")
Back to Journals » Journal of Pain Research » Volume 17
CT-Guided Microwave Ablation with Vertebral Augmentation for Spinal Metastases with Posterior Wall Defects
Authors Zhang X, Niu J, Fan J, Hu M, Xing C, Yuan Q, Yang S, Wang B, Li P, Man Q, Ren Y, Wu L , Zhang K
Received 5 April 2024
Accepted for publication 21 August 2024
Published 29 August 2024 Volume 2024:17 Pages 2823—2832
DOI https://doi.org/10.2147/JPR.S463266
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amitabh Gulati
Xusheng Zhang,1,* Jiacheng Niu,2,* Jing Fan,1 Miaomiao Hu,1 Chao Xing,1 Qianqian Yuan,1 Shen Yang,1 Baohu Wang,1 Peishun Li,1 Qirong Man,1 Yanchen Ren,1 Linlin Wu,1 Kaixian Zhang1
1Department of Oncology, Tengzhou Central People’s Hospital Affiliated to Jining Medical College, Tengzhou, Shandong Province, People’s Republic of China; 2Medical Imaging Center, Tengzhou Central People’s Hospital Affiliated to Jining Medical College, Tengzhou, Shandong Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Kaixian Zhang, Email [email protected]
Purpose: To evaluate the efficacy and safety of combined microwave ablation (MWA) and vertebral augmentation (VA) in the treatment of spinal metastases with posterior wall defects.
Patients and Methods: A retrospective review was conducted for 67 patients (42 men, 25 women) with painful spine metastases and posterior wall defects who underwent MWA combined with VA. Among these patients, 52 vertebrae had no epidural invasion and 33 had mild invasion but did not compress the spinal cord. Procedural effectiveness was determined by comparing visual analog scale (VAS) scores and Oswestry disability index (ODI) scores before the procedure and during the follow-up period.
Results: The procedure was technically successful in all patients. The mean VAS score declined significantly from 6.85 ± 1.81 before the procedure to 3.27 ± 1.97 at 24 h, 1.96 ± 1.56 at 1 week, 1.84 ± 1.50 at 4 weeks, 1.73 ± 1.45 at 12 weeks, and 1.71 ± 1.52 at 24 weeks post-procedure (p < 0.01). The mean ODI score was lower post-procedure than before the procedure (p < 0.001). Transient nerve injury occurred in two patients (SIR classification D), and the incidence of asymptomatic bone cement (SIR classification A) was 43.5% (37/85).
Conclusion: MWA combined with VA is an effective and safe treatment for painful spine metastases with posterior wall defects.
Keywords: microwaves, vertebroplasty, spinal, metastases
Introduction
The spinal metastatic disease is a common complication of advanced malignant tumors, and the incidence of spinal metastasis is second only to lung metastasis and liver metastasis.1 Osteolytic metastasis is the most common type of spinal metastasis, and approximately 31% of patients undergoing imaging examinations have damaged the posterior edge of the vertebral body.2 These patients often have severe pain. When the lesions invade the spinal cord, they may be accompanied by neurological symptoms and paraplegia. Because of the short-life expectancy and poor quality of life for these patients, a minimally invasive approach is desirable. New therapeutic strategies that offer curative options have recently become available. Fast pain relief and prevention of spinal compression symptoms are the primary treatment goals for patients with posterior wall defects.
Radiotherapy is the standard treatment plan for the spinal metastases. However, radiotherapy is effective in approximately 60% cases, and about half of these patients experience a recurrence of pain within one year.3,4 Microwave ablation (MWA), radiofrequency ablation, cryoablation, and vertebral augmentation (VA) are commonly used minimally invasive treatments for spinal metastases.5–8
During thermal ablation, the protective barrier of the spinal cord is lost because of the incomplete posterior margin of the vertebral body; therefore, the spinal cord may be caused temporary injury during this procedure.9 Destruction of the posterior edge of the vertebral body is prone to bone cement leakage, which leads to spinal stenosis and is a relative contraindication to vertebroplasty Therefore, whether VA can be performed in patients with posterior edge destruction of the vertebral body is currently controversial.10–13
Although MWA with VA has proven effective for controlling pain associated with spinal metastases,14,15 there are few reports with regard to vertebral metastases with incomplete posterior edges of the vertebral body. Therefore, we analyzed the safety and effectiveness of MWA with VA in treating posterior edge destruction of the vertebral body and tumors invading the spinal canal but not compressing the spinal cord.
