")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 17
Cost-Effectiveness of a Community First Responder System for Out-of-Hospital Cardiac Arrest in Poland
Authors Jaskuła J , Medic G , Verma S, Maurer J, Kooy TA , Greef BD
Received 18 December 2024
Accepted for publication 15 April 2025
Published 2 May 2025 Volume 2025:17 Pages 375—386
DOI https://doi.org/10.2147/CEOR.S510907
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Giorgio Lorenzo Colombo
Jerzy Jaskuła,1 Goran Medic,2 Sanjay Verma,2 Joachim Maurer,3 Tom A Kooy,4 Bianca de Greef2
1Department of Medical Education, Centre for Innovative Medical Education, Jagiellonian University Medical College, Krakow, Poland; 2Chief Medical Office – Health Economics and Outcome Research, Philips, Amsterdam, Netherlands; 3Connected Care – Emergency Care, Philips, Amsterdam, Netherlands; 4Research Department, Stan BV, Udenhout, Netherlands
Correspondence: Goran Medic, Email [email protected]
Objective: Out-of-Hospital Cardiac Arrest (OHCA) is a significant public health issue in Poland, with only an 8.4% survival rate to hospital discharge. Early initiation of Basic Life Support and defibrillation through a Community First Responder (CFR) system can markedly improve survival rates and neurological outcomes.
Methods: A decision tree and Markov model compared the cost-effectiveness of three scenarios against standard care by estimating costs and quality-adjusted life years (QALYs). Scenario 1 involved raising public awareness and educating on the 30:2 CPR protocol. Scenario 2 added equipping blue-light service vehicles with Automated External Defibrillators (AEDs) and training personnel. Scenario 3 implemented a full CFR system with integrated AEDs, dispatch centers, and trained citizen responders. The analysis included survival to hospital discharge, with sensitivity analyses assessing robustness.
Results: The incremental cost-effectiveness ratios (ICERs) were € 15,221 for Scenario 1, € 30,659 for Scenario 2, and € 16,205 for Scenario 3 per QALY gained—all below the threshold of € 50,197. Improvements were observed in all stages, including survival to hospital discharge and neurologically intact survival. Probabilistic sensitivity analyses confirmed the robustness of the results.
Conclusion: Implementing a CFR system in Poland is a cost-effective strategy that enhances survival rates after OHCA at an acceptable cost per QALY. The study emphasizes the importance of AED accessibility, trained CFRs, and streamlined emergency responses to improve survival and quality of life for OHCA patients. These findings support policy development and resource allocation to strengthen Poland’s emergency medical response to OHCA.
Keywords: out-of-hospital cardiac arrest, community first responder, automated external defibrillator, cost-effectiveness, defibrillation
Introduction
Out-of-hospital cardiac arrest (OHCA) is a leading cause of death in Europe and the US, with significant mortality rates.1 Polish studies report OHCA incidence rates of 34.7–156 per 100,000 annually,2–8 consistent with the EuReCa TWO study across 28 European countries.9 In Europe, 275,000 cases occur annually,10 with only 8.5% surviving to hospital discharge and 8.4% in Poland.9 The prognosis for OHCA patients in Poland remains poor, with an overall survival rate of 2% to 11%, varying by region.11 This highlights the need for effective interventions to improve OHCA outcomes.
Many OHCA cases are of cardiac origin,12 predominantly caused by ventricular fibrillation, requiring early defibrillation and a robust chain of survival.13 Rapid emergency medical services (EMS) response and timely intervention, including cardiopulmonary resuscitation (CPR) and automated external defibrillator (AED) use, are crucial for improving outcomes.14
AEDs, both static and mobile, are crucial for early defibrillation, greatly improving survival chances.15 Despite proven benefits16–18 and recommendations to place AEDs in public places, their use during OHCA remains low.19–22 As of October 2024, Poland had AEDs installed at 8,659 locations,23 with many sites hosting multiple devices. Public AED use has been increasing since 2016.24
Time is crucial, as delayed perfusion leads to continual cell death; with each passing second, the possibility of a good outcome decreases.25 Community First Responder (CFR) System, designed to supplement EMS and reduce time to defibrillation, have gained support.26,27 CFR systems can improve survival rates and neurological outcomes, enhancing public health and emergency response.28 However, their implementation requires careful evaluation due to significant logistical and financial challenges.29
In optimal cases, such as witnessed sudden cardiac arrest (SCA) with a shockable rhythm and early defibrillation, return of spontaneous circulation (ROSC) is achieved in 30% to 40% of cases.4,30 AED use significantly increases ROSC rates, especially when applied early in CPR.31,32 Despite this, improvements in bystander CPR and AED use are needed.33 Only 25% of EMS-treated patients are transported to the hospital, and less than 30% of hospitalized patients survive to discharge.33 The presence of a trained EMS professional as a witness notably improves CPR initiation rates.34
This study evaluates the cost-effectiveness of a 3-scenario approach to implement a CFR system for witnessed OHCA incidents in Poland. By comparing the costs and benefits of an optimized CFR system to the current standard of care (SoC), this research offers insights to support decision-making and policy development for EMS in Poland.
Methods
A cost-effectiveness analysis was performed using a decision tree and long-term Markov model. The model compared the costs and quality-adjusted life years (QALYs) of three scenarios with the existing SoC. The structure of the model is shown in Figure 1.
 |
Figure 1 Schematic view of the Decision tree and Markov model. Abbreviations: ED, emergency department; OHCA, out-of-hospital cardiac arrest. |
Setting
Poland has a population of 37,562,000 inhabitants,35 with 32,991 experiencing OHCAs annually,36 managed by 23 emergency dispatch centers.37 Based on EuReCa TWO study showing a mean OHCA patient age of 65 years,9 this age was selected as the starting point for our model.
