")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 17
Cost-Effectiveness of Oral Nutritional Supplements in Malnourished or at Risk of Disease-Related Malnutrition Cancer Patients in North Macedonia
Authors Kapedanovska Nestorovska A , Sterjev Z
Received 1 December 2024
Accepted for publication 8 March 2025
Published 26 March 2025 Volume 2025:17 Pages 265—276
DOI https://doi.org/10.2147/CEOR.S504094
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Giorgio Lorenzo Colombo
Aleksandra Kapedanovska Nestorovska, Zoran Sterjev
Center for Medication Therapy Management, Faculty of Pharmacy, Ss. Cyril and Methodius University in Skopje, Skopje, Republic of North Macedonia
Correspondence: Aleksandra Kapedanovska Nestorovska, Center for Medication Therapy Management, Faculty of Pharmacy, Ss. Cyril and Methodius University in Skopje, Skopje, Republic of North Macedonia, Tel +389 72 228 998, Email [email protected]
Purpose: This study aimed to assess the cost-effectiveness of medical nutritional support in a cancer care program in North Macedonia, comparing specialized oral nutritional supplements (ONS) with the standard of care (SOC) in managing disease-related malnutrition (DRM) in patients with or at risk of tumor cachexia syndrome.
Methods: A previously published decision tree model was employed to evaluate the economic impact of supportive treatment in cancer patients eligible for ONS. Monthly transition probabilities between health states, length of hospital stay for each treatment strategy, and utility parameters were derived from the literature. For base-case analysis, the cancer care program duration was set at 30 days. The analysis was conducted from the perspective of a national health insurance fund, utilizing a 13-year time horizon with monthly cycles. Only direct supportive care costs, estimated from publicly available data, were considered. Quality-adjusted life-years (QALYs) gained per patient and associated costs were calculated, with outcomes and costs discounted at 3.0% annually. One-way and probabilistic sensitivity analyses were performed to assess results robustness.
Results: In the base case analysis, ONS was the dominant treatment strategy, with total costs per patient of € 2605.01 for ONS versus € 3759.23 for SOC, indicating a significant cost reduction. Reduced hospitalization expenses outweighed the higher acquisition costs of ONS. Additionally, ONS provided greater health benefits, achieving 8.21 QALY vs 7.91QALY in the SOC group. The resulting Incremental Cost-Effectiveness Ratio (ICER) was negative, reinforcing ONS as the dominant strategy. Sensitivity analyses confirmed that the cost-effectiveness was primarily driven by cancer program duration, with cost-saving benefits up to 132 days.
Conclusion: Our findings demonstrate that specialized ONS is a cost-effective treatment option within a cancer care program compared with SOC. While this study focuses on North Macedonia, the results are applicable to countries with similar economic and healthcare structures, reinforcing ONS as a valuable intervention across comparable healthcare systems.
Plain Language Summary: Approximately 50% of patients with advanced cancer present with cachexia syndrome, a severe form of disease-related malnutrition (DRM). Medical nutrition is a specialized category of nutrition that addresses specific dietary needs and deficiencies. Early nutritional interventions with specialized oral nutritional supplements (ONSs) have demonstrated the ability to alleviate the negative effects of cancer and its treatments on nutritional status.
Assessing the economic impact of specialized ONSs is essential for managing chronic diseases such as cancer, which creates considerable financial challenges. Evidence of economic implications is limited and differs across healthcare settings, intervention types, and patient demographics.
This study aimed to provide decision-makers in the Republic of North Macedonia with supportive evidence on the relative and incremental cost-effectiveness of ONS in managing patients with cancer who are malnourished or at risk of severe DRM. Our findings indicate that the cost-effectiveness of early ONS intervention is primarily driven by the duration of the cancer care program, with cost-saving benefits observed within the 30-day base-case scenario and up to 132 days in sensitivity analysis. Beyond this period, ONS remained cost-effective within the willingness-to-pay threshold. This supports reimbursement decisions for addressing malnutrition in this vulnerable patient group, helping to maximize health benefits within constrained budgets.
