")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 17
Cost-Minimization Analysis and Budget Impact Analysis About Subcutaneous Natalizumab in Relapsing-Remitting Multiple Sclerosis in Italy
Authors Prosperini L , Pradelli L , Santoni L, Perini D, Cottone S, Vercellino M
Received 18 October 2024
Accepted for publication 8 March 2025
Published 11 April 2025 Volume 2025:17 Pages 315—333
DOI https://doi.org/10.2147/CEOR.S501716
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Giorgio Lorenzo Colombo
Luca Prosperini,1 Lorenzo Pradelli,2 Laura Santoni,3 Daria Perini,3 Salvatore Cottone,4 Marco Vercellino5
1S. Camillo-Forlanini Hospital, Rome, Italy; 2AdRes Health Economics and Outcomes Resources, Turin, Italy; 3Biogen Italia, Milan, Italy; 4Department of Neurology, A.R.N.A.S. Civico, Palermo, Italy; 5AOU Città della Salute e della Scienza di Torino, Torino, 10126, Italy
Correspondence: Lorenzo Pradelli, AdRes Health Economics and Outcomes Resources, Via Alfieri, 17, Turin, 10121, Italy, Tel +390117651239, Email [email protected]
Purpose: Two analyses, a cost-minimization and a budget impact, were conducted to estimate the economic and financial impact of subcutaneous (SC) vs intravenous (IV) natalizumab in terms of administration times and costs in the Italian setting from the perspective of multiple sclerosis (MS) center, patient, and society.
Patients and Methods: Cost minimization analysis (CMA) adopted a Markov model with three different states, and it is based on the results of REFINE study and its post-hoc analysis, which evaluated and demonstrated the non-inferiority of natalizumab SC vs IV formulation. The economic inputs came mainly from EASIER study, that estimated the administration time, resource consumption, and costs of natalizumab SC vs IV. A lifetime horizon was considered. Budget impact analysis (BIA) was conducted with a cost calculator approach and compared a base scenario (without SC natalizumab) with an alternative scenario (with SC natalizumab). The inputs were shared with the CMA and a 3-year time horizon was considered. A progressive increase in the number of patients treated with natalizumab SC was estimated from the 1st to the 2nd to the 3rd year after reimbursement in Italy.
Results: CMA estimated that savings due to the use of SC instead of IV natalizumab would be € 2,824, € 1,137, and € 9,170 per patient from the perspectives of MS center, patient, and society, respectively, thus depicting a weak dominance (lower costs and non-inferiority efficacy). BIA estimated that the savings were approximately 3.2 million euros from the perspective of MS centers and around 10.3 million euros from the perspective of society in the first 3 years following reimbursement.
Conclusion: Administering natalizumab subcutaneously rather than intravenously to treatment-eligible patients would result in administration time and cost savings thus determining a favorable impact for the MS center, the patient and the society.
Keywords: intravenous natalizumab, subcutaneous natalizumab, multiple sclerosis, MS center, patient perspective, society perspective
Introduction
Multiple sclerosis (MS) is a chronic disease affecting the central nervous system that represents the leading cause of non-traumatic neurological disability in young adult people. In Italy, the prevalence and incidence of MS were estimated to be 221/100,000 and 6 new cases per year every 100,000 persons, respectively (excluding Sardinia, which nearly doubles both prevalence and incidence).1 In 2023, around 137,000 patients are affected by MS in Italy, thus resulting in social costs of about €6 billion.1
The cost per MS patient is high: it was calculated that Italian National Healthcare Service (NHS) has to sustain a mean cost per treated patient with MS equal to €21,069.2 From the societal perspective, the mean annual costs for MS were estimated at €39,307 per patient in Italy.2
Relapsing remitting MS, the most common presentation, is characterized by alternating relapsing and remitting phases.3 Disease-modifying therapies (DMTs) can reduce the number of relapses and slow disease progression.4
Natalizumab is a humanized monoclonal antibody targeting α4-integrin on the surface of lymphocytes, thus preventing immune cells from entering the central nervous system.5 It is indicated for adult patients affected by highly active relapsing remitting multiple sclerosis (RRMS), in patients who have failed a full course with another DMT, and in those with rapidly evolving severe RRMS.6 The Phase 3 Natalizumab Safety and Efficacy in Relapsing Remitting Multiple Sclerosis (AFFIRM) trial proved that intravenous (IV) natalizumab 300 mg every 4 weeks, as compared to placebo, reduced the rate of clinical relapse by 68% and lowered the risk of sustained disability progression by 42% over 2 years in patients with RRMS.7 A new subcutaneous (SC) formulation of natalizumab has been approved by the European Medicines Agency and recently reimbursed by the Italian Medicines Agency (AIFA).
The SC formulation was compared with the IV formulation in the Safety, Tolerability and Efficacy of Multiple Regimens of Natalizumab in Adult Participants With Relapsing Multiple Sclerosis (REFINE) study8 and its post-hoc analysis,9 which concluded that SC natalizumab was non-inferior to IV natalizumab in terms of efficacy, pharmacokinetics/pharmacodynamics, and safety. Both formulations were administered at a dosage of 300 mg every 4 weeks. SC formulations proved to be more convenient than IV formulations with monoclonal antibodies in different settings.10–16 In the case of natalizumab, furthermore, the continuity of all supporting services already in place for the IV formulation is guaranteed.
