")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 17
Cost-Benefit Analysis of Genetic Testing as a Prenatal Diagnostic Tool for Thalassemia: A Single-Center Study From Central Thailand
Authors Malasai K, Jittikoon J, Udomsinprasert W, Talungchit P , Youngkong S, Sangroongruangsri S , Mahasirimongkol S, Chaikledkaew U
Received 14 October 2024
Accepted for publication 9 January 2025
Published 4 February 2025 Volume 2025:17 Pages 33—43
DOI https://doi.org/10.2147/CEOR.S500802
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Giorgio Lorenzo Colombo
Kwandao Malasai,1,2 Jiraphun Jittikoon,3 Wanvisa Udomsinprasert,3 Pattarawalai Talungchit,4,5 Sitaporn Youngkong,5,6 Sermsiri Sangroongruangsri,6 Surakameth Mahasirimongkol,7 Usa Chaikledkaew5,6
1Social, Economic and Administrative Pharmacy (SEAP) Graduate Program, Faculty of Pharmacy, Mahidol University, Bangkok, Thailand; 2Social Pharmacy Research Unit, Faculty of Pharmacy, Mahasarakham University, Maha Sarakham, Thailand; 3Department of Biochemistry, Faculty of Pharmacy, Mahidol University, Bangkok, Thailand; 4Department of Obstetrics and Gynecology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand; 5Mahidol University Health Technology Assessment (MUHTA) Graduate Program, Mahidol University, Bangkok, Thailand; 6Social and Administrative Pharmacy Division, Department of Pharmacy, Faculty of Pharmacy, Mahidol University, Bangkok, Thailand; 7Information and Communication Technology Center, Office of the Permanent Secretary, Ministry of Public Health, Nonthaburi, Thailand
Correspondence: Usa Chaikledkaew, Social and Administrative Pharmacy Division, Department of Pharmacy, Faculty of Pharmacy, Mahidol University, 447 Sri-Ayudhaya Road, Rachathewi, Phayathai, Bangkok, 10400, Thailand, Email [email protected]
Purpose: This study aimed to evaluate the costs and benefits of genetic testing, specifically mutation analysis and prenatal diagnostic testing, for the confirmation of thalassemia in at-risk pregnancies in Thailand, providing crucial insights to inform public health policy decision-making.
Patients and Methods: We analyzed the costs and benefits of following standard screening guidelines, which included a sequence of tests such as mean corpuscular volume (MCV)/mean corpuscular hemoglobin (MCH) with dichlorophenol indophenol precipitation (DCIP), hemoglobin (Hb) typing, genetic testing, and amniocentesis. A decision-tree model was employed for this analysis. The study compared the scenarios with and without genetic testing, adopting a societal perspective that accounted for costs during pregnancy and the lifetime of a child born with thalassemia. Both one-way and probabilistic sensitivity analyses were conducted to account for uncertainties in the parameters used.
Results: The results revealed that adhering to the standard screening program with genetic testing resulted in a cost-savings of approximately 490 USD per prevented thalassemia case. Among the diagnostic methods, the specificity of the MCV/MCH with DCIP showed a higher degree of sensitivity relative to other testing methods, significantly influencing the outcomes. From a governmental perspective, with a full uptake of genetic testing, the incremental budget required was estimated to be 3.7 million USD (131 million THB) for one year.
Conclusion: These findings are particularly valuable for policymakers, as they provide robust evidence supporting potential revisions to the reimbursement structure within Thailand’s Universal Health Coverage benefit package, facilitating better management of thalassemia and improving prenatal care.
