and HAQ questionnaires. The most commonly used data analysis models (57.1%) were decision trees and simulations of treatment therapies, 28.6% were clinical trials and cross-referencing of prescriptions with the way patients take their medications, and the remaining 14.3% corresponded to a macro-costing study based on DRGs (Diagnosis-Related Groups). Regarding treatment technologies, only 28.5% report using the same bDMARDs as Brazil (ADA, INF, ETA) and 14.3% (Clinical Trial) carried out a three-stage procedure. Cost analysis was the predominant method for 71.4% followed by CE studies (28.6%). Only 43% did a sensitivity analysis. Of these, 28.5% report sensitivity in the scenarios proposed and the other 14.3% report Abatacept (ABA) as the most cost-effective alternative with dominance over the other drugs.
 |
Table 3 Specific Characteristics in Economic Evaluations of Items From Mexico and Other Countries |
With respect to the results, these were calculated with the exchange rates presented by the articles and brought forward to the year 2023 while factoring in the country’s annual inflation. The total direct costs in 2005 were $152,704.11 dollars, $1735.27 per patient/year. The costs of medical care were US$78,386.43, US$890.75 per patient/year.27 The total direct costs would have been US$204,001.7, US$2317.84 per patient/year, and the medical care costs would have been US$104,718.13, US$1188.98 per patient/year, as of 2023. The average treatment costs for patients treated with Tocilizumab (TCZ) in 2010 with a time horizon of 5 years were US$198,705, ADA US$188,534.45, INF US$175,838.79, ETA US$172,033.87, ABA US$169,263.20 and with Rituximab (RTX) US$97,373. Of these, ABA is the most cost-effective and would result in greater well-being for the population since each year of life gained, adjusted for quality of life, would cost US$86,375.43.25 As of 2023 with a time horizon of 5 years, the treatment costs for patients treated with TCZ will probably be US$247,045.25; for those treated with ADA US$234,399.89; with INF, US$218,615.25; with ETA, US$213,885.67; with ABA, US$210,440.71; and with RTX US$121,061.56. The quality-of-life-adjusted life year has a cost of US$107,388.01. And one last article from 2013 reported that treatment with ETA was more cost-effective because it presented the lowest cost per case with a successful response at a cost of $187,740 per patient which was the lowest associated cost for the treatment of RA: US$21,170.10 less than ADA, US$4484.70 less than INF and US$9064.05 less than TCZ.29 In 2023 figures, the cost trend per patient with ETA would have been US$219,606.93 and US$24,763.39 less than the ADA, US$5240.43 less than the INF and US$10,602.52 less than the TCZ. Last of all, an article from 2023 mentions that laboratory and diagnostic tests accounted for 69.3% of the total costs over the two years of the study, followed by surgical procedures on the musculoskeletal system with 19.1% and 18.7% of the total costs, and physical therapy between 2.6% and the 3.2%.39 This article did not include studies of drug costs.
Argentina
Only one article was identified for this country. The authors compiled 13 clinical trials where a cost evaluation was done with no economic perspective or sensitivity analysis reported. They conclude that the average annual cost per RA patient under treatment with bDMARDs in 2016 cost a total of US$30,567.40 while for csDMARDs it was US$104.90.34 As of 2023, treatment with bDMARDs cost US$17,551.31, while for csDMARDs it was US$59.72. This drop in prices can be attributed to the depreciation of this country’s currency, which ranks third in Latin America, as of 2023.
Cooperative Study (Brazil, Mexico, Colombia and Argentina)
Corresponds to a published article carried out in these countries. This is the only study that does the analysis from a social perspective. The method used to analyze the information were individual economic models. In all 4 countries, the same procedure was carried out with: ABA, ADA, Certolizumab Pegol (CZP), ETA, INF, RTX and TCZ. The evaluation carried out is a cost study. The research reviewed expanded use of bDMARDs products between 2012 and 2022 for RA patient resulted in a cumulative net cost savings of $2.351 billion Argentine pesos, $9.004 billion reals in Brazil, $728.577 billion Colombian pesos, $18.02 billion Mexican pesos by the year 2012.31 Carried forward to the year 2023, the cumulative cost savings for each country would be: 5089 billion Argentine pesos, $8286 billion Brazilian reals, $3482 billion Colombian pesos, and $3789 billion Mexican pesos.
Mexico and Puerto Rico
This is a study that was done in the US, but it was based on a population from Mexico and Puerto Rico that lives in the US The source of information was HAQ questionnaires, a visual analog scale, and SF36. The analysis of the information was carried out by means of 1000 repetitions through a Monte Carlo simulation. The type of evaluation done was a cost evaluation. Sensitivity analysis was done with the prevalence of the use of biological therapy. The total direct medical cost of patients with RA in 2001 was US$951915. Given the average US inflation rate for the last 22 years, which is reported to be 2.45%, the direct medical cost calculated for 2023 would be US$23,321.55.
General Characteristics of Conference Abstracts
Of the 48 abstracts reviewed, there is a yearly publication frequency starting in 2003. The years in which the most publications were reported in 2011, 2013, 2015, and 2019. The distribution of articles published by country places Colombia in first place with 35.4%, followed by Brazil with 17%, Mexico with 10.4%, Costa Rica with 6.3%, Argentina, Chile, Ecuador, Guatemala and Venezuela each with 4.1%, and Honduras, Panama, Dominican Republic, El Salvador and collaboration between countries, each with 2.08%. In general, the time horizon of each abstract varies from 6 months to 50 years. From the analysis perspective, the supplier’s perspective predominates at 66.6%. This perspective is broken down into the following categories: 37.5% from the point of view of the general supplier, 34.3% from the private supplier, 22% from the public supplier, and 6.2% from the mixed supplier. The following percentage of the analysis perspective, 33.3%, corresponds to that of the third-party payer. Regarding the method of information analysis, the results are distributed as follows: the most used is the decision tree (29%), followed by the Markov model and treatment simulations (18.7%). The predominant economic evaluation in the abstracts, in turn, is that of CE at 35%, followed by cost analysis at 27%, Profitability study at 25%, CU at 9% and one study with a combination of CE and CU that accounts for 4%. A table and qualitative description of these summaries can be found in. (Supplementary data 5).
