")
Back to Journals » Journal of Inflammation Research » Volume 17
Construction and Comparison of Multiple Serum-Based Prognostic Models for Predicting the Prognosis of Acute Exacerbations of Chronic Obstructive Pulmonary Disease
Authors Wang N, Wang G, Li M, Liu T , Ji W, Hu T, Shi Z
Received 6 August 2024
Accepted for publication 2 November 2024
Published 7 November 2024 Volume 2024:17 Pages 8395—8406
DOI https://doi.org/10.2147/JIR.S461961
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Na Wang, Guangdong Wang, Mengcong Li, Tingting Liu, Wenwen Ji, Tinghua Hu, Zhihong Shi
Department of Respiratory and Critical Care Medicine, First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, Shaanxi, CN, 710061, People’s Republic of China
Correspondence: Zhihong Shi, Department of Respiratory and Critical Care Medicine, First Affiliated Hospital of Xi’an Jiaotong University, No. 277 Yanta Road, Yanta District, Xi’an, Shaanxi, CN, 710061, People’s Republic of China, Tel +862985323854, Email [email protected]
Purpose: Acute exacerbations of chronic obstructive pulmonary disease (AECOPD) are associated with significant poor prognosis. Lymphocyte-to-Monocyte Ratio (LMR), Neutrophil-to-Lymphocyte Ratio (NLR), Eosinophil-to-Lymphocyte Ratio (ELR), Basophil-to-Lymphocyte Ratio (BLR), Platelet-to-Lymphocyte Ratio (PLR), and Hemoglobin, Albumin, Lymphocyte, and Platelet (HALP) are vital indicators for inflammation, immune status, and nutritional condition. This study evaluated the predictive value of these indicators in AECOPD and developed predictive models to assess the prognosis of AECOPD based on these indicators.
Patients and Methods: We retrospectively collected data from 2609 AECOPD patients. The outcomes assessed included occurrence of respiratory failure (RF), intensive care unit (ICU) stay, mechanical ventilation (MV), and 30-day readmission. We evaluated the predictive ability of LMR, NLR, PLR, BLR, ELR, and HALP for predicting the prognosis of AECOPD patients. Furthermore, based on these indicators, we utilized LASSO regression and multivariable analysis to develop models for predicting the prognosis of AECOPD patients. The predictive value of these indicators and the performance of the models were assessed using AUCs.
Results: LMR exhibited AUCs of 0.612 for RF, 0.715 for ICU stay, 0.714 for MV, and 0.624 for 30-day readmission. Other indicators, including NLR, PLR, BLR, EMR, and HALP, showed AUCs ranging from 0.621 to 0.699 for predicting these outcomes in AECOPD. The models developed using LASSO regression and multivariable analysis yielded AUCs of 0.717 for RF, 0.773 for ICU stay, 0.780 for MV, and 0.682 for 30-day readmission. Incorporating LMR, NLR, PLR, BLR, ELR, and HALP into the models individually further enhanced predictive performance, particularly with LMR (AUCs of 0.753 for RF, 0.797 for ICU stay, 0.802 for MV, and 0.697 for 30-day readmission), NLR (AUCs of 0.753 for RF, 0.796 for ICU stay, 0.802 for MV, and 0.698 for 30-day readmission), and HALP (AUCs of 0.752 for RF, 0.790 for ICU stay, 0.797 for MV, and 0.697 for 30-day readmission).
Conclusion: Indicators of LMR, NLR, PLR, BLR, ELR, and HALP showed good performance in predicting outcomes for AECOPD patients. The integration of these indicators into prognostic models significantly enhances their predictive efficacy.
Keywords: AECOPD, prediction, outcome, models
Introduction
Chronic obstructive pulmonary disease (COPD) is a prevalent chronic condition worldwide, characterized by persistent airflow limitation.1 Acute exacerbation of COPD (AECOPD) refers to the worsening of respiratory symptoms in patients, is the primary cause of increased hospitalizations, in-hospital mortality, readmission and healthcare costs among individuals with COPD.2–5
Accurate prognostic modeling for AECOPD is essential for early identification of high-risk patients, particularly given the potential for occurrence of respiratory failure (RF), the need for intensive care unit (ICU) stay, and mechanical ventilation (MV) usage, as well as the risk of 30-day readmission. Several studies have previously attempted to develop predictive models for AECOPD outcomes. For instance, one study created a model to predict the likelihood of RF in AECOPD patients upon hospital admission,6 while another utilized machine learning to identify patient profiles at high risk for hospital readmissions in France.7 Additionally, a model focused on predicting ICU admissions based on blood indicators for AECOPD patients.8 These models typically incorporate routine clinical and serological indicators; however, there is no consensus on the most effective serum-based biomarkers. Recent literature has suggested various serum-based ratios, such as the Lymphocyte-to-Monocyte Ratio (LMR) and Neutrophil-to-Lymphocyte Ratio (NLR), as potentially valuable prognostic indicators. Nonetheless, comprehensive models that fully integrate these indicators remain underexplored.