Materials and Methods
This retrospective analysis was approved by the Institutional Review Committee of our hospital (Ethics number: 2020-Ethics Review-12). Informed consent was obtained from all patients before treatment. Medical records including demographic pain scores and Oswestry disability index (ODI) scores were obtained and reviewed.
Patient
Overall, 67 patients (42 men, 25 women) with 85 vertebral metastases were treated with MWA and VA at our institution from June 2015 to June 2022. The mean age of patients was 62.2 years (range, 18–82 years). In 67 patients, there were 38 thoracic vertebrae and 47 lumbar vertebrae. A total of 53 (79.1%), 13 (19.4%), and 2 (1.5%) patients had 1, 2, and 3 lesions, respectively. The baseline clinical characteristics of the patients are listed in Table 1.
 |
Table 1 Baseline Characteristics of the Study Participants |
Preprocedural Evaluation
All patients underwent computed tomography (CT) and magnetic resonance imaging (MRI) scans of the lesions before the procedure, mainly to evaluate the location and scope of the lesions, the degree of damage to the posterior edge of the vertebral body, and the relationship with the epidural space and spinal cord.
According to the modified Epidural Spinal Cord Compression Scale proposed by Gang Sun, Bilsky, and Shimony, the degree of epidural invasion and spinal cord compression is classified as type A, B, and C.12,16,17 Type A is vertebral posterior wall defects without epidural invasion. Type B is mild epidural involvement without compression of the spinal cord. Type C is epidural involvement with compression of the spinal cord. Type C was not included in this study. The height of the vertebral body was measured on the sagittal CT digital. This was compared to the adjacent vertebral body and used to calculate the percentage of vertebral body compression. Neurological level of injury was sub-divided into levels A, B, C, D, and E according to the Frankel scale.18
The visual analog scale (VAS) (range 0–10) was used to assess the patient’s pain before procedure. The pain of patients with multiple metastatic sites was recorded as the highest VAS score. Before the procedure, the patients’ filled out ODI questionnaire was used to assess their quality of life.
Inclusion Criteria
We included patients with the following: (1) Thoracolumbar metastasis confirmed by pathology of the primary tumor. (2) Persistent or recurrent pain after radiotherapy or refusal of radiotherapy. (3) Intractable, localized pain (VAS score ≥4 at all metastatic sites). (4) Destruction of the posterior margin of the vertebral cortex or invasion of the spinal canal without compression of the spinal cord (type A or B). (5) Grade E spinal cord Frankel function. (6) Expected survival time of at least three months.
Exclusion Criteria
We excluded patients with the following: (1) Non-correctable coagulation disorder (platelets <50×109/L; international normalized ratio > 1.50). (2) A posterior margin of the vertebral body that destroyed by tumor and compresses the spinal cord with neurological symptoms (type C). (3) Spinal cord Frankel function ≤Grade D. (4) An Eastern Cooperative Oncology Group performance status of 3.
Procedural Details
All procedures were performed by the same interventionalist with >10 years of experience in ablation treatment. An interdisciplinary team of radiologists, pain physicians, surgeons, and oncologists evaluated all patients before procedure. All procedures were completed under CT guidance.
The patient would lay prone on the CT bed and fixed with a vacuum negative pressure pad to prevent their movement during the procedure. We used a 3–5 mm CT scan to reconfirm the location of the lesion and measure the needle angle and depth. Throughout the procedure, patients were under moderate sedation with continuous intravenous infusion of sufentanil (50 ug/mL diluted 1:10 with saline solution) and local anesthesia by 20 g × 20 cm puncture needle (2% lidocaine hydrochloride and 0.25% ropivacaine hydrochloride). If the tumor was located on one side of the vertebral body and did not exceed the midline of the vertebral body, a unilateral pedicle puncture was used; otherwise, a bilateral pedicle puncture was used.