Currently, OHCA management in Poland involves two main strategies (Figure 1): the intervention strategy, which deploys first responders like firefighters, police officers, and citizen responders for immediate care, and the comparator strategy, which relies on EMS or nearby bystanders until paramedics arrive. Both aim for timely intervention, but differ in roles and effectiveness, forming the basis for comparing OHCA outcomes.
The Ethics/Institutional approval is not applicable.
Overview of the Polish EMS
The Polish EMS system comprises three main components: 1) medical dispatch centers where paramedics and nurses handle calls; 2) EMS teams (ground, air, and water), mostly staffed by paramedics, sometimes with nurses or doctors; and 3) emergency departments.4 Upon receiving an emergency call, emergency medical dispatchers assign a priority code: C1 represents the highest priority, requiring an ambulance to depart within 60 seconds using emergency lights and sirens, while C2 represents the second-highest priority, with the ambulance needing to leave within 120 seconds.4
Survival rates, presented in Table 1, are derived from various publications.9,38,39 The model’s target population consists of all OHCA patients for whom EMSs attempt resuscitation, excluding cases with clear signs of death.
 |
Table 1 Clinical and Cost Inputs |
Scenarios
Scenario 1 initiates a broad public awareness campaign using various media to educate people about OHCA and essential emergency responses.
Scenario 2 equips emergency vehicles (EV), police, firefighters, and rescue services, with AEDs.
Scenario 3 focuses on implementing a CFR system to improve pre-hospital care for OHCA patients.
The base case comparator is the current SoC, characterized by uncoordinated AED access, existing emergency services, and limited first responder coverage in certain areas. The three implementation scenarios were selected to provide a stepwise and adaptable approach to improving OHCA outcomes in Poland, recognizing that full CFR system implementation may require significant resources and that these scenarios can be implemented in phases, with each phase providing incremental benefits. Details of all scenarios are in the Supplementary Material.
Estimated Effect
The projected impact of three scenarios was based on data from the Amsterdam Resuscitation Study (ARREST)40 and other Dutch initiatives. Detailed clinical estimates (Table 1), are derived from Dutch programs like the HartslagNu Foundation and the Netherlands Heart Foundation, with more information available in the Supplementary Material (Supplementary Table 1 and Supplementary Figure 1). Cost estimates are adjusted to Polish setting (Table 1).
Resources
Drawing on the experience from the Netherlands,40 it is estimated that 1.75% of the population would need to be recruited as CFRs, amounting to 659,715 Polish individuals. We assume that half of these CFRs will have a professional background (eg, healthcare professionals, medical doctors, firefighters, etc.) and therefore will not require additional training in CPR and AED usage. Of the remaining half, it is anticipated that 80% will need to undergo training. Of the remaining half, 80% are expected to undergo training, resulting in 263,886 CFRs being trained in Scenario 3.
Outcomes
The analysis evaluated a number of key stages of survival, including following:
- Survival to the Emergency Department.
- Survival to Hospital Admission.
- Survival to Discharge.
- Neurologically Intact Survival: This evaluates patients’ neurological status upon discharge, specifically looking at those who are neurologically intact, categorized as having a cerebral performance category (CPC) of 1 or 2.52
All survival rates were calculated based on the previous stage.
Other Data Inputs
Other data inputs, such as transition probabilities for the Markov component of the model, QALY data, and costs associated with both the decision tree and Markov model, are summarized in Table 2.
 |
Table 2 Other Clinical and Costs Inputs |
Model Structure
A decision tree model was selected to capture event-driven processes over short timeframes, mapping patient pathways from cardiac arrest to hospital discharge or death. A two-state Markov model will also be used to assess long-term outcomes, including life years, quality of life, and treatment costs for OHCA survivors. This combined approach offers a comprehensive evaluation of the CFR system’s impact.
The official Polish cost-effectiveness willingness-to-pay (WTP) threshold is set at €50,197.55 The Markov model, with a 15-year horizon and annual cycles, incorporates Polish life tables56 and clinical survival data. Costs and benefits will be discounted at 5% and 3.5%, respectively, per Polish guidelines.57 A similar model and analysis were performed in a different setting in Belgium.58
Sensitivity Analyses
A univariate one-way deterministic sensitivity analysis (OWSA) and probabilistic sensitivity analysis (PSA) were performed to assess the robustness and uncertainty of the model. In OWSA, individual parameters were varied by ±10% while keeping others constant to identify their impact on results. PSA used Monte Carlo simulation to sample 1,000 values from predefined distributions, introducing real-world variability and providing a broader view of parameter uncertainty. Together, these analyses offer insights into the reliability of the model’s findings.
Results
The awareness campaign and implementation of the CFR system resulted in incremental cost-effectiveness ratio (ICER) of €15,221, €30,659 and €16,205 per QALY gained for scenarios 1, 2 and 3, respectively, over a 15-year time horizon, with half-cycle corrections (Table 3). All three values are significantly below the Polish WTP threshold of €50,197.55 The analyses demonstrated improvements across all stages, including survival to hospital discharge and neurologically intact survival, CPC 1 and CPC2.
 |
Table 3 Summary of results for All Three Scenarios, With Half-Cycle Correction (15-year Time Horizon) |
Comparable results were obtained for all scenarios, even without half-cycle corrections (Supplementary Table 2), indicating the outcomes are robust. The half-cycle correction, typically used in Markov models to account for mid-cycle events, had minimal impact on the effectiveness and cost-effectiveness, confirming the reliability of the findings across different modelling methods.
