")
Back to Journals » Clinical Ophthalmology » Volume 18
Corneal Biomechanical Changes in Patients with Inherited Retinal Diseases
Authors Marta A , Ferreira A , Couto I, Neves MM , Gomes M , Oliveira L , Azevedo Soares C , Menéres MJ , Lemos C, Melo Beirão J
Received 19 July 2024
Accepted for publication 12 September 2024
Published 19 September 2024 Volume 2024:18 Pages 2611—2618
DOI https://doi.org/10.2147/OPTH.S478846
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ana Marta,1,2 André Ferreira,1,3,4 Inês Couto,1 Miguel Mesquita Neves,1 Miguel Gomes,1 Luis Oliveira,1 Celia Azevedo Soares,5– 8 Maria João Menéres,1,2 Carolina Lemos,2,8 João Melo Beirão1,2
1Department of Ophthalmology, Centro Hospitalar Universitário de Santo António, Unidade Local de Saúde de Santo António, Porto, Portugal; 2Instituto Ciências Biomédicas Abel Salazar (ICBAS), Porto, Portugal; 3Department of Biomedicine - Unit of Anatomy, Faculty of Medicine of University of Porto, Porto, Portugal; 4Centre for Health Technology and Services Research, Health Research Network (CINTESIS@RISE), Faculty of Medicine of the University of Porto, Porto, Portugal; 5Medical Genetics Department, Centro Hospitalar Universitário de Santo António, Unidade Local de Saúde de Santo António, Porto, Portugal; 6Unit for Multidisciplinary Research in Biomedicine, Instituto de Ciências Biomédicas Abel Salazar, Universidade do Porto, Porto, Portugal; 7Medical Science Department, Universidade de Aveiro, Aveiro, Portugal; 8i3S - Instituto de Investigação e Inovação em Saúde, Universidade do Porto, Porto, Portugal
Correspondence: Ana Marta, Centro Hospitalar Universitário de Santo António, Unidade Saúde Local de Santo António, EPE (ULSSA), Largo do Prof. Abel Salazar, Porto, 4099-001, Portugal, Email [email protected]
Purpose: Inherited retinal diseases (IRDs) are a group of degenerative disorders of the retina, that can be potentially associated with changes in the anterior segment, but their prevalence and impact are not known. Exploring these concomitant ophthalmologic changes with biomechanical assessment may help identify other non-retina causes of vision loss in these patients, such as corneal ectasia or susceptibility to glaucoma. This study aimed to measure and compare corneal biomechanics in patients with and without IRDs.
Methods: A total of 77 patients (154 eyes) with IRD were recruited as the study group. The control group consisted of 77 healthy adults (154 eyes) with matched age and sphere equivalents. All participants underwent a comprehensive assessment including corneal tomography (Pentacam®) and biomechanical assessment (Corvis ST®). A total of 4 second-generation biomechanical parameters and 3 indexes were collected: Ambrosio Relational Thickness (ARTh), Deflection Amplitude Ratio Max (DARM), Integrated Radius (IR) and Stiffness Parameter at Applanation (SP-A1), the final deviation value D of the Belin/Ambrosio Enhanced Ectasia Display (BAD-D), Corvis Biomechanical Index (CBI) and Tomographic Biomechanical Index (TBI).
Results: For IRD patients, there was a higher DARM (p < 0.001), lower ARTh (p < 0.001), higher CBI (p < 0.001), higher TBI (p< 0.001), and higher BAD-D (p < 0.001) compared to the control group. Regarding discrimination of healthy subjects and IRD patients, ARTh was the most sensitive parameter.
Conclusion: The results showed that IRD patients tend to have softer corneal behaviour, compared to eyes without pathology, which may predispose patients to corneal ectasia or glaucoma development. ARTh could be used to screen IRD patients if a non-retina cause of vision loss is suspected.
Keywords: IRD, corneal biomechanics, corneal tomography
Introduction
Inherited retinal diseases (IRDs) are a group of degenerative disorders of the retina, characterized by clinical and genetic heterogeneity.1 Despite this heterogeneity, overall, retinal findings have been well characterized.2–5 Associations with other non-retina findings, such as cataracts, open-angle glaucoma, keratoconus and uveitis, have also been reported.6–11 However, their prevalence and impact are not known. Exploring these concomitant ophthalmologic changes may help identify other non-retina causes of vision loss in these patients.
