")
Back to Journals » Clinical Ophthalmology » Volume 18
Cost Analysis of Scleral Buckle and Pars Plana Vitrectomy for Retinal Detachment Surgery
Authors Rallo-López ÁJ , Martínez-Costa Pérez R
Received 21 June 2024
Accepted for publication 7 October 2024
Published 14 October 2024 Volume 2024:18 Pages 2891—2895
DOI https://doi.org/10.2147/OPTH.S482861
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr John Miller
Álvaro J Rallo-López,1 Rafael Martínez-Costa Pérez2
1Department of Ophthalmology, Clínica Baviera, Valencia, Spain; 2Department of Ophthalmology – Retina and Vitreous, Hospital Universitario y Politécnico La Fe, Valencia, Spain
Correspondence: Álvaro J Rallo-López, Email [email protected]
Background and Objective: To compare the cost and utility of scleral buckle (SB) and pars plana vitrectomy (PPV) techniques for repairing moderately complex rhegmatogenous retinal detachment (RRD).
Patients, Materials, and Methods: A cost-utility analysis was conducted using data from the Primary Retinal Detachment Outcomes Study (PRO) and a study conducted by the author. Total costs, patient utility over a lifetime, and cost per quality-adjusted life year (QALY) were calculated for each surgical procedure.
Results: The cost of scleral buckle surgery was € 287.93, with an estimated lifetime QALY of 7.49. Costs per QALY were € 38.44. According to the PRO study and Belin et al, total costs were $5975, with a lifetime QALY of 5.4 and costs per QALY of $1106. The cost of pars plana vitrectomy (PPV) was € 1468.26, with an estimated lifetime QALY of 6.84 and costs per QALY of € 214.65. Based on the PRO study and Belin et al, total costs were $8125, with a lifetime QALY of 4.7 and costs per QALY of $2196.
Conclusion: Repairing moderately complex RRD presents a highly cost-effective profile for both SB and PPV techniques, well below recommended QALY thresholds. SB demonstrated a slightly more favorable profile compared to PPV.
Keywords: retinal detachment, pars plana vitrectomy, scleral buckle, cost-utility analysis, QALY
Introduction
In recent years, the rise in healthcare costs has prompted the need to assess the cost-effectiveness of medical and surgical interventions, given the increase in population life expectancy.1,2 In response to these challenges, strategies to optimize resources have emerged, including the evaluation of costs per intervention, lifetime utility, and quality-adjusted life year (QALY).3
Retinal detachment repair has seen a shift in the most commonly used techniques, with pars plana vitrectomy (PPV) gaining ground over scleral buckle surgery.4–6 Nonetheless, findings from the PRO study have shown favorable outcomes for scleral buckle surgery in terms of visual function recovery and anatomical surgical success.7 These findings suggest the viability of equitable indication between both techniques, emphasizing the importance of individualized decision-making for each case to benefit the patient.
This study aims to conduct a cost-utility analysis for the treatment of moderately complex retinal detachment with macula involvement. We will compare scleral buckle surgery with pars plana vitrectomy based on the results from the PRO study and research conducted by the author, which also addresses the visual outcomes of both surgical techniques.7,8
Materials and Methods
The study comparing the visual outcomes of both surgical techniques, conducted by the author, received approval from the Ethics Committee for Drug Research at the La Fe University and Polytechnic Hospital in Valencia, Spain. This study adhered to the principles of the Helsinki Declaration. The methodology used for this study is based on the studies by Elhusseiny and Belin.9,10 Data published by the author and from the study by Belin et al, based on the PRO study, were used to calculate resource utilization, visual outcomes, and the effectiveness of surgical repair for moderately complex retinal detachment in phakic patients (Tables 1 and 2). The definition of moderate complexity can be found in the PRO study.