Results of OWSA for three scenarios are presented in Figure 2.
 |
Figure 2 One-way sensitivity analyses – Scenarios 1, 2 and 3 with half-cycle corrections. Abbreviations: AED, Automated External Defibrillators; CPC, cerebral performance category; ED, emergency department; ICER, Incremental Cost-Effectiveness Ratio. |
Figure 3 illustrates the cost-effectiveness planes generated from the PSAs, revealing a strong positive correlation between costs and effects.
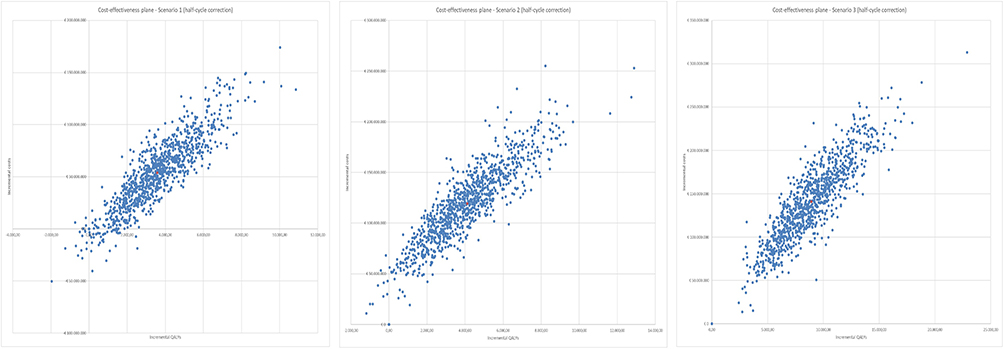 |
Figure 3 Cost-effectiveness planes – Scenarios 1, 2 and 3 with half-cycle corrections. Abbreviation: QALY, Quality-adjusted life year. |
Additionally, the cost-effectiveness acceptability curves in Supplementary Figure 2 demonstrate that all three scenarios have a 100% probability of being cost-effective in Poland, at the current WTP threshold of €50,197.55
Discussion
The present study is of critical importance in the light of the growing emphasis on optimizing healthcare spending and the necessity to focus on interventions that deliver the most substantial health benefits for the general population. Notably, this analysis is the first of its kind conducted in Poland, marking a significant contribution to the field. The findings from this cost-effectiveness model demonstrate that survival outcomes can be notably improved through a comprehensive awareness campaign (Scenario 1), equipping EVs with AEDs (Scenario 2) and the implementation of a CFR system (Scenario 3). The ICERs are €15,221, €30,659 and €16,205 per QALY gained for scenarios 1, 2 and 3, respectively, over a 15-year time horizon with half-cycle corrections applied. The 15-year time horizon was selected based on the average age of OHCA patients (approximately 65 years) and the limitations of the WHO life tables for Poland, which cap mortality at age 85.56 Supporting this decision, a recent systematic literature review and meta-analysis by Amacher et al (2022) also used a 15-year maximum follow-up and reported 15-year survival rates of 57.5% after OHCA.59 Recognizing that OHCA patients often have reduced survival compared to the general population, this horizon realistically captures their expected survival period. While acknowledging that a 15-year horizon might slightly underestimate the intervention’s long-term impact, this conservative approach was intentionally adopted to provide a cautious and realistic evaluation.
Starting with Scenario 1 can significantly improve survival outcomes even before fully implementing CFR systems (Scenario 3). This initial phase, involving fewer stakeholders, provides important benefits and sets the stage for broader implementation. Discrepancies between our findings and other studies3,34), especially in bystander responses, may result from differences in demographics, CPR training,34 public awareness,34 regional protocols, cultural factors, or trust in healthcare systems. Although our study provides valuable economic insights, it highlights the importance of expanding health education to improve bystander CPR and public awareness to improve outcomes in emergency situations.34
Cost-effectiveness studies on AEDs fall into two categories: those focused on public AED deployment53,60–65 and those evaluating AEDs within a CFR system.3,66–70
Studies on AED placement focus on cost-effectiveness in high-traffic areas, aligning with our findings on health benefits and QALYs.34,53,60–65 However, they often overlook the potential of CFR systems to improve survival and cost-efficiency, highlighting the need for detailed analysis and strategic planning to optimize health outcomes in Polish emergency response.
The second category of studies integrating AEDs into CFR systems consistently show significant increases in pre-EMS CPR and defibrillation rates (from 4.2% to 10.3%).66–70 For example, Siddiqui et al in Singapore reported that CFRs improved community OHCA responses, with alerts received increasing from 62% to 96% and 50% of responders arriving on scene.66 Similarly, Starck et al69 in Denmark and Baumgarten et al68 in rural Germany confirmed that CFRs enhance early intervention during OHCAs.
Our study differs from previous studies by evaluating the economic implications of CFR systems, addressing a gap in previous research that focused mainly on survival outcomes. We provide a framework assessing both cost and survival benefits, offering policymakers a valuable tool. Our results align with studies highlighting the cost-effectiveness of AED deployment when combined with CFR networks and public awareness efforts. Both study categories agree on the clinical benefits of AEDs, whether through strategic placement or as part of comprehensive emergency response systems. Bednarz et al34 supported a community-based approach, emphasizing public training and strategic AED deployment to maximize OHCA survival, echoing our findings.