Keywords: cost-benefit analysis, genetic testing, prenatal screening, thalassemia, pregnancy
Introduction
Thalassemia represents a diverse spectrum of genetic disorders caused by the reduced synthesis of alpha or beta chains of hemoglobin (Hb), and it is inherited, meaning at least one parent must be a carrier of the disease.1 The prevalence of α-thalassemia is notably high in Asia, especially Southeast Asia, where it is estimated to affect 22.6% of the population,2 while β-thalassemia is more commonly observed in Mediterranean regions.1 In Thailand, the prevalence of α-thalassemia is approximately 20.1%,2 with β-thalassemia affecting between 3% to 9% of the population.3 Projections based on gene frequencies and annual births suggest that approximately 1.2% of newborns in Thailand will have severe thalassemia.4 Consequently, the Thai government has implemented a strategic plan for the prevention and control of thalassemia in pregnancy, aiming to reduce the incidence of this condition through early detection and intervention.5
Genetic testing serves as the definitive step in prenatal screening, facilitating the identification of couples at risk for severe thalassemia and providing them with crucial information to make informed reproductive decisions and pursue prenatal diagnosis if necessary.6 Both the National Health Service (NHS) and the American College of Obstetricians and Gynecologists recommend antenatal thalassemia screening protocols similar to those adopted in Thailand.6–8 The screening process in Thailand begins with a pregnant woman undergoing a combination of the single tube osmotic fragility (OF) test or red cell indices such as mean corpuscular volume (MCV) and mean corpuscular hemoglobin (MCH) along with dichlorophenol indophenol precipitation (DCIP) tests.8 If these initial screening results are positive, the pregnant woman’s partner is also invited to participate in the same screening tests.8 Couples who both test positive for any of the screening tests (OF, MCV, MCH, or DCIP) then proceed to hemoglobin typing (Hb typing) and/or DNA analysis. Couples identified as high-risk for having a child with severe thalassemia are advised to undergo prenatal diagnosis (PND), commonly performed via amniocentesis, to confirm the diagnosis in the fetus.8,9
The Thalassemia Prevention and Control Program, initiated by the World Health Organization (WHO), and the Ministry of Public Health of Thailand in 1992, was designed to reduce the incidence of severe thalassemia in newborns and enhance the quality of life for individuals affected by the disorder.4 In 2014, the initiative gained further support from the National Health Security Office (NHSO) through the Thalassemia Prevention and Control in Pregnancy Program.4 While thalassemia screening is included in the Universal Health Coverage (UHC) benefit package for pregnant women, comprehensive coverage for genetic testing especially for β-thalassemia remains limited across Thailand’s health insurance schemes.10 Despite a formal request from the NHSO, no economic evaluation of genetic testing for prenatal thalassemia screening has been conducted to date. This gap in knowledge limits the ability to make evidence-based decision about the potential adoption of a universal prenatal screening policy. In response, this study seeks to evaluate the cost-benefit of incorporating genetic testing into prenatal thalassemia screening in Thailand. The analysis compares scenarios that include genetic testing against those without it and estimates the budget impact assuming a 100% uptake rate for each scenario. The findings of this study aim to fill the current knowledge gap and provide critical insights for decision-makers, helping to inform potential revisions in national policies and health coverage for prenatal thalassemia screening.
Materials and Methods
Study Design
We conducted a cost-benefit analysis using a decision-analytic model to compare the costs and benefits of standard thalassemia screening program with genetic testing versus screening without genetic testing for pregnant women in Thailand. The study population included cohorts of pregnant women of all age groups, along with their at-risk spouses. Spouses underwent screening if the pregnant woman’s initial test either MCV, MCH, or DCIP yielded positive results, following the Royal Thai College of Obstetricians and Gynecologists Clinical Practice Guidelines.8 We modeled the costs and benefits during pregnancy and throughout the lifetime of individuals with thalassemia from a societal perspective. An annual discounting rate of 3% was applied to both costs and outcomes according to the Thai Health Technology Assessment Guidelines.11 Cost-benefit calculation was measured as net benefit and benefit-to-cost ratio. Net benefit (Δ benefit-Δ cost) reflects the incremental difference between the benefits and costs of the standard screening program with genetic testing versus screening without genetic testing. Benefit-to-cost ratio (Δ benefit/Δ cost) represents the efficiency of the investment in the screening program with genetic testing. Here, Δ benefit denotes the difference in benefits between the standard screening and screening without genetic testing, while Δ cost represents the difference in costs between the two approaches. Additionally, we estimated the financial implications of adopting each screening strategy by multiplying the per-person total cost from the governmental perspective by the number of 700,000 single pregnancies occurring annually in Thailand.12
Model Structure
The decision-analytic model employed in this study was derived from the Royal Thai College of Obstetricians and Gynecologists Clinical Practice Guidelines.8 To ensure the accuracy and reliability of the model, face validity was performed by three obstetricians. The model simulates two scenarios ie, standard thalassemia screening program involving genetic testing and screening without genetic testing. Figure 1 depicts decision tree model used in this study. The process starts with all pregnant women either accepting or declining MCV/MCH with DCIP screening test (Figure 1a). If they decline the screening, the pregnancy outcomes include normal newborns, miscarriage, and severe or non-severe thalassemia in newborns. If they accept the screening, results can be either positive or negative, determined by the test’s sensitivity and specificity. In the case of a negative test result, the pregnancy outcomes (normal newborns, miscarriage, or thalassemia) are monitored. For a positive test result, the at-risk husband is then offered MCV/MCH with DCIP screening to determine whether both partners are carriers of thalassemia (Figure 1b). If both are positive, the couple is then offered a Hb typing test to confirm their carrier status (Figure 1c). If the Hb typing test is positive, genetic resting for either α-thalassemia, β-thalassemia or both is then offered to the pregnant woman (Figure 1d). In contrast, pregnant women in the scenario of screening without genetic testing would proceed directly to a final diagnosis to assess whether they have babies with thalassemia or not (Figure 1e). If a final diagnosis is needed, the pregnant woman is offered amniocentesis, which has the following outcomes: procedure-related loss, such as miscarriage due to the test, true or false positives, and true of false negatives, depending on the test’s sensitivity and specificity. If the pregnant woman declines the amniocentesis, the outcomes are spontaneous abortion or live birth with either severe thalassemia, non-severe thalassemia, or a normal newborn.