Regarding natalizumab, the Italian da Endovenoso A Sottocutaneo: Indagine su Efficienza e Risparmio (EASIER) study estimated that SC natalizumab reduced the patient procedure time by about 50%, health care professionals’ active working time by 55% and the occupancy time of the infusion chair by approximately 59% with respect to IV natalizumab.17 In addition, the cost per natalizumab administration procedure would be reduced by 63% for the multiple sclerosis center, by approximately 42% from the social perspective, and 17% from the patient’s perspective.17
Based on data from the REFINE study, its post-hoc analysis, and the EASIER study, we carried out two analyses to evaluate the pharmacoeconomic profile of natalizumab SC vs natalizumab IV: a cost-minimization analysis (CMA) and a budget impact analysis (BIA). The CMA aims to compare, based on non-inferior efficacy, the costs between IV natalizumab and SC natalizumab from the perspectives of the MS center, the patient, and the society. The BIA aims to estimate the differential costs between the base scenario, without SC natalizumab, and the alternative scenario, in which SC natalizumab represents an alternative in Italy for patients with highly active RRMS.
Methods
Overview
Cost-minimization analysis is a simplified cost-effectiveness analysis between treatments sharing the same level of clinical effectiveness. Given the same clinical benefit, CMA involves calculating costs to analyze the least costly alternative or therapeutic modality.
Data derived from the REFINE study8 and its post-hoc analysis18 demonstrated that the SC administration of natalizumab at a dosage of 300 mg every 4 weeks was non-inferior to IV natalizumab in terms of efficacy, pharmacokinetics/pharmacodynamics, and safety.
Budget impact analysis estimates the short-term financial consequences of adopting a new health technology in a specific area from the perspective of the healthcare service, which, by definition, is characterized by resource constraints.
Based on the information reported, a CMA and a BIA were conducted to evaluate a pharmacoeconomic profile of natalizumab SC vs IV. Though having different study designs, these analyses shared the same source data, as reported in the following paragraph.
Shared Data Sources
Clinical Inputs
Two alternatives were compared: SC natalizumab 300 mg every 4 weeks vs IV natalizumab 300 mg every 4 weeks.
The population analyzed was made up of adult patients affected by RRMS treated with natalizumab having baseline characteristics of the REFINE8 study population (mean age 38 years, 69% females), which overlapped with the EASIER study17 used to derive the resource consumption associated with the two routes of administration.
The Italian setting was based on data from REFINE study8 and its post-hoc analysis.18
Data about the discontinuation rate, which was assumed to be equal for IV and SC natalizumab, were derived from the Tysabri Observational Program (TOP) study.19
Expert opinion came from a board composed of neurologists from different areas of Italy with expertise in MS treatment to evaluate the resources consumed for monitoring and management of adverse events (AEs) in terms of visits, laboratory and instrumental tests, and drugs prescribed. In particular, two online sessions were held, and an Excel file was filled by each of them. They also suggested the most suitable method to evaluate adverse events analyzed (mild/moderate or severe) indicating the Diagnosis Related Group (DRG) or the Day Hospital (DH) number or outpatient code. The monitoring of the first year was not included since SC natalizumab is approved for use after one year of IV natalizumab use. Therefore, we compared SC and IV natalizumab populations starting from the second year of natalizumab use. Experts estimated that monitoring of IV and SC natalizumab could be assumed to be overlapping. The Supplementary Material provides details about the resources used for monitoring (Supplementary Tables S1–S3) and the management of adverse events (Supplementary Tables S4–S6) and serious adverse events (Supplementary Tables S7 and S8).
Mild-to-moderate AE rates were derived from the main manuscript of the REFINE study,8 whereas serious AE rates came from the details reported on the website ClinicalTrials.gov about the REFINE study (NCT01405820).20
Clinical inputs included annual risk of discontinuation (6.52%),19 MS relative mortality risk (2.88),21 and administration route-specific AE rates,8,20 which is detailed in the Supplementary Tables S1–S8.
Time Inputs
The mean time dedicated to drug administration (IV and SC) was derived from the observational, multicenter, cross-sectional EASIER study14 and included: time of patient stay in the MS center, healthcare professional (HCP) active working time, time of occupancy of infusion chair, working hours lost by the patient, time for unpaid patient activities, and the time spent by the caregiver accompanying the patient to the MS center.
In particular, “patient time” was defined as the time from patient acceptance until he leaves the MS center; “HCP time” was defined as active working time of the HCP within the patient time; “chair time” was defined as the time occupied by the infusion chair within the patient time.
Economical Inputs
From the perspective of MS centers, direct healthcare costs were considered with the aim of capturing the impact of the introduction of natalizumab SC in terms of costs of acquisition and administration of the drug, costs of monitoring, and costs for the management of adverse events.
From the perspective of the society, in addition to direct healthcare costs, direct non-healthcare costs, and indirect costs were also included.
The valorization of consumed resources was based on the EASIER study17 regarding consumables used during the administration of natalizumab and the depreciation of durable equipment.
The remaining cost items were based on the rates for outpatient services determined in the DRG decree,22 the literature,8,23 and the Gazzetta Ufficiale 167/2023 (Table 1).
The valorization of resources used for monitoring and the managements of adverse events and serious adverse events are reported in the Supplementary Material.
 |
Table 1 Description of Direct Healthcare/Non-Healthcare and Indirect Costs [Data From8,17,22–30 and the Gazzetta Ufficiale 167/2023] |
Cost-Minimization Analysis—Study Design
The CMA was conducted by adapting a Markov model to the Italian setting based on data from REFINE study8 and its post-hoc analysis.18 The analyses were conducted from the MS center (reflecting the NHS perspective), patient (which includes direct non-healthcare costs and indirect costs), and society perspectives (which includes direct healthcare costs, direct non-healthcare costs and indirect costs).