There were 23 cases of unilateral pedicle puncture of the vertebral body and 62 vertebral bodies subjected to bilateral pedicle puncture. The bone puncture needle (13 gauge × 130mm, Shandong Guanlong Medical Utensils Co., Ltd., Jinan, China) was inserted into the front edge of the vertebral body lesion, and three-dimensional reconstruction was employed to adjust the direction of the puncture needle.
We used the coaxial method to advance the MWA antenna (1.6mm × 200mm, ECO Microwave Electronic Institute) along the bone puncture needle to the anterior edge of the tumor, and the bone puncture needle was withdrawn to expose the microwave antenna by at least 1.5–2.0 cm. We then inserted the temperature measuring electrode (20 gauge × 200mm, ECO Microwave Electronic Institute) into the ipsilateral intervertebral foramen. The appropriate ablation power and time to perform ablation were selected. We closely monitored the temperature measurement of the electrode during the ablation process, and we terminated the ablation once the temperature exceeded 44°C.19 During the ablation process, patients were constantly asked for any abnormal sensation and movement in their upper and lower extremities. If there was severe pain sensation and abnormal movement, the ablation was stopped immediately.
The MWA power was set between 20 and 40W (mean 30.5W, SD 5.4W), which was applied for 2–5min (mean 3.4min, SD 1.4min). Ablation power and duration were chosen according to the lesion. If the lesion was close to the front of the vertebral body, the ablation power was 30–40 W for 3–5 min. Whereas if the lesion was close to the back of the vertebral body, the ablation power was 20–30 W for 2–3 min. After the ablation was completed, the microwave antenna was withdrawn, and the bone puncture needle was advanced again to tumor’s front edge.
The polymethylmethacrylate bone cement (Osteopal V; Heraeus) was extracted with a 1 mL syringe and put into ice brine to prolong the setting time of the cement. We waited 10 min for the vertebral body temperature to drop before injecting bone cement. To prevent extravasation of the bone cement, a CT scan was used to observe the distribution of the bone cement A single vertebral body was scanned each time, and the scanning time was approximately 3s.
When the bone cement was close to the posterior edge of the vertebral body, we reduced the single injection dose of the cement to 0.3–0.5 mL. If the bone cement was found to overflow in the spinal canal or intervertebral foramen, we immediately stopped the injection. A CT scan and three-dimensional reconstruction were performed immediately after the injection was completed to observe and record the distribution and leakage of bone cement (Figure 1). The mean volume of bone cement injected per lesion was 5.2mL (SD 2.2ML, range 2.0–8.5mL). Radiologic and operative characteristics are listed in Table 2
 |
Table 2 Radiologic and Operative Characteristics |
 |
Figure 1 A 52-year-old male with painful osteolytic L2 metastases from lung Squamous carcinoma was treated with MWA combined with VA (a) Preprocedure MRI showed L2 vertebral metastasis with posterior wall defect. (b) Preprocedure axial CT shows L2 osteolytic destruction with posterior wall defect. (c) The MWA antenna is inserted into the lesion via a transpedicular approach. (d) Sagittal reconstruction CT showing the microwave antenna centrally located in the Vertebrae. (e) A thermometric electrode is placed in the right intervertebral foramen to monitor the temperature changes in the foramen during the ablation process in real time. (f) Post-ablation axial CT shows a decrease in density and vacuole formation in the lesion area. (g) Post-procedure axial CT shows the distribution of bone cement with in the treated vertebral body. |
Technical success was defined as the accurate placement of the antenna in the lesion, achievement of the target ablation power and time, and placement of adequate cement in the lesion.
Follow-Up Schedule
All patients undergoing MWA and VA completed a preprocedure evaluation and were followed up 24 h, 1 week, and 4, 12, 24 weeks after the procedure. The patients personally filled out a questionnaire to record their VAS scores and ODI scores. CT and MRI of the target vertebral bodies were performed to evaluate the local control of vertebral tumors at 4, 12, 24 weeks after the procedure. Local tumor progression was defined as the growth of an osteolytic defect or a soft tissue component of the tumor.
Outcome Assessment
Before the implementation of MWA and VA, each patient self-evaluated their pain score from 0 to 10 according to the VAS scoring standard. The patient’s VAS score was reevaluated again at follow-up point after procedure and compared to the preprocedure score. The treatment effect was evaluated according to the change in the pain score. The ODI scores were evaluated before the procedure and 4, 12, and 24 weeks after procedure, and the improvement of the patient’s quality of life and mobility was evaluated according to the changes in ODI scores.