The prognosis of AECOPD is influenced by various factors, including the degree of inflammation, immune status, and nutritional status.9–11 Indicators such as Eosinophil-to-Lymphocyte Ratio (ELR) reflect the degree of inflammation, NLR can indicate immune status, Basophil-to-Lymphocyte Ratio (BLR) plays a role in inflammatory responses, Platelet-to-Lymphocyte Ratio (PLR) is associated with inflammation and thrombosis,12 LMR reflects immune-inflammatory status,13 and the composite index Hemoglobin, Albumin, Lymphocyte, and Platelet (HALP) provides a comprehensive evaluation of nutritional status and immune function,14 these factors hold significant relevance in the realms of inflammation, immune status, and nutritional condition, and are widely utilized in the prognosis assessment and treatment monitoring of various diseases, such as prostate cancer and kidney cancers.15,16 Within the domain of AECOPD, these indicators potentially holding predictive value for the prognosis of AECOPD patients, and research on these indicators is gradually expanding.14 Some indicate that these indicators are associated with the length of hospital stay (LOS), disease severity, and prognosis of AECOPD patients.17,18 However, previous studies have focused on individual or a few of these indicators, rarely comparing the predictive value of these clinical indicators within the same study population, and have not developed predictive models based on these clinical indicators. Therefore, it is necessary to conduct more in-depth research to explore the potential roles and clinical application prospects of these indicators in AECOPD patients.
To address the research gap, this study aims to evaluate the predictive abilities of LMR, NLR, PLR, BLR, ELR, and HALP for the outcomes of hospitalized patients with AECOPD, specifically focusing on RF, ICU stay, MV usage, and 30-day readmission. Further, we will utilize LASSO regression and multivariate analysis to identify factors associated with AECOPD prognosis and develop predictive models based on these indicators. We aim to provide more beneficial information for personalized medical care and precision treatment, thereby improving the treatment outcomes of AECOPD patients. This research will contribute to expanding our understanding of AECOPD prognosis assessment, offering new insights and directions for clinical practice and future research.
Materials and Methods
Ethical Considerations
This study adhered to the tenets of the Declaration of Helsinki. Approval from the Ethics Committee of the First Affiliated Hospital of Xi’an Jiaotong University was secured (Approval number: XJTU1AF2022LSL-012). Additionally, ethical clearance (Approval number: XJTU1AF2022LSK-324) was obtained for exemptions related to privacy removal, including informed consent exemptions.
Study Population
Data of patients hospitalized due to AECOPD between January 1, 2018 and December 31, 2022 were anonymously collected from the Biobank of the First Affiliated Hospital of Xi’an Jiaotong University. The diagnostic code of AECOPD was (ICD: J44.900). The diagnosis of COPD was based on the GOLD 2017 criteria, where pulmonary function tests revealed a post-bronchodilator forced expiratory volume in 1 second/forced vital capacity (FEV1/FVC) ratio of less than 0.7.1 AECOPD was defined as an exacerbation of respiratory symptoms (increased dyspnea, sputum volume, and purulence) beyond daily variations, necessitating additional treatment.1
Exclusion criteria included: (1) Age < 40 years; (2) Coexisting any of the following diseases: asthma, active tuberculosis, any malignancy; (3) Presence of other acute diseases: acute myocardial infarction or acute heart failure; (4) Death during hospitalization.
Data Collection
Patient demographics (age, gender), comorbidities, and LOS, which indicates the length of hospital stay from admission to discharge, were collected. Comorbidities included coronary heart disease (CHD), congestive heart failure, hypertension, diabetes, autoimmune disease, chronic kidney disease (CKD), and chronic liver disease. Upon admission, laboratory tests included routine blood tests, hepatic and renal function, blood coagulation function, C-reactive protein (CRP), N-terminal pro-B-type natriuretic peptide (NT-proBNP), and erythrocyte sedimentation rate (ESR) levels. ELR, NLR, BLR, PLR, LMR, and HALP were derived from the laboratory findings. HALP score was calculated as hemoglobin (g/L) × albumin (g/L) × lymphocytes (/L)/platelets (/L).14 Treatment included systemic corticosteroid usage (oral or intravenous), inhaled corticosteroids (ICS), antibiotics, oxygen therapy, and MV during the hospital stay. ICU stay and all-cause readmission within 30 days post-discharge were also recorded.