The cost-effectiveness model has limitations due to its reliance on Dutch data, which may not fully generalize to regions with different infrastructures and demographics. Poland’s EMS system is transitioning to predominantly paramedic-based teams, with only 18% now including doctors; only helicopter EMS teams require physicians. Some countries, like France and the Netherlands, have implemented SMS systems to notify volunteers about cardiac arrests and nearby AEDs.71,72 The model does not account for post-intervention care, though early intervention remains crucial, and assumes a median age of 65, which may not represent all age groups. It also overlooks staggered costs among stakeholders, assuming simultaneous expenses. The random distribution of AEDs may limit their impact; geographic information system-based analysis, as suggested by Buter et al (2024), could prioritize high-risk areas.65 With an estimated 10,000 AEDs in Poland, inconsistent mapping methods exist due to the lack of legal regulation. Gradual AED rollout may delay effectiveness, emphasizing the need for coordinated integration with the CFR system. Estimating costs for in-hospital mortality and post-discharge care is challenging due to recent payment system changes; thus, the model assumes previous unit costs. While the assumption that 50% of EVs could be equipped with AEDs is realistic due to two-thirds of police officers serving in prevention departments (like patrol and traffic units), expecting this to happen within a year is overly optimistic. The process will likely take 3 to 5 years, necessitating a careful assessment of equipment needs before the AED program is implemented. It is impractical to train all emergency staff simultaneously, as the associated costs and efforts would need to be distributed over several years. While socioeconomic factors affecting bystander CPR were not the focus of this study, previous research shows disparities disadvantaging resource-limited communities.34 Socioeconomic factors play a crucial role in shaping both bystander CPR rates and EMS response times, particularly in the context of urban-rural differences. In Poland, as in many other countries, these disparities can lead to significant variations in emergency response effectiveness, with rural areas often experiencing longer EMS response times and lower rates of bystander CPR intervention. Research has consistently shown that individuals in lower-income or rural communities are less likely to receive bystander CPR due to lower CPR training rates,73–79 limited awareness,73–79 and reduced availability of AEDs.80,81 Additionally, EMS response times tend to be longer in rural areas due to greater geographic distances82 and fewer available resources,80,81 which can negatively impact survival outcomes for OHCA patients.80–82 EMS arrival times for OHCA are 8 minutes in cities up to 10,000 inhabitants and 15 minutes in smaller towns and villages.83 Poland’s 250,000 volunteer firefighters, mainly in rural areas, together with the country’s one million healthcare and emergency personnel, could help address response time disparities in the CFR program and improve survival outcomes for OHCA events. The latest Polish data show that EMS recognized 36,314 OHCA events, 80% (29,046) of which occurred at home.84 While our model does not explicitly stratify outcomes based on socioeconomic factors, we recognize that these disparities can influence both the effectiveness and accessibility of OHCA interventions. Addressing socioeconomic disparities in OHCA outcomes requires targeted strategies such as expanding CPR training, improving AED accessibility in rural areas, optimizing EMS resource allocation, and leveraging mobile technology, while future research should explore tailored interventions to enhance equity in emergency response. A further limitation comes from the absence of age-stratified Polish OHCA survival data, which necessitated the use of aggregated extrapolated estimates using Dutch data from Blom et al 2014.40
Recognizing these limitations highlights the importance of a comprehensive evaluation of the entire treatment pathway for cost-effectiveness. As emphasized in the recently published systematic literature review by Werner et al 2024, there is a critical need for high-quality, nationally representative studies to effectively assess both survival outcomes and associated costs.85
In light of the evidence presented, we suggest that Polish health authorities consider the adoption of a national strategy for OHCA management that incorporates the key elements of the CFR system. This strategy should include provisions for sustainable funding mechanisms to support CFR training, AED procurement and maintenance, and the necessary technological infrastructure for efficient dispatch and coordination of CFRs. By considering and implementing these recommendations, Poland can significantly enhance its capacity to respond to OHCA events, ultimately saving lives and reducing the long-term burden of OHCA on individuals, families, and the healthcare system.
In summary, the success of public-access defibrillation programs depends on strategically placing AEDs, equipping EVs, raising public awareness, and implementing a CFR system. The first responder system for OHCA can be easily expanded to address other life-threatening emergencies in medicine without incurring additional costs. Without these focused efforts, AEDs might be poorly located, reducing their cost-effectiveness. This study provides a compelling call to action for policymakers to prioritize and invest in evidence-based interventions for OHCA.
Conclusions
The enhancement of the CFR system in Poland represents a cost-effective approach to improving survival rates following OHCA, delivering favorable outcomes at a reasonable cost per QALY. This study underscores the importance of accessible AEDs, the role of CFRs, and a streamlined emergency response system in increasing survival rates and enhancing the quality of life for OHCA patients. The findings offer valuable insights for informing policy development and resource allocation aimed at strengthening Polish emergency medical response infrastructure for OHCA, ensuring the efficacy and economic viability of life-saving interventions. Additionally, this approach may serve as a useful model for other regions seeking to optimize their emergency response systems.
Funding
There is no funding to report.
Disclosure
Jerzy Jaskuła, an employee of the Jagiellonian University Medical College, Poland, was also paid for his consultancy services by Philips. Bianca de Greef, Sanjay Verma, Goran Medic, Joachim Maurer are the employees of Philips. Tom Kooy is the employee of Stan BV, Research Department in the Netherlands. The authors report no other conflicts of interest in relation to this work.