The bone cement leakage during the procedure was evaluated based on the CT scan immediately after the procedure, and we recorded whether the bone cement spilled out, the location of the spill, and whether it was associated with neurological symptoms. The complications of MWA and VA were evaluated according to the Society of Interventional Radiology SIR evaluation criteria.20
Statistical Analysis
All data analysis was performed using GraphPad Prism software, version 6.0 (GraphPad Software, La Jolla, California). Numerical data were expressed as means and SD or as medians and ranges, as appropriate. Qualitative data were expressed as frequencies and percentages. The analyses of changes in VAS score and ODI score before and after treatment were tested by Student’s t-tests. A P value <0.05 was considered statistically significant.
Results
MWA and VA had a 100% success rate. The median follow-up time was 11.6 months (range 6–21).
Effectiveness Assessments
The mean VAS scores were 6.85 (SD 1.81) before the procedure and 3.27 (SD 1.97) at 24 h, 1.96 (SD 1.56) at 1 week, 1.84 (SD 1.50) at 4 weeks, 1.73 (SD 1.45) at 12 weeks, and 1.71 (SD 1.52) at 24 weeks after the procedure. There were statistically significant differences in VAS scores before and after the procedure (p < 0.001) (Figure 2). VAS scores decreased significantly 24 h after procedure in 63 patients, whereas 54 patients remained pain relived for more than six months.
 |
Figure 2 The graph shows the mean ± SD of the VAS scores before and after the procedure. |
The mean ODI score was 40.75 (SD 3.53) before the procedure and 21.24 (SD 6.85) at 4 weeks, 17.26 (SD 6.34) at 12 weeks, and 16.3 (SD 6.25) at 24 weeks after the procedure. The differences between the median preprocedural ODI score and postprocedure scores at 1 week and 4, 12, 24 weeks were statistically significant (p < 0.001) (Figure 3).
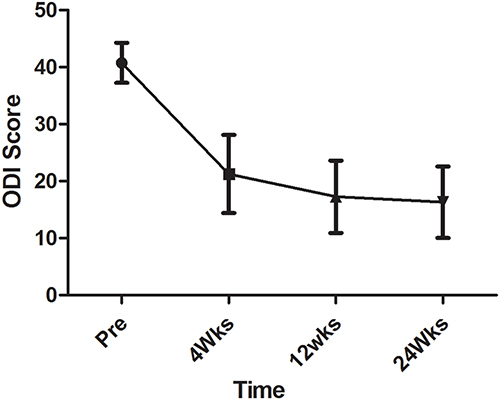 |
Figure 3 The graph shows the mean ± SD of the ODI scores before and after the procedure. |
A total of eight patients died of tumor progression during follow-up. Among the remaining 59 patients, 56 patients (71 lesions) completed the follow-up imaging data, of which MR imaging was 82% (58/71), CT imaging was 72% (51/71), and 24 weeks tumors. The local control rate was 76% (54/71).
Safety Assessments
Two patients had transient lower limb muscle strength impairment after procedure, and muscle strength returned to the normal range after symptomatic support treatment.
In one patient with type B, the muscle strength of both lower extremities decreased to grade 3 after the procedure (SIR classification D). This patient was treated with 30W intermittent ablation for 4.5min, the intraoperative maximum temperature of the ipsilateral foramen area was 40 °C, a total of 7.5mL bone cement was injected, and no bone cement leakage occurred. The decrease in muscle strength may be due to the mass effect caused by the injection of bone cement, resulting in tumors in the spinal canal compressing the spinal cord. After the procedure, the patient’s muscle strength in both lower extremities was restored to the normal range after administration of mannitol (125mL IV q8h), a glucocorticoid (methylprednisolone, 200mg/day IV for 3 days, then reduced by 20% every 3 days) combined with radiotherapy (30Gy in 10 fractions).
In another patient with type B, the muscle strength of their lower limb decreased to grade 4 after procedure (SIR classification D), and the muscle strength returned to the normal range after 48h of postprocedure treatment with mannitol (125mL IV q8h) and methylprednisolone sodium succinate (120mg/day IV for 2 days).