In recent years, there has been interest in corneal biomechanics, primarily for early keratoconus screening and for the safe selection of patients for refractive surgery. Another clinical application is to improve intraocular pressure measurement in glaucoma patients.12 Corneal biomechanics can also reflect the vulnerability of the optic nerve head to glaucoma.13 Furthermore, it is believed that the elastic properties of the cornea reflect the overall elasticity of collagen fibres in the entire eyeball, making corneal biomechanics as an indicator of overall globe biomechanical properties.14,15
Exploring the biomechanical properties of biological tissue can also be important to improve our understanding of disease pathogenesis, staging, and optimise the surgical manipulation of tissues and, potentially, the design and properties of implantable prostheses and other therapies.16
To this date, no studies have been published in the literature presenting the results of the corneal biomechanical assessments in IRDs. In the same way that keratoconus can be potentially associated with anatomical and functional changes in the posterior segment,17 IRDs can be potentially associated with changes in the anterior segment, including changes in cornea biomechanical behaviour.
The aim of this study was to measure and compare corneal biomechanics in patients with and without IRDs. This can help to understand if there is a higher risk of corneal ectasia or glaucoma development in these patients.
Methods
Study Design
An observational cross-sectional study was performed, and it included a group of patients with a diagnosis of IRDs (Group 1) and a comparison group of healthy patients (Group 2) observed at the Ophthalmology department at the Unidade Local Saúde de Santo António (ULSSA) between November 2022 and November 2023. The study complied with the tenets of the Declaration of Helsinki for biomedical research. Institutional Review Board (IRB)/Ethics Committee approval was obtained from the Departamento de Ensino, Formação e Investigação (DEFI) of Centro Hospitalar Universitário de Santo António (CHUdSA) with reference number 2021.269 (216-DEFI/224-CE). Written informed consent was obtained from all patients.
Participants
The inclusion criteria for Group 1 were a clinical diagnosis of IRD, known genetic testing results and collaborative ability to undergo the complementary diagnostic exams mentioned in the parameters section.
The inclusion criteria for Group 2 were: patients similar in age and sphere equivalent (within ± 1.5D) to the study group and absence of known ocular and systemic pathology (microvascular, neurological, inflammatory, infectious, metabolic, or genetic).
Eyes with amblyopia, keratoconus, uveitis, glaucoma, or underwent prior intraocular surgeries were excluded. The following IRD diagnostic subgroups with 5 or fewer patients were excluded for more reliable analysis: Pattern dystrophy (ORPHA 63454), Best vitelliform macular dystrophy (ORPHA 1243), X-linked retinoschisis (ORPHA 792), Achromatopsia (ORPHA 49382), and Choroideremia (ORPHA 180).
Parameters
This study analysed:
-demographic characteristics of the study’s population: gender, age at the visit, and clinical diagnosis based on classification covered by the national, web-based IRD registry (IRD-PT);18
-clinical features: spherical equivalent (SE);
-dynamic corneal response second-generation parameters assessed through ultra-high-speed Scheimpflug imaging during noncontact tonometry (Corvis ST, OCULUS®): Ambrosio Relational Thickness (ARTh), Deflection Amplitude Ratio Max (DARM), Integrated Radius (IR) and Stiffness Parameter at Applanation (SP-A1);
-indexes obtained by a Scheimpflug camera (Pentacam and Corvis ST, OCULUS®): the final deviation value D of the Belin/Ambrosio Enhanced Ectasia Display (BAD-D), corvis biomechanical index (CBI) and tomographic biomechanical index (TBI)].
-anatomic features: axial length (AL) measured by a high-resolution swept-source OCT (ANTERION®) and central corneal thickness (CCT) measured by Corvis ST, OCULUS®.
Statistical Analysis
Statistical analysis was performed using the SPSS program (IBM SPSS Statistics, version 28.0.1.0 for Mac). The normality of the variables was evaluated by the Kolmogorov–Smirnov test. Descriptive statistics are shown as mean ± standard deviation. For categorical variables, descriptive statistics are presented as absolute and relative frequencies. Linear mixed-effects models, using patient identification number as a random effect to correct for the inclusion of both eyes of all participants, were used to test the differences among tomographic and biomechanical parameters between groups, adjusting for age, axial length and corneal thickness. The comparison between categorical variables was performed using the chi-square test. Spearman’s bivariate correlation test was used to study linear correlations. For interpretation, a correlation coefficient was considered “very weak” if between 0 and ±0.19, “weak” if between ±0.20 and ±0.39, “moderate” if between ±0.40 and ±0.59, “strong” if between ±0.60 and ±0.79 and “very strong” if between ±0.80 and ±1.00. To assess the discriminative ability of each parameter, we performed receiver operating characteristic (ROC) curves and calculated the area under the curve (AUC) and the ideal cutoff points. P values lower than 0.05 were considered statistically significant.