Statistical Analysis
In our study, the proportion of missing values for individual variables was less than 10% (9.05%) (Supplementary Figure 1), we used multiple imputation to handle data. We implemented the predictive mean matching method and created a total of 5 imputed datasets. We used the variance inflation factor (VIF) calculations for assessing multicollinearity, variables with VIFs above 10 were typically considered to have problematic multicollinearity and were removed (neutrophil, eosinophil percentage, and lactose dehydrogenase), details were shown in Supplementary Table 1. Outcomes were occurrence of RF during hospitalization, ICU stay, MV requirement, and 30-day readmission. Diagnosis of RF was determined by discharge records but not arterial blood gas analysis. We compared the with and without RF groups during hospitalization, ICU stay and non-ICU stay groups, MV and non-MV groups, as well as all-cause readmission and non-readmission within 30 days groups, respectively. Continuous variables were presented as means ± standard deviations (SD) or median with interquartile range (IQR), and categorical variables as frequencies and percentages (%). Statistical comparisons used Student’s t-test or the Mann–Whitney U-test for continuous variables, and either chi-square test or Fisher’s exact test for categorical variables.
We first assessed the predictive performance of indicators (LMR, NLR, PLR, BLR, ELR, and HALP) individually for outcomes with area under the curve (AUC), and using receiver operating characteristic (ROC) curves to visualize. After that, we screened the variables by least absolute shrinkage and selection operator (LASSO) regression from significant factors (listed in Supplementary Table 2). The selected factors further entered a multivariable analysis to identify factors significantly associated with the outcomes. The identified factors were furthor included to develop models for predicting the prognosis of AECOPD patients. LASSO improves computational efficiency by determining optimal adjustment parameter values, balancing bias and variance for better regression analysis. It also addresses overfitting by shrinking regression coefficients to zero, enhancing model interpretability.19 Model stability and generalizability were assessed using 10-fold cross-validation. Finally, based on LMR, NLR, PLR, BLR, ELR, and HALP, added the variables above selected by LASSO regression and multivariate analysis to establish the prediction models. The predictive performances of models were assessed by AUCs, and also visualized bu ROC curves.
All of the analyses were performed using R software (version 4.3.2), P < 0.05 was considered to be statistically significant (two-sides).
Results
Patients Enrollment and Baseline Characteristics of the Study Population
As shown in Figure 1, A total of 3611 patients hospitalized due to AECOPD between January 1, 2018 and December 31, 2022. 7 patients were excluded for age < 40 years, 995 patients were excluded for coexisting asthma, active tuberculosis, malignancy, acute myocardial infarction, acute heart failure, or died during hospitalization. Finally, 2609 patients were enrolled in this study, among them, 727 (27.87%) developed RF during hospitalization, 618 (23.69%) required ICU stay, 455 (17.44%) needed MV, and 199 (7.63%) patients readmission within 30 days of discharge.
 |
Figure 1 Flow chart of the study. Abbreviations: AECOPD, acute exacerbations of chronic obstructive pulmonary disease; RF, respiratory failure; ICU, intensive care unit; MV, mechanical ventilation. Notes: a including patients who coexisting multiple diseases or died during hospitalization. |
Of the total patients in this study, the median age was 71 years, 1998 (77%) patients were male, median length of hospitalization was 7 days, and cost was 13904 RMB. Congestive heart failure was the most prevalent comorbidity among these patients (970, 37%), followed by hypertension (766, 29%), CHD (722, 28%), arrhythmia (507, 19%), diabetes (305, 12%), CKD (77, 3.0%), and chronic liver disease (76, 2.9%), only 0.8% (21) of patients had a coexisting autoimmune disease. The median LMR was 2.56, NLR was 5, PLR was 174, BLR was 0.017, ELR was 0.06, and HALP was 29 (Table 1).
 |
Table 1 Baseline Characteristics of All Population and Comparison Between the RF and Non-RF Group |
Compared to patients who did not develop respiratory failure (RF) during hospitalization, those who did experienced higher hospitalization costs, longer LOS, and a greater prevalence of coexisting cardiovascular diseases and diabetes (all P < 0.05). Among the laboratory findings upon admission, significant differences were observed in NT-proBNP, CRP, leukocyte counts, LMR, NLR, PLR, and HALP (all P < 0.05). Furthermore, these patients required more systemic corticosteroid therapy, antibiotics, and MV, and they had a higher rate of admission to the ICU (all P < 0.01) (Table 1).
Similar findings were noted when comparing the ICU stay versus non-ICU stay groups, MV versus non-MV groups, and those readmitted within 30 days versus those not readmitted; further details are provided in Supplementary Tables 3–5.
Predictive Ability of LMR, NLR, PLR, BLR, ELR, and HALP
We assessed the predictive ability of individual indicators for outcomes in AECOPD patients. As detailed in Table 2, the AUC for LMR in predicting the development of RF during hospitalization was 0.612, while it was 0.715 for ICU stay, 0.714 for MV, and 0.624 for 30-day readmission, indicating a good predictive ability for LMR. The AUC for NLR was 0.667 for predicting RF during hospitalization, 0.689 for ICU stay, 0.687 for MV, and only 0.629 for 30-day readmission, suggesting a limited predictive capacity for 30-day readmission. Similarly, PLR, BLR, EMR, and HALP showed good predictive abilities for ICU stay and MV usage but exhibited poor predictive capabilities for RF during hospitalization and 30-day readmission. Detailed AUC values (95% CI) for each indicator in predicting outcomes are presented in Table 3, while maximum sensitivity and specificity are provided in Supplementary Table 6.