A lifetime horizon (60 years) was considered to cover the entire patient treatment period. Therefore, considering that the average age of entry into the model is 38 years, the lifetime horizon is long enough to cover the residual life expectancy of the cohort and to capture all the relevant consequences as per ISPOR recommendations.
The model, developed in Microsoft Excel®, had already been adopted in MS32 and consists of 3 health states: treatment state, non-treatment state, absorbing state (death) (Figure 1).
 |
Figure 1 Health states in the Markov model used in the cost-minimization analysis. |
At the beginning of the evaluation, all patients were being treated with natalizumab (IV or SC): from this health state, patients could interrupt the treatment by moving to the non-treatment state or die; from the non-treatment state patients could move only to the death state.
At each 28-day cycle, the probabilities of switching between states were determined by the natalizumab treatment discontinuation rate described in the TOP study19 and the probability of death of the Italian population by sex and age33 adjusted for the probability of death specific to MS.21
The model estimated the number of patients who remained in treatment over time to record and compare the accumulation of costs related to the treatment itself (acquisition and administration), the management of adverse events, monitoring, and other cost categories considered depending on the analysis perspective.
The model also estimated the times (patient, HCP, infusion chair, etc) of patients being treated with SC and IV natalizumab.
The reliability of the model and the robustness of the results were tested using univariate deterministic sensitivity analysis and probabilistic sensitivity analysis.
Budget Impact Analysis—Study Design
An impact analysis on budget and administration time was conducted by adapting a static model to the Italian setting (cost calculator approach).
The analysis was carried out from the perspectives of MS centers (reflecting NHS) or society.
A 3-year time horizon was considered.
The model, developed in Microsoft Excel®, compared a base scenario (the scenario 1, in which natalizumab SC was not available as a treatment option reimbursed by the Italian NHS), with an alternative scenario, (scenario 2, following the introduction of natalizumab SC) (Figure 2).
 |
Figure 2 Budget impact model. Abbreviations: HCP, healthcare professional; IV, intravenous; RRMS, relapsing remitting multiple sclerosis; SC, subcutaneous. |
From the perspective of MS centers (NHS), for each of the years of the time horizon considered (3 years), the model calculated the total annual costs (acquisition and administration of drugs, monitoring, and management of adverse events) and times (patient, HCP, infusion chair) for the treatment of patients included in the analysis.
Times and costs accumulated until the end of the 3-year time horizon in each scenario. Subsequently, they were compared to calculate the expense and time impact due to the progressive adoption of SC natalizumab.
The analysis was conducted in compliance with the ISPOR methodological guidelines,34 which recommend a structured framework for the BIA, offer recommendations on how to gather and utilize data, and suggest a standardized reporting format to enhance standardization and transparency.
The economic analysis considered that the size of the population receiving natalizumab remained stable during the simulation based on the assumption that the flow of incident patients starting treatment was in line with the flow leaving the treatment, due to discontinuation or death.
Scenario 1, without SC natalizumab, reflected the number of patients being treated in Italy with IV natalizumab (assumed constant for the 3 years of the simulation).
The treatment mix for scenario 2, with natalizumab SC, was estimated internally considering the number of patients who could start and be treated with natalizumab SC in the first, second and, third year after reimbursement.
It was assumed that 35%, 50%, and 55% of patients treated with IV natalizumab could be treated with natalizumab SC respectively in the first, second, and third year after reimbursement (Table 2).
 |
Table 2 Market Shares in Scenario 1 and Scenario 2 of the Budget Impact Model |
The reliability of the model and the robustness of the results were tested using a one-way deterministic sensitivity analysis.
Results
Cost-Minimization Analysis
Table 3 shows data about costs per patient by year according to each perspective considered in the analysis.
 |
Table 3 Costs per Patient by year According to MS Center, Patient, and Society Perspectives |
MS Center Perspective
CMA estimates that, from the perspective of the MS center, the use of the SC formulation results in savings for each patient over the mean duration of therapy equal to 166 hours of patient stay at the MS center, 13 hours of neurologist active working time, 24 hours of nurse active working time, 168 hours of infusion chair time (Table 4).
 |
Table 4 Per Patient Time Savings Over the Mean Duration of Treatment Estimated by the Cost-Minimization Analysis From the Perspective of the Multiple Sclerosis Center |
Direct healthcare costs related to the acquisition of study drugs, administration, monitoring, and management of adverse events were included.
As SC natalizumab was shown to be non-inferior to IV natalizumab,9 thus laying the foundation for performing a CMA, the years of life lived, total, and under treatment with natalizumab were the same in both treatment arms.
With the same acquisition cost, the SC vs IV formulation leads to savings especially in the cost of administration, due to decreased HCP active working time, infusion chair time, and consumption of healthcare consumables.17
Natalizumab SC is dominant (weak dominance,35 due to non-inferior efficacy8,18 and lower costs) compared to the IV formulation from the perspective of the MS center (reflecting NHS), as it generated a saving of €2,824 per patient treated over the mean length of therapy with natalizumab (Table 5).
 |
Table 5 Results of the Cost-Minimization Analysis From the MS Center Perspective: per Patient, Over the Mean Duration of Natalizumab Treatment |
Patient Perspective
The CMA estimates that, from the patient perspective, SC formulation results in savings for each patient over the mean duration of therapy equal to 166 hours of patient stay at the MS center and 245 hours of working time lost by the patient (considering the working hours lost by those in paid employment).
The direct non-healthcare costs relating to formal assistance (eg, babysitting) and transport towards the MS center at the expense of the patient were included. The working time lost by the patient and not reimbursed was also included.