This paper is available as a preprint on SSRN at: https://dx.doi.org/10.2139/ssrn.5001906
References
1. Roger VL, Go AS, Lloyd-Jones DM, et al. Executive summary: heart disease and stroke statistics--2012 update: a report from the American Heart Association. Circulation. 2012;125(1):188–197. doi:10.1161/CIR.0b013e3182456d46
2. Szczerbinski S, Ratajczak J, Lach P, et al. Epidemiology and chronobiology of out-of-hospital cardiac arrest in a subpopulation of southern Poland: a two-year observation. Cardiol J. 2020;27(1):16–24. doi:10.5603/CJ.a2018.0025
3. Sielski J, Kaziród-Wolski K, Solnica M, Rychlik WA, Mizia-Stec K, Sadowski M. Out‑of‑hospital cardiac arrest registry: preliminary results from the Świętokrzyskie Province. Kardiol Pol. 2019;77(7–8):710–712. doi:10.5603/KP.a2019.0047
4. Nadolny K, Zyśko D, Obremska M, et al. Analysis of out-of-hospital cardiac arrest in Poland in a 1-year period: data from the POL-OHCA registry. Kardiol Pol. 2020;78(5):404–411. doi:10.33963/KP.15241
5. Nadolny K, Szarpak L, Gotlib J, et al. An analysis of the relationship between the applied medical rescue actions and the return of spontaneous circulation in adults with out-of-hospital sudden cardiac arrest. Medicine. 2018;97(30):e11607. doi:10.1097/MD.0000000000011607
6. Rudner R, Jalowiecki P, Karpel E, Dziurdzik P, Alberski B, Kawecki P. Survival after out-of-hospital cardiac arrests in Katowice (Poland): outcome report according to the “Utstein style”. Resuscitation. 2004;61(3):315–325. doi:10.1016/j.resuscitation.2004.01.020
7. Gach D, Nowak JU, Krzych Ł J. Epidemiology of out-of-hospital cardiac arrest in the Bielsko-Biala district: a 12-month analysis. Kardiol Pol. 2016;74(10):1180–1187. doi:10.5603/KP.a2016.0086
8. Rebes K, Cebula G, Mydlowska A, Andres J. The efficacy of cardiopulmonary resuscitation, in a large city, based on Krakow’s Emergency Medical Service. Folia Med Cracov. 2017;57(4):107–116.
9. Gräsner JT, Wnent J, Herlitz J, et al. Survival after out-of-hospital cardiac arrest in Europe - Results of the EuReCa TWO study. Resuscitation. 2020;148:218–226. doi:10.1016/j.resuscitation.2019.12.042
10. Randjelovic SS, Nikolovski SS, Tijanic JZ, et al. Out-of-hospital cardiac arrest prospective epidemiology monitoring during the first five years of EuReCa program implementation in Serbia. Prehosp Disaster Med. 2023;38(1):1–8. doi:10.1017/S1049023X22002424
11. Berdowski J, Berg RA, Tijssen JG, Koster RW. Global incidences of out-of-hospital cardiac arrest and survival rates: systematic review of 67 prospective studies. Resuscitation. 2010;81(11):1479–1487. doi:10.1016/j.resuscitation.2010.08.006
12. Fröhlich GM, Lyon RM, Sasson C, et al. Out-of-hospital cardiac arrest -optimal management. Curr Cardiol Rev. 2013;9(4):316–324. doi:10.2174/1573403X10666140214121152
13. AHA. Out-of-hospital Chain of Survival. Available from: https://cpr.heart.org/en/resources/cpr-facts-and-stats/out-of-hospital-chain-of-survival.
14. Kristiansson M, Andersson Hagiwara M, Svensson L, et al. Drones can be used to provide dispatch centres with on-site photos before arrival of EMS in time critical incidents. Resuscitation. 2024;202:110312. doi:10.1016/j.resuscitation.2024.110312
15. Elhussain MO, Ahmed FK, Mustafa NM, et al. The role of automated external defibrillator use in the out-of-hospital cardiac arrest survival rate and outcome: a systematic review. Cureus. 2023;15(10):e47721. doi:10.7759/cureus.47721
16. Ringh M, Jonsson M, Nordberg P, et al. Survival after public access defibrillation in Stockholm, Sweden--A striking success. Resuscitation. 2015;91:1–7. doi:10.1016/j.resuscitation.2015.02.032
17. Nishi T, Takei Y, Kamikura T, Ohta K, Hashimoto M, Inaba H. Improper bystander-performed basic life support in cardiac arrests managed with public automated external defibrillators. Am J Emerg Med. 2015;33(1):43–49. doi:10.1016/j.ajem.2014.10.018
18. Mitani Y, Ohta K, Yodoya N, et al. Public access defibrillation improved the outcome after out-of-hospital cardiac arrest in school-age children: a nationwide, population-based, Utstein registry study in Japan. Europace. 2013;15(9):1259–1266. doi:10.1093/europace/eut053
19. Rea TD, Olsufka M, Bemis B, et al. A population-based investigation of public access defibrillation: role of emergency medical services care. Resuscitation. 2010;81(2):163–167. doi:10.1016/j.resuscitation.2009.10.025
20. Culley LL, Rea TD, Murray JA, et al. Public access defibrillation in out-of-hospital cardiac arrest: a community-based study. Circulation. 2004;109(15):1859–1863. doi:10.1161/01.CIR.0000124721.83385.B2
21. Hawkes C, Booth S, Ji C, et al. Epidemiology and outcomes from out-of-hospital cardiac arrests in England. Resuscitation. 2017;110:133–140. doi:10.1016/j.resuscitation.2016.10.030
22. Deakin CD, Shewry E, Gray HH. Public access defibrillation remains out of reach for most victims of out-of-hospital sudden cardiac arrest. Heart. 2014;100(8):619–623. doi:10.1136/heartjnl-2013-305030
23. Reanimator_app. Reanimator Community mobile app. 2024. Available from https://play.google.com/store/apps/details?id=pl.zosprp.reanimator.community&hl=pl.