Discussion
This is one of the few studies that sought to synthesize and compile the most relevant information for evaluating the health costs of RA in Latin America. A novel strategy was developed to update the actual value of the costs to the current year. To determine the value in current prices of the costs of care and treatment of RA patients in the countries evaluated, the authors developed a financial methodology to update to present value the cost of the studies carried out in previous years. In this method, the exchange rate of the base year multiplied by the base price in dollars of the study was determined for each study, and the resulting value was weighted in accordance with the annual inflation index reported by the World Bank. The inflation result was adjusted to the country’s currency and the exchange rate for the year 2023. Inflation thus estimated is considered indicative of the cost of living and reflects the loss of purchasing power of money, and the subsequent increase in the value of goods in the basic family basket of goods. In a way, it is a reflection of the savings possibilities for society and of the impact on the prices of essential drugs, such as those used for RA. This finding is similar to the one reported in the study done by Cid et al.89 This report referred to the lack of financial protection that affects a large part of the population and also shows how there are groups of countries with greater difficulties than others due to the cost of medicine and exposure to greater situations of vulnerability and thus denotes great inequity. This same study, endorsed by the Pan American Health Organization (PAHO), identifies policies in some countries that could be associated with the evolution of financial protection. In addition, they concluded that public spending should be increased to increase the financing of health systems and transform them into a universal health model to replace out-of-pocket spending as shown in the study done by Petrera and Jiménez.90
From the review carried out, it is evident that the cost analyses are the most used (85%), and in a much higher proportion than other studies such as those of CE and CU. This is probably because these cost analyses are easier to implement based on financial records, equipment use, workforce and quality without involving the stage of measuring procedures and their results, which would cause more complexity in carrying out the CE. In the study by Catalá-López and García-Altés, carried out in Spain, they mention that the most predominant economic evaluation is that of CE at 62.5%.91 This corresponds to the results of our review in which the predominant type of study in the abstracts was found to be CE but in a proportion of only 35%, and in the articles, it occupies the second place at 7.4%.
Moreover, several studies have shown that the direct cost of the disease increases depending on the phases, cycles, or years of treatment, particularly the cost associated with drugs with the cost of biological drugs being clearly higher. Likewise, in the ESPOIR cohort, which has included patients with early RA in France in a multicenter and consecutive manner, the study by Chevreul et al, showed that the direct cost was higher for users of biological therapies, especially for those who used them within the first year, followed by users who received them in consecutive years.92 The authors conclude that their analysis suggests that early use of biologicals may reduce other health care costs by slowing disease progression although the extent to which the high direct costs of early use of biologicals may be offset by reduced need for surgeries or other procedures after the fourth year of disease is unknown. These statements as well as those in the above-mentioned study could be applied to the present review since, due to the type of design, the exact impact on cost reduction associated with this therapy is unknown. However, in some of the studies included, particularly in the Colombian population, it was shown that increasing the number of patients in remission and with low disease activity resulted in cost savings.
It should be noted that the present review did not focus on studies that analyze indirect costs or the burden of disease through DALYs. Other authors have recently reported, based on a systematic review of the literature, that these costs can represent up to 30% of the costs of the disease in the Latin American region.8 In that review, the authors found a wide variability in these costs within the region that was similar to what was found in the present review with respect to direct costs or those with CE design since they varied from one country to another even when the same health technologies were analyzed. Thus, for example, the same group of anti-TNF drugs showed great variability in terms of costs in countries such as Brazil, Mexico, and Colombia.
It was not possible, however, to analyze studies that researched the economic impact of rotating or switching a patient between different anti-TNF drugs or switching to other therapies after using this class of drugs. Other reviews that have addressed this issue have not included Latin American studies and, in fact, have highlighted the need for greater uniformity in the methodology used in economic evaluations of rotation versus switching strategies after the use of anti-TNF for patients with RA. It is not possible to draw conclusions about the costs attributed to dose escalation, particularly in drugs such as anti-TNF drugs.93 Although there are previous reviews that have analyzed this issue, such as the one done by Moots RJ et al, in which only one article from the Latin American region was included, the authors concluded that, although there are different definitions and several methods were used to calculate dose escalation with biologicals, the results were consistent with the individual comparative studies.94 In addition, not only are the costs of biological drugs increasing, but so are the total costs of RA.
A systematic review of the literature on the burden of disease in the biological era that was completed by February 2019, in turn, included a total of 72 articles from 28 countries of which only 3 were from Latin America, the same 3 included in the present review.95 The other articles were dominated by the European continent. In that review, it was striking that the direct cost attributed to drugs has been increasing over the years from 2000 to 2016. The authors note that, due to different definitions in the limited number of studies, it was a challenge to compare the breakdown of costs. Just as in the present review, the heterogeneity and variability of these costs was large with drug costs contributing between 9.8% and 87.2% to direct costs.
With respect to the differentiation of costs by type of drug based on technology, it should be noted that the results of the present study did not include findings regarding biosimilars. However, the impact that these have on RA costs must be considered, a fact that is even more significant in Latin America given the economic restrictions of the health systems. Now, the introduction of biological therapy is known to have marked a substantial change in the course of RA. However, the costs of this therapy can cause difficulties in terms of access because the purchase prices are often high.96 In view of the above, consideration should be given to the fact that large-scale production of these drugs could improve their introduction into the market and this fact will positively affect the accessibility of this medication in the future. It is well known that biosimilars have shown an efficacy and safety similar to the reference pharmaceutical products which translates into lower disease costs. From this perspective, greater access to biological therapies that can help to control more severe stages of the disease could be generated.97,98
In this regard, the study by Haustein R et al, estimated that between 2.3 and 11.7 billion euros could have been saved in Germany, France, and the United Kingdom between 2007 and 2020 with the introduction of biosimilars and concluded that these savings could have improved the quality of care and, above all, increased access to the various biological therapies.99 Most of the cost analyses related to treatment with biosimilars have been with INF since it is the first product to have received approval for use in daily practice. Its profile has proven to be a CE therapy in disease control compared to the reference therapy although cost analyses have also been done with ETA biosimilar molecules and have shown some benefits.100,101 This seems to demonstrate that the use of biosimilars in populations with diverse sociodemographic characteristics and different economic levels may have a certain advantage, and although many more studies are needed in Latin America to prove it, the introduction of biosimilars could change the tendency to use conventional therapy since greater access to biological therapy at a lower price would be sought. However, studies evaluating the cost-effectiveness of conventional vs biosimilar therapy are lacking.