 |
Figure 1 (a) Overall decision-tree model, (b) Decision-tree model for at-risk husbands screened by MCV/MCH with DCIP (S2), (c) Decision-tree model for couple screened by Hb typing (S3), (d) Decision-tree model for pregnant women screened by genetic testing (S4) (e) Decision-tree model for pregnant women diagnosed by amniocentesis (S5). |
Model Parameters
The input parameters manipulated in the model were categorized into four groups, as follows: epidemiological data and probabilities, screening performance, cost, and benefit. The values of these parameters are detailed in Table 1.
 |
Table 1 Input Parameters Used in the Model |
Epidemiological Data and Probabilities
We obtained epidemiological data on the disease and probabilities for screening and uptake rates from a previous study which collected data from a retrospective chart review of 4,062 pregnancies in Siriraj hospital database from January 2019 to December 2019.13 The ethics of this study was approved by Siriraj Institutional Review Board (SIRB) (MU-MOU COA Si 1053/2020) and the ethics committee waived the requirement for informed consent. All methods were carried out in accordance with International Guidelines for Human Research Protection such as the Declaration of Helsinki, Belmont Report, CIOMS Guidelines and International Conference on Harmonization in Good Clinical Practice (ICH-GCP). Additionally, this study utilized data from published studies focusing on the outcomes of prenatal thalassemia screening in Thailand.9,20 The calculations were performed using a formula derived from an economic evaluation of disease screening,21 where the probability of a positive test is defined as (sensitivity × prevalence) + [(1-specificity) × (1-prevalence)]. Here, prevalence is the number of cases that tested positive on the screening divided by the total number of cases screened, while sensitivity and specificity represent the performance of the screening test.
Screening Performance
We used sensitivity and specificity data from a previous study which retrieved data from Siriraj hospital database13 and published studies.19
Cost
The resource utilization costs in this study were evaluated from a societal perspective, encompassing direct medical costs, direct non-medical costs, and indirect costs adjusted to 2023 values using the consumer price index (CPI). Subsequently, costs were converted from Thai baht (THB) to USD at an exchange rate of 35.37 THB per 1 USD (2023 prices). All future costs and health outcomes were discounted to their present values at a rate of 3% per annum. Direct medical costs, including those associated with prenatal screening and diagnostic tests, ultrasound examinations, medical services related to procedure-related loss, delivery procedures (elective termination, normal labor, cesarean section), and service care for termination of pregnancy or miscarriage, were derived from price lists of governmental and hospital databases.13,14 The ratio of total cesarean sections to the number of normal deliveries was 54:46.13
Direct non-medical costs comprised travel, food, and opportunity costs of pregnant women and caregivers during the screening test, sourced from general hospital data on the Standard Cost List for Health Technology Assessment (HTA), a recognized reference cost list in Thailand.15 Indirect costs reflected productivity losses due to miscarriage resulting from definitive diagnosis or termination of a non-thalassemia case, calculated using a human capital approach.19 Productivity loss or income loss was estimated by multiplying the working age range by the Thai Gross Domestic Product (GDP) per capita per year (6,908.8 USD).22 The working age range was assumed to be 45 years (15–60 years). Following the recommendation from Thai HTA guidelines, considering different cost values over time, future values of total expected productivity loss (FV) were adjusted to present values (PV) using an annual discount rate of 3% based on the formula: PV = FV × [1/(1+r)n], where PV = present value, FV = future value, r = discount rate, and n = each year in the future.11 Additionally, we assumed an annual income growth rate of 4%, derived from the income growth rate during 1990–2023 in Thailand.23 Furthermore, productivity loss due to a decrease in working capacity in β-thalassemia was obtained from a published study by Riewpaiboon et al.17