Keywords: health economics, medical nutrition, tumor cachexia, reimbursement, cancer care program
Introduction
Disease-related malnutrition (DRM) implies insufficient nutrition (malnutrition) caused by changes in the body’s metabolism due to acute or chronic diseases and/or treatment interventions, which increases the daily nutritional need.1 It is a common condition in cancer patients and remains a key challenge in oncology practice. Although malnutrition develops in approximately one-third of patients with malignancies, up to 70% may experience DRM at any time during the disease. Approximately 50% of all patients with advanced cancer manifest cachexia syndrome, a severe form of malnutrition characterized by fatigue, loss of weight and muscle mass. Poor nutritional status and weight loss can lead to poor outcomes for cancer patients, including reduced quality of life, decreased functional status, increased rates of complications, and interruptions in treatment.2 It is estimated that up to 20% of patient cancer deaths may be attributable to DRM and tumor cachexia syndrome rather than to the disease itself. The Impaired nutritional status was evident from the patient’s first visit to a medical oncology center; 51% have nutritional disorders, 43% are considered at risk of malnutrition, and 9% are diagnosed with tumor cachexia. The probability of developing malnutrition depends on the age of the patient, the type of cancer, and the stage of cancer.3–5 Tumor cachexia cannot be fully reversed by conventional nutritional support, but it is important to establish a continuous treatment schedule based on the implementation of nutrition, food supplements, anticachectic drug therapy, exercise, and psychological counseling which, if correctly associated with effective anticancer therapies, can contribute to preserve the patients’ quality of life and improve the prognosis.6 DRM too often remains unrecognized and untreated. Several surveys carried out to gain insights into the awareness and treatment of cancer cachexia among healthcare professionals revealed inadequate management of this comorbidity.7 The most recent ESPEN guidelines also highlight inadequate nutritional support in cancer patients since their first visit and recommending optimization of the quality of life of cancer patients in each stage of the disease through specific nutritional interventions by multidisciplinary teams.8
Medical nutrition (MN), a specific category of nutrition that addresses specific dietary needs and/or nutrient deficiencies in patients who require assistance with eating and who are unable to eat normally, covers parenteral nutrition and all forms of nutritional support defined as “Foods for Special Medical Purposes –FSMPs, regardless of the method of administration.9 There is a strong clinical indication that nutritional interventions – such as nutritional counseling, oral nutritional supplements (ONS), and enteral (EN) or parenteral (PN) nutrition - can positively impact various clinical outcomes, especially for cancer patients who are at high risk of malnutrition.10,11 According to the results from the EFFORT trial (Effect of early nutritional support on Frailty, Functional Outcomes, and Recovery of malnourished medical inpatients Trial - one of the largest, prospective, non-commercial, multicenter, randomized controlled trials conducted in eight hospitals in Switzerland), which evaluated the outcomes of providing nutritional support to patients with tumor cachexia, the probability of achieving caloric and protein goals and 30-day survival is significantly higher in patients with provided individualized nutritional support compared to patients on standard hospital food.12 A secondary analysis of the EFFORT study, focused on a subgroup of oncology patients with different types of cancer, confirms that nutritional treatment is associated with significantly lower mortality risk and better functional and quality of life outcomes.13
ONS are a key management strategy for malnutrition. A systematic review and meta-analysis reported that the use of multi nutrient, high protein oral nutritional supplements (ONS providing 20% total energy from protein) is associated with improved outcomes in a range of patient populations in a variety of healthcare settings and that there is little evidence that it suppresses normal food intake.14 The published literature also provides evidence that early nutritional intervention with high protein-calorie ONS can cushion the negative effects of malignant disease and pharmacological treatment; improve patients’ clinical, nutritional, and functional status; reduce complications and hospital readmissions during a 2- to 12-month period following discharge, and thereby contributing to increased survival in community-based patients at risk of tumor cachexia syndrome.15–18
This favorable clinical profile could be coupled with a favorable economic impact in this disease area, where health spending is increasing faster than cancer incidence.19 However, there is limited evidence of its economic implications, whose profile is often tied to the type of healthcare setting, nutritional intervention, and patient group.20–22 A better understanding of the economic effect of specialized ONS treatments is fundamental in the case of a lifelong disease with a substantial financial burden, such as cancer. The need for economic evaluations becomes even more potent in informing decisions about which interventions to prioritize and how to ensure that maximum health benefits are gained from fixed budgets.
In the Republic of North Macedonia, there are currently no national or officially issued guidelines for nutritional pathways in cancer patients. Furthermore, despite the high rates of malnutrition and tumor cachexia, the diagnoses were not coded. Additionally, although different ONS indicated as nutritional support in specific DRM are currently available in R. N. Macedonia, and in parallel with the generally low level of awareness of DRM, none of them are reimbursed by the Macedonian Health System. Therefore, in addition to the necessary efforts in terms of increased training and hiring of personnel and the creation of organizational pathways aimed at treatment optimization, evidence of the economic value for the use of specialized, nutritionally complete, energy-dense, high-protein ONS formulation in the cancer patient population is needed. The purpose of the pharmacoeconomic analysis was to assess the cost-effectiveness of individualized nutritional support as part of a cancer care program using specialized oral nutritional supplements (ONS) in comparison with standard of care (SOC) in the management of DRM in patients with or at risk for tumor cachexia syndrome in R.N. Macedonia.
Materials and Methods
Design and Structure
In the absence of national epidemiological data, the applied patient cohort corresponds to the population of patients with malignant diseases (age 61–74 years) included in the research by Shaver et al (2021), based on data from the National Health and Nutrition Examination Survey (NHANES) from the Registry for the National Center for Health Statistics, part of the Centers for Disease Control and Prevention in the USA. To evaluate the cost-effectiveness of ONS, we employed a previously published decision tree model that simulates costs and QOL among cancer patients.23 Figure 1 displays the abbreviated influence diagram used to create the decision tree. Patients were entered into the simulation model upon receiving a clinical diagnosis of DRM and/or manifestation of tumor cachexia syndrome, with no contraindication for ONS. Following nutritional assessment, patients can be treated in a hospital or outpatient facility, with potential outcomes categorized as survival or mortality.
For the base-case analysis, the duration of cancer care program was set to 30 days. This duration reflects a clinically relevant period for observing the immediate, short-term effects of early ONS intervention on cancer patients, particularly in the context of managing disease-related malnutrition and tumor cachexia syndrome, with longer durations considered in sensitivity analyses to explore the long-term cost-effectiveness of ONS treatment.24 The model assumes a start age of 61 years for the cohort, with a normal distribution used to model age progression over the 13-year time horizon, which aligns with the follow-up period, average age and weighted life expectancy in the NHANES study cohort, as well as the life expectancy in Macedonia (72–74 years).25 A one-month cycle length was employed to align with standard cost-effectiveness analyses practices, assuming the monthly progression of health states, treatment interventions, and associated costs, while reflecting the 30 days duration of cancer care program.