As explained before, regarding MS center perspective, the years of life lived, total, and under treatment with natalizumab were the same in both treatment arms.
With the same cost for travel/transport, the SC formulation results in a saving on the costs incurred by the patient, especially indirect ones due to lost earnings, which are not reimbursed by social security bodies.
Natalizumab SC is dominant (weak dominance,35 due to non-inferior efficacy18 and lower costs) compared to the IV formulation from the perspective of the patient, as it generated a saving of €1,137 per patient treated over the mean length of therapy with natalizumab (Table 6).
 |
Table 6 Results of the Cost-Minimization Analysis From the Patient Perspective: per Patient, Over the Mean Duration of Natalizumab Treatment |
Society Perspective
CMA estimates that, from the society perspective, the use of the SC formulation results in savings for each patient over the mean duration of therapy equal to: 166 hours of patient stay at the MS center, 37 hours of HCP active working time (neurologist and nurse), 245 hours of working time lost by the patient, 168 hours of infusion chair occupancy.
Furthermore, other time savings should be added, such as the time spent by informal caregivers (relatives/friends) to accompany/assist the patient during administration (151 hours), the time lost by the patient for unpaid activities (131 hours), and the working time lost by the patient reimbursed by social security bodies (included in the 245 working hours lost by the patient) (Table 7).
 |
Table 7 Per Patient Time Savings Over the Mean Duration of Treatment Estimated by the Cost-Minimization Analysis From the Perspective of the Society |
The expense that the society incurs to administer SC or IV natalizumab includes all costs borne by the MS center (which provides the administration), the patient (who receives the administration), and a third party identifiable as “all others”.
Regarding this last point, the analysis also shows a saving relevant to the reduction of the patient’s loss of productivity, whether reimbursed or not reimbursed by the social security bodies, to the time lost by unpaid patients, and to the costs that the society sustains for the time that friends and relatives dedicate to a patient to the detriment of their routine activities.
Natalizumab SC is dominant (weak dominance,35 due to non-inferior efficacy18 and lower costs) compared to the IV formulation from the perspective of the society, as it generated a saving of €9,170 per patient treated over the mean length of therapy with natalizumab (Table 8).
 |
Table 8 Results of the Cost-Minimization Analysis From the Society Perspective: per Patient, Over the Mean Duration of Natalizumab Treatment |
Univariate Deterministic Sensitivity Analysis
The tornado diagram (Figure 3) shows the results of the univariate deterministic sensitivity analysis. Only the parameters that determine the greatest effect on the outcome are reported. The most relevant parameters that can influence the outcome are represented by the administration costs and, to a lesser extent, by the costs of managing adverse events. The variation of these parameters, nonetheless, does not result in a shift in the outcome’s sign, which consistently stays in favor of SC natalizumab.
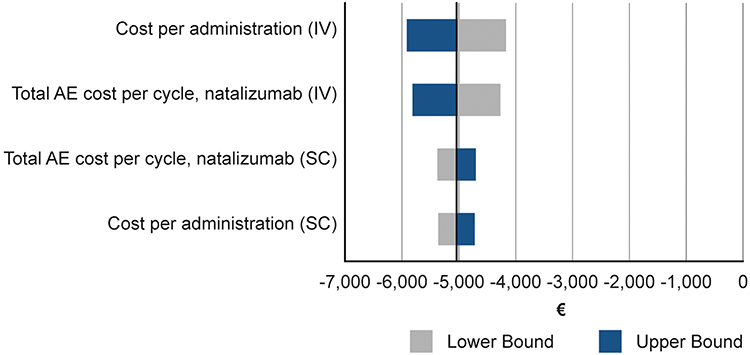 |
Figure 3 Tornado diagram showing the results of the univariate deterministic sensitivity analysis performed on the cost-minimization analysis from NHS perspective. Abbreviations: AE, adverse events; IV, intravenous; SC, subcutaneous. |
Probabilistic Sensitivity Analysis
In Figure 4, the scatter plot’s 1,000 points depict the probabilistic estimates for the overall costs associated with IV natalizumab (in red), the total costs associated with SC natalizumab (in green), and the total cost difference between the two strategies (in light blue).
 |
Figure 4 Scatter plot’s showing the results of the probabilistic sensitivity analysis performed on the cost-minimization analysis from NHS perspective. Estimates about total and differential costs (SC vs IV). Abbreviations: IV, intravenous; SC, subcutaneous. |
The cluster of cost difference estimates between the two strategies is highly condensed, suggesting the robustness of the findings. It is predominantly situated below the cost equivalence line, ie, in the area denoting savings with the adoption of SC natalizumab. A delta of the opposite sign estimated in only 0.1% of the simulations.
The results of the sensitivity analyses confirm the stability of the model and the robustness of the base case results.
Budget Impact Model
MS Centers Perspective
Budget Impact Model (BIM) estimates that, from the MS centers perspective, treating 4,598 patients with SC natalizumab, in the first 3 years after reimbursement, leads to overall savings of 186,207 hours of patient stay at the MS centers, 14,034 hours of neurologist active working time, 28,046 hours of nurse active working time, and 188,355 hours of infusion chair time (Table 9).
 |
Table 9 Time Savings Estimated by the Budget Impact Analysis From the Perspective of the Multiple Sclerosis Centers Over the First 3 years After Reimbursement |
Direct healthcare costs related to the acquisition of study drugs, administration, monitoring, and management of adverse events were included.
With the same acquisition cost, the SC vs IV formulation leads to savings especially in the cost of administration, due to decreased HCP active working time, infusion chair time, and consumption of healthcare consumables.