Benefit
We utilized direct benefit data as a measure of cost avoidance achieved by averting the occurrence of severe thalassemia types α and β, including non-severe thalassemia in children resulting from each screening. This benefit data was derived from a previous study,13 which involved determining the average total healthcare costs of patients with severe thalassemia type β and non-severe thalassemia. Concurrently, the costs of treating patients with severe thalassemia type α were obtained from a previous study utilizing governmental databases.18 Moreover, we estimated indirect benefits in terms of productivity gains for caregivers who were not required to care for children with severe thalassemia due to the prenatal screening test. The human capital approach was employed by multiplying the average expected survival of severe thalassemia patients with the expected income of caregivers, referencing the annual Thai GDP per capita (6,908.8 USD).16 We assumed a one-year survival for fetuses with severe thalassemia type α and a 30-year survival for those with severe thalassemia type β, based on expert opinions and a published study by Dhanya et al.24 For caregivers of children with severe thalassemia type β, the future values of total expected productivity gain were adjusted to their present values using a discount rate of 3%11 and an income growth rate of 4% per year.23
Uncertainty Analysis
We conducted both one-way and probabilistic sensitivity analyses (PSA) to assess the model’s sensitivity to each input parameter. One-way sensitivity analysis involved varying each input parameter within its 95% confidence interval (CI), and the resulting range of net benefit values was presented using a Tornado diagram. Furthermore, we simultaneously evaluated the uncertainty of all parameters through a 1,000 Monte Carlo simulation. Probabilities were assigned a beta distribution, performances followed a log-normal distribution, and cost and benefit parameters adhered to a gamma distribution. The PSA results were depicted as a cost-benefit plane.
Results
Cost-Benefit Analysis
The decision-analytical model employed in this study simulated a scenario wherein pregnant women and at-risk husbands underwent tests for screening without genetic testing, as well as a standard screening program with genetic testing throughout the pregnancy and over the lifetime of a thalassemia-affected newborn. Table 2 presents the estimated total costs, benefits, net benefit, and the benefit-to-cost (B/C) ratio. From a societal perspective, the analysis revealed that the implementation of a standard thalassemia screening program with genetic testing resulted in a net benefit of 490 USD compared to screening without genetic testing. Consequently, a cost saving was observed with the adoption of the standard thalassemia screening program with genetic testing.
 |
Table 2 Cost-Benefit Analysis Results (USD) |
Uncertainty Analysis
The results of the one-way sensitivity analysis for the standard thalassemia screening program with genetic testing are illustrated in Figure 2. The net benefit was the most sensitivity to the specificity of the MCV/MCH with DCIP test, with subsequent sensitivity observed in the cost avoidance of non-severe thalassemia, the acceptance rate of MCV/MCH+DCIP in pregnant women, the probability of a positive test result for MCV/MCH+DCIP in pregnant women, and the discount rate for outcomes. Figure 3 portrays the outcomes derived from the PSA. The cost-benefit plane revealed that the majority of simulations were situated in the northeast quadrant.