24. Ślęzak D, Robakowska M, Żuratyński P, Krzyżanowski K. Network of automated external defibrillators in Poland before the SARS-CoV-2 pandemic: an in-depth analysis. Int J Environ Res Public Health. 2022;19(15):9065. doi:10.3390/ijerph19159065
25. Lancet T, The_Lancet. Editorial: out-of-hospital cardiac arrest: a unique medical emergency. Lancet. 2018;391(10124):911. doi:10.1016/S0140-6736(18)30552-X
26. Masterson S, Robinson E, Wright P, Dowling J, Murphy A. Community cardiac first responders in Ireland. Resuscitation. 2013;84(Suppl 1):S33. doi:10.1016/j.resuscitation.2013.08.096
27. Healthcare_Commission, Healthcare Commission. The role and management of community first responders. 2007. Available from: https://glostext.gloucestershire.gov.uk/Data/Joint%20Great%20Western%20Ambulance%20Overview%20and%20Scrutiny%20Committee/20080418/Agenda/Community%20First%20Responders.pdf.
28. Simmons KM, McIsaac SM, Ohle R. Impact of community-based interventions on out-of-hospital cardiac arrest outcomes: a systematic review and meta-analysis. Sci Rep. 2023;13(1):10231. doi:10.1038/s41598-023-35735-y
29. Folke F, Andelius L, Gregers MT, Hansen CM. Activation of citizen responders to out-of-hospital cardiac arrest. Curr Opin Crit Care. 2021;27(3):209–215. doi:10.1097/MCC.0000000000000818
30. Cebula GM, Osadnik S, Wysocki M, et al. Comparison of the early effects of out-of-hospital resuscitation in selected urban and rural areas in Poland. A preliminary report from the Polish cardiac arrest registry by the Polish resuscitation council. Kardiol Pol. 2016;74(4):356–361. doi:10.5603/KP.a2016.0001
31. Grunau B, Reynolds J, Scheuermeyer F, et al. Relationship between time-to-ROSC and survival in out-of-hospital cardiac arrest ECPR candidates: when is the best time to consider transport to hospital? Prehosp Emerg Care. 2016;20(5):615–622. doi:10.3109/10903127.2016.1149652
32. Reynolds JC, Grunau BE, Elmer J, et al. Prevalence, natural history, and time-dependent outcomes of a multi-center North American cohort of out-of-hospital cardiac arrest extracorporeal CPR candidates. Resuscitation. 2017;117:24–31. doi:10.1016/j.resuscitation.2017.05.024
33. Bujak K, Nadolny K, Ładny JR, et al. Epidemiology, management, and survival rate of out-of-hospital cardiac arrest in Upper Silesia, Poland: an Utstein-style report. Postepy Kardiol Interwencyjnej. 2021;17(4):366–375. doi:10.5114/aic.2021.111926
34. Bednarz K, Goniewicz K, Al-Wathinani AM, Goniewicz M. Emergency medicine perspectives: the importance of bystanders and their impact on on-site resuscitation measures and immediate outcomes of out-of-hospital cardiac arrest. J Clin Med. 2023;12(21):6815. doi:10.3390/jcm12216815
35. StatisticsPoland. Statistics Poland - Basic data. 2024. Available from: https://stat.gov.pl/en/basic-data/.
36. Narodowy Fundusz Zdrowia. National Health Fund reporting data, Republic of Poland. Letter, case number NFZ-DAMJiOS.660.26.2023 2023.362470.ELPI, national health fund, department of analysis, quality monitoring and healthcare services. 2022. Available from: https://www.nfz.gov.pl.
37. Ministry of Health. State emergency medical services command support system (SWD PRM). 2024. Available from: https://www.gov.pl/web/zdrowie/system-wspomagania-dowodzenia-panstwowego-ratownictwa-medycznego-swd-prm-.
38. Genbrugge C, De Deyne C, Eertmans W, et al. Cerebral saturation in cardiac arrest patients measured with near-infrared technology during pre-hospital advanced life support. Results from Copernicus I cohort study. Resuscitation. 2018;129:107–113. doi:10.1016/j.resuscitation.2018.03.031
39. de Longueville D, Magali B, Stefano M, et al. P088 Survival after out-of-hospital cardiac arrest in Belgium - 5 years of experience of the Belgian’s Cardiac arrest registry B-CAR. Resuscitation. 2022;175:S67–S68. doi:10.1016/S0300-9572(22)00498-1
40. Blom MT, Beesems SG, Homma PC, et al. Improved survival after out-of-hospital cardiac arrest and use of automated external defibrillators. Circulation. 2014;130(21):1868–1875. doi:10.1161/CIRCULATIONAHA.114.010905
41. Pijls RW, Nelemans PJ, Rahel BM, Gorgels AP. A text message alert system for trained volunteers improves out-of-hospital cardiac arrest survival. Resuscitation. 2016;105:182–187. doi:10.1016/j.resuscitation.2016.06.006
42. Polish_police. 2024. Available from: https://info.policja.pl/inf/wyposazenie/radiowozy/48644,Policyjne-radiowozy-i-inne-pojazdy.html.