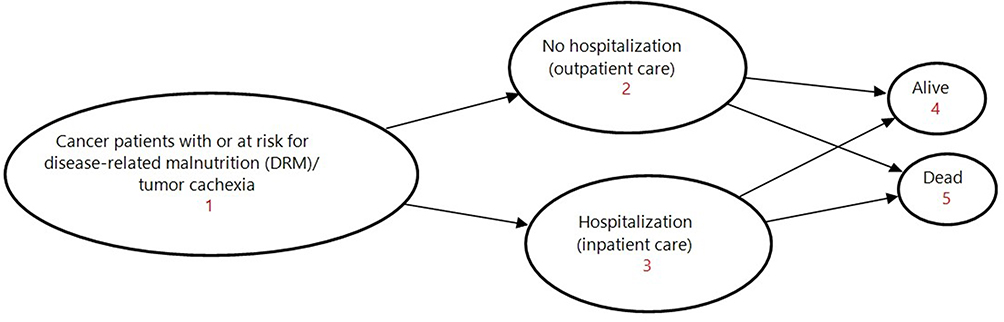 |
Figure 1 Influence diagram (decision and value nodes) for decision tree model. |
To ensure that the decision tree model provided a clinically meaningful and methodologically appropriate simplification of disease progression and treatment pathways, we consulted a panel of tree clinical experts—oncologist, gastroenterologist and dietitian. The purpose of this consultation was to assess whether the model structure adequately reflected key aspects of clinical practice while maintaining a level of abstraction appropriate for economic evaluation. Expert input was specifically used to determine whether: 1) the assumptions regarding DRM and tumor cachexia progression were aligned with real-world clinical experience; 2) the representation of standard care and decision-making processes was consistent with oncology practice, and 3) the model was parsimonious yet sufficient to address the cost-effectiveness question.
Model construction and cost-effectiveness analyses were performed using Tree Age Pro Healthcare software (v.24.2.0).
Model Inputs
All the model input parameters related to natural history, costs, resource use, and utilities are summarized in Table 1.
 |
Table 1 Model Input Parameters in Base-Case Scenario |
Natural History
The model focuses on cancers with a high incidence in older adults, including lung, colorectal, prostate, and breast cancer. These cancers are among the most common types of cancer in older adult populations, with high incidence and significance for early intervention.26 Relapse cases were excluded, as the primary focus was on initial treatment. Monthly transition probabilities between health states were extracted from the literature, primarily following the methodology of Shaver et al (2021).23 The length of hospital stay (LHS) during ward and intensive care hospitalization was obtained from the study of Bargetzi et al (2021), and applied to each treatment strategy.13 The model did not consider the probability of the occurrence of treatment-associated adverse reactions. Patients were assumed to adhere 100% to ONS treatment (ie, receiving treatment according to the recommended dosing schedule specified on the product label) as part of a comprehensive cancer care program. Additionally, treatment effects were assumed to remain constant over time, without considering waning effects.
Cost and Resource Use
The model estimates the effect from the perspective of the Macedonian Health Insurance Fund, accounting solely for direct, supportive care costs associated with the treatment and management of patients. Supportive care costs included ONS costs and SOC costs incurred during inpatient hospitalization. The investigative ONS product was a specialized, nutritionally complete, energy-dense (302 kcal/240 mL), high-protein (16 g/240 mL) ready-to-drink liquid formulation enriched with 1.1 g of EPA (an Omega-3 fatty acid), containing fructooligosaccharides (FOS), fibrin, and vitamins to support the normal function of the GIT and immune system and to decrease tiredness and fatigue. The ONS costs were calculated using the unit cost (wholesale acquisition cost [WAC] and retail reference price of the available preparations in R. N. Macedonia as of June 2020) in correlation with the recommended dosing schedules.
The recommended intake amount was based on the product label (two servings/day; 2×220 mL bottles per day). All costs were based on 2023 Euros (EUR). We used a Euroconversion rate of 0.0165 Euros for one Macedonian denar (MKD). The SOC costs were estimated using official publicly available data of the national health insurance fund in accordance with the price list of health services.27 They reflected only the sum of payments for care provided during inpatient hospital care and does not comprise out-of-pocket payments and payments by private insurance, administration and monitoring of therapy, cost related to the treatment of adverse events and drug therapy.
The analysis did not consider the costs associated with dietary consultation and nutritional assessment. Indirect nonmedical costs (eg, transportation to a clinical center for receiving therapy, loss of productivity, and working ability of the patient or family member or caregiver) due to the impossibility of their accurate assessment in the absence of relevant databases were not considered.
Utilities
Effectiveness was measured in quality-adjusted life years (QALY), which is equal to the patient’s survival time in a certain health state multiplied by the health utility value (quality of life weight) during that period. Annual utility indices for each health state (condition) were also derived from previously published literature, where they were estimated using the EuroQol 5-Dimensions (EQ-5D) method.23
Model Outputs
The total direct costs, clinical outcomes, and incremental cost-effectiveness ratios (ICERs) of ONS and SC have been reported. The total direct costs included the costs of ONS and supportive care. Clinical outcomes included quality-adjusted life-years (QALYs). ICERs included incremental costs per QALY. All cost and effectiveness measures were discounted at 3.0% per year. Half-cycle correction was performed. Treatments were considered “cost-effective” if the ICER was equal to or less than a willingness to pay threshold (WTP) of three times Macedonian per capita gross domestic product (GDP) for 2022 (6275.0 EUR, report of the European Commission, Directorate-General for trade).