 |
Figure 2 Tornado diagram for the standard thalassemia screening program with genetic testing. Abbreviations: MCV, mean corpuscular volume; MCH, mean corpuscular hemoglobin; DCIP, dichlorophenol indophenol precipitation; Hb, hemoglobin. |
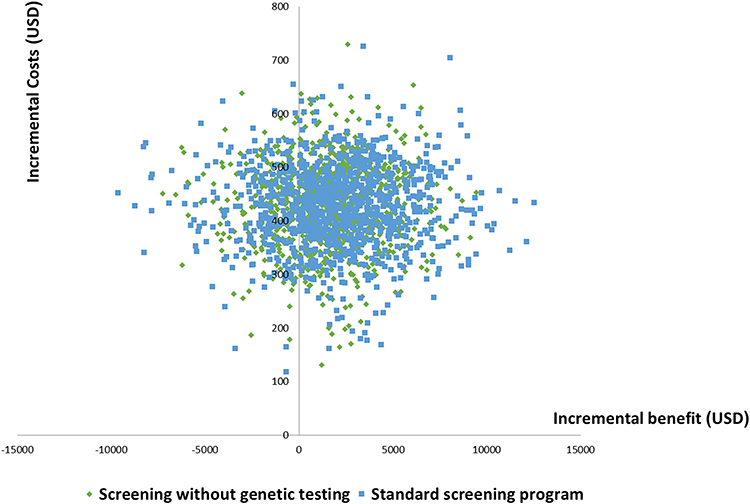 |
Figure 3 Cost-benefit plane. Green diamonds represent the cost and benefit outcomes of screening without genetic testing, while blue squares represent those of standard screening with genetic testing. |
Budget Impact Analysis
Table 3 provides insight into the budgetary impact of each screening test from the governmental perspective over the course of one year. The incremental budget, amounting to approximately 3,703,457 USD (130,991,266 THB) was incurred for the standard thalassemia screening program with genetic testing, assuming a 100% uptake rate.
 |
Table 3 Budget Impact Analysis of Each Screening Test With a 100% Uptake Rate |
Discussion
This study represents the first comprehensive evaluation of the cost-benefit of genetic testing for prenatal thalassemia screening in comparison to screening without genetic testing among Thai pregnant women and at-risk husbands suspected of carrying thalassemia in Thailand. The findings indicated that the standard thalassemia screening program with genetic testing was more cost-saving than screening without genetic testing. Moreover, results from the PSA suggested that while the costs were comparable, genetic testing proved more beneficial than screening without genetic testing. Our finding was consistent with several previous cost-benefit and cost-effectiveness analysis studies, which suggested that thalassemia screening program in pregnancy was more cost-saving than no screening.25–28 Consequently, genetic testing for β-thalassemia is currently fully reimbursed in Thailand’s health benefit packages.29
While all tests in the prenatal thalassemia screening strategy are provided free of charge, the uptake rate for each screening test was notably low, particularly in the case of test acceptance among husbands during the initial screening, registering at only 27.9%.13 This low acceptance rate has implications for the potential loss of identifying suspected husbands who may be carriers of thalassemia, increasing the risk of having offspring with thalassemia. Additionally, accessibility to screen for Hb typing and genetic testing was limited across general hospitals, tertiary hospitals, and university hospitals. The survey conducted across 95 hospitals in Thailand revealed that Hb typing was available in 67.4% of the facilities, while genetic testing was accessible in only 24.2%.23
Although the Royal Thai College of Obstetricians and Gynecologists has established clinical guidelines for prenatal screening and diagnosis in pregnant women, variations in strategies exist among different hospitals.23,30 The approach adopted depends on the prevalence of thalassemia in each region of Thailand, including the Northeast. In this context, pregnant women and their husbands decide to undergo simultaneous screening of MCV and MCH with DCIP initially, given the high prevalence of Hb E in the Northeast of Thailand.4,23 Furthermore, certain university hospitals opt for screening Hb typing instead of DCIP to streamline the process, reduce waiting times, and enhance test acceptance among at-risk husbands.30 This screening approach bears similarities to the thalassemia screening in Australia and the carrier screening for thalassemia and hemoglobinopathies in Canada.31,32
Despite the significant findings presented herein, it is imperative to acknowledge several limitations. Firstly, the uptake rate for screening and epidemiological data was derived solely from one hospital located in the central region of Thailand, characterized by a low to medium prevalence of thalassemia. As a result, our analysis may underestimate the potential benefits associated with identifying new thalassemia cases. Secondly, the intangible benefit of pregnant women’s willingness to pay for screening was not taken into consideration, this omission may underestimate the overall benefit of screening, leaving room for future studies to explore this aspect further. Lastly, the current study revealed that the percentage of screening genetic testing for both α- and β-thalassemia was 100%, higher than the prevalence of either genetic testing for α- or β-thalassemia in Thailand in 2019, which stood at 28–87%.9 Therefore, this would result in an overestimation of the budget impact.