The progressive use of SC natalizumab leads to savings, from the perspective of MS centers, estimated at €790,939, €1,129,913, and €1,242,904 for the first, second, and third year, respectively. The total savings for the three-year period is approximately 3.2 million euros (Table 10).
 |
Table 10 Results of the Budget Impact Analysis From the MS Centers Perspective: First 3 years After Reimbursement |
Society Perspective
BIM estimates that, from the society perspective, treating 4,598 patients with SC natalizumab, in the first 3 years after reimbursement, leads to overall savings of 186,207 hours of patients stay at the MS centers, 14,034 hours of neurologist active working time, 28,046 hours of nurse active working time, 188,355 hours of infusion chair time, 278,197 hours of working time lost by the patients, 145,982 hours lost by the patients for unpaid activities, and 175,650 hours spent by informal caregivers (relatives/friends) to accompany/assist the patient during administration (Table 11).
 |
Table 11 Time Savings Estimated by the Budget Impact Analysis From the Societal Perspective Over the First 3 years After Reimbursement |
With the same acquisition cost, the SC vs IV formulation leads to savings due the decrease in the cost of administration, patient stay at the MS center, and subsequent reduction in the absenteeism from work and time spent for unpaid activities, and assistance from caregivers (relatives/friends).
The progressive use of SC natalizumab leads to savings, from the perspective of the society, estimated at about 10.3 million euros in the first 3 years after reimbursement (Table 12).
 |
Table 12 Results of the Budget Impact Analysis From the Societal Perspective: First 3 years After Reimbursement |
Univariate Deterministic Sensitivity Analysis
MS Centers Perspective
The tornado diagram (Figure 5) shows the results of the univariate deterministic sensitivity analysis from the perspective of the MS centers. Only the parameters that determine the greatest effect on the outcome are reported.
 |
Figure 5 Tornado diagram showing the results of the univariate deterministic sensitivity analysis performed on the budget impact analysis from the perspective of the MS centers. Abbreviations: IV, intravenous; MS, multiple sclerosis; SC, subcutaneous. |
The tornado diagram shows the percentage variation in the absolute value of the base case in year 3. The blue arms show the result, in terms of percentage increase or reduction, in savings depending on the parameters in their high value. The gray arms indicate the same result associated with the low value. The arm width indicates the size of the overall impact, the uncertainty of the parameter, on the final result.
From the perspective of MS centers (NHS), administration costs and, to a lesser extent, population size are the parameters that can influence the outcome.
However, the variation of these parameters does not change the trend of the model, and the result is still favorable to SC natalizumab. The analyses on years 1 and 2 are in line with the analysis on the third year, thus confirming the stability of the model and the robustness of the base case results.
Society Perspective
From the perspective of society, the model is sensitive to the working time lost by the patients and the caregivers assistance time (Figure 6).
 |
Figure 6 Tornado diagram showing the results of the univariate deterministic sensitivity analysis performed on the budget impact analysis from the perspective of the society. Abbreviations: IV, intravenous; MS, multiple sclerosis; SC, subcutaneous. |
The tornado diagram shows the percentage variation in the absolute value of the base case in year 3. The blue arms show the result, in terms of percentage increase or reduction, in savings depending on the parameters in their high value. The gray arms indicate the same result associated with the low value. The arm width indicates the size of the overall impact, the uncertainty of the parameter, on the final result.
However, the variation of these parameters does not change the trend of the model, and the result is still favorable to SC natalizumab.
The analyses on years 1 and 2 are in line with the analysis on the third year, thus confirming the stability of the model and the robustness of the base case results.
Discussion
The two analyses conducted provide a complete picture of the pharmacoeconomic profile of SC natalizumab compared with IV natalizumab. In our analyses, the results relating to the different points of view (MS center and therefore NHS, patients, and society) give a specific estimate for each of them and provide robust data to support decision making.
CMA was conducted considering a lifetime horizon and the costs were calculated per treated patient. It estimated that savings due to the use of SC instead of IV natalizumab would be €2,824, €1,137, and €9,170, per patient from the perspectives of the MS center, the patient, and the society, respectively, thus depicting a weak dominance with respect to the IV formulation in all the three perspectives considered, because SC natalizumab had non-inferior efficacy and lower costs than IV natalizumab.
The most relevant parameters that can influence the outcome are represented by the administration costs and, to a lesser extent, the costs of managing adverse events.
The stability of the model and the robustness of the base case results were confirmed by the sensitivity analyses.
We chose to include in the analysis the mild and moderate adverse events that occurred during the REFINE study. We conducted a further analysis considering an alternative scenario that included also serious adverse events: the results confirmed the dominance of SC vs IV with savings of €5,041, €1,137, and €11,387 in the perspectives of the MS center, the patient, and the society, respectively.
The BIM estimated the amount of savings over the 3 years after the introduction of SC formulation considering the possible patients eligible for natalizumab in Italy.
The impact analysis on time and cost suggests that the adoption of SC compared with IV natalizumab in Italian clinical practice may result in savings for MS centers (which represent the point of view of the National Health Service) and for the society as a whole. In particular, the savings are approximately 1.2 million euros from the perspective of the MS centers and around 4 million euros from the perspective of the society considering a progressive use of SC natalizumab in the first 3 years after reimbursement (4,598 patients undergoing treatment at third year).
From the perspective of MS centers (NHS), administration costs and, to a lesser extent, population size are the parameters that can influence the outcome.
From the perspective of society, the model is sensitive to the working time lost by the patients and the caregivers assistance time. However, the variation of these parameters does not change the trend of the model, and the result is always favorable to SC natalizumab.