Sensitivity Analysis
A one-way deterministic sensitivity analysis (DSA) was performed to determine the impact of individual model parameter inputs on the overall results. The parameters tested in the DSA (varied in an interval of± 25% from the base case inputs) included length of hospital stay, SOC costs, ONS costs, and duration of cancer care program. Following the base-case analysis, additional sensitivity analyses were conducted to explore ONS treatment durations beyond 30 days. Specifically, treatment duration of 120 days and one year after tumor diagnosis and during tumor treatment were considered. Further sensitivity tests assessed the impact of ±25% variation in this alternative ONS treatment durations. To further address the uncertainty in the model inputs, a probabilistic sensitivity analysis (PSA) was conducted using a second-order Monte Carlo simulation, applied both to the base case and alternative scenarios. All costs, utility weights, and the duration of ONS treatment were varied using a gamma distribution, while transition probabilities were varied according to a beta distribution during 10,000 model iterations. The PSA results were expressed in a cost-effectiveness plane and cost-effectiveness acceptability curve.
This study was conducted in accordance with the principles of the Declaration of Helsinki. Given the non-interventional nature of this study, approval from the ethics committee was not required.
Results
Base Case
In the base-case analysis, oral nutritional supplements (ONS) demonstrated superior cost-effectiveness compared to the standard of care (SOC) without ONS in terms of cost per QALY gained, as evidenced by a more favorable cost per QALY gained. Specifically, ONS resulted in both reduced total costs and improved health outcomes compared to SOC (Table 2). The discounted QALYs for ONS were higher than for SOC (8.21 vs.7.91 QALY). Furthermore, ONS incurred lower total costs per patient than SOC (2605.01 vs 3759.23 EUR), yielding an estimated cost saving of 1154.22 EUR. With a negative ICER, ONS intervention was considered a dominant strategy-both less costly and more effective. The observed dominance and associated cost savings were primarily attributable to reduced hospitalization cost, which compensated for higher ONS acquisition costs leading to a lower overall cost for patients receiving ONS. The segmented annual costs/patient associated with each final health outcome (hospitalization, survival, and mortality) for each treatment strategy are summarized in Table 2.
 |
Table 2 Base-Case Results (Discounted) |
Deterministic Sensitivity Analysis
ONS remained dominant over SOC in all scenarios of ± 25% variation in the base-case input parameters (Table 3). Even with a +25% increase in the cost of the daily ONS dose, the strategy remained cost-saving highlighting the economic viability of the ОNS pricing. The primary factor influencing the justification of ONS price was the duration of the cancer care program (ie, days of ONS treatment). The dominance of ONS was maintained in the alternative scenario for up to 120 days of ONS treatment. Further sensitivity analysis evaluating ±25% variation in the scenario of a 120-day cancer care program showed that ONS remained cost-saving up to 132 days. When the treatment duration exceeded 132 days, ONS become a cost-effective strategy, and the justification for reimbursement will depend on the nationally established WTP. Importantly, in all scenarios considered in the model, the ICER was less than the established WTP threshold of 3GDP per QALY gained.
 |
Table 3 Deterministic Sensitivity Analysis |
Probabilistic Sensitivity Analysis
The probabilistic sensitivity analysis (PSA) confirmed the dominance of ONS in the base-case scenario, with a 100% probability of ONS being cost-saving compared to SOC, consistently demonstrating lower costs and better outcomes. In an alternative scenario with a 120-day treatment duration for ONS, the probability of ONS being cost-effective was 47.64% at a willingness-to-pay (WTP) threshold of 3GDP per QALY gained (Figure 2). In 39.76% of the cases, ONS dominated SOC. The acceptability of ONS at nationally defined WTP was 87.75% (Figure 3).
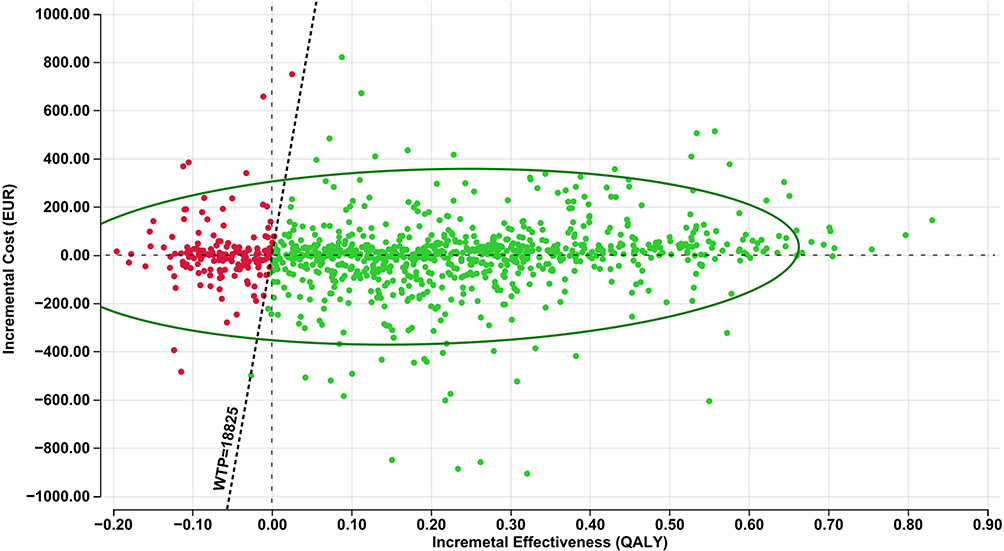 |
Figure 2 Incremental Cost- Effectiveness Scatterplot of ONS vs SOC. Abbreviations: ONS, Oral Nutritional Supplements; SOC, standard of care (no ONS); WTP, Willingness-to-Pay (€/QALY); QALY, Quality Adjusted Life Year. |
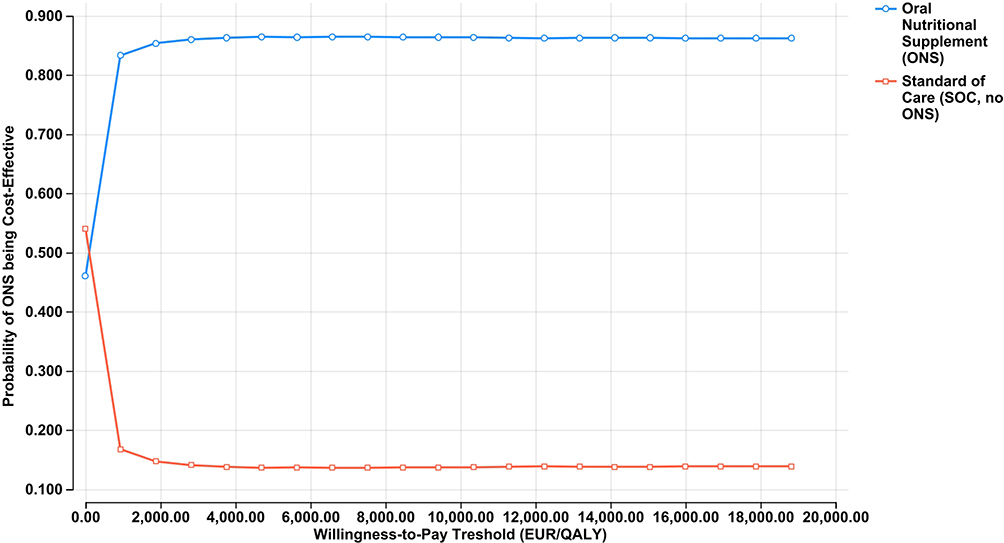 |
Figure 3 Cost-effectiveness Acceptability Curve. Abbreviations: ONS, Oral Nutritional Supplements; SOC, standard of care (no ONS); WTP, Willingness-to-Pay (€/QALY); QALY, Quality Adjusted Life Year. |
Discussion