43. Firestation. Polish fire web-portal “Firestation”. 2024. Available from: https://remiza.com.pl/dzien-strazaka-panstwowa-i-ochotnicza-straz-pozarna-w-liczbach/.
44. Jaskula J, Stolarz-Skrzypek K, Jaskuła K. Estimate by Jerzy Jaskula based on the conversion rates of the number of city guards and service vehicles in Warsaw and Krakow, Poland. Adv Med Sci. 2024;70:51–56. doi:10.1016/j.advms.2024.12.002
45. Statistics_Poland. Statistics Poland, Emergency rescue services activity in 2023 report, Estimate by Jaskula Jerzy. There are 118 water rescue organizations. We can assume that they have 2-10 vehicles (cars, boats, etc.) each. For calculations we used 5 vehicles per organization. 2023. Available from: https://stat.gov.pl/en/topics/health/health/emergency-rescue-services-activity-in-2023,14,7.html.
46. GOPR. Mountain Volunteer Rescue Service (GOPR). 2024. Available from: https://www.gopr.pl/gopr/o-gopr.
47. Polish_police. 2024. Available from: https://www.policja.pl/pol/aktualnosci/183752,Liczba-policjantow-w-polskiej-Policji-fakty.html.
48. National Headquarters of the State Fire Service of Poland (KG PSP). Annual bulletin of the State Fire Service for the year 2022, 2024. Available from: https://www.gov.pl/web/kgpsp/biuletyny-informacyjne-psp-roczne. [
49. Polish fire web-portal “Firestation”. 2024. Available from: https://remiza.com.pl/dzien-strazaka-panstwowa-i-ochotnicza-straz-pozarna-w-liczbach/.
50. Ministry of the Interior and Administration. Republic of Poland. 2024. Available from: https://archiwum.mswia.gov.pl/pl/bezpieczenstwo/straze-gminne-miejskie/dane-statystyczne-doty/16193,Dane-statystyczne-za-2016-rok.html.
51. CSO. Emergency service operations in 2023. Report of the Central Statistical Office. 2023.
52. Ajam K, Gold LS, Beck SS, Damon S, Phelps R, Rea TD. Reliability of the cerebral performance category to classify neurological status among survivors of ventricular fibrillation arrest: a cohort study. Scand J Trauma Resusc Emerg Med. 2011;19:38.
53. Moran PS, Teljeur C, Masterson S, O’Neill M, Harrington P, Ryan M. Cost-effectiveness of a national public access defibrillation programme. Resuscitation. 2015;91:48–55. doi:10.1016/j.resuscitation.2015.03.017
54. Moulaert VR, Goossens M, Heijnders IL, Verbunt JA, Heugten CM. Early neurologically focused follow-up after cardiac arrest is cost-effective: a trial-based economic evaluation. Resuscitation. 2016;106:30–36. doi:10.1016/j.resuscitation.2016.06.015
55. AHTAPOL. Komunikat Prezesa AOTMiT w sprawie obowiązującej wysokości progu kosztu uzyskania dodatkowego roku życia skorygowanego o jakość. 2024. Available from: https://www.aotm.gov.pl/aktualnosci/najnowsze/komunikat-prezesa-aotmit-w-sprawie-obowiazujacej-wysokosci-progu-kosztu-uzyskania-dodatkowego-roku-zycia-skorygowanego-o-jakosc/.
56. WHO. Life tables - Poland. 2024. Available from: https://apps.who.int/gho/data/view.searo.LT62160?lang=en.
57. Agency for Health Technology Assessment and Tariff System in Poland. Health Technology Assessment v3.0. 2016. Available from: https://www.aotm.gov.pl/wp-content/uploads/2020/07/20160913_Wytyczne_AOTMiT-1.pdf.
58. de Greef B, Genbrugge C, Verma S, et al. Cost-effectiveness of a community first responder system for out-of-hospital cardiac arrest in Belgium. Open Heart. 2025;12(1):e003098. doi:10.1136/openhrt-2024-003098
59. Amacher SA, Bohren C, Blatter R, et al. Long-term survival after out-of-hospital cardiac arrest: a systematic review and meta-analysis. JAMA Cardiol. 2022;7(6):633–643. doi:10.1001/jamacardio.2022.0795
60. Nichol G, Valenzuela T, Roe D, Clark L, Huszti E, Wells GA. Cost effectiveness of defibrillation by targeted responders in public settings. Circulation. 2003;108(6):697–703. doi:10.1161/01.CIR.0000084545.65645.28
61. Walker A, Sirel JM, Marsden AK, Cobbe SM, Pell JP. Cost effectiveness and cost utility model of public place defibrillators in improving survival after prehospital cardiopulmonary arrest. BMJ. 2003;327(7427):1316. doi:10.1136/bmj.327.7427.1316
62. Folke F, Lippert FK, Nielsen SL, et al. Location of cardiac arrest in a city center: strategic placement of automated external defibrillators in public locations. Circulation. 2009;120(6):510–517. doi:10.1161/CIRCULATIONAHA.108.843755
63. Cram P, Vijan S, Fendrick AM. Cost-effectiveness of automated external defibrillator deployment in selected public locations. J Gen Intern Med. 2003;18(9):745–754. doi:10.1046/j.1525-1497.2003.21139.x
64. Shaker MS, Abrams EM, Oppenheimer J, et al. Estimation of health and economic benefits of a small automatic external defibrillator for rapid treatment of sudden cardiac arrest (SMART): a cost-effectiveness analysis. Front Cardiovasc Med. 2022;9:771679. doi:10.3389/fcvm.2022.771679
65. Buter R, van Schuppen H, Stieglis R, Koffijberg H, Demirtas D. Increasing cost-effectiveness of AEDs using algorithms to optimise location. Resuscitation. 2024;201:110300. doi:10.1016/j.resuscitation.2024.110300
66. Siddiqui FJ, Fook-Chong S, Shahidah N, et al. Technology activated community first responders in Singapore: real-world care delivery & outcome trends. Resusc Plus. 2023;16:100486. doi:10.1016/j.resplu.2023.100486
67. Barry T, Doheny MC, Masterson S, et al. Community first responders for out-of-hospital cardiac arrest in adults and children. Cochrane Database Syst Rev. 2019;7(7):Cd012764. doi:10.1002/14651858.CD012764.pub2
68. Baumgarten MC, Röper J, Hahnenkamp K, Thies KC. Drones delivering automated external defibrillators-Integrating unmanned aerial systems into the chain of survival: a simulation study in rural Germany. Resuscitation. 2022;172:139–145. doi:10.1016/j.resuscitation.2021.12.025
69. Starck SM, Jensen JJ, Sarkisian L, Schakow H, Andersen C, Henriksen FL. The association between the experience of lay responders and response interval to medical emergencies in a rural area: an observational study. BMC Emerg Med. 2023;23(1):46. doi:10.1186/s12873-023-00803-z
70. Matinrad N, Reuter-Oppermann M. A review on initiatives for the management of daily medical emergencies prior to the arrival of emergency medical services. Cent Eur J Oper Res. 2022;30(1):251–302.