 |
Table 1 PRO Study Outcome Data |
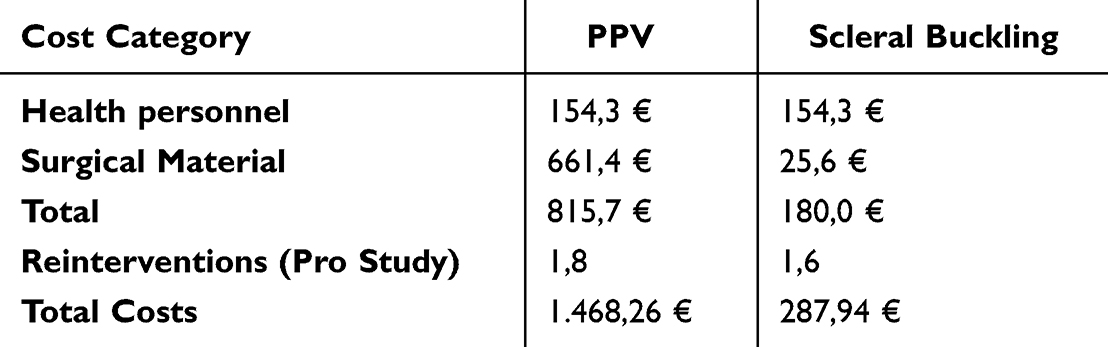 |
Table 2 Surgery Costs (Personnel, Materials, Total) |
To calculate the costs (in €) of surgical repair for both techniques in the year 2023, the costs of surgical materials and healthcare personnel in the Valencian Community (Spain) were considered,11 including the salaries of the surgeon, anesthesiologist, nursing staff, nursing assistant, and orderly (Table 3). Hospitalization costs were not applied, as the visitation regime was outpatient. The probability of reintervention due to retinal detachment recurrence (obtained from the PRO study) was also considered. The cost derived from reinterventions were considered. The technique assumed for reoperation was pars plana vitrectomy (the cost of PPV was multiplied by the surgical failure rate, multiplied by the average number of reoperations for recurrent retinal detachment). Additional costs for cataract extraction, if required, were considered (acquired from the PRO study). A discount rate of 3% per year (for intervention cost and QALY obtained) was applied for the cost-utility analysis in both groups from the second year (month 13) onwards, as proposed by Brown.12 These calculated costs were used to conduct the cost-utility analysis for each treatment (total costs, lifetime QALY, and cost per QALY).
 |
Table 3 Total Imputed Costs (in €) for RRD Repair, QALY Gained, and Cost per QALY at 12 Months |
Ophthalmic surgeries are considered not to influence life expectancy but do affect vision-related quality of life.3 Utility values from the study proposed by Brown,11 were used as a reference for both the analysis of the first (other) eye and the second (better) eye. An untreated retinal detachment is associated with a visual acuity of counting fingers, corresponding to a utility value of 0.52.10 Postoperative visual acuity in the pars plana vitrectomy group was 20/44, and in the scleral buckle group was 20/30 (PRO study). Visual acuity in the study conducted by the author was 20/32 in the PPV group and 20/40 in the scleral buckle group. Utility values proposed by Brown13 in the analysis of the first eye range from 0.87 for visual acuity ranging from counting fingers to 20/30, indicating minimal differences between non-intervention and retinal detachment surgery. However, utility gains in the analysis of the second eye can be calculated by obtaining the difference in utility for untreated counting fingers vision (0.52) and the postoperative vision obtained in the studies (ranging from 0.84 for 20/30 vision to 0.8 for 20/40 vision).
The mean age in the PRO study was 56.2 years in the scleral buckle group and 60.0 in the PPV group. The mean age in the author’s study was 56.45 in the scleral buckle group and 58.75 in the PPV group. Life expectancy was obtained from data from the Ministry of Health of Spain, which was 83.2 years.2 Lifetime QALY and cost per QALY were calculated based on the age of each group in the PRO study and the author’s study. Microsoft Excel was used for data analysis.
Results
Retinal Detachment of Moderate Complexity, Repaired with Scleral Buckling
The total cost of the intervention (on an outpatient basis), including healthcare personnel and surgical material, was €287.93. The estimated lifetime QALY was 7.49 QALYs (macula off). The costs per QALY were €38.44. Based on the PRO study and Belin et al7,10 (Table 4), the total costs were $5975. The lifetime QALY was 5.4. The costs per QALY were $1106.
 |
Table 4 Total Imputed Costs (in US Dollars) for RRD Repair, QALY Gained, and Cost per QALY at 12 Months (PRO Study, Belin et al Study) |
Retinal Detachment of Moderate Complexity, Repaired with Pars Plana Vitrectomy
The total cost of the intervention (on an outpatient basis), including healthcare personnel and surgical material, was €1468.26. The estimated lifetime QALY was 6.84 QALYs (macula off). The costs per QALY were €214.65. Based on the PRO study and Belin et al7,10 (Table 4), the total costs were $8125. The lifetime QALY was 4.7. The costs per QALY were $2196.