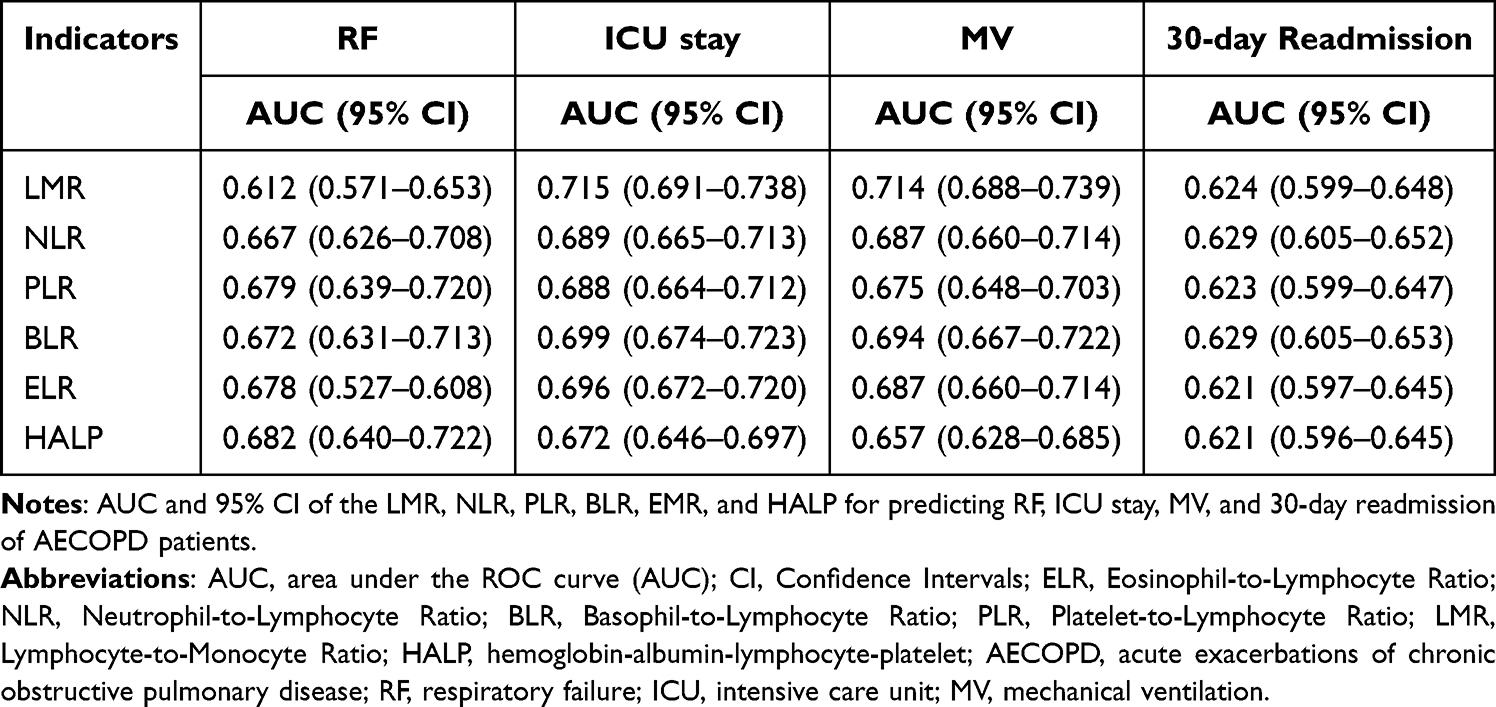 |
Table 2 AUC and 95% CI of the LMR, NLR, PLR, BLR, EMR, and HALP |
 |
Table 3 Multivariate Analysis of Predictive Factors of RF in AECOPD Patients |
Development of Models Based on LASSO Regression and Multivariate Analysis
A total of 27 factors encompassing age, gender, comorbidities, and laboratory tests were considered as potential prognostic factors influencing RF and were integrated into the LASSO regression analysis.
For the outcome of RF, the LASSO regression and 10-fold cross-validation results identified 15 factors associated with in-hospital mortality, with an optimal λ value of 0.0169 (Figure 2). These factors were subsequently included in the multivariate regression analyses. The findings indicated that older patients, as well as those with congestive heart failure, hypertension, CKD, higher leukocyte counts, total bilirubin levels, blood glucose, and alanine aminotransferase (ALT), along with increased NT-proBNP and lower levels of albumin and lymphocytes, as well as prolonged prothrombin time (PT), were more likely to have a poorer prognosis for RF (all P < 0.05) (Table 3).
 |
Figure 2 Results of LASSO regression and 10-fold cross-validation for outcome of RF. Abbreviations: LASSO, least absolute shrinkage and selection operator; RF, respiratory failure. Notes: Results of LASSO regression (a) and 10-fold cross-validation (b). 15 variables were selected when the optimal λ value was 0.0169. |
Regarding ICU stay, the LASSO regression and 10-fold cross-validation results demonstrated that 13 factors were associated with ICU stay when the optimal λ value was 0.0196 (Supplementary Figure 2). These factors were then included in the subsequent multivariate regression analyses, which unveiled 11 factors associated with ICU stay outcomes: congestive heart failure, CHD, CKD, leukocyte count, lymphocyte count, eosinophil count, basophil count, NT-proBNP, blood glucose, albumin, and PT (all P < 0.05) (Supplementary Table 7).