In the last decade, the Pan American League of Rheumatology Associations (PANLAR) put forward a consensus statement on biosimilars that highlighted several points including proper pharmacovigilance and possible lower prices.102 More recently, the study by González et al, analyzed the prices of biological drugs in the United States, Spain, and three Latin American countries.103 The article highlights that the economic effort made by Latin American countries to get access to these drugs is much greater than that of the US and Spain.
The results show a difference between countries in the costs of care and treatment. This may be due to the acceleration of technological innovation and the increase in new drug molecules. This development is due to not only scientific but also economic reasons.104 A report by the Chilean economic observatory states that the level of prices between countries is related to the higher level of productivity and income. The higher the productivity, the higher the prices tend to be. Tariffs, transportation costs in the international market, taxes and subsidies, labor costs, and the degree of competition in the market between generic and commercial drugs also play a role.105 In the study done by Xu et al between 2000 and 2016, there was a decrease of 56% to 44% in out-of-pocket spending by families in almost all regions of the world, mostly explained by the increase in public spending on health, the increase in co-payments, care fees, and drug costs that can reach 85% of out-of-pocket spending. This has resulted in a decrease in medical care, an increase in the number of patients who give up on treatment.106
Among some mitigation strategies include managing risk to identify the vulnerability of the population and applying treatments that reduce the progression of the disease and its complications. In the case of RA, the causal factors that can be effectively managed are early detection and suspicion of the disease while the factors that modify prognosis are manageable and contribute greatly to improving patient health outcomes.107
The preparation of updated recommendations, supported by scientific evidence, will provide guidance to rheumatology specialists and other professionals involved in the care of patients with RA. These recommendations will facilitate informed therapeutic decision making in order to mitigate the risks associated with treatment and improve patients’ quality of life.108
However, the constant rise in health costs leads to the need to economically evaluate treatments in order to prioritize those that have and offer the best value or benefit related to the local context. The use of economic evaluations supports decision making in health care and represents a valuable mechanism for improving the efficiency of budget distribution among the different levels of health care, thus promoting the efficient use of resources.109
Limitations
Regarding the study limitations, the inclusion of conference abstracts, while broadening the scope of available evidence, may introduce potential limitations and bias related to the preliminary nature and quality of the data, which are discussed in the Supplementary Materials and acknowledged in this section. Also, a limitation of this study is the exclusion of studies from 2024, which may have resulted in missing recent publications, who can contribute further results. Additionally, the number of publications on economic evaluations of RA in Latin America is limited, and as such, we found more conference abstracts than full-text articles. This constraint is acknowledged and discussed in the Supplementary Materials, and it may affect the comprehensiveness of the findings. Additionally, Due to the heterogeneity of the included studies, we were unable to perform a meta-analysis of the costs or conduct a quantitative analysis. However, to maximize the use of the available data, we followed the SwiM guidelines for qualitative analysis, ensuring a thorough synthesis of the information extracted from the studies.
It had also not possible to determine how the cost of the disease affects the purchasing power and, therefore, the economic balance of both the population and the health system of each country, because there is no standardization of prices, as there is no single currency as in the European Union. On the other hand, the size of each economy, as indicated by the Gross Domestic Product (GDP) in Latin American countries, is very different compared with European countries, and inflation behaves differently, as do the indicators of wealth distribution, as reflected in World Bank reports.
Conclusion
The analysis of costs for Latin American patients with RA emphasizes the need for careful management of expenditures by insurers and care providers and highlights the relevance of sound health policies and risk management in the world’s health systems. This study shows through cost analyses that the use of biological therapies makes up the majority of direct costs. In addition, there are important differences in the costs of biologics between different countries, as well as differences depending on the stage of disease progression. Therefore, it would be important that each country should implement strategies to make cost analyses from the payer perspective. Regional technology assessment agencies could play an important role in this regard. On the other hand, more research is needed in Latin American RA population with an emphasis on measuring health outcomes to strengthen cost analyses with the use of biosimilars versus traditional therapies.
Acknowledgments
We would like to thank Fernando Rodriguez-Florido for design and reviewing this manuscript for stablish the graphics of the data, and Nicolas Gutierrez, and Laura Villarreal for the contribution of data collection.
Disclosure
Adriana Rojas-Villarraga: reports Adriana Rojas-Villarraga reports fees for conferences from AbbVie, Amgen, Aztra Zeneca, Janssen, andPfizer in the last three years, and fees for conferences and grant for a research protocol fromAsoreuma (Colombian National Rheumatology Scientific Society) outside the submitted work and with no influence on it. Pedro Santos-Moreno reports fees for conferences from Abbvie, Abbott, Biopas-UCB, Bristol, Janssen, Pfizer, Roche, Sanofi, AbbVie, Abbott, Biopas-UCB, Bristol, Janssen, Pfizer, Roche, Sanofi. The authors report no other conflicts of interest in this work.
References
1. OCDE - Mejores politicas para una vida mejor. OCDE. Indicadores clave - gasto en salud. 2020. Available from: https://www.oecd.org/centrodemexico/estadisticas/gastoensalud.htm.
2. de Alto Costo C. Fondo Solidadario de Enfermedades de Alto Costo. Cuenta de Alto Costo - Lineas de acción. Available from: https://cuentadealtocosto.org/quienes-somos/lineas-de-accion/.