Results
Demographic Data
This study included 154 patients (308 eyes), 46.1% male and 53.9% female, aged 8 to 79 years, with a mean age of 43.9 ± 17.5 years.
Group 1 included 77 patients (154 eyes), from 77 families, 55.8% diagnosed with Non-syndromic Retinitis Pigmentosa (NS-RP) (ORPHA 791), 20.8% with Cone-rod dystrophy (CRD) (ORPHA 1872), 11.7% with Syndromic Retinitis Pigmentosa (S-RP) (ORPHA 519325) and 11.7% with Stargardt Disease (STGD) (ORPHA 827). S-RP subgroup included patients with Usher syndrome (n = 4), Bardet–Biedl syndrome (n = 2), Neuropathy, ataxia, and retinitis pigmentosa (NARP) syndrome (n=2) and Congenital disorder of glycosylation type Ia (n = 1). Disease-causing genotypes were distributed across 26 different genes. The 3 most frequently implicated genes were as follows: ABCA4 (12.9), RHO (7.8%), and EYS (5.2%). The average age was 44.0 ± 17.5 years and 54.5% were female.
Group 2 included 77 patients (154 eyes). The average age was 43.9 ± 17.5 years and 53.2% were male. There was no statistically significant difference in the comparison of age (p = 0.943), gender (p = 0.909), SE (p = 0.860), AL (p=0.880), or CCT (p = 0.156) between the groups (Table 1).
 |
Table 1 Global Characterization of the Sample |
Biomechanical Properties and Indexes
The results of the comparison study of biomechanical parameters and indexes between the group 1 (study group) and group 2 (control group) can be seen in Figure 1. Differences were seen in DARM, ARTh, CBI, TBI and BAD-D parameters (p < 0.001 for all).
 |
Figure 1 Biomechanical parameters and indexes by study groups. Values represent the 95% CI for mean. p-values are presented for comparison between groups (group 1 vs group 2). ARTh, Ambrosio Relational Thickness (horizontal 8 mm); BAD-D, the final deviation value D of the Belin/Ambrosio Enhanced Ectasia Display; CBI, corvis biomechanical index; DARM, Deflection Amplitude Ratio Max; IR, integrated radius; IRDs, Inherited Retinal Dystrophies; SP-A1, stiffness parameter at applanation 1; TBI, tomographic biomechanical index. |
The comparison of tomographic and biomechanical parameters and indexes between subtypes of IRDs and control group can be seen in Table 2.
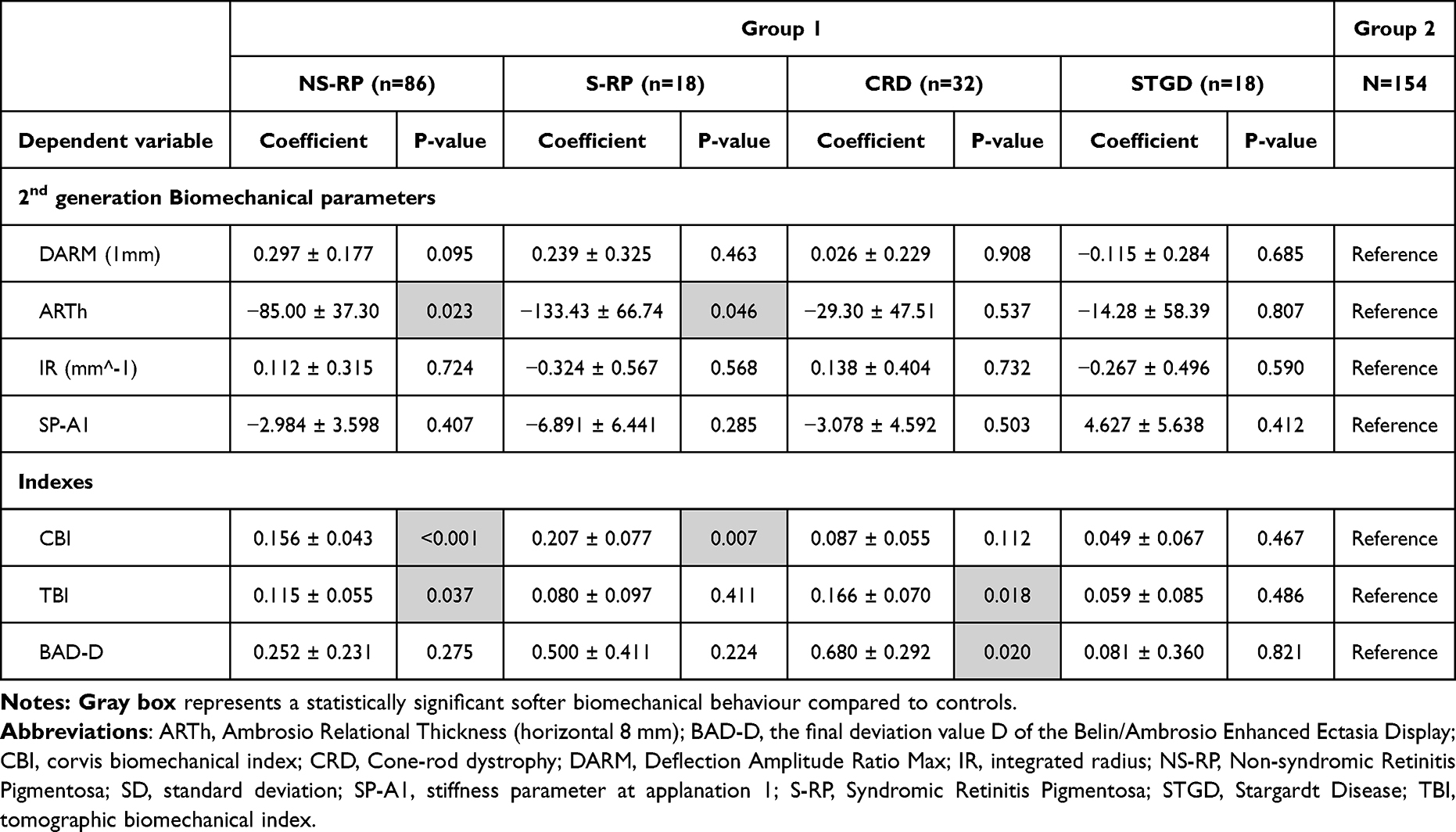 |