Discussion
Surgery for moderate difficulty retinal detachment has proven to be highly cost-effective in both surgical techniques (slightly favoring scleral buckling). Both interventions demonstrate significantly lower costs/QALY than the maximum threshold of $100,000–$150,000/QALY.14,15 Compared to the costs/QALY of other medical treatments, it has been shown to be superior to the treatment of arterial hypertension (7389$),3 dyslipidemia (77800$),3 or hemodialysis in chronic kidney disease (72476$).16 Likewise, using the second eye as a model (better eye),11 compared to other ophthalmological treatments, it is superior to surgical treatment of epiretinal membrane (4680$/QALY)17 and wet AMD treatment with intravitreal ranibizumab injections (45995$/QALY),18 which are widely used in daily ophthalmological practice.
Similar previous studies had shown a very favorable profile for scleral buckling in phakic patients, while PPV had shown to be more favorable in pseudophakic patients.19 However, these studies were based on the RRD study,20 which showed less favorable final visual acuities (20/80). Other comparative articles between pneumatic retinopexy and PPV, using similar methods, also showed highly cost-effective results, slightly favoring pneumatic retinopexy.17,21
It is important to note the limitations of our study, such as the calculation of total costs based on personnel costs from the Valencian community. Therefore, while these results may be approximate, they cannot be extrapolated exactly to the rest of Spain or Europe due to the lack of salary uniformity between regions. Another significant limitation would be the difference in age between surgical groups, being lower in the scleral buckling group, thus influencing the costs/QALY, slightly benefiting the scleral buckling group.
Conclusions
This study demonstrates that surgeries for moderate difficulty retinal detachment repair present a highly favorable cost-effectiveness profile in both surgical techniques, surpassing that of other widely used treatments in medicine. Additionally, it is well below the $100,000–$150,000/QALY threshold. Scleral buckling surgery exhibits a more favorable profile compared to PPV. These results should guide other specialists in choosing the most appropriate surgical technique in each case, considering the individual characteristics of each patient.
Abbreviations
PPV, Pars plana vitrectomy; RRD, rhegmatogenous retinal detachment; QALY, quality-adjusted life year.
Ethical Considerations
All of the methods within this study were in compliance with the declaration of Helsinki.
Acknowledgments
We would like to express our gratitude to Lorena Duart, Eva Lodeiro, and Lidia Monreal for their assistance in calculating the prices of the different surgical techniques. Special thanks to Luis Tormo for his help in data analysis.
Disclosure
The authors declare no conflicts of interest.
References
1. Hartman M, Martin AB, Benson J, Catlin A, National Health Expenditure Accounts Team. National Health Care spending in 2018: growth driven by accelerations in medicare and private insurance spending. Health Aff. 2020;39(1):8–17. doi:10.1377/hlthaff.2019.01451