3. Pabón-Porras MA, Molina-Ríos S, Flórez-Suárez JB, Coral-Alvarado PX, Méndez-Patarroyo P, Quintana-López G. Rheumatoid arthritis and systemic lupus erythematosus: pathophysiological mechanisms related to innate immune system. SAGE Open Med. 2019;7. doi: 10.1177/2050312119876146.
4. Londoño J, Peláez Ballestas I, Cuervo F, et al. Prevalence of rheumatic disease in Colombia according to the Colombian Rheumatology Association (COPCORD) strategy. Prevalence study of rheumatic disease in Colombian population older than 18 years. Revista Colombiana de Reumatologia. 2018;25(4):245–256. doi:10.1016/j.rcreu.2018.08.003
5. Maldonado-Restrepo AI, González-Rodríguez JL. Artritis reumatoide: carga económica y calidad de vida relacionada con la salud en Colombia y en El Mundo: revisión de alcance. Revista Repertorio de Medicina y Cirugía. 2023;32(3):197–207. doi:10.31260/repertmedcir.01217372.1486
6. IETS. Ministerio de la Protección Social. Posicionamiento Terapéutico Para El Tratamiento Farmacológico de La Artritis Reumatoide. 2022.
7. Papadimitropoulos E, Brnabic A, Vorstenbosch E, Leonardi F, Moyano S, Gomez D. The burden of illness of rheumatoid arthritis in Latin America—A systematic literature review. Int J Rheum Dis. 2022;25(4):405–421. doi:10.1111/1756-185X.14295
8. Blanco Aspiazu MA, Shunchao K, Xueqing L. Comorbidity and its value for the general doctor in Internal Medicine. Revista Habanera de Ciencias Médicas. 2017;16(1):12–24.
9. de Alto Costo C. Criterios Para Identificar Patologias de Alto Costo En Colombia. 2014.
10. Soriano ER, Mysler E, Rios C, Xavier RM, Cardiel MH, Citera G. Rheumatoid arthritis in Latin America: pharmacotherapy and clinical challenges. Expert Opin Pharmacother. 2024;25(15):2023–2033. doi:10.1080/14656566.2024.2412247
11. Loyola-Sanchez A, Richardson J, Wilkins S, et al. Barriers to accessing the culturally sensitive healthcare that could decrease the disabling effects of arthritis in a rural Mayan community: a qualitative inquiry. Clin Rheumatol. 2016;35(5):1287–1298. doi:10.1007/S10067-015-3061-4
12. Mourad O, Hossam H, Zbys F, Ahmed E. Rayyan-a web and mobile app for systematic reviews. Syst Rev. 2016;5(1). doi:10.1186/s13643-016-0384-4
13. The Joanna Briggs Institute. Checklist for Systematic Reviews and Research Syntheses Critical. 2017. Available from http://joannabriggs.org/research/critical-appraisal-tools.htmlwww.joannabriggs.org.
14. Campbell M, McKenzie JE, Sowden A, et al. Synthesis without meta-analysis (SWiM) in systematic reviews: reporting guideline. BMJ. 2020:368. doi:10.1136/bmj.l6890.
15. Michaud K, Messer J, Choi HK, Wolfe F. Direct medical costs and their predictors in patients with rheumatoid arthritis: a three-year study of 7527 patients. Arthritis Rheum. 2003;48(10):2750–2762. doi:10.1002/art.11439
16. Ricardo P-T, Giovanna A, Patricia R, J.m A. Impacto de la enfermedad cardiovascular en los costos de hospitalización de pacientes con artritis reumatoidea. Biomédica. 2004;24:366–374. doi:10.7705/biomedica.v24i4.1286
17. Pineda-Tamayo R, Arcila G, Restrepo P, Tobón GJ, Camargo JF, Anaya JM. Costos médicos directos dela artritis reumatoide temprana. Revista Colombiana de Reumatología. 2005;(2):89–96
18. Blanca H-C, Rafael -A-A, Mario C-R. Costs of the standard rheumatology care in active rheumatoid arthritis patients seen in a tertiary care center in Mexico City. Clinica Reumatologica. 2006;2(3):124–130. doi:10.1016/S1699-258X(06)73033-9
19. Chermont GC, Kowalski SC, Ciconelli RM, Ferraz MB, Ferraz MB. Resource utilization and the cost of rheumatoid arthritis in Brazil. Clin Exp Rheumatol. 2008;26:24–31.
20. De Azevedo ABC, Ferraz MB, Ciconelli RM. Indirect costs of rheumatoid arthritis in Brazil. Value Health. 2008;11(5):869–877. doi:10.1111/j.1524-4733.2008.00332.x
21. Monteiro RDC, Zanini AC. Análise de custo do tratamento medicamentoso da artrite reumatóide. Revista Brasileira de Ciências Farmacêuticas Brazilian J Pharmaceut Sci. 2008;44(1):25–33. doi:10.1590/S1516-93322008000100004
22. Mould-Quevedo J, Peláez-Ballestas I, Vázquez-Mellado J, et al. El costo de las principales enfermedades reumáticas inflamatorias desde la perspectiva del paciente en México. Hospital General Regional. 2008;144(3):225–231.
23. Mora C, Diaz J, Quintana G, Díaz JD. Costos directos de la artritis reumatoide temprana en el primer año de atención: simulación de tres situaciones clínicas en un hospital universitario de tercer nivel de Colombia. Biomedica. 2009;29:43–50. doi:10.7705/biomedica.v29i1.40
24. Aceves-Avila FJ, Benites-Godínez V, Ramos-Remus C. Cost of medication errors in rheumatic patients in Mexico. Clin Rheumatol. 2011;30(11):1421–1424. doi:10.1007/s10067-011-1837-8
25. Rojas F, Chacaltana CB, Zingoni C, Bergman G, Drost P. Cost-effectiveness of Abatacept compared to other biological agents for the treatment of moderately to severely active rheumatoid arthritis in patients who failed with methotrexate in Peruvian Social Security during 2010. Acta Med Per. 2011;28(4):200–210.
26. Quintana G, Restrepo JP, Caceres H, Rueda JD, Rosselli D. Evaluación económica del tratamiento de artritis reumatoide con terapia biológica anti TNF en Colombia. Acta Medica Colombiana. 2011;36(1):24–28.