Concerning MV outcomes, the LASSO regression and 10-fold cross-validation results indicated that 14 factors were linked to MV when the optimal λ value was 0.0169 (Supplementary Figure 3). These factors were subsequently incorporated into the multivariate regression analyses, revealing 10 associated factors: LOS, congestive heart failure, CHD, leukocyte count, lymphocyte count, eosinophil count, total bilirubin, blood glucose, albumin, and ESR (all P < 0.05) (Supplementary Table 7).
For the outcome of 30-day readmission, the LASSO regression and 10-fold cross-validation results highlighted that 15 factors were associated with readmission when the optimal λ value was 0.0056 (Supplementary Figure 4). These factors were then included in subsequent multivariate regression analyses, which indicated that male patients, older individuals, those with longer LOS, lower albumin levels, higher CRP and creatinine levels, and prolonged APTT were associated with 30-day readmission (all P < 0.1) (Supplementary Table 7). In the multivariate analysis, only 4 variables (gender, age, LOS, and APTT) were significantly linked to the outcome at P < 0.05. Considering their clinical significance, variables with a statistical significance of P < 0.1 were included in establishing the model.
Performance of Individual Indicators and the Models
Based on factors identified through LASSO regression and multivariate analysis, we developed four predictive models: Model 1 for predicting the development of RF during hospitalization, Model 2 for predicting ICU stay, Model 3 for predicting MV usage, and Model 4 predicting 30-day readmission.
As shown in Figure 3, the AUC for Model 1 was 0.717, indicating good discrimination, while Model 2 achieved an AUC of 0.773, indicating excellent discrimination. Model 3 demonstrated an AUC of 0.780, also showing excellent discrimination, and Model 4 had an AUC of 0.682, indicating good discrimination.
 |
Figure 3 The ROC curve and AUC of the indicators and models. Abbreviations: AUC, area under the ROC curve (AUC); ROC, receiver operating characteristic; AECOPD, acute exacerbations of chronic obstructive pulmonary disease; RF, respiratory failure; ICU, intensive care unit; MV, mechanical ventilation. Notes: The ROC curve and AUC of the Models for predicting RF (a), ICU stay (b), MV usage (c), and 30-day readmission (d) of AECOPD patients. Model 1–4 were based on LASSO regression and multivariable analysis. Model 1: age, congestive heart failure, hypertension, CKD, Leukocyte, lymphocyte, NT-proBNP, total bilirubin, blood glucose, ALT, albumin, PT. Model 2: congestive heart failure, CHD, CKD, Leukocyte, lymphocyte, eosinophil, basophils, NT-proBNP, blood glucose, albumin, PT. Model 3: LOS, congestive heart failure, CHD, Leukocyte, lymphocyte, eosinophil, total bilirubin, blood glucose, albumin, erythrocyte sedimentation rate. Model 4: gender, age, LOS, albumin, CRP, creatinine, APTT. |
Next, we individually incorporated indicators of LMR, NLR, PLR, BLR, EMR, and HALP into Models 1 to 4 to enhance predictions for AECOPD patient outcomes. As shown in Figure 3, the predictive ability of the models significantly improved with the addition of these indicators, particularly LMR (AUCs of 0.753 for RF, 0.797 for ICU stay, 0.802 for MV, and 0.697 for 30-day readmission), NLR (AUCs of 0.753 for RF, 0.796 for ICU stay, 0.802 for MV, and 0.698 for 30-day readmission), and HALP (AUCs of 0.752 for RF, 0.790 for ICU stay, 0.797 for MV, and 0.697 for 30-day readmission).
Discussion
In this study, we explored the potential value of the indicators, including LMR, NLR, PLR, BLR, EMR, and HALP, in predicting the prognosis of AECOPD patients. We constructed multiple prognostic models based on these indicators, demonstrating their significant predictive capabilities, particularly in relation to serious outcomes such as RF, ICU stay, MV, and 30-day readmission, providing valuable insights into the clinical application of these indicators and models.