2. Ministerio de Sanidad. Esperanzas de vida en España, 2021. Madrid: Ministerio de Sanidad; 2023. Spanish.
3. Brown MM, Brown GC, Lieske HB, Lieske PA. Preference-based comparative effectiveness and cost–effectiveness: a review and relevance of value-based medicine for vitreoretinal interventions. Curr Opin Ophthalmol. 2012;23(3):163–174. doi:10.1097/ICU.0b013e3283523fc1
4. McLaughlin MD, Hwang JC. Trends in vitreoretinal procedures for medicare beneficiaries, 2000 to 2014. Ophthalmology. 2017;124(5):667–673. doi:10.1016/j.ophtha.2017.01.001
5. Chong DY, Fuller DG. The declining use of scleral buckling with vitrectomy for primary retinal detachments. Arch Ophthalmol. 2010;128(9):1206–1207. doi:10.1001/archophthalmol.2010.190
6. Wong CW, Wong WL, Yeo IY, et al. Trends and factors related to outcomes for primary rhegmatogenous retinal detachment surgery in a large asian tertiary eye center. Retina. 2014;34(4):684–692. doi:10.1097/IAE.0b013e3182a48900
7. Ryan EH, Ryan CM, Forbes NJ, et al. Primary retinal detachment outcomes study report number 2: phakic retinal detachment outcomes. Ophthalmology. 2020;127(8):1077–1085. doi:10.1016/j.ophtha.2020.03.007
8. Rallo-López AJ, Martínez-Costa R, Llovet-Rausell A. Evaluación de la integridad macular, tras cirugía de desprendimiento de retina, mediante microperimetría MAIA. Archivos de la Sociedad Española de Oftalmología. 2024;99:281–287. Spanish. doi:10.1016/j.oftal.2024.04.006
9. Elhusseiny AM, Yannuzzi NA, Smiddy WE. Cost analysis of pneumatic retinopexy versus pars plana vitrectomy for rhegmatogenous retinal detachment. Ophthalmol Retina. 2019;3(11):956–961. doi:10.1016/j.oret.2019.06.003
10. Belin PJ, Yannuzzi NA, Wagley S, Smiddy WE, Ryan EH. Cost analysis of scleral buckle, pars plana vitrectomy, and pars plana vitrectomy with scleral buckle for retinal detachment repair. Retina. 2022;42(1):33–37. doi:10.1097/IAE.0000000000003298
11. Tablas retributivas del personal al servicio de las instituciones sanitarias de la Conselleria competente en materia de sanidad. Conselleria Sanitat; 2023. Spanish.
12. Brown MM, Brown GC, Sharma S, Landy J. Health care economic analyses and value-based medicine. Surv Ophthalmol. 2003;48(2):204–223. doi:10.1016/s0039-6257(02)00457-5
13. Brown GC, Brown MM, Stein JD, Smiddy WE, Ophthalmic Utility Research Study Group. Vision-related quality of life associated with unilateral and bilateral ocular conditions. Ophthalmology. 2018;125(7):965–971. doi:10.1016/j.ophtha.2017.12.033
14. Brown GC, Brown MM, Sharma S, et al. Value-based medicine and ophthalmology: an appraisal of cost-utility analyses. Trans Am Ophthalmol Soc. 2004;102:177–188.
15. Vanness DJ, Lomas J, Ahn H. A health opportunity cost threshold for cost-effectiveness analysis in the United States. Ann Internal Med. 2021;174(1):25–32. doi:10.7326/M20-1392
16. Axelrod DA, Schnitzler MA, Xiao H, et al. An economic assessment of contemporary kidney transplant practice. Am J Transplant. 2018;18(5):1168–1176. doi:10.1111/ajt.14702
17. Gupta OP, Brown GC, Brown MM. A value-based medicine cost-utility analysis of idiopathic epiretinal membrane surgery. Am J Ophthalmol. 2008;145(5):923–928. PMID: 18329000. doi:10.1016/j.ajo.2007.12.037
18. Brown GC, Brown MM, Lieske HB, Turpcu A, Rajput Y. The comparative effectiveness and cost-effectiveness of ranibizumab for neovascular macular degeneration revisited. Int J Retina Vitreous. 2017;3:5. PMID: 28289548; PMCID: PMC5304393. doi:10.1186/s40942-016-0058-3
19. Seider MI, Naseri A, Stewart JM. Cost comparison of scleral buckle versus vitrectomy for rhegmatogenous retinal detachment repair. Am J Ophthalmol. 2013;156(4):661–666. doi:10.1016/j.ajo.2013.05.019
20. Heimann H, Bartz-Schmidt KU, Bornfeld N, Weiss C, Hilgers RD, Foerster MH, Scleral Buckling versus Primary Vitrectomy in Rhegmatogenous Retinal Detachment Study Group. Scleral buckling versus primary vitrectomy in rhegmatogenous retinal detachment: a prospective randomized multicenter clinical study. Ophthalmology. 2007;114(12):2142–2154. doi:10.1016/j.ophtha.2007.09.013
21. Hillier RJ, Felfeli T, Berger AR, et al. The pneumatic retinopexy versus vitrectomy for the management of primary rhegmatogenous retinal detachment outcomes randomized trial (PIVOT). Ophthalmology. 2019;126(4):531–539. doi:10.1016/j.ophtha.2018.11.014
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.