Health technology assessment (HTA) is a common practice in European countries at the point of market entry to assess the therapeutic and economic value of new treatment strategies and to guide decisions regarding scarce health resource allocation. However, although medical nutrition (MN) products have been on the market for more than three decades, despite being classified as health technologies that may be subject to reimbursement similar to pharmaceuticals, MN remains under-recognized and under-prescribed, with limited evidence regarding its pharmacoeconomic value.28,29 An accumulating body of evidence supports the effectiveness and economic impact of ONS in managing tumor cachexia and DRM, demonstrating favorable treatment outcomes and lower costs relative to the standard of care without ONS. Several economic evaluations of ONS, covering different patient populations in different healthcare settings, including cancer, have shown that the use of MN in the management of DRM can be cost-efficient from a health economic perspective and offers a real opportunity to reduce healthcare expenditures.22,30–36 Compared with other invasive procedures, ONS use in oncology patients can protect against adverse events requiring intensive care, leading to major complications and death at a significantly lower cost per patient compared to no ONS. Systematic reviews assessing the cost and cost-effectiveness of ONS, the most studied MN intervention, have concluded that ONS use, compared to “no ONS” or routine care, leads to valuable clinical outcomes including reduced complications, lower mortality, and decreased length of hospital stay coupled with increased QALY and overall cost savings in patients with cancer-associated malnutrition (tumor cachexia). When used according to national protocols (with or without dietary therapy consultation), ONS is associated with favorable economic outcomes, including cost savings, no significant additional costs per unit of clinical and/or functional improvement, or significantly higher costs per unit of clinical and/or functional improvement, but still within the established cost-effectiveness threshold for outpatient treatment defined by the National Health authorities.37,38
Given variations in clinical practice and reimbursement policies, the outcomes of pharmacoeconomic evaluations cannot be automatically extrapolated to other national healthcare systems. This study represents the first cost-effectiveness study of early oral nutritional supplementation in DRM or risk DRM cancer patients conducted in R.N. Macedonia. The results confirm that specialized ONS is a cost-effective strategy for the nutritional management of community – based cancer patients with DRM or those at risk for DRM and tumor cachexia in our country. Delaying or even preventing DRM by using ONS has the potential to reduce the economic burden of cancer treatment by minimizing the time spent in the hospital. Currently, reimbursement decisions based on HTA in R. N. Macedonia primarily focus on outpatient pharmaceuticals, while medical nutrition remains largely excluded from structured reimbursement policies. In this line, it is generally not provided based on a medical prescription and under the supervision of a healthcare professional, and unlike in other countries from the region, there is no funding by the Macedonian health system for extremely vulnerable cancer patients in outpatient settings. Based on the official country- specific data from the International Agency for Research on Cancer (IARC), there are approximately 11400 patients with malignant disease in R.N. Macedonia.39 Considering that 30% of newly diagnosed patients develop tumor cachexia, and 20% of patients experience disease relapse and are at risk of developing DRM, the estimated annual population of patients in our country who could benefit from specialized ONS is approximately 4500.40 The findings of this study hold significance for both the scientific community and national healthcare stakeholders. From a scientific perspective, this research contributes to the growing body of evidence on the cost-effectiveness of ONS in oncology care, reinforcing its role in improving clinical outcomes and quality of life in malnourished cancer patients. From a policy perspective, the study provides critical insights for healthcare payers, decision-makers, physicians, and patients, highlighting the economic benefits of ONS and its potential to optimize resource allocation within healthcare systems. Given the substantial burden of DRM and tumor cachexia, these findings support the need for structured reimbursement policies that enhance access to cost-effective nutritional interventions while improving oncology patient outcomes and reducing healthcare expenditures.