27. Álvarez-Hernández E, Peláez-Ballestas I, Boonen A, et al. Catastrophic health expenses and impoverishment of households of patients with rheumatoid arthritis. Reumatol Clin. 2012;8(4):168–173. doi:10.1016/j.reuma.2012.05.002
28. Bagatini BF, Blatt CR, Estima Marasciulo AC, Nair L, Rocha F. Estudo de custo-análise do tratamento da artrite reumatoide grave em um município do Sul do Brasil. Cad Saude Publica. 2013;29(Suppl1). doi:10.1590/0102-311X00013513
29. Salinas - Escudero G, Vargas - Valencia J, Garcia - Garcia E, Muciño- Ortega E, Galindo- Suarez R. Cost - effectiveness analysis of etanercept compared with other biologic therapies in the treatment of rheumatoid arthritis. Revista Medica Instituto Mexicano de Seguro Social. 2013;51(5):514–521. doi:10.3111/13696998.2011.649327
30. Costa J de O, Almeida AM, Junior AAG, Cherchiglia ML, Andrade EIG, Acurcio F de A. Tratamento da artrite reumatoide no Sistema Único de Saúde, Brasil: gastos com infliximabe em comparação com medicamentos modificadores do curso da doença sintéticos, 2003 a 2006. Cad Saude Publica. 2014;30(2):283–295. doi:10.1590/0102-311X00017913
31. Tundia N, Kotze PG, Rojas serrano J, et al. Economic impact of expanded use of biologic therapy for the treatment of rheumatoid arthritis and Crohn’s disease in Argentina, Brazil, Colombia, and Mexico. J Med Econ. 2016;19(12):1187–1199. doi:10.1080/13696998.2016.1209508
32. Gomes R, Antero P, Cuce NM, da Sá Marchi M, Kozechen RJ. Impact of rheumatoid arthritis in the public health system in Santa Catarina, Brazil: a descriptive and temporal trend analysis from 1996 to 2009. Rev Bras Reumatol. 2017;57(3):204–209. doi:10.1016/j.rbre.2016.07.003
33. da SGD, Andrade EIG, Cherchiglia ML, Almeida AM, Guerra AA, Acurcio FDA. Profile of spending on the treatment of rheumatoid arthritis for patients of the unified health system in the state of Minas Gerais - 2008-2013. Ciencia e Saude Coletiva. 2018;23(4):1241–1253. doi:10.1590/1413-81232018234.16352016
34. Liberman F, Elgart J, Strusberg I. Beneficio económico de los ensayos clínicos controlados patrocinados: el gasto evitable en medicamentos para el tratamiento de la artritis reumatoidea. Value Health Reg Issues. 2019;20:7–11. doi:10.1016/j.vhri.2018.10.007
35. Barreto RDSJ, Ribeiro da Silva MR, Maciel AA, De Assis AF, Alvares-Teodoro J. Cost-utility analysis of the anti-TNF therapy for rheumatoid arthritis in a real-world based model. Expert Rev Pharmacoecon Outcomes Res. 2021;21(5):1011–1016. doi:10.1080/14737167.2021.1840980
36. Machado-Alba JE, Machado-Duque ME, Gaviria-Mendoza A, Reyes JM, Gamboa NC. Use of healthcare resources in a cohort of rheumatoid arthritis patients treated with biological disease-modifying antirheumatic drugs or tofacitinib. Clinic Reumathol. 2021;40:1273–1281. doi:10.1007/s10067-020-05432-6/Published
37. Santos-Moreno P, Alvis-Zakzuk NJ, Castillo E, et al. Quantifying potential cost-savings through an alternative imaging-based diagnostic process in presumptive seronegative rheumatoid arthritis. Clinicoecon Outcomes Res. 2021;13:519–529. doi:10.2147/CEOR.S302404
38. Santos-Moreno P, Alvis-Zakzuk NJ, Villarreal-Peralta L, Carrasquilla-Sotomayor M, De la hoz-restrepo F, Alvis-Guzmán N. Centers of excellence implementation for treating rheumatoid arthritis in Colombia: a cost-analysis. Clinicoecon Outcomes Res. 2021;13:583–591. doi:10.2147/CEOR.S308024
39. Mendoza-Gutierrez CF, Montiel-Ojeda D, Vargas-Chanes D, et al. Health and economic impact associated with rheumatoid arthritis discharges: a cost analysis of a two-year cohort in Mexico. BMC Health Serv Res. 2023;23(1):1–8. doi:10.1186/s12913-023-10298-w
40. Mega TP, Mendes Da Silva R. Expenditure of biological drugs for rheumatoid arthritis treatment in the Brazilian public health system. Rev Saude Publica. 2023;57:41. doi:10.11606/s1518-8787.2023057004280
41. Zhang F, Cui Y, Gao X. Time trends in the burden of autoimmune diseases across the BRICS: an age-period-cohort analysis for the GBD 2019. RMD Open. 2023;9(4):e003650. doi:10.1136/rmdopen-2023-003650
42. Audisio MJ, Strusberg I, De Sergio OB, et al. Semester direct cost by rheumatoid arthritis in patients in a university hospital. Revista Facultad de Ciencias Medicas Universidad Nacional de Cordoba. 2003;60(2):35–41. doi:10.31053/1853.0605.v60.n2.36661
43. Aguirre A, García E, Bierschwale H, Arce C. Cost- effectiveness of the use of Etanercept vs Anti -TNF Monoclonal antibodies in patients with Rheumatoid Arthritis in Mexico. Value Health. 2009;12(7):522–523. doi:10.1016/s1098-3015(10)75481-4
44. Gao X, Hwang S, Carpiuc K, et al. Cost- effectiveness of the use ofEtanercept vs. Rituximab in patients with rheumatoid arthritis in Mexico. Value Health. 2009;12(3):67. doi:10.1016/s1098-3015(10)73398-2
45. Carlos F, Aguirre A, Peláez-Ballestas I. Cost- effectiveness of Tocilizumab for the management of patients with active rheumatoid arthritis despite previous DMARDs therapy in Mexico. Value Health. 2010;13(7):A308. doi:10.1016/s1098-3015(11)72186-6
46. Carlos F. Cost- effectiveness of Rituximab vs alternative anti-tumor necrosis factor (TNF) therapy after previous failure of one anti-TNF agent for treatment of rheumatoid arthritis in Costa Rica. Value Health. 2010;13(7):A309. doi:10.1016/s1098-3015(11)72191-x
47. Carlos F. Cost-Effectiveness of Tocilizumab for the management of patients with active rheumatoid arthritis despite previous DMARDs therapy in Costa Rica. Value Health. 2010;13(7):A309. doi:10.1016/s1098-3015(11)72189-1
48. Alfonso -cristancho R, Aiello EC, Roa CN, Valencia JE. What is the value of the new kid on the block?: Tocilizumab versus abatacept for rheumatoid arthritis in colombia. In: Value in Health. 14. Elsevier BV;2011:A563. doi:10.1016/j.jval.2011.08.1680
49. Cristancho A, Serra N, Aiello EC, Roa CN. Abatacept or Infliximab for Rheumatoid Arthritis in Venezuela? Cost - Effectiveness Analysis. University of Washington; 2011:A1–A214.