71. Smith CM, Wilson MH, Ghorbangholi A, et al. The use of trained volunteers in the response to out-of-hospital cardiac arrest - the GoodSAM experience. Resuscitation. 2017;121:123–126. doi:10.1016/j.resuscitation.2017.10.020
72. Zijlstra JA, Stieglis R, Riedijk F, Smeekes M, van der Worp WE, Koster RW. Local lay rescuers with AEDs, alerted by text messages, contribute to early defibrillation in a Dutch out-of-hospital cardiac arrest dispatch system. Resuscitation. 2014;85(11):1444–1449. doi:10.1016/j.resuscitation.2014.07.020
73. Lee S, Ahn KO, Cha MI. Community-level socioeconomic status and outcomes of patients with out-of-hospital cardiac arrest: a systematic review and meta analysis. Medicine. 2021;100(3):e24170. doi:10.1097/MD.0000000000024170
74. Lee SY, Song KJ, Shin SD, et al. A disparity in outcomes of out-of-hospital cardiac arrest by community socioeconomic status: a ten-year observational study. Resuscitation. 2018;126:130–136. doi:10.1016/j.resuscitation.2018.02.025
75. Sasson C, Magid DJ, Chan P, et al. Association of neighborhood characteristics with bystander-initiated CPR. N Engl J Med. 2012;367(17):1607–1615. doi:10.1056/NEJMoa1110700
76. Moncur L, Ainsborough N, Ghose R, Kendal SP, Salvatori M, Wright J. Does the level of socioeconomic deprivation at the location of cardiac arrest in an English region influence the likelihood of receiving bystander-initiated cardiopulmonary resuscitation? Emerg Med J. 2016;33(2):105–108. doi:10.1136/emermed-2015-204643
77. Dahan B, Jabre P, Karam N, et al. Impact of neighbourhood socio-economic status on bystander cardiopulmonary resuscitation in Paris. Resuscitation. 2017;110:107–113. doi:10.1016/j.resuscitation.2016.10.028
78. Sasson C, Haukoos JS, Bond C, et al. Barriers and facilitators to learning and performing cardiopulmonary resuscitation in neighborhoods with low bystander cardiopulmonary resuscitation prevalence and high rates of cardiac arrest in Columbus. OH Circ Cardiovasc Qual Outcomes. 2013;6(5):550–558. doi:10.1161/CIRCOUTCOMES.111.000097
79. Grubic N, Hill B, Allan KS, et al. Mediators of the association between socioeconomic status and survival after out-of-hospital cardiac arrest. Systemat Rev Can J Cardiol. 2024;40(6):1088–1101. doi:10.1016/j.cjca.2024.01.002
80. Brown TP, Perkins GD, Smith CM, Deakin CD, Fothergill R. Are there disparities in the location of automated external defibrillators in England? Resuscitation. 2022;170:28–35. doi:10.1016/j.resuscitation.2021.10.037
81. Dicker B, Garrett N, Wong S, et al. Relationship between socioeconomic factors, distribution of public access defibrillators and incidence of out-of-hospital cardiac arrest. Resuscitation. 2019;138:53–58. doi:10.1016/j.resuscitation.2019.02.022
82. Connolly MS, Goldstein Pcp JP, Currie M, et al. Urban-rural differences in cardiac arrest outcomes: a retrospective population-based cohort study. CJC Open. 2022;4(4):383–389. doi:10.1016/j.cjco.2021.12.010
83. Sejmu K. Act on State Emergency Medical Service System, 2024. Available from: https://isap.sejm.gov.pl/isap.Nsf/DocDetails.xsp?id=WDU20240000652.
84. NMC. National Monitoring Center for Emergency Medical Services (Data for 2023); 2024.
85. Werner K, Hirner S, Offorjebe OA, et al. A systematic review of cost-effectiveness of treating out of hospital cardiac arrest and the implications for resource-limited health systems. Int J Emerg Med. 2024;17(1):151. doi:10.1186/s12245-024-00727-w
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.