While this study provides valuable insights into the cost-effectiveness of ONS in oncology care, its findings should be interpreted in light of several limitations. First, the applied patient cohort consists of individuals aged 61–74 years with malignant diseases, based on NHANES data.23 The model does not account for variations in outcomes across other age groups or key independent variables—such as gender, tumor site, cancer stage, and the cost of subsequent oncological and anticachexia therapies. These factors could introduce heterogeneity in healthcare utilization and disease progression, which was not explicitly captured in the model. Additionally, while the exclusion of relapse cases simplifies the model, it also limits the broader applicability of the findings to patients with recurrent cancer. While previous studies have segmented healthcare costs into distinct phases (initial diagnosis, treatment, and end-of-life care) to address these variations, the absence of official national epidemiological data on cancer burden in our country constrained our ability to apply a similar approach.
Second, although the model was parameterized using real-world data from NHANES, its validation was primarily descriptive. The model structure and key assumptions were derived from literature and while this approach aligns with established economic evaluation methodologies, it does not constitute a comprehensive empirical validation based on national cancer registry data. Future research should integrate external calibration with independent datasets and validation using country-specific epidemiological data, as currently, there are no published long-term natural history data or officially available national oncology registries in our country.
Third, we acknowledge the inherent simplifications in decision-analytic modeling compared to real-world clinical practice. In clinical settings, a patient’s treatment history, comorbidities, and prior interventions influence disease-related malnutrition (DRM) progression. However, decision tree and Markov model, assume that all patients within a given health state transition probabilistically, without accounting for individualized treatment pathways. This assumption, while necessary for computational feasibility, may not fully reflect real-world variability in disease management. Nevertheless, as this limitation applies uniformly to both ONS- and standard-of-care (SOC)-treated patients, it was not expected to introduce systematic bias into the comparative model outcomes.
Fourth, while the model incorporates real-world data from NHANES, the transition probabilities from Shaver et al (2021) were applied uniformly across the entire ONS treatment period, without accounting for temporal variations in disease progression or clinical practices. This approach assumes static disease progression and does not account for potential temporal variations due to advancements in oncological treatments, evolving clinical guidelines, or demographic shifts. Furthermore, transition probabilities were not stratified by cancer type, despite well-documented differences in disease progression and treatment response across malignancies. These simplifications may limit the model’s applicability in diverse oncological populations. Future research should incorporate time-dependent transition probabilities and stratified estimates by cancer type to enhance model precision and translational value.
Finally, the model assumes 100% adherence to ONS treatment, meaning that all patients receive the prescribed dosage without discontinuation. In clinical practice, adherence rates are often lower due to tolerability issues, disease progression, or patient preference, which may impact treatment effectiveness. Additionally, the model assumes a constant treatment effect over time, without accounting for waning effects or diminishing efficacy in long-term use. These assumptions may overestimate the sustained benefits of ONS. Future research should incorporate real-world adherence rates and time-dependent treatment effects to improve the model’s predictive accuracy and external validity.
Given the complexity of evaluating nutritional interventions in oncological settings, it remains methodologically challenging to isolate the direct impact of ONS consumption on health outcomes relative to pharmacological interventions. This underscores the need for refined health economic methodologies that better capture the long-term benefits and cost-effectiveness of nutritional support in oncology. Development of specific and adapted health economic methodologies for DRM would enhance the precision and applicability of future cost-effectiveness assessments.28
Despite the limitations above, our study provides valuable information about utilizing specialized ONS in real-world conditions, that may complement and support country-specific decision-making process about its pharmacoeconomic value. While primarily focused on North Macedonia, the findings are relevant to other countries in the Western Balkans including Albania, Bosnia and Herzegovina, Kosovo, Montenegro, and Serbia. These countries, though geographically close, have distinct healthcare and economic contexts compared to EU member states like Slovenia, Croatia, and Bulgaria, where ONS are included in reimbursement lists. In contrast, countries in the Western Balkans do not currently reimburse ONS. However, they face similar challenges in healthcare resource allocation and experience a high burden of disease-related malnutrition (DRM) in oncology patients, making the study’s conclusions applicable to these nations as well.
Expanding ONS reimbursement policies in the Western Balkans could be a cost-effective strategy to improve clinical outcomes and reduce financial pressures on healthcare systems. Given the high burden of disease-related malnutrition (DRM) in oncology patients and shared challenges in healthcare resource allocation across these countries, the study’s findings can inform policy decisions aimed at enhancing cancer care. By highlighting these implications, our research contributes to the broader discussion on healthcare optimization in middle-income countries and provides a framework adaptable to similar regions.
