")
Back to Journals » Clinical Ophthalmology » Volume 19
Determinants of Healthcare Professionals’ Knowledge on Age-Related Macular Degeneration Risk Factors in Ethiopia
Authors Alemu DS , Munaw MB , Bekele MM , Asmare Kindie C, Ayele FA, Limenih MA
Received 23 January 2025
Accepted for publication 23 May 2025
Published 4 June 2025 Volume 2025:19 Pages 1771—1785
DOI https://doi.org/10.2147/OPTH.S514480
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Destaye Shiferaw Alemu,1,* Minychil Bantihun Munaw,2 Matiyas Mamo Bekele,2 Chalie Asmare Kindie,3 Fisseha Admassu Ayele,3 Miteku Andualem Limenih1,*
1Department of Epidemiology and Biostatistics, Institute of Public Health, College of Medicine and Health Sciences, Comprehensive Specialized Hospital, University of Gondar, Gondar, Amhara National Regional State, Ethiopia; 2Department of Optometry, School of Medicine, College of Medicine and Health Sciences, Comprehensive Specialized Hospital, University of Gondar, Gondar, Amhara National Regional State, Ethiopia; 3Department of Ophthalmology, School of Medicine, College of Medicine and Health Sciences, Comprehensive Specialized Hospital, University of Gondar, Gondar, Amhara National Regional State, Ethiopia
*These authors contributed equally to this work
Correspondence: Destaye Shiferaw Alemu, Department of Epidemiology and Biostatistics, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, P.O.Box: 196, Gondar, Ethiopia, Tel +251938316951, Email [email protected]
Purpose: The aim of this study was to assess knowledge of healthcare professionals on risk factors of age-related macular degeneration and to identify factors that affect their level of knowledge.
Patients and Methods: A cross-sectional study design was employed to collect data from 607 healthcare professionals in Gondar City from August 1 to 30, 2024. Systematic random sampling was used to select study participant. Interviewer administered questionnaire was used to collect data. Bi-variable and multivariable logistic regression analyses were conducted using R statistical software to identify determinants affecting knowledge on age-related macular degeneration risk factors. The strength and precision of relationships between the outcome and the factors were quantified using adjusted odds ratios with 95% confidence intervals. P – value below 5% was used to declare statistically significance associations.
Results: Six hundred seven healthcare professionals took part in this study. Less than one-third of the participants (29.7%; 95% CI: 25.0%, 34.8%) showed adequate knowledge of risk factors of age-related macular degeneration. Male sex (AOR: 1.68; 95% CI: 1.16, 2.43), healthcare service experience less than five years (AOR: 1.86; 95% CI: 1.23, 2.88), ten years of experience in healthcare (AOR: 0.57; 95% CI: 0.34, 0.95), eye health-related training (AOR: 1.91; 95% CI: 1.23, 2.83), hypertension history (AOR: 2.28; 95% CI: 1.52, 3.44) and diabetes mellitus (AOR: 2.48; 95% CI: 1.02, 6.27) determine healthcare professionals’ knowledge of age-related macular degeneration risk factors.
Conclusion: The study highlights a significant knowledge gap among healthcare professionals regarding age-related macular degeneration risk factors. Gender, years of experience in healthcare, and receiving eye health-related training are key determinates of knowledge on age-related macular degeneration risk factors, underscoring the importance of directed educational and trainings to improve healthcare professionals’ knowledge on age-related macular degeneration risk factors.