Table 2 Comparison of Tomographic and Biomechanical Parameters and Indexes Using Mixed-Effects Regressions Models Adjusted for Age, Axial Length and Central Corneal Thickness |
RP patients, both syndromic and non-syndromic, presented significantly lower values of ARTh (p = 0.023 for NS-RP and p = 0.046 for S-RP) and higher values of CBI (p < 0.001 for NS-RP and p = 0.007 for S-RP) compared with healthy subjects. NS-RP also had higher values of TBI (p = 0.037). CRD patients displayed higher values of TBI (p = 0.018) and BAD-D (p = 0.020) compared with healthy subjects. No differences were found for the STGD group.
Table 3 presents the performance of tomographic and biomechanical parameters studies to discriminate groups 1 and 2. CBI, TBI and BAD-D presented the highest values of specificity and AUC whereas ARTh was the most sensitive parameter.
 |
Table 3 Performance of Tomographic and Biomechanical Parameters for Discrimination of Healthy Subjects and IRD Patients |
Discussion
This pioneering study is the first to evaluate biomechanical properties for IRDs. Overall, this study found that IRD patients can have different biomechanical behaviours compared to healthy patients depending on the IRD subtype.
NS-RP and S-RP patients showed significantly softer behaviour in the same second-generation biomechanical corneal parameter (ARTh). The difference between them was in indexes. CBI was worse in both subgroups than the control group, meaning that both had biomechanical changes supporting the ectasia and glaucoma risk. However, TBI was only significantly worse in NS-RP. TBI is calculated using an artificial intelligence approach by combining tomographic data with biomechanical data to improve sensitivity and specificity in the detection of patients with risk for ectasia.19 This can mean that NS-RP patients can have a higher risk than S-RP for ectasia. We don´t know if it is related to genetic or environmental factors (such as rubbing habits) or a combination of both (neither of which were considered in the analysis in this study). It was already known that NS-RP patients may have glaucoma and corneal morphological disorders and aberrations that can affect vision.11,20,21 We found that corneal biomechanics changes may also be present and these changes can be extended to S-RP patients, although apparently in a lighter way.