The incidence of asymptomatic bone cement leakage was 43.5% (37/85; SIR classification A). There were 13 cases of intervertebral discs at the site of leakage, 12 cases for the spinal canal, nine cases for paravertebrae, two cases for retrovertebral veins, and one case of intervertebral foramen. None of the instances of cement leakage caused clinical symptoms. The bone cement leakage rate of type A patients was 44.2%, whereas for type B patients was 42.4%. There was no significant difference in the bone cement leakage rate between the type A and type B patients (p = 0.525).
During the follow-up period, no bone cement embolization, skin burns, infection nor pathological fractures were observed. Furthermore, no perioperative deaths were observed.
Discussion
The destruction of the posterior edge of the vertebral body facilitates the loss of the barrier effect of bone cement. Thus the cement is more likely to overflow into the spinal canal and cause spinal stenosis. A study of VA after laser ablation on fresh cadaveric bone confirmed that laser ablation before bone augmentation improved bone cement distribution and tumor tissue ablation before vertebroplasty created voids that resulted in the preferential filling of the defect and reduced the risk of cement extravasation from the vertebral body.21
There are some reports on radiofrequency ablation combined with VA in treating spinal metastases with the destruction of the posterior edge of the vertebral body. Nakatsuka A reported 15 cases of vertebral metastases with posterior margin destruction or pedicle involvement in patients undergoing radiofrequency ablation combined with VA. Four cases had nerve damage, and three eventually had hemiplegia.22 The reason may be that the early radiofrequency ablation electrodes could not precisely control the temperature, and the destruction of the cortical bone at the posterior edge of the vertebral body lost heat isolation. Edwin then used a radiofrequency ablation system to precisely control heat output and monitor tissue temperature to treat 12 patients who had vertebral metastases with posterior edge destruction.9 All patients were treated with radiofrequency ablation combined with VA, and their pain was effectively controlled without complications such as nerve damage.
Compared to radiofrequency ablation, MWA generally heats tissue faster and precisely, which results in better and more complete coagulation necrosis.23 Similar results were achieved in our study by MWA combined with VA for 67 cases of spinal metastatic carcinoma with the destruction of the posterior margin of 85 vertebral bodies. In our study, 94.03% of patients experienced pain improvement 24 h after procedure, and 85.71% of patients remained pain relieved for more than 6 months.
Bone cement leakage is the main complication of VA, and Sun12 reported that the bone cement leakage rate in the treatment of incomplete spinal cord by VA alone was 69.6%. We adopted a combined treatment mode of MWA followed by bone cement injection, and the leakage rate of bone cement was 43.5%, which was lower than Sun’s report. Furthermore, we found no difference in the bone cement leakage between Type A and Type B patients. After MWA, a potential cavity can be formed in the ablated vertebral body, which reduces the pressure during bone cement injection and simultaneously forms a void around the ablation. An ablation shell acts as a medium barrier. Additionally, thrombosis caused by ablation can reduce the leakage of bone cement into the vertebral vein and posterior wall.24
To reduce the bone cement leakage rate during injection, we used a 1mL syringe instead of a high-pressure injection. Therefore, the amount of bone cement injected each time did not exceed 1 mL. When the bone cement was close to the posterior edge of the vertebral body, 0.3–0.5 mL of bone cement was slowly injected each time. When the bone cement overflowed along the fracture direction of the spinal canal, we paused for 30–60 s to allow the bone cement to solidify at the fracture position and then slowly injected the liquid again. The injection was terminated immediately when the CT scan showed infiltration of the bone cement into the spinal canal or intervertebral foramen. To prolong the setting time of the bone cement, the cement extracted by the 1 mL syringe was placed in ice saline. After each bone cement injection, the cement was completely pushed out by the occipital core of the bone puncture needle to prevent the remaining bone cement in the bone puncture needle from solidifying.