Conclusion
The clinical superiority of ONS in the management of cancer patients who are malnourished, have tumor cachexia, or are at risk of developing it compared to standard of care (SOC) without ONS, has been demonstrated in previous randomized controlled trials. Our analysis further confirms the economic value of specialized ONS, demonstrating its cost-effectiveness compared to SOC within a cancer care program in R.N. Macedonia. These findings provide evidence supporting early use of ONS as a strategy to achieve improved clinical outcomes at lower healthcare costs, reinforcing its potential role in reducing hospitalizations and overall healthcare expenditures. This evidence is particularly relevant for reimbursement decision-making in the management of DRM and tumor cachexia, ensuring access to cost-effective nutritional interventions for this vulnerable patient population not only in Macedonia but also in other countries in the region with similar economic and healthcare conditions, where ONS remains largely unreimbursed despite the high burden of malnutrition and its economic impact on healthcare systems.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Holdoway A, Page F, Bauer J, Dervan N, Maier AB. Individualised nutritional care for disease-related malnutrition: improving outcomes by focusing on what matters to patients. Nutrients. 2022;14(17):3534. doi:10.3390/nu14173534
2. Maia FD, Silva TA, de Vasconcelos Generoso S, Correia MI. Malnutrition is associated with poor health-related quality of life in surgical patients with gastrointestinal cancer. Nutrition. 2020;75:110769. doi:10.1016/j.nut.2020.110769
3. Kubrak C, Martin L, Gramlich L, et al. Prevalence and prognostic significance of malnutrition in patients with cancers of the head and neck. Clin Nutr. 2020;39(3):901–909. doi:10.1016/j.clnu.2019.03.030
4. Muscaritoli M, Lucia S, Farcomeni A, et al. Prevalence of malnutrition in patients at first medical oncology visit: the PreMiO study. Oncotarget. 2017;8(45):79884–79896. doi:10.18632/oncotarget.20168
5. Aprile G, Basile D, Giaretta R, et al. The clinical value of nutritional care before and during active cancer treatment. Nutrients. 2021;13(4):1196. doi:10.3390/nu13041196
6. Maccio A, Sanna E, Neri M, Oppi S, Madeddu C. Cachexia as evidence of the mechanisms of resistance and tolerance during the evolution of cancer disease. Int J mol Sci. 2021;22(6):2890. doi:10.3390/ijms22062890
7. Muscaritoli M, Corsaro E, Molfino A. Awareness of cancer-related malnutrition and its management: analysis of the results from a survey conducted among medical oncologists. Front Oncol. 2021;11:682999. doi:10.3389/fonc.2021.682999
8. Arends J, Bachmann P, Baracos V, et al. ESPEN guidelines on nutrition in cancer patients. Clin Nutr. 2017;36(1):11–48. doi:10.1016/j.clnu.2016.07.015
9. Commission directive 1999/21/EC of 25 March 1999 on dietary foods for special medical purposes. European Commission. Available from: https://eur-lex.europa.eu/legal-content/EN/ALL/?uri=CELEX:31999L0021.
10. Rinninella E, Cintoni M, Raoul P, et al. Effects of nutritional interventions on nutritional status in patients with gastric cancer: a systematic review and meta-analysis of randomized controlled trials. Clin Nutr ESPEN. 2020;38:28–42. doi:10.1016/j.clnesp.2020.05.007
11. Cook F, Rodriguez JM, McCaul LK. Malnutrition, nutrition support and dietary intervention: the role of the dietitian supporting patients with head and neck cancer. Br Dent J. 2022;233(9):757–764. doi:10.1038/s41415-022-5107-8
12. Schuetz P, Fehr R, Baechli V, et al. Individualised nutritional support in medical inpatients at nutritional risk: a randomised clinical trial. Lancet. 2019;393(10188):2312–2321. doi:10.1016/S0140-6736(18)32776-4
13. Bargetzi L, Brack C, Herrmann J, et al. Nutritional support during the hospital stay reduces mortality in patients with different types of cancers: secondary analysis of a prospective randomized trial. Ann Oncol. 2021;32(8):1025–1033. doi:10.1016/j.annonc.2021.05.793
14. Stratton RJ, Hebuterne X, Elia M. A systematic review and meta-analysis of the impact of oral nutritional supplements on hospital readmissions. Ageing Res Rev. 2013;12(4):884–897. doi:10.1016/j.arr.2013.07.002
15. Richards J, Arensberg MB, Thomas S, Kerr KW, Hegazi R, Bastasch M. Impact of early incorporation of nutrition interventions as a component of cancer therapy in adults: a review. Nutrients. 2020;12(11):3403. doi:10.3390/nu12113403
16. de van der Schueren MA, Laviano A, Blanchard H, Jourdan M, Arends J, Baracos VE. Systematic review and meta-analysis of the evidence for oral nutritional intervention on nutritional and clinical outcomes during chemo (radio) therapy: current evidence and guidance for design of future trials. Ann Oncol. 2018;29(5):1141–1153. doi:10.1093/annonc/mdy114
17. Baldwin C, Smith R, Gibbs M, Weekes CE, Emery PW. Quality of the evidence supporting the role of oral nutritional supplements in the management of malnutrition: an overview of systematic reviews and meta-analyses. Adv Nutr. 2021;12(2):503–522. doi:10.1093/advances/nmaa108
18. Cawood AL, Elia M, Stratton RJ. Systematic review and meta-analysis of the effects of high protein oral nutritional supplements. Ageing Res Rev. 2012;11(2):278–296. doi:10.1016/j.arr.2011.12.008
19. Chen S, Cao Z, Prettner K, et al. Estimates and projections of the global economic cost of 29 cancers in 204 countries and territories from 2020 to 2050. JAMA Oncol. 2023;9(4):465–472. doi:10.1001/jamaoncol.2022.7826
20. Baggs GE, Middleton C, Nelson JL, et al. Impact of a specialized oral nutritional supplement on quality of life in older adults following hospitalization: post-hoc analysis of the NOURISH trial. Clin Nutr. 2023;42(11):2116–2123. doi:10.1016/j.clnu.2023.09.004
21. Schuetz P, Sulo S, Walzer S, et al. Economic evaluation of individualized nutritional support in medical inpatients: secondary analysis of the EFFORT trial. Clin Nutr. 2020;39(11):3361–3368. doi:10.1016/j.clnu.2020.02.023
22. Martin B, Cereda E, Caccialanza R, Pedrazzoli P, Tarricone R, Ciani O. Cost-effectiveness analysis of oral nutritional supplements with nutritional counselling in head and neck cancer patients undergoing radiotherapy. Cost Eff Resour Alloc. 2021;19(1):35. doi:10.1186/s12962-021-00291-7
23. Shaver AL, Tufuor TA, Nie J, et al. Cost-effectiveness of nutrient supplementation in cancer survivors. Cancers. 2021;13(24):6276. doi:10.3390/cancers13246276
24. Arends J, Baracos V, Bertz H, et al. ESPEN expert group recommendations for action against cancer-related malnutrition. Clin Nutr. 2017;36(5):1187–1196. doi:10.1016/j.clnu.2017.06.017
25. World Health Organization. North Macedonia [Country overview]. 2025. Available from: https://data.who.int/countries/807.