CRD patients showed no significant biomechanical differences compared to the control group, but they scored worse on two indexes: BAD-D and TBI. This can mean that in this case, glaucoma risk is similar to non-IRD patients and the higher ectasia risk may be primarily attributed to tomographic changes and not biomechanics, some of which have only been previously described in isolated case reports.7,22
STGD patients showed biomechanical behaviour and tomographic indexes similar to the control group, which means an equal ectasia and glaucoma risk.
Regarding discrimination of healthy subjects and IRD patients, ARTh was the most sensitive parameter, and it could be used to screen these patients if a non-retina cause of vision loss is suspected.
One of the strengths of this study is the biomechanical assessment with an ultra-high-speed Scheimpflug camera that takes 140 horizontal 8mm frames throughout 33ms, allowing a more detailed evaluation of the deformation process compared to the Ocular Response Analyzer (ORA) (Reichert Ophthalmic Instruments, Buffalo, NY).12 Another strength is the quality of the control group used, as it presents similar age, gender and anatomical characteristics compared to the study group, namely AL, SE and CCT. These factors can influence biomechanical results.23–26 Additionally, there is no known association between atopy and these IRD types, highlighting that these results are not influenced by this factor. Furthermore, we included a wide range of ages, meaning indirectly the possibility of various stages of disease.
However, this study has some limitations. This study did not include an analysis among genotypes, as these subgroups were not sufficiently representative. This would be important to understand whether there is a genotype more susceptible to these changes. Another limitation was the inclusion of only four IRD types. While the included IRD types were among the most frequent and therefore more representative, it’s important to note the presence of a potential sample bias. Additionally, some patients were excluded because they did not have the capacity to perform exams due to syndromic characteristics (such as anatomic limitations, development delay, or intellectual development disorder), eye problems (unstable fixation as nystagmus, very low vision as light perception or hand motion) and age (child, elderly). We also did not ask patients about chronic eye-rubbing habits, which are a major risk factor for corneal changes. However, there is no known association between atopy and these IRD types as we mentioned above, and many people have eye-rubbing habits and are unaware of it, making the survey unreliable.
In the future, prospective and longitudinal studies will be necessary to validate these changes and determine if there are differences among different genotypes.
In conclusion, this study revealed that IRD patients showed statistically significant differences in biomechanical characteristics, compared to eyes without pathology, which may predispose patients to corneal ectasia or glaucoma development in some IRD subtypes. Thus, biomechanical assessment can help to identify other non-retina causes of vision loss in these patients.
Data Sharing Statement
All the data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
Institutional Review Board (IRB)/Ethics Committee approval was obtained from the Departamento de Ensino, Formação e Investigação (DEFI) of Centro Hospitalar Universitário de Santo António with reference number 2021.269 (216-DEFI/224-CE). Written informed consent was obtained from all patients.
Acknowledgments
This article was prepared with the assistance of Pedro Moniz (medical writing).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
Dr Miguel Neves reports Consultant from Alcon Portugal – Produtos e Equipamentos, Lda., outside the submitted work. The authors declare that they have no competing interests.
References
1. Ratra D, Ozdek S, Raviselvan M, Elchuri S, Sharma T. Approach to inherited retinal diseases. Indian J Ophthalmol. 2022;70(7):2305. doi:10.4103/ijo.IJO_314_22
2. Verbakel SK, van Huet RAC, Boon CJF, et al. Non-syndromic retinitis pigmentosa. Prog Retinal Eye Res. 2018;66:157–186. doi:10.1016/j.preteyeres.2018.03.005
3. Tatour Y, Ben-Yosef T. Syndromic inherited retinal diseases: genetic, clinical and diagnostic aspects. Diagnostics. 2020;10(10):779. doi:10.3390/diagnostics10100779
4. Tanna P, Strauss RW, Fujinami K, Michaelides M. Stargardt disease: clinical features, molecular genetics, animal models and therapeutic options. Br J Ophthalmol. 2017;101(1):25–30. doi:10.1136/bjophthalmol-2016-308823
5. Hamel CP. Cone rod dystrophies. Orphanet J Rare Dis. 2007;2:7. doi:10.1186/1750-1172-2-7
6. Zemba M, Zaharia AC, Dumitrescu OM. Association of retinitis pigmentosa and advanced keratoconus in siblings. Rom J Ophthalmol. 2020;64(3):313–321.
7. Fogla R, Iyer GK. Keratoconus associated with cone-rod dystrophy: a case report. Cornea. 2002;21(3):331–332. doi:10.1097/00003226-200204000-00020
8. Hung MC, Chen YY. Association between retinitis pigmentosa and an increased risk of primary angle closure glaucoma: a population-based cohort study. PLoS One. 2022;17(9):e0274066. doi:10.1371/journal.pone.0274066
9. Peng T, Wu L, Zhou W. Retinitis pigmentosa associated with glaucoma--clinical analysis. Yan Ke Xue Bao. 1990;6(1–2):17–19.