Conclusion
This study provided supportive evidence that from a societal perspective, genetic testing, when incorporated into the prenatal thalassemia screening strategy, was more cost-beneficial than screening without genetic testing for pregnant women and at-risk husbands with suspected thalassemia carriers in Thailand, offering long-term benefits that outweighed the costs to society as a whole. The estimated annual budget impact of screening with a 100% uptake rate during pregnancy amounted to 3.7 million USD (131 million THB). Our research contributes valuable insights that may guide policymakers advocating for the incorporation of genetic testing for β-thalassemia into Thailand’s UHC benefit package, aligning with the WHO and Thailand’s operational strategy to prevent and control new thalassemia cases. Further investigations should be undertaken to assess the inclusion of various prevalence rates in determining the most value-centric strategy in future studies.
Ethics Approval
Our study used data from previous published studies. The ethics of this study was approved by Siriraj Institutional Review Board (SIRB) (MU-MOU COA Si 1053/2020). The need for informed consent for this study was waived by the ethics committees, as all data were obtained from published studies. All methods were carried out in accordance with International Guidelines for Human Research Protection such as the Declaration of Helsinki, Belmont Report, CIOMS Guidelines and International Conference on Harmonization in Good Clinical Practice (ICH-GCP). All procedures performed in the study were in compliance with international guidelines for human research protection such as Declaration of Helsinki, the Belmont Report.
Acknowledgment
The authors express their gratitude to the Social Economic and Administrative Pharmacy (SEAP) Graduate Program at Mahidol University for their support in facilitating the research facility. This research project has been funded by Mahidol University (Fundamental Fund: fiscal year 2024 by National Science Research and Innovation Fund (NSRF). It is noteworthy that the funder played no role in the analysis, interpretation of results, drawing conclusions, or the preparation of the manuscript. The first author extends appreciation to Mahasarakham University for granting the Ph.D. scholarship. The authors gratefully acknowledge Assoc. Prof. Panutsaya Tientadakul, Head of the Department of Clinical Pathology, Faculty of Medicine Siriraj Hospital, Mahidol University for kind support for data collection in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hamza B, Hajira BT. Available from: https://www.ncbi.nlm.nih.gov/books/NBK545151/.
2. Goh LPW, Chong ETJ, Lee PC. Prevalence of alpha(alpha)-Thalassemia in Southeast Asia (2010-2020): a meta-analysis involving 83,674 subjects. Int J Environ Res Public Health. 2020;17(20):7354. doi:10.3390/ijerph17207354
3. Chaibunruang A, Sornkayasit K, Chewasateanchai M, Sanugul P, Fucharoen G, Fucharoen S. Prevalence of Thalassemia among newborns: a re-visited after 20 years of a prevention and control program in Northeast Thailand. Mediterr J Hematol Infect Dis. 2018;10(1). doi:10.4084/MJHID.2018.054
4. Paiboonsukwong K, Jopang Y, Winichagoon P, Fucharoen S. Thalassemia in Thailand. Hemoglobin. 2022;46(1):53–57. doi:10.1080/03630269.2022.2025824
5. Fucharoen S, Winichagoon P. Thalassemia in Southeast Asia: problems and strategy for prevention and control. Southeast Asian J Trop Med Public Health. 1992;23(4):647–655.
6. ACOG Committee on Obstetrics. ACOG practice bulletin no. 78: hemoglobinopathies in pregnancy. Obstet Gynecol. 2007;100(1):229–237.
7. National Health Support Service. Antenatal haemoglobinopathy screening programme. Available from: https://www.pnsd.scot.nhs.uk/wp-content//2015-Antenatal-Haemoglobinopathy-Protocols-version-1.pdf.
8. The Royal Thai College of Obstetricians and Gynecologists. RTCOG clinical practice guideline prenatal screening and diagnosis of Thalassemia.
9. Health Intervention and Technology Assessment Program. An evaluation of thalassemia prevention and control in pregnancy program. Available from: https://www.hitap.net/documents/174625.
10. National Health Security Office. National health security fund management handbook. Available from: https://www.nhso.go.th/storage/files/shares/PDF/fund_man01.pdf.
11. HTA Guidelines Development Working Group. Guideline for health technology assessment in Thailand updated edition: 2019.
12. Office of the National Economic and Social Development Council. Birth rate 1993–2019. Available from: https://social.nesdc.go.th/SocialStat/StatReport_Final.aspx?reportid=68&template=2R1C&yeartype=M&subcatid=1.