The results of our study indicated that LMR exhibited a good predictive ability across multiple outcomes, particularly with an AUC of 0.715 for ICU stay and 0.714 for MV. These findings align with previous literature that suggests the potential of LMR as an inflammatory marker in respiratory diseases, particularly in lung cancer,20–23 as well as in AECOPD17 and the prognosis of RF in patients with myasthenia gravis.24 Previous studies have found that the indicators of LMR, NLR, PLR, BLR, EMR, and HALP, which relevance in the realms of inflammation, immune status, and nutritional condition, are associated with the prognosis of a variety of diseases. A study based on NHANES 1999–2018 about general population found the HALP score was independently associated with all-cause mortality and cardiovascular mortality, and proposed that HALP score might be a reliable predictor of long-term outcome.14 Compared to healthy volunteers, the PLR, NLR, MLR, and ELR were correlated with increased in-hospital mortality in AECOPD patients.17 Moreover, the positive predictive capacities of NLR, PLR, BLR, ELR, and HALP for ICU stay and MV use reinforce the notion that systemic inflammatory responses play a crucial role in the trajectory of patients with AECOPD. Specifically, the AUC results indicate a varying level of efficacy among the different indicators in predicting the same clinical outcomes, highlighting the importance of selecting appropriate biomarkers for prognosis evaluation.
Interestingly, while some indicators demonstrated promising predictive capability, others showed limited utility, particularly in predicting RF during hospitalization and 30-day readmission. For instance, NLR displayed a relatively lower predictive value for 30-day readmission (AUC = 0.629), suggesting that factors beyond inflammatory indicators may be at play influencing this outcome. This finding compels further exploration into other potential predictors and their interactions with systemic inflammation in AECOPD patients.
The use of LASSO regression and multivariable analysis allowed us to identify key factors that contribute to prognosis and to develop four distinct predictive models tailored to each outcome of interest. The development of Model 1 for RF prediction achieved an AUC of 0.717, while Model 2 and Model 3 showcased excellent discrimination with AUCs of 0.773 and 0.780, respectively. However, Model 4 demonstrated slightly less predictive power (AUC = 0.682), indicating that while our models provide valuable insight into prognostic predictions, the prediction of 30-day readmission may benefit from additional or refined variables.
Significantly, the incorporation of serum-based indicators into our models notably enhanced predictive power, especially with the addition of LMR, NLR, and HALP. Notably, enhancements in predictive accuracy were observed, with AUCs improving to 0.753 for RF and 0.802 for MV with the inclusion of LMR, NLR, and HALP. This underscores the pivotal role these serum markers play in refining clinical predictions and decision-making processes in AECOPD management.
In conclusion, these findings suggest a promising avenue for personalizing management strategies in AECOPD patients, allowing clinicians to identify those at higher risk and tailor interventions accordingly. Future research could focus on validating these models in diverse populations and integrating them into clinical practice, potentially improving outcomes for patients through early identification and proactive treatment strategies. Additionally, exploring the underlying mechanisms of these inflammatory ratios may provide further insights into the pathophysiology of AECOPD and highlight new therapeutic targets.
This study has some strengths. Firstly, it covers a wide range of biomarkers, evaluating their potential value in predicting the prognosis of AECOPD patients from multiple perspectives. This comprehensive research design helps provide more comprehensive information and offers more options for clinical practice. Secondly, the study established multiple models to assess the predictive ability of biomarkers, including LASSO regression, univariate analysis, and multivariate analysis. This multi-model evaluation helps validate the stability and consistency of the results, enhancing the study’s credibility. Additionally, we considered a variety of clinical and laboratory parameters, including general clinical characteristics and biochemical markers. This comprehensive consideration aids in a more thorough assessment of the predictive value of biomarkers. In our previous research,25 we utilized a Lasso-Cox model, primarily focusing on the survival probabilities of AECOPD patients. This study employs more recent data (from January 1, 2018, to December 31, 2022, while previous research from January 01, 2012 to December 31, 2022), in which the proportion of missing values for individual variables was less than 10%. We applied multiple imputation methods to address data gaps (key variables such as CRP and NT-proBNP) and utilized a logistic regression model to assess various clinical outcomes, including death, ICU stay, MV usage, and 30-day readmissions, thereby advancing this research. This approach permitted the inclusion of critical inflammatory markers and composite indicators, allowing for an exploration of the clinical predictive efficacy of several composite measures. Furthermore, by constructing multiple predictive models, we significantly enhanced the model’s predictive capacity and provided insights of greater clinical relevance for patient management. Lastly, our study findings revealed limitations in the predictive efficacy of Model 3 and individual biomarkers, pointing towards new research directions for future studies. This discovery can guide the direction of future research and drive advancements in related fields.
This study also has some limitations. Firstly, as a retrospective single-center study, there may be selection bias and information bias. Retrospective study designs may not control for all potential confounding factors, and single-center data may not represent the diversity and variability of the entire patient population. Therefore, caution is needed when generalizing the study results to a broader population, and further multicenter studies may be required to validate the findings. Secondly, this study lacks some important data such as lung function, Body Mass Index, and smoking status, which are vital for assessing the severity and prognosis of AECOPD patients. The absence of these data may impact the comprehensive evaluation of the overall patient condition and could influence the results of the correlation analysis between the indicators and clinical outcomes. Future research should aim to collect more comprehensive data to more accurately assess the role of these indicators in the prognosis of AECOPD patients. Additionally, while we utilized LASSO regression with 10-fold cross-validation to ensure the stability of our selected variables in model construction, the lack of separate training and validation cohorts presents another limitation. This absence may affect the external validity of our predictive model. Acknowledging this, we recommend that future studies include independent datasets to validate our findings and enhance the robustness of the model.