It is reported in the literature that once the temperature exceeds 44°C, it may cause irreversible nerve damage.19 To avoid nerve thermal damage, we inserted a thermocouple needle at the nerve root on the same side of the ablation antenna or at the posterior edge of the vertebral body near the spinal cord and measured the temperature of this area in real-time during the ablation process. Once the temperature exceeded 44°C, the ablation was immediately stopped, and 5% ice dextrose was injected into the spinal canal to protect the spinal cord. During the procedure, the patient was awake, and the possible spinal cord injury was judged using the patient’s biofeedback, such as the abnormal sensation of limbs and impairment of limb movement. If the patient had symptoms such as severe pain and limb numbness, ablation was immediately stopped. In our study, under real-time temperature monitoring, there were no complications involving irreversible nerve injury caused by MWA.
This study has some limitations. First, it was a single-center retrospective study with a small sample size, with no research control group. In addition, the short-life expectancy and frailty of the patients enrolled, the short follow-up period for many subjects, and the rapid progression of the disease may have masked the benefits and risks of the procedure. Some patients were also receiving systemic treatments. These tumor treatments are effective and may have caused some pain relief.
Conclusion
CT-guided MWA with VA is safe and effective for treating metastatic carcinoma of the vertebral body with the destruction of the posterior edge of the vertebral body. For advanced spinal metastasis with moderate-to-severe pain, it provides a minimally invasive treatment that can quickly relieve pain and improve the quality of life.
Abbreviations
CT, computed tomography; MWA, microwave ablation; VA, vertebral augmentation; RFA, radiofrequency ablation; VAS, visual analog scale; ODI, Oswestry Disability Index.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The protocol conformed to the principles of the declaration of Helsinki and was approved by the Ethics Committee of the Tengzhou Central People’s Hospital Review Board (Ethics number: 2020- Ethics Review-12). Informed consent was obtained from all patients before treatment. All the methods were carried out in accordance with relevant guideline and regulation.
Acknowledgments
We thank my colleagues in the Oncology Department of Tengzhou Central People’s Hospital for their support in the writing of the paper. This paper has been uploaded to Research square as a preprint: https://assets.researchsquare.com/files/rs-3349316/v1/681470b7-e874-4670-9d74-d6cf7c7e91c9.pdf?c=1695651544
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Medical and Health Science and Technology Development Program of Shandong Province, China (202103101038).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sciubba DM, Gokaslan ZL. Diagnosis and management of metastatic spine disease. Surg Oncol. 2006;15(3):141–151. doi:10.1016/j.suronc.2006.11.002
2. Shah LM, Salzman KL. Imaging of spinal metastatic diseaseInt. J Surg Oncol. 2011;2011:769753. doi:10.1155/2011/769753
3. Chow E, Zeng L, Salvo N, Dennis K, Tsao M, Lutz S. Update on the systematic review of palliative radiotherapy trials for bone metastases. Clin Oncol. 2012;24(2):112–124. doi:10.1016/j.clon.2011.11.004
4. Huisman M, van den Bosch MA, Wijlemans JW, van Vulpen M, van der Linden YM, Verkooijen HM. Effectiveness of reirradiation for painful bone metastases: a systematic review and meta-analysis. Int J Radiat Oncol Biol Phys. 2012;84(1):8–14. doi:10.1016/j.ijrobp.2011.10.080
5. Kastler A, Alnassan H, Aubry S, Kastler B. Microwave thermal ablation of spinal metastatic bone tumors. J Vasc Interv Radiol. 2014;25(9):1470–1475. doi:10.1016/j.jvir.2014.06.007
6. Wallace AN, Greenwood TJ, Jennings JW. Radiofrequency ablation and vertebral augmentation for palliation of painful spinal metastases. J Neurooncol. 2015;124(1):111–118. doi:10.1007/s11060-015-1813-2
7. Tomasian A, Wallace A, Northrup B, Hillen TJ, Jennings JW. Spine cryoablation: pain palliation and local tumor control for vertebral metastases. AJNR Am J Neuroradiol. 2016;37(1):189–195. doi:10.3174/ajnr.A4521
8. Xie P, Zhao Y, Li G. Efficacy of percutaneous vertebroplasty in patients with painful vertebral metastases: a retrospective study in 47 cases. Clin Neurol Neurosurg. 2015;138:157–161. doi:10.1016/j.clineuro.2015.08.026
9. van der Linden E, Kroft LJ, Dijkstra PD. Treatment of vertebral tumor with posterior wall defect using image-guided radiofrequency ablation combined with vertebroplasty: preliminary results in 12 patients. J Vasc Interv Radiol. 2007;18(6):741–747. doi:10.1016/j.jvir.2007.02.018
10. Heini PF, Wälchli B, Berlemann U. Percutaneous transpedicular vertebroplasty with PMMA: operative technique and early results. A prospective study for the treatment of osteoporotic compression fractures. Eur Spine J. 2000;9(5):445–450. doi:10.1007/s005860000182
11. Murphy KJ, Deramond H. Percutaneous vertebroplasty in benign and malignant disease. Neuroimaging Clin N Am. 2000;10(3):535–545.