13. Chaikledkaew U, Jittikoon J, Udomsinprasert W, et al. Economic evaluation of genetic testings for thalassemia carrier diagnosis among married couple in Thailand. Available from: https://kb.hsri.or.th/dspace/handle/11228/5752?locale-attribute=th.
14. Drug and Medical Supply Information Center. Public health service rates handbook for units under the ministry of public health. Available from: https://dmsic.moph.go.th/index/detail/8026.
15. Riewpaiboon A. Standard cost lists for health economic evaluation in Thailand. J Med Assoc Thai. 2014;97(Suppl 5):S127–34.
16. The World Bank. Thai gross domestic product per capita. Available from: https://data.worldbank.org/indicator/NY.GDP.%20PCAP.CD?locations=TH.
17. Riewpaiboon A, Nuchprayoon I, Torcharus K, Indaratna K, Thavorncharoensap M, Ubol BO. Economic burden of beta-thalassemia/Hb E and beta-thalassemia major in Thai children. BMC Res Notes. 2010;3(1):29. doi:10.1186/1756-0500-3-29
18. Medical Affairs Division DoMS, Ministry of Public Health. Guidelines for the care of thalassemia patients in general practice. Available from: https://www.biogenetech.co.th/wp-content/uploads/2018/01/Guidelines-for-thalassemia-care.pdf.
19. Nillakupt K, Nathalang O, Arnutti P, et al. Prevalence and hematological parameters of thalassemia in Tha Kradarn subdistrict Chachoengsao Province, Thailand. J Med Assoc Thai. 2012;95 Suppl 5:S124-32.
20. Laoarayawat T, Bamrungsawad N, Dilokthornsakul P, Wong P, Upakdee N. Cost-effectiveness analysis of prenatal screening program for Thalassemia between semi-accelerated screening step and current program. Rama Med J. 2020;43(1):13–23. doi:10.33165/rmj.2020.43.1.227046
21. Praditsitthikorn N. Economic evaluation of screening for disease. J Med Assoc Thai. 2014;97(Suppl 5):S94–101.
22. Marques N, Gerlier L, Ramos M, et al. Patient and caregiver productivity loss and indirect costs associated with cardiovascular events in Portugal. Rev Port Cardiol. 2021;40(2):109–115. doi:10.1016/j.repc.2020.05.019
23. The World Bank. Thai GDP growth (annual %). Available from: https://data.worldbank.org/indicator/NY.GDP.%20MKTP.KD.ZG?locations=TH.
24. Dhanya R, Sedai A, Ankita K, et al. Life expectancy and risk factors for early death in patients with severe thalassemia syndromes in South India. Blood Advances. 2020;4(7):1448–1457. Blood Adv. doi:10.1182/bloodadvances.2019000760.
25. Koren A, Profeta L, Zalman L, et al. Prevention of beta Thalassemia in Northern Israel - a cost-benefit analysis. Mediterr J Hematol Infect Dis. 2014;6(1):e2014012. doi:10.4084/MJHID.2014.012
26. Ahmadnezhad E, Sepehrvand N, Jahani FF, et al. Evaluation and cost analysis of national health policy of thalassaemia screening in west-Azerbaijan province of Iran. Int J Prev Med. 2012;3(10):687–692.
27. Ratanasiri T, Charoenthong C, Komwilaisak R, et al. Prenatal prevention for severe thalassemia disease at Srinagarind hospital. J Med Assoc Thai. 2006;89(Suppl 4):S87–93.
28. Ginsberg G, Tulchinsky T, Filon D, Goldfarb A, Abramov L, Rachmilevitz EA. Cost-benefit analysis of a national thalassaemia prevention programme in Israel. J Med Screen. 1998;5(3):120–126. doi:10.1136/jms.5.3.120
29. National Health Security Office. Management of health promotion and disease prevention services fiscal year. 2023. Available from: http://www.sshos.go.th/wp-content/uploads/2022/09/PP-Fee-shedule_66.pdf.
30. Department of Obstetrics and Gynaecology Siriraj hospital. Screening of Thalassemia in pregnancy.
31. Bowden DK. Screening for thalassaemia. Austr Prescr. 2001;24(5):120–123.
32. Genetics Committee of the Society of Obstetricians and Gynaecologists of Canada (SOGC). Carrier screening for thalassemia and hemoglobinopathies in Canada. J Obstet Gynaecol Can. 2008;30(10):950–959. doi:10.1016/S1701-2163(16)32975-9
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.