Conclusions
Our study highlights the significant predictive value of LMR, NLR, PLR, BLR, ELR, and HALP measure in determining the prognosis of AECOPD patients. The developed predictive models, utilizing LASSO regression and multivariable analysis, demonstrated enhanced accuracy across key clinical outcomes, including respiratory failure, ICU stay, mechanical ventilation requirements, and 30-day readmissions. Our work paves the way for a more nuanced understanding of AECOPD prognosis and reinforces the importance of integrating inflammatory and immune status indicators into clinical assessments.
Abbreviations
AECOPD, acute exacerbation of chronic obstructive pulmonary disease; APTT, activated partial thromboplastin time; AUC, area under the ROC curve; BLR, Basophil-to-Lymphocyte Ratio; BUN, blood urea nitrogen; COPD, chronic obstructive pulmonary disease; CKD, chronic kidney disease; CHD, coronary heart disease; CRP, C-reactive protein; CI, confidence interval; ELR, Eosinophil-to-Lymphocyte Ratio; ESR, erythrocyte sedimentation rate; FEV1, forced expiratory volume in one-second; FVC, forced vital capacity; GOLD, Global Initiative for Chronic Obstructive Lung Disease; HALP, hemoglobin-albumin-lymphocyte-platelet; ICU, intensive care unit; ICS, inhaled corticosteroids; IQR, interquartile range; LMR, lymphocyte -to-monocyte ratio; LOS, length of hospital stay; LASSO, least absolute shrinkage and selection operator; MV, mechanical ventilation; NT-proBNP, N-terminal pro-B-type natriuretic peptide; NLR, Neutrophil-to-Lymphocyte ratio; OR, odds ratio; PLR, platelet-to-lymphocyte ratio; PT, prothrombin time; ROC, receiver operating characteristic; SD, standard deviation; VIF, variance inflation factor.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
We thank all the team members. We thank the biobank of First Affiliated Hospital of Xi’an Jiao tong University for providing clinical data. We thank the National Key Research and Development Program for supporting the study.
Funding
This work was supported by the National Key Research and Development Program (Project Number: 2016YFC1304602).
Disclosure
The authors declares that there is no conflict of interest.
References
1. Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am J Respir Crit Care Med. 2017;195(5):557–582. doi:10.1164/rccm.201701-0218PP
2. Rodriguez-Roisin R. Toward a consensus definition for COPD exacerbations. Chest. 2000;117(5 Suppl 2):398s–401s. doi:10.1378/chest.117.5_suppl_2.398s
3. Criner GJ, Bourbeau J, Diekemper RL, et al. Prevention of acute exacerbations of COPD: American college of chest physicians and Canadian thoracic society guideline. Chest Apr. 2015;147(4):894–942. doi:10.1378/chest.14-1676
4. GOLD. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2023 REPORT). Available from: https://goldcopd.org/2023-gold-report-2/.
5. Alqahtani JS, Aldabayan YS, Aldhahir AM, Al Rajeh AM, Mandal S, Hurst JR. Predictors of 30- and 90-Day COPD exacerbation readmission: a prospective cohort study. Int J Chron Obstruct Pulmon Dis. 2021;16:2769–2781. doi:10.2147/copd.S328030
6. Hu S, Zhang Y, Cui Z, Tan X, Chen W. Development and validation of a model for predicting the early occurrence of RF in ICU-admitted AECOPD patients: a retrospective analysis based on the MIMIC-IV database. BMC Pulm Med. 2024;24(1):302. doi:10.1186/s12890-024-03099-2
7. Cavailles A, Melloni B, Motola S, et al. Identification of patient profiles with high risk of hospital re-admissions for acute COPD exacerbations (AECOPD) in France using a machine learning model. Int J Chron Obstruct Pulmon Dis. 2020;15:949–962. doi:10.2147/copd.S236787
8. Bai JS, Liu JX, Zhang Q, et al. A predictive model based on blood indicators for admission to the ICU with AECOPD. Clin Lab. 2022;68(10). doi:10.7754/Clin.Lab.2022.220145
9. Zeng Z, Ke X, Gong S, et al. Blood urea nitrogen to serum albumin ratio: a good predictor of in-hospital and 90-day all-cause mortality in patients with acute exacerbations of chronic obstructive pulmonary disease. BMC Pulm Med. 2022;22(1):476. doi:10.1186/s12890-022-02258-7