26. Zahed H, Feng X, Sheikh M, et al. Age at diagnosis for lung, colon, breast, and prostate cancers: an international comparative study. Int J Cancer. 2024;154(1):28–40. doi:10.1002/ijc.34671
27. Health insurance fund of the republic of North Macedonia. price list of health services. 2024. Available from: https://fzo.org.mk/cenovnik-na-zdravstveni-uslugi.
28. Perugini M, Johnson TJ, Beume TM, et al. Are we ready for a new approach to comparing coverage and reimbursement policies for medical nutrition in key markets: an ISPOR special interest group report. Value Health. 2022;25(5):677–684. doi:10.1016/j.jval.2022.01.011
29. Nuijten M. Health economics in medical nutrition: an emerging science. In: Meier RF, Reddy BR, Soeters PB, editors. The Importance of Nutrition as an Integral Part of Disease Management. Karger Publishers; 2015:129–141.
30. Zhong Y, Cohen JT, Goates S, Luo M, Nelson J, Neumann PJ. The cost-effectiveness of oral nutrition supplementation for malnourished older hospital patients. Appl Health Econ Health Policy. 2017;15(1):75–83. doi:10.1007/s40258-016-0269-7
31. Neelemaat F, Bosmans JE, Thijs A, Seidell JC, van Bokhorst-de van der Schueren MAE. Oral nutritional support in malnourished elderly decreases functional limitations with no extra costs. Clin Nutr. 2012;31(2):183–190. doi:10.1016/j.clnu.2011.10.009
32. Norman K, Pirlich M, Smoliner C, et al. Cost-effectiveness of a 3-month intervention with oral nutritional supplements in disease-related malnutrition: a randomised controlled pilot study. Eur J Clin Nutr. 2011;65(6):735–742. doi:10.1038/ejcn.2011.31
33. Ballesteros-Pomar MD, Martínez Llinàs D, Goates S, Sanz Barriuso R, Sanz-Paris A. Cost-effectiveness of a specialized oral nutritional supplementation for malnourished older adult patients in Spain. Nutrients. 2018;10(2):246. doi:10.3390/nu10020246
34. Wyers CE, Reijven PL, Evers SM, et al. Cost-effectiveness of nutritional intervention in elderly subjects after Hip fracture. A randomized controlled trial. Osteoporos Int. 2013;24(1):151–162. doi:10.1007/s00198-012-2009-7
35. Smedley F, Bowling T, James M, et al. Randomized clinical trial of the effects of preoperative and postoperative oral nutritional supplements on clinical course and cost of care. Br J Surg. 2004;91(8):983–990. doi:10.1002/bjs.4578
36. Schuetz P, Sulo S, Walzer S, Krenberger S, Brunton C. Nutritional support during the hospital stay is cost-effective for preventing adverse outcomes in patients with cancer. Front Oncol. 2022;12:916073. doi:10.3389/fonc.2022.916073
37. Freijer K, Bours MJ, Nuijten MJ, et al. The economic value of enteral medical nutrition in the management of disease-related malnutrition: a systematic review. Jl Am Med Dir Assoc. 2014;15(1):17–29. doi:10.1016/j.jamda.2013.09.005
38. Elia M, Normand C, Laviano A, Norman K. A systematic review of the cost and cost effectiveness of using standard oral nutritional supplements in community and care home settings. Clin Nutr. 2016;35(1):125–137. doi:10.1016/j.clnu.2015.07.012
39. Ferlay J, Ervik M, Lam F, et al. Global cancer observatory: cancer today. Lyon, France: International Agency for Research on Cancer; 2024. Available from: https://gco.iarc.who.int/today.
40. Argilés JM, López-Soriano FJ, Stemmler B, Busquets S. Cancer-associated cachexia—understanding the tumour macroenvironment and microenvironment to improve management. Nat Rev Clin Oncol. 2023;20(4):250–264. doi:10.1038/s41571-023-00734-5
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.