12. Sun G, Li L, Jin P, Liu XW, Li M. Percutaneous vertebroplasty for painful spinal metastasis with epidural encroachment. J Surg Oncol. 2014;110(2):123–128. doi:10.1002/jso.23608
13. Sun H, Yang Z, Xu Y, et al. Safety of percutaneous vertebroplasty for the treatment of metastatic spinal tumors in patients with posterior wall defects. Eur Spine J. 2015;24(8):1768–1777. doi:10.1007/s00586-015-3810-8
14. Khan MA, Deib G, Deldar B, Patel AM, Barr JS. Efficacy and safety of percutaneous microwave ablation and cementoplasty in the treatment of painful spinal metastases and myeloma. AJNR Am J Neuroradiol. 2018;39(7):1376–1383. doi:10.3174/ajnr.A5680
15. Chen L, Hou G, Zhang K, et al. Percutaneous CT-guided microwave ablation combined with vertebral augmentation for treatment of painful spinal metastases. AJNR Am J Neuroradiol. 2022;43(3):501–506. doi:10.3174/ajnr.A7415
16. Shimony JS, Gilula LA, Zeller AJ, Brown DB. Percutaneous vertebroplasty for malignant compression fractures with epidural involvement. Radiology. 2004;232(3):846–853. doi:10.1148/radiol.2323030353
17. Bilsky MH, Laufer I, Fourney DR, et al. Reliability analysis of the epidural spinal cord compression scale. J Neurosurg Spine. 2010;13(3):324–328. doi:10.3171/2010.3.SPINE09459
18. Ryu S, Yoon H, Stessin A, Gutman F, Rosiello A, Davis R. Contemporary treatment with radiosurgery for spine metastasis and spinal cord compression in 2015. Radiat Oncol J. 2015;33(1):1–11. doi:10.3857/roj.2015.33.1.1
19. Uchiyama S, Yashiro K, Takahashi H, et al. An experimental study of spinal cord evoked potentials and histologic changes following spinal cord heating. Spine. 1989;14(11):1215–1219. doi:10.1097/00007632-198911000-00014
20. Dariushnia SR, Wallace MJ, Siddiqi NH, et al. Society of interventional radiology standards of practice committee. Quality improvement guidelines for central venous access. J Vasc Interv Radiol. 2010;21:976–981. doi:10.1016/j.jvir.2010.03.006
21. Ahn H, Mousavi P, Chin L, et al. The effect of pre-vertebroplasty tumor ablation using laser-induced thermotherapy on biomechanical stability and cement fill in the metastatic spine. Eur Spine J. 2007;16(8):1171–1178. doi:10.1007/s00586-007-0375-1
22. Nakatsuka A, Yamakado K, Maeda M, et al. Radiofrequency ablation combined with bone cement injection for the treatment of bone malignancies. J Vasc Interv Radiol. 2004;15(7):707–712. doi:10.1097/01.rvi.0000133507.40193.e4
23. Lubner MG, Brace CL, Hinshaw JL, Lee FT. Microwave tumor ablation: mechanism of action, clinical results, and devices. J Vasc Interv Radiol. 2010;21(8 Suppl):S192–S203. doi:10.1016/j.jvir.2010.04.007
24. Zhang X, Ye X, Zhang K, et al. Computed tomography‒guided microwave ablation combined with osteoplasty for the treatment of bone metastases: a multicenter clinical study. J Vasc Interv Radiol. 2021;32(6):861–868. doi:10.1016/j.jvir.2021.03.523
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.