10. Ugajin M, Yamaki K, Iwamura N, Yagi T, Asano T. Blood urea nitrogen to serum albumin ratio independently predicts mortality and severity of community-acquired pneumonia. Int J Gen Med. 2012;5:583–589. doi:10.2147/ijgm.S33628
11. Sehgal IS, Dhooria S, Agarwal R. Chronic obstructive pulmonary disease and malnutrition in developing countries. Curr Opin Pulm Med. 2017;23(2):139–148. doi:10.1097/mcp.0000000000000356
12. Kökoğlu K, Şahin MI. Use of neutrophil, eosinophil, basophil, and platelet to lymphocyte ratio to predict patient satisfaction after septoplasty plus inferior turbinate reduction. J Craniofac Surg. 2019;30(4):1022–1026. doi:10.1097/scs.0000000000005527
13. Gawiński C, Mróz A, Roszkowska-Purska K, et al. A prospective study on the roles of the Lymphocyte-to-Monocyte Ratio (LMR), Neutrophil-to-Lymphocyte Ratio (NLR), and Platelet-to-Lymphocyte Ratio (PLR) in patients with locally advanced rectal cancer. Biomedicines. 2023;11(11):3048. doi:10.3390/biomedicines11113048
14. Pan H, Lin S. Association of hemoglobin, albumin, lymphocyte, and platelet score with risk of cerebrovascular, cardiovascular, and all-cause mortality in the general population: results from the NHANES 1999-2018. Front Endocrinol. 2023;14:1173399. doi:10.3389/fendo.2023.1173399
15. Hadadi A, Smith KE, Wan L, et al. Baseline basophil and basophil-to-lymphocyte status is associated with clinical outcomes in metastatic hormone sensitive prostate cancer. Urol Oncol. 2022;40(6):271.e9–271.e18. doi:10.1016/j.urolonc.2022.03.016
16. Peng D, Zhang CJ, Tang Q, et al. Prognostic significance of the combination of preoperative hemoglobin and albumin levels and lymphocyte and platelet counts (HALP) in patients with renal cell carcinoma after nephrectomy. BMC Urol. 2018;18(1):20. doi:10.1186/s12894-018-0333-8
17. Liao QQ, Mo YJ, Zhu KW, et al. Platelet-to-Lymphocyte Ratio (PLR), Neutrophil-to-Lymphocyte Ratio (NLR), Monocyte-to-Lymphocyte Ratio (MLR), and Eosinophil-to-Lymphocyte Ratio (ELR) as biomarkers in patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease (AECOPD). Int J Chron Obstruct Pulmon Dis. 2024;19:501–518. doi:10.2147/copd.S447519
18. Yao C, Liu X, Tang Z. Prognostic role of neutrophil-lymphocyte ratio and platelet-lymphocyte ratio for hospital mortality in patients with AECOPD. Int J Chron Obstruct Pulmon Dis. 2017;12:2285–2290. doi:10.2147/copd.S141760
19. Zhou ZR, Wang WW, Li Y, et al. In-depth mining of clinical data: the construction of clinical prediction model with R. Ann Transl Med. 2019;7(23):796. doi:10.21037/atm.2019.08.63
20. Diem S, Schmid S, Krapf M, et al. Neutrophil-to-Lymphocyte ratio (NLR) and Platelet-to-Lymphocyte ratio (PLR) as prognostic markers in patients with non-small cell lung cancer (NSCLC) treated with nivolumab. Lung Cancer. 2017;111:176–181. doi:10.1016/j.lungcan.2017.07.024
21. Mandaliya H, Jones M, Oldmeadow C, Nordman II. Prognostic biomarkers in stage IV non-small cell lung cancer (NSCLC): neutrophil to lymphocyte ratio (NLR), lymphocyte to monocyte ratio (LMR), platelet to lymphocyte ratio (PLR) and advanced lung cancer inflammation index (ALI). Transl Lung Cancer Res. 2019;8(6):886–894. doi:10.21037/tlcr.2019.11.16
22. Sehgal SA, Malik G, Sachdeva A, et al. Pretreament neutrophil-lymphocyte ratio (NLR): a felicitous prognostic marker in carcinoma lung. J Cancer Res Ther. 2023;19(Suppl 2):S719–s723. doi:10.4103/jcrt.jcrt_688_22
23. Ramos R, Macía I, Navarro-Martin A, et al. Prognostic value of the preoperative lymphocyte-to-monocyte ratio for survival after lung cancer surgery. BMC Pulm Med. 2021;21(1):75. doi:10.1186/s12890-021-01446-1
24. Huang X, Xu M, Wang Y, et al. The systemic inflammation markers as possible indices for predicting respiratory failure and outcome in patients with myasthenia gravis. Ann Clin Transl Neurol. 2023;10(1):98–110. doi:10.1002/acn3.51706
25. Wang N, Li M, Wang G, et al. Development and validation of a nomogram for assessing survival in acute exacerbation of chronic obstructive pulmonary disease patients. BMC Pulm Med. 2024;24(1):287. doi:10.1186/s12890-024-03091-w
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.