Keywords: age-related macular degeneration, knowledge gap, risk factor, Ethiopia
Introduction
Age-related macular degeneration (AMD) is emerging as the major reason for severe visual impairment and blindness among individual age 50 and older, in the world1 and it is the root cause of legal blindness in industrialized nations.2 It is becoming a pressing health challenge because of increased longevity of the ageing populations.3 Worldwide, 8.7% of the population is affected by AMD,4 which contributes to 9% of all blindness cases.5 Its prevalence has been steadily rising overtime; in 2015, AMD accounted for 8.4 million cases of moderate or severe vision impairment.6,7 By 2020 an estimated 196 million were affected, with projections reaching 288 million by 2040.4 The total of individuals with AMD is estimated to rise as life expectancy continues to rise.8 By 2025, the global elderly population will become 1200 million, with 70% residing in developing countries,9 and the world’s population will reach around 10.3 billion in the middle of 2080, from 8.2 billion in 2024.10 In Ethiopia the prevalence of age related macular degenerative ranges from 9.9% to 24.1%.11–14
Age related macular degeneration is a chronic disease of the retinal that typically triggers gradual deterioration of central vision.15 It encompasses pathologic alterations to the innermost layers of the retinal part of the macular and surrounding vascular network.16 It is marked by the existence of drusen, which are extracellular white or yellow deposits, along with abnormalities in pigmentation.17 Clinically, there are two primary types of AMD – atrophic (dry)-type representing approximately 85–90% cases of AMD, and neovascular (wet) -type AMD. Late AMD can lead to a sudden and rapid decline in vision if it takes the neovascular form,18 resulting is potential blindness.19
Age-related macular degeneration is a disease influenced by multiple factors: aging, environment, and genetic susceptibility.2,20 There is a growing evidence that sheds light on the various amenable and not amenable factors to change that contribute to AMD advancement.18,21 Smoking is among the most significant modifiable environmental factors consistently linked to AMD,22 with smokers being 2–4 times more likely to develop the condition.23 Furthermore, smoking is associated with more severe forms of AMD.24 The other most important non-modifiable risk factor for developing AMD is age,16,25,26 with its impact can be influenced by other contributing factors.1 The likelihood of developing AMD rises with each passing decade after the age of 60.11 Sunlight exposure throughout one’s working life is a notable risk factor for AMD.27 Epidemiological studies suggest that people exposed to higher sunlight experience increased risk AMD.28 Occupationals with long-term exposure to solar radiation has also been linked to macular degeneration in outdoor workers29 though this association remains controversial.30 Eyes that have undergone cataract surgery have higher AMD progression risk, likely due to the loss of the lens’ natural protection from sunlight.28 High consumption of beef and overweight are linked to higher risk of developing advanced AMD, whereas fruits offered a protective effect.31 The Age-Related Eye Disease Study demonstrated that nutritional additives reduced AMD progression from earlier to late stages by 34% in a six-year follow-up.32 Other key risk factors for associated with AMD include uncontrolled hypertension,24,30,33 hyperlipidemia,30 a body mass index over 25,24,33 family history of AMD,26 ethnicity,16 and cardiovascular risk factors.34
Age related macular degeneration significantly affects the elderly quality of life, reducing their ability to perform everyday tasks.35–37 Impaired vision from AMD leads to falls and fractures risks,38 depression, recognizing faces and performing basic living functions.39 Central vision loss associated with AMD impacts essential activities, including reading, driving, and face recognition,40 and early and intermediate stages can impair driving performance, particularly in complex situations, making drivers less safe.41 AMD poses both physical and mental challenges for those affected.36 Studies show that individuals with AMD experience much stress and depression compared to healthy individuals.35,39 Additionally, AMD is linked to impaired cognitive functions and Alzheimer’s disease,42 with patients facing a 1.46 times more likely of developing Alzheimer’s or Parkinson’s disease.43 Research has also shown that AMD is linked to a 20% higher risk of overall death and a 46% higher risk of cardiovascular disease.44 Furthermore, the progressive decline in visual function among individuals with AMD significantly affects their well-being and incurs substantial social expenses.45 The financial burden associated with blindness from AMD is considerable, with yearly additional costs for each blind person estimated at around USD 5000.46 Globally, the total cost of visual impairment due to AMD exceeds $300 billion, with more than $250 billion attributed to direct healthcare expenses.47 Considering the growing elderly population in developed nations and the rising engagement of older adults in the workforce, AMD impacts workplace productivity. Individuals with AMD suffer from decreased work productivity with average unemployment rate associated with AMD varies between 5.50% and 77%.48