50. Alfonso-Cristancho R. Cost- effectiveness of Abatacept or Infliximab in rheumatoid arthritis in Colombia. Value Health. 2011;14(3):A127.
51. Fernandes RA, Boada V, Mould JF. Economic analysis of etanercept in rheumatoid arthritis from a public perspective in Venezuela. Value Health. 2011;14(7):A308. doi:10.1016/j.jval.2011.08.418
52. Fernandes RA, Tovar DAB, Mould JF. Economic analysis of etanercept in rheumatoid arthritis from a public perspective in Colombia. Value Health. 2011;14(7):A308–A309. doi:10.1016/j.jval.2011.08.422
53. Lutz M, Cuesta G, Morales G. Cost- effectiveness analysis of etanercept versus available anti - TNF and IL-6 blockers for treating rheumatoid arthritis in Guatemala. Value Health. 2011;14(7):A562–A563. doi:10.1016/j.jval.2011.08.1679
54. Lutz MA, Bogantes JP, Cuesta G, Saenz R. Cost-Effectiveness Analysis of Etanercept Versus Available Anti-Tnf and Il-6 Blockers for Treating Rheumatoid Arthritis in Costa Rica. Vol. 16. Elsevier BV;2013. doi:10.1016/j.jval.2013.03.1137
55. Lutz MA, Alonzo H, Bogantes JP, Cuesta G. Cost-effectiveness analysis of etanercept versus available anti-tnf and il-6 blockers for treating rheumatoid arthritis in Honduras. Value Health. 2013;16(3):A224. doi:10.1016/j.jval.2013.03.1137
56. Lutz MA, Zelaya R, Bogabantes JP, Cuesta G. Cost-effectiveness analysis of etanercept versus available anti-tnf and Il-6 blockers for treating rheumatoid arthritis In Salvador. Value Health. 2013;16(3):A224. doi:10.1016/j.jval.2013.03.1137
57. Vargas - Valencia J, Sotelo - Guzman M, Mould- Quevedo J, Muciño- Ortega E, Galindo- Suarez RM. Cost- effectiveness analysis of etanercept in the treatment of rheumatoid arthritis in Mexico. Value Health. 2011;14(3):A127. doi:10.1016/j.jval.2011.02.707
58. Ferré F, Moura CS, Kakahasi AM, et al. Profile of use of anti-tumor necrosis factor (antiTNF) agents in rheumatoid arthritis patients in a Brazilian healt-care database, 2008 −2010. Pharmacoepidemiol Drug Saf. 2012;21(Suppl 3):404. doi:10.1002/pds.3324
59. Piha T, Meirelles EDS, w K, Miranda PA. Cost effectiveness analysis of certolizumab pegol in patients with rheumatoid arthritis from a Brazilian private perspective. Value Health Reg Issues. 2012;15(7):A446. doi:10.1016/j.jval.2012.08.1394
60. Takemoto M, Fernandes RA, Fujii RK, Mould J, Tang B. Etanercept in early rheumatoid arthritis: economic evaluation from the public payer perspective in Brazil. Value Health. 2012;15(7):A512–A513. doi:10.1016/j.jval.2012.08.1748
61. Albuja MF, Torres FG, Mould J, Estévez C. Cost-effectiveness analysis of etanercept in the treatment of rheumatoid arthritis in institutional market in Ecuador. Value Health. 2013;16(7):A717. doi:10.1016/j.jval.2013.08.2224
62. Elgart JF, Gonzalez L, Aiello EC. Abatacept for the treatment of patients with rheumatoid arthritis in Argentina: a cost effectiveness analysis. Value Health. 2013;16(3):A223–A224.