Natalizumab SC reduces patient stay in hospital, HCP active working time, and the occupancy time of durable equipment (infusion chair, bed, room) with a consequent improvement in MS center organization because the resources that are made available can be appropriately reallocated to other activities, thus promoting system efficiency.
The shorter patient stay in hospital results in a decreased number or duration of work permits, but also in the reduction of the mean time that the informal caregiver must dedicate to the patient. Furthermore, the need for “formal care” managed by babysitters/professional caregivers who replace the patient and/or informal caregiver during the administration is reduced.
Generally speaking, subcutaneous administration presents additional benefits compared with intravenous infusion. As already shown in studies in the oncology setting investigating monoclonal antibodies, such as trastuzumab and rituximab, among the advantages of adopting a subcutaneous instead of intravenous administration route are chair, patient, and HCP time reduction,10,11,15 increase in the number of treated patients, with consequent speed up in the waiting list,10 decrease in direct and indirect healthcare costs associated with decreased use of consumables,12,13,16 and reduced loss of productivity,14,16 respectively. It was also shown that the preference of patients generally goes with subcutaneous administration.12,16
Regarding SC natalizumab, Alonso Torres and colleagues recently published a cost-minimization analysis in the Spanish context.36 Comparing analyses from the point of view of two different healthcare services is always challenging, trivially because different costs and tariffs are considered, but in this case there were also differences in the methods, data input, and study objective. The Spanish cost model was based on assumptions made solely by a panel of national experts. Conversely, our CMA was based on the EASIER study results17 that directly measured the time and resources consumption relevant to IV administration through a tailored App in a time-and-motion study, whereas the time spent for SC administration was estimated by national experts through a web-based specific-use questionnaire. In addition, the EASIER study17 estimated direct, indirect, and intangible costs and quality of life (QoL) for patients receiving IV natalizumab and the expected impact of the shift to SC administration through a questionnaire administered to patients.
Regarding dedication time for the administration process, the EASIER study17 took into account only HCP active working time, while the Spanish paper considered that the whole administration process was to be counted as HCP working time.36 As a result, the estimations of the Spanish cost-minimization analysis in terms of minutes spent by HCP were far greater than those measured by the EASIER study17 used in this CMA analysis.
In addition, the Spanish study considered even natalizumab-naïve patients,36 while in Italy SC natalizumab cannot be prescribed to such a subset of patients.
The CMA performed in Sweden37 by the group of Gianinazzi was based on the same three-state Markov model that we used and the inputs are almost the same, obviously taking into account the relevant national costs. The discontinuation rate was slightly different (6.26% vs 6.52%), as they used a different source (the AFFIRM study7 instead of the TOP study19). The Swedish analysis considered only mild and moderate adverse events coming from the published REFINE article, while we conducted also an alternative scenario that included also serious adverse events coming from the details reported on the website ClinicalTrials.gov about the REFINE study (NCT01405820). The administration time was completely fed by expert opinion, whereas, in the case of intravenous formulation, we used measured data from a time-and-motion study (the EASIER study17).
Two main differences are apparent: Gianinazzi and colleagues assumed a reduction in the monitoring time of SC natalizumab, that contributes half of the savings on administration time. In fact, they considered a full hour of monitoring for all the cycles in IV natalizumab and only for the first 6 cycles for SC natalizumab, thus resulting in greater time and money savings than our study. Furthermore, they also valorized the impact of administering natalizumab in a primary care setting instead of a specialized center.
In the Swedish analysis, the savings associated with the use of SC instead of IV natalizumab were estimated at 83.2% in administration costs (slightly higher than our percentage, ie, 63%) and 47% in time (very similar to our 48%).37 In the Swedish study, the cost categories included acquisition, administration, adverse events, and social cost.37
Despite the different approaches, the estimates relevant to the savings in terms of time and cost due to the use of SC instead of IV natalizumab show considerable and fairly comparable savings in three European countries (Italy, Spain,36 and Sweden37).
Although we followed well-known guidelines published by authoritative associations34,38 and relied on the best available evidence and our clinical experience in selecting our inputs, our economic evaluations have some limitations. The main limitation concerns input data about patient, HCP, and infusion chair times in SC administration. In fact, these data were only estimated based on questionnaires administered to HCPs and patients (in the EASIER study17), instead of being measured. However, as SC natalizumab was not yet on the Italian market when the EASIER study was conducted, a direct measurement was impossible.
Like most economic analyses, we also used data that derive from expert opinion and are not published in the literature. However, this method allows to include data suitable for a more complete comparison and, above all, makes the results more consistent with clinical practice. Sensitivity analyses were also conducted to evaluate how much any variability in the data could influence the final result and therefore test the reliability of the model and the robustness of the results.
Conclusion
The results of the conducted analyses indicate that natalizumab SC has a positive pharmacoeconomic profile compared to the IV formulation. In fact, administering natalizumab subcutaneously rather than intravenously to treatment-eligible RRMS patients results in time and cost savings from every perspective considered, the MS center, the patient, and the society. The SC formulation is dominant compared to IV administration. A progressive use of SC natalizumab shows, at the third year after SC natalizumab introduction, a remarkable budget impact both from the perspective of the MS centers (1.2 million euros) and the society (4 million euros).
Abbreviations
AE, adverse events; BI, budget impact; BIA, budget impact analysis; BIM, budget impact model; CMA, cost-minimization analysis; DMT, disease-modifying therapies; HCP, healthcare professional; ICER, incremental cost-effectiveness ratio; IV, intravenous; MS, multiple sclerosis; NHS, National Healthcare Service; RRMS, relapsing remitting multiple sclerosis; SC, subcutaneous.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
Economic analyses were performed by AdRes Health Economics and Outcome Research and funded by Biogen Italia. Medical writing, publishing support, and journal styling services were provided by SEEd Medical Publishers and funded by Biogen Italia.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was funded by Biogen Italia.