10. Leroy BP, Witters J, Laey J–JD, Kestelyn P. Progressive rod–cone dystrophy with subacute angle–closure glaucoma. Invest Ophthalmol Visual Sci. 2004;45(13):5153.
11. Zeki Fikret C, Ucgun NI, Karaca EE, Evren Kemer O. Corneal characteristics in patients with retinitis pigmentosa. Photodiagn Photodyn Ther. 2023;42:103554. doi:10.1016/j.pdpdt.2023.103554
12. Esporcatte LPG, Salomão MQ, Lopes BT, et al. Biomechanical diagnostics of the cornea. Eye Vision. 2020;7(1):9. doi:10.1186/s40662-020-0174-x
13. Zimprich L, Diedrich J, Bleeker A, Schweitzer JA. Corneal Hysteresis as a Biomarker of Glaucoma: current Insights. Clin Ophthalmol. 2020;14:2255–2264. doi:10.2147/OPTH.S236114
14. Kotecha A. What biomechanical properties of the cornea are relevant for the clinician? Surv Ophthalmol. 2007;52(Suppl 2):S109–114. doi:10.1016/j.survophthal.2007.08.004
15. Garcia-Porta N, Fernandes P, Queiros A, Salgado-Borges J, Parafita-Mato M, González-Méijome JM. Corneal biomechanical properties in different ocular conditions and new measurement techniques. Int Scholarly Res Notices. 2014;2014:e724546. doi:10.1155/2014/724546
16. Ferrara M, Lugano G, Sandinha MT, Kearns VR, Geraghty B, Steel DHW. Biomechanical properties of retina and choroid: a comprehensive review of techniques and translational relevance. Eye. 2021;35(7):1818. doi:10.1038/s41433-021-01437-w
17. Hashemi H, Heirani M, Ambrósio R, Hafezi F, Naroo SA, Khorrami-Nejad M. The link between keratoconus and posterior segment parameters: an updated, comprehensive review. Ocular Surf. 2022;23:116–122. doi:10.1016/j.jtos.2021.12.004
18. Marques JP, Carvalho AL, Henriques J, Murta JN, Saraiva J, Silva R. Design, development and deployment of a web-based interoperable registry for inherited retinal dystrophies in Portugal: the IRD-PT. Orphanet J Rare Dis. 2020;15(1):304. doi:10.1186/s13023-020-01591-6
19. Ambrósio R, Lopes BT, Faria-Correia F, et al. Integration of Scheimpflug-based corneal tomography and biomechanical assessments for enhancing ectasia detection. J Refract Surg. 2017;33(7):434–443. doi:10.3928/1081597X-20170426-02
20. Küçük B, Yıldırım Y, Özsaygılı C. Anterior chamber characteristics assessed by rotating Scheimpflug imaging in patients with retinitis pigmentosa. Arq Bras Oftalmol. 2019;82(6):507–510. doi:10.5935/0004-2749.20190096
21. Gartner S, Schlossman A. Retinitis pigmentosa associated by glaucoma*. Am J Ophthalmol. 1949;32(10):1337–1350. doi:10.1016/S0002-9394(49)91752-3
22. Kannan B. Keratoconus associated with cone-rod dystrophy. Asian J Ophthalmol. 2016;14(3):115–117. doi:10.35119/asjoo.v14i3.128
23. Liu G, Rong H, Zhang P, et al. The effect of axial length elongation on corneal biomechanical property. Front Bioeng Biotechnol. 2021;9:777239. doi:10.3389/fbioe.2021.777239
24. Qiu K, Lu X, Zhang R, Wang G, Zhang M. Corneal biomechanics determination in healthy myopic subjects. J Ophthalmol. 2016;2016:2793516. doi:10.1155/2016/2793516
25. Kenia VP, Kenia RV, Pirdankar OH. Age-related variation in corneal biomechanical parameters in healthy Indians. Indian J Ophthalmol. 2020;68(12):2921–2929. doi:10.4103/ijo.IJO_2127_19
26. Strobbe E, Cellini M, Barbaresi U, Campos EC. Influence of age and gender on corneal biomechanical properties in a healthy Italian population. Cornea. 2014;33(9):968–972. doi:10.1097/ICO.0000000000000187
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.