63. Elgart JF, Gonzalez L, Aiello EC. Cost-effectiveness of abatacept for the treatment of patients with rheumatoid arthritis after an inadequate response to methotrexate in Chile. Value Health. 2013;16(3):A223. doi:10.1016/j.jval.2013.03.1133
64. Gamboa O, Bárbosa D, Parada L, Latorre M. Cost-effectiveness analysis of tocilizumab in rheumatoid arthritis, in Colombia. Value Health. 2013;16(7):A563. doi:10.1016/j.jval.2013.08.1490
65. Mould-Quevedo J. Economic outcomes for celecoxib in Latin America: a cost-effectiveness study of Cox-2 inhibitors against NSAIDs+Ppi for adult patients with osteoarthritis and rheumatoid arthritis In Brazil, Mexico, Colombia, Argentina And Costa Rica. Value Health. 2013;16(3):A221. doi:10.1016/j.jval.2013.03.1121
66. Garita M, Peralta M, Muñoz-Louis R. Cost-effectiveness analysis of etanercept versus other available. Value Health. 2014;17(3):A47. doi:10.1016/j.jval.2014.03.279
67. Ferreira C, Rufino C, Santana C, Dulcine M. Assessment of tofacitinib for rheumatoid arthritis from the perspective of the Brazilian health-care system. Value Health. 2015;18(7):A646. doi:10.1016/j.jval.2015.09.2317
68. Ferreira CN, Rufino CS, Amaral LM, Fernandes RA. Economic analysis of biologic alternatives in the management of rheumatoid arthritis, psoriasis and ankylosing spondylitis from public and private perspectives in Brazil. Value Health. 2015;18(3):A162. doi:10.1016/j.jval.2015.03.941
69. Garita-Aguilar M, Peralta-Acon M, Chavez-Perez N. Cost effectiveness of tofacitinib as second line treatment vs using biological therapies in the treatment of moderate rheumatoid arthritis after failure of DMARDs in Guatemala in 2014. Value Health. 2015;18(3):A163. doi:10.1016/j.jval.2015.03.943
70. Garita-Aguilar M, Peralta-Acon M, Gorriz-Añorbes L. Cost effectiveness of tofacitinib as second line treatment vs using biological therapies in the treatment of moderate rheumatoid arthritis after failure of DMARDs in Panama in 2014. Value Health. 2015;18(3):A162. doi:10.1016/j.jval.2015.03.939
71. Peirano I, Puig A. Budget impact of golimumab iv for rheumatoid arthritis in the Chilean private sector. Value Health. 2015;18(7):A874–A875. doi:10.1016/j.jval.2015.09.034
72. Almeida R, Alcívar I, Cabezas M, Fornasini M, Albert A. Cost - effectiveness of biologic therapies for rheumatoid arthritis in a large public hospital in Ecuador. Value Health. 2016;19(3):A233. doi:10.1016/j.jval.2016.03.1150
73. Santos-Moreno P, Villarreal L, Ballesteros G, et al. Drug usage analysis and medication expenses in patients with rheumatoid arthritis using biological therapy in Colombia. Value Health. 2016;19(3):A232. doi:10.1016/j.jval.2016.03.1143
74. De Hair MJ, Safy M, IJff N, Jacobs JW, van Laar JM. Drug usage analysis and comparative medication expenses in patients with rheumatoid arthritis using conventional or biological therapy. Ann Rheum Dis. 2016;75(Suppl 2):710–711. doi:10.1136/annrheumdis-2016-eular.3859
75. Diaz Rojas A, Moreno A, Urrego J, Huerfano C, Davila F, Quintana G. Cost - effectiveness of therapies for early Rheumatoid Arthitis in the context of the evidence - based clinical practice guideline for Colombia. Value Health. 2017;20(5):A146.
76. Santos - Moreno P, Villareal L, Aza A, et al. Real-world costs of rheumatoid arthritis in a specialized center in Bogota Colombia Results of a registry during five years. Value Health. 2017;20(5):A154.
77. Santos -moreno P, Villareal L, Aza A, et al. Clinical response at week 52 and costs in patients with rheumatoid arthritis using biological therapy in a specialized center in Colombia. Value Health. 2017;20(5):A144.
78. Santos-Moreno P, Villarreal Peralta L, Alvis-Zakzuk N, et al. Conventional and biological therapy in patients with rheumatoid arthritis. A cost analysis in Colombia. Value Health. 2017;20(9):A938. doi:10.1016/j.jval.2017.08.2975
79. Santos-Moreno P, Buitrago-Garcia D, Villarreal L, Alvis-Zakzuk N, Carrasquilla M, Alvis Guzman N. Costs and trends in the usage of biological therapy for rheumatoid arthritis - a retrospective study. Value Health. 2018;21:S195. doi:10.1016/j.jval.2018.04.1328
80. Garzielle S, Jualina A, Eli Iola A, et al. Cost- utility analysis: adalimumab versus etanercept in rheumatoid arthritis - Brazil. Int J Technol Assess Health Care. 2018;33(S1):171–172. doi:10.2217/cer-2016-0045
81. Alvis-Zakzuk NJ, Santos-Moreno P, Villarreal Peralta L, Alvis-Guzmán N, Carrasquilla M. How expensive is treating patients in a center of excellence for rheumatoid arthritis in Colombia? Value Health. 2019;22:S242. doi:10.1016/j.jval.2019.04.1131
82. Alvis-Zakzuk NJ, Santos-Moreno P, Carrasquilla M, Alvis-Guzmán N. Potential cost-savings due to the application of a center of excellence care model in rheumatoid arthritis in Colombia. Value Health. 2019;22:S241. doi:10.1016/j.jval.2019.04.1129
83. Rosim MP, Mourão JO, Kuribayashi J, et al. Cost - effectiveness of interferon-gamma release assay compared to tuberculin skin test for detection of latent tuberculosis in rheumatoid arthritis patients using inmunobiological treatments. Value Health Reg Issues. 2019;19:S42. doi:10.1016/j.vhri.2019.08.243
84. Santos-Moreno P, Villarreal Peralta L, Cabrera M, Alvis Zakzuk N, Buitrago-Garcia D. Cost- analysis of treatment for moderate and severe rheumatoid arthritis in a specialized rheumatology center. Value Health. 2019;19:S54–S55. doi:10.1016/j.vhri.2019.08.311
85. Valencia O, Castillo E, Villarreal L, Alvis-Zakzuk NJ, Santos-Moreno P. Preliminary cost analysis of misdiagnosis of rheumatoid arthritis. Value Health. 2019;19:S6–S7. doi:10.1016/j.vhri.2019.08.035