Disclosure
MV has received travel grants and advisory board fees from Biogen, Roche, Novartis, Merck. LoPr is the co‐owner and an employee of AdRes, which has received project funding from Biogen; also reports grants from Roche, grants from Johnson and Johnson, grants from Sanofi, grants from Novartis, outside the submitted work. DP and LS are employees of and may hold stock in Biogen. SC has received grants to attend scientific congresses or speaker honoraria from Biogen, Merck-Serono, Novartis, Roche, Sanofi/Genzyme, Teva. LuPr has received personal fees and non-financial support from Biogen, Bristol-Mayer Squibb, Merck, Novartis, Roche, Sanofi, Viatris. The authors report no other conflicts of interest in this work.
References
1. Associazione Italiana Sclerosi Multipla APS/ETS. Barometro della sclerosi multipla e patologie correlate 2023. 2023. Available from: https://agenda.aism.it/2023/.
2. Battaglia MA, Bezzini D, Cecchini I, et al. Patients with multiple sclerosis: a burden and cost of illness study. J Neurol. 2022;269(9):5127–5135. doi:10.1007/s00415-022-11169-w
3. Perrone V, Veronesi C, Giacomini E, et al. The Epidemiology, Treatment Patterns and Economic Burden of Different Phenotypes of Multiple Sclerosis in Italy: relapsing-Remitting Multiple Sclerosis and Secondary Progressive Multiple Sclerosis. Clin Epidemiol. 2022;14:1327–1337. doi:10.2147/CLEP.S376005
4. English C, Aloi JJ. New FDA-Approved Disease-Modifying Therapies for Multiple Sclerosis. Clin Ther. 2015;37(4):691–715. doi:10.1016/j.clinthera.2015.03.001
5. Plavina T, Fox EJ, Lucas N, Muralidharan KK, Mikol D. A Randomized Trial Evaluating Various Administration Routes of Natalizumab in Multiple Sclerosis. J Clin Pharmacol. 2016;56(10):1254–1262. doi:10.1002/jcph.707
6. Tysabri EMA. Summary of Product Characteristics. 2016. Available from: https://www.ema.europa.eu/en/documents/product-information/tysabri-epar-product-information_en.pdf.
7. Polman CH, O’Connor PW, Havrdova E, et al. A randomized, placebo-controlled trial of natalizumab for relapsing multiple sclerosis. N Engl J Med. 2006;354(9):899–910. doi:10.1056/NEJMoa044397
8. Trojano M, Ramió-Torrentà L, Grimaldi LM, et al. A randomized study of natalizumab dosing regimens for relapsing-remitting multiple sclerosis. Mult Scler. 2021;27(14):2240–2253. doi:10.1177/13524585211003020
9. Mealli F, Mattei A, Mariottini A, Massacesi L. Non-inferiority analysis of subcutaneous versus intravenous 300 mg monthly natalizumab administration: a post hoc analysis of the REFINE study. Mult Scler. 2024;30(8):1077–1080. doi:10.1177/13524585241238136
10. De Cock E, Kritikou P, Sandoval M, et al. Time Savings with Rituximab Subcutaneous Injection versus Rituximab Intravenous Infusion: a Time and Motion Study in Eight Countries. PLoS One. 2016;11(6):e0157957. doi:10.1371/journal.pone.0157957
11. De Cock E, Pivot X, Hauser N, et al. A time and motion study of subcutaneous versus intravenous trastuzumab in patients with HER2-positive early breast cancer. Cancer Med. 2016;5(3):389–397. doi:10.1002/cam4.573
12. Dent S, Ammendolea C, Christofides A, et al. A multidisciplinary perspective on the subcutaneous administration of trastuzumab in HER2-positive breast cancer. Curr Oncol. 2019;26(1):e70–e80. doi:10.3747/co.26.4220
13. Dychter SS, Gold DA, Haller MF. Subcutaneous drug delivery: a route to increased safety, patient satisfaction, and reduced costs. J Infus Nurs. 2012;35(3):154–160. doi:10.1097/NAN.0b013e31824d2271
14. Lopez-Vivanco G, Salvador J, Diez R, et al. Cost minimization analysis of treatment with intravenous or subcutaneous trastuzumab in patients with HER2-positive breast cancer in Spain. Clin Transl Oncol. 2017;19(12):1454–1461. doi:10.1007/s12094-017-1684-4
15. Olofsson S, Norrlid H, Karlsson E, Wilking U, Ragnarson Tennvall G. Societal cost of subcutaneous and intravenous trastuzumab for HER2-positive breast cancer - An observational study prospectively recording resource utilization in a Swedish healthcare setting. Breast. 2016;29:140–146. doi:10.1016/j.breast.2016.07.008
16. Pivot X, Gligorov J, Müller V, et al. Preference for subcutaneous or intravenous administration of trastuzumab in patients with HER2-positive early breast cancer (PrefHer): an open-label randomised study. Lancet Oncol. 2013;14(10):962–970. doi:10.1016/S1470-2045(13)70383-8
17. Filippi M, Grimaldi L, Conte A, et al. Intravenous or subcutaneous natalizumab in patients with relapsing-remitting multiple sclerosis: investigation on efficiency and savings-the EASIER study. J Neurol. 2024;271(1):340–354. doi:10.1007/s00415-023-11955-0
18. Mealli F, Mattei A, Mariottini A, Massacesi L. EPR-190. Non-inferiority efficacy analysis of natalizumab (TYSABRI) subcutaneous versus intravenous administration. Eur J Neurol. 2023;30(Suppl 1):247.