86. Aranda DF, Benincasa T, Romero-Sánchez C, Chila L, Bautista Molano W. Estimation of the impact of a strategy to optimize costs on national health-care system in patients with rheumatoid arthritis: a direct cost analysis. Ann Rheum Dis First Published. 2020;79(Suppl1):513–514. doi:10.1136/annrheumdis-2020-eular.2964Getrightsandcontent
87. Tanaka S, Porter JK, Santos F, Aratangy G. Cost-effectiveness analysis of adalimumab biosimilar for rheumatoid arthritis in Brazil compared to delayed biologic treatment initiation. Value Health. 2020;23:S413–S414. doi:10.1016/j.jval.2020.08.097
88. Peña S, Lopez Q, Diaz J. Cost- effectiveness analysis of the clinical approach for RA patients in the early phase versus those in the established phase from a fourth -level health servicie provider institution in Colombia. Ann Rheum Dis. 2021;80(Suppl 1):1428–1429. doi:10.1136/annrheumdis-2021-eular.3877
89. Cid C, Flores G, Del Riego A, Fitzgerald J. Sustainable development goals: impact of lack of financial protection in health in Latin American and Caribbean countries. Revista Panamericana de Salud Publica/Pan Ame J Public Health. 2021;45:1–10. doi:10.26633/RPSP.2021.95
90. Petrera Pavone M, Jiménez Sánchez E. Determinants of out-of-pocket spending on health among the poor population served by public health services in Peru, 2010–2014. Revista Panamericana de Salud Publica/Pan Ame J Public Health. 2018;42:e20. doi:10.26633/RPSP.2018.20
91. Catalá -lópez F, García-Altés A. Evaluación económica de intervenciones sanitarias en España 1983 a 2008. Rev Esp Salud Publica. 2010;84(4):353–369. doi:10.1590/S1135-57272010000400002
92. Chevreul K, Haour G, Lucier S, et al. Evolution of direct costs in the first years of rheumatoid arthritis: impact of early versus late biologic initiation - An economic analysis based on the ESPOIR cohort. PLoS One. 2014;9(5). doi:10.1371/journal.pone.0097077
93. Karpes Matusevich Aliza R, Suarez- Almorzor Maria E, Cantor Scott B, Lal Lincy S, Swint JM, Lopez-Olivo Maria A. Systematic review of economic evaluations of cycling versus swapping medications in patients with Rheumatoid Arthritis after failure to respond to tumor necrosis factor inhibitors. Arthritis Cares Res. 2020;72(3):343–352. doi:10.1002/acr.23859
94. Moots RJ, Mays R, Stephens J, Tarallo M. Burden of dose escalation with tumor necrosis factor inhibitors in rheumatoid arthritis: a systematic review of frequency and costs. Clin Exp Rheumatol. 2015;33(5):737–745.
95. Ping-Husuan H, Olivia W, Claudia G, Emma M, Lain M, Stefan S. Economic burden of rheumatoid arthritis: a systematic review of literature in biologic era. Ann Rheum Dis. 2020;79(6):771–777. doi:10.1136/annrheumdis-2019-216243
96. Yoo DH. The rise of biosimilars: potential benefits and drawbacks in rheumatoid arthritis. Expert Rev Clin Immunol. 2014;10(8):981–983. doi:10.1586/1744666X.2014.932690
97. Lapadula G, Ferraccioli GF. Biosimilars in rheumatology: pharmacological and pharmacoeconomic issues. Clin Expert Rheumatol. 2012;4(73):S102–106.
98. Gulácsi L, Brodszky V, Baji P, et al. Biosimilars for the management of rheumatoid arthritis: economic considerations. Expert Rev Clin Immunol. 2015;11:S43–S52. doi:10.1586/1744666X.2015.1090313
99. Haustein R, de Millas C, Ariane H. Saving money in the European healthcare systems with biosimilars. GaBI J. 2012;1(3–4):120–126. doi:10.5639/gabij.2012.0103-4.036
100. Juang H, Alex K. 5 year budget impact analysis of biosimilar infliximab for the treatment of rheumatoid arthritis in UK, Italy, France and Germany - ACR meeting abstracts. Arthritis Rheumatol. 2014;11:S512.
101. Aladul MI, Fitzpatrick RW, Chapman SR. Impact of infliximab and etanercept biosimilars on biological disease-modifying antirheumatic drugs utilisation and NHS budget in the UK. BioDrugs. 2017;31(6):533–544. doi:10.1007/s40259-017-0252-3
102. Kowalski SC, Benavides JA, a B RP, et al. PANLAR consensus statement on biosimilars. Clin Rheumatol. 2019; 38:1485–96. doi:10.1007/s10067-019-04496-3
103. Gónzález G. Economía de la salud en el contexto de la salud pública cubana. Rev Cub Salud Publica. 2003;29(4):1.
104. Organización Panamericana de la salud. El Acceso a Los Medicamentos de Alto Costo En Las Américas: contexto, Desafios y Perspectivas. Organización Panamericana de la Salud; 2009. Available from: https://www3.paho.org/hq/dmdocuments/2009/Acceso-alto-costo-Inf-Tec-1-Oct-5-2009.pdf.
105. Valentina A, Juan O. Informe-19 La Diferencia En El Nivel de Precios Entre Paises Causas y Comparación.; 2023. Available from: https://ocec.udp.cl/proyecto/informe-no19-la-diferencia-en-el-nivel-de-precios-entre-paises-causas-y-comparacion/.
106. Xu K, Soucat A, Kutzin J, et al. Public Spending on Health: a Closer Look at Global Trends. World Health Organization; 2018. Available from: https://iris.who.int/bitstream/handle/10665/276728/WHO-HIS-HGF-HF-WorkingPaper-18.3-eng.pdf.
107. de Alto Costo C. Fondo Colombiano de Enfermedades de Alto Costo. Consenso Basado En Evidencia. Indicadores de Gestión Del Riesgo En Pacientes Con Artritis Reumatoide.; 2018. Available from: https://cuentadealtocosto.org/wp-content/uploads/2019/10/indicadores_de_gestion_de_riesgo_artritis_reumatoide.pdf.
108. Balsa Criado A, Diaz Del Campo Fontecha P, Aguado García J, et al. Recomendaciones SER sobre la gestión de riesgo del trtamiento con FAME biológicos o sintéticos dirigidos en pacientes con Artritis Reumatoide. Reumatol Clin. 2023;19(10):533–548. doi:10.1016/j.reuma.2023.07.001
109. Zarate V. Evaluaciones económicas en salud: conceptos básicos y clasificación. Rev Med Chile. 2010;138(2):93–97. doi:10.4067/S0034-98872010001000007
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.