19. Butzkueven H, Kappos L, Wiendl H, et al. Long-term safety and effectiveness of natalizumab treatment in clinical practice: 10 years of real-world data from the Tysabri Observational Program (TOP). J Neurol Neurosurg Psychiatry. 2020;91(6):660–668. doi:10.1136/jnnp-2019-322326
20. Biogen. A Randomized, Blinded, Parallel-Group, Phase 2 Study Exploring the Safety, Tolerability, and Efficacy of Multiple Regimens of Natalizumab in Adult Subjects With Relapsing Multiple Sclerosis. 2015. Available from: https://clinicaltrials.gov/study/NCT01405820.
21. Kingwell E, van der Kop M, Zhao Y, et al. Relative mortality and survival in multiple sclerosis: findings from British Columbia, Canada. J Neurol Neurosurg Psychiatry. 2012;83(1):61–66. doi:10.1136/jnnp-2011-300616
22. Ministero della Salute. DECRETO 18 ottobre 2012. Remunerazione delle prestazioni di assistenza ospedaliera per acuti, assistenza ospedaliera di riabilitazione e di lungodegenza post acuzie e di assistenza specialistica ambulatoriale. Gazzetta Ufficiale. 2012. Available from: https://www.gazzettaufficiale.it/eli/gu/2013/01/28/23/so/8/sg/pdf.
23. Garattini L, Castelnuovo E, Lanzeni D, Viscarra C, Gruppo Di Studio DYSCO VISITE DV. Visite DVG di studio D. Durata e costo delle visite in medicina generale: il progetto DYSCO. Farmeconomia Health Econ Ther Pathways. 2003;271(1):109–114. doi:10.7175/fe.v4i2.773
24. ISTAT. Anno 2010. Struttura delle retribuzioni. 2013. Available from: https://www.istat.it/it/files/2013/02/struttura-delle-retribuzioni.pdf.
25. ISTAT. Multiscopo sulle famiglie: uso del tempo - file per la ricerca. 2019. Available from: https://www.istat.it/it/archivio/202520.
26. CNEL, ISTAT. La Valorizzazione Economica Del Lavoro Volontario Nel Settore Non Profit. 2011:63
27. Costi Chilometrici ACI. September 1, 2022. Available from: http://www.aci.it/i-servizi/servizi-online/costi-chilometrici.html.
28. Avenali A, Boitani A, Catalano G, D’Alfonso T, Matteucci G. Un modello per la determinazione del costo standard nei servizi di trasporto pubblico locale su autobus in Italia°. Econ Polt Ind. 2014;(4):181–213. doi:10.3280/POLI2014-004009
29. Comune di Milano. Servizio taxi e tariffe applicate. Comune di Milano. Available from: https://www.comune.milano.it/aree-tematiche/mobilita/taxi.
30. Ebilcoba. Nuovo contratto collettivo nazionale di lavoro colf e badanti. Available from https://www.inps.it/docallegatiNP/Mig/Allegati/701Nuovo_CCNL_colf_badanti_Ebilcoba.pdf.
31. AIFA. DETERMINA 10 luglio 2023. Riclassificazione del medicinale per uso umano «Tysabri», ai sensi dell’articolo 8, comma 10, della legge 24 dicembre 1993, n. 537. (Determina n. 477/2023). (23A04048) (GU Serie Generale n.167 del 19-07-2023). Gazzetta Ufficiale. 2023. Available from: https://www.gazzettaufficiale.it/eli/id/2023/07/19/23A04048/sg.
32. Gianinazzi M, Santoni L, Spidalieri A, et al. EPV-228. Cost-minimisation Analysis of Natalizumab Extended Interval Dosing Compared with Standard Interval Dosing in Italy. Eur J Neurol. 2022;29(Suppl 1):862.
33. ISTAT. Tavole di mortalità della popolazione residente. 2021. Available from: https://demo.istat.it/app/?i=TVM.
34. Sullivan SD, Mauskopf JA, Augustovski F, et al. Budget impact analysis-principles of good practice: report of the ISPOR 2012 Budget Impact Analysis Good Practice II Task Force. Value Health. 2014;17(1):5–14. doi:10.1016/j.jval.2013.08.2291
35. Drummond MF, O’Brien B, Stoddart GL, Torrance GW. Methods for the Economic Evaluation of Health Care Programmes.
36. Alonso Torres AM, Arévalo Bernabé AG, Becerril Ríos N, et al. Cost-Analysis of Subcutaneous vs Intravenous Administration of Natalizumab Based on Patient Care Pathway in Multiple Sclerosis in Spain. Pharmacoecon Open. 2023;7(3):431–441. doi:10.1007/s41669-023-00394-2
37. Gianinazzi M, Soderbarg K, Jomaa K, Ralph L, Davison N, Fink K. A cost-minimization analysis shows significant resource savings associated with the introduction of natalizumab by subcutaneous injection in Sweden, from a socioeconomic perspective. ECTRIMS 2021 – ePoster. Mult Scler. 2021;27(2_suppl):134–740. doi:10.1177/13524585211044667
38. Roberts M, Russell LB, Paltiel AD, Chambers M, McEwan P, Krahn M. Conceptualizing a Model: a Report of the ISPOR-SMDM Modeling Good Research Practices Task Force-2. Value Health. 2012;15(6):804–811. doi:10.1016/j.jval.2012.06.016
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.