Although there is no viable treatment available for both early AMD and geographic atrophy, there are management and prevention strategies that can help prevent or slow disease progression and rehabilitate those affected.49 Any treatment that lowers the likelihood of progressing to advanced AMD is crucial in lessening the burden on patients, their family members, and the society at large.32 For advanced neovascular AMD, the gold-standard treatment is intraocular injections.16 Intravitreal anti-VEGF (vascular endothelial growth factor) agent is very effective in treating neovascular AMD, and has significantly reduced the rates of visual impairment in populations around the globe.19 These targeted therapies have transformed treatment for patient with neovascular AMD.50 Randomized clinical trials have shown that intravitreal injections of anti-VEGF agents to treat choroidal neovascularization in patients with neovascular AMD lowered the likelihood of moderate vision loss to less than 10% over a 24-month period.51,52 Low vision aids and rehabilitation focus on optimizing the use of remaining vision following significant loss of vision teaching skills to improve daily visual functioning, helping individuals adapt to permanent vision loss and enhancing their psychosocial well-being.53 In addition, there is increasing evidence supporting the beneficial effect of a healthy diet rich in anti-oxidant supplements to reduce the risk of intermediate-stage AMD progressing to advanced stages.54,55
However, current treatments can only partially slow disease progression and cannot stop it, consequently, understanding how to prevent its onset and identifying risk factors is essential. While no specific preventive method has been established, understanding the high-risk factors for AMD and making lifestyle changes are important for managing this multifactorial disease.56 Studying risk factors is crucial because there are no effective treatments for AMD, and identifying modifiable risk factors can improve prevention and slow AMD progression. Effective communication between patients and care providers can improve AMD care and enhancing understanding of the risk factors of AMD is essential to enhance understanding of the diagnosis and treatment of AMD, and reduce anxiety and stress related to illness.57 Future advancements are anticipated to come from improved prevention, risk factor modification, personalized medicine, new anti-VEGF treatments, and regenerative therapies.19 Furthermore, research into more stringent control and prevention measures for AMD emphasizes its risk factors to facilitate early intervention.58 This study provides information how general knowledge on AMD risks helps to make patient counselling and referral links if needed. As the aging population continues to grow it leads to an increase in the numbers visual impaired people related to AMD. Furthermore, as healthcare providers are generally considered as front-line informers and educators of health, understanding their knowledge and influencing factors plays a significant role in increasing public knowledge of the risks of AMD. Assessing healthcare providers knowledge of risk factors of AMD is imperative for identifying areas where awareness needs to be raised to facilitate the prompt identification and treatment of the condition. The aim of this study was to assess knowledge of general healthcare providers on AMD risk factors and to identify the influencing factors.
Materials and Methods
Study Design, Setting and Period
A cross-sectional study was carried out to collect data from healthcare professionals in Gondar City. Gondar city is located in the Amhara National Regional State, Central Gondar Zone 727 km from Addis Ababa, the capital of Ethiopia. The data collection period spanned from August 1to 30, 2024. The city administration is home to a variety of healthcare facilities, including eight health centers, one general hospital, and one comprehensive specialized hospital. The comprehensive specialized hospital serves as a teaching and referral hospital and includes a tertiary eye care center, providing both general and specialty eye care services through outpatient and inpatient units. In total, there are 2611 healthcare providers in the city’s government health facilities, encompassing general practitioners, nurses, midwives, psychiatric nurses, anesthesiologists, and laboratory technologists. In addition, Gondar city has a network of 61 private healthcare facilities, including 33 specialty clinics, 24 medium clinics, 2 eye care clinics, 1 primary hospital, and 1 general hospital.
Study Population
All healthcare providers working in public healthcare facilities in the study area were eligible to the study. However, eye care professionals, including ophthalmologists, optometrists, cataract surgeons, and ophthalmic nurses, were excluded from the study as the main objective of the study was to assess the knowledge of non-eye care regarding AMD risk factors. Healthcare workers in private healthcare facilities were excluded from the study to avoid collecting duplicate data, as it is believed that most privately employed in the study area also work in government facilities. Additionally, this decision was made to ensure feasibility in terms of data collection.
Sample Size Determination
The single population proportion formula was used to determine the sample size for the study taking 95% confidence level (Zα /2 = 1.96), 50% proportion of knowledge on risk factors of AMD, as no prior studies on this topic were available, 4% degree of precision in to consideration. Based on these parameters, the sample size was 600, and with an estimated non-response rate of 10%, 660 was the final number of study participants. The total 660 sample was distributed for the randomly selected hospitals proportional to number of healthcare providers.
Sampling Technique and Procedures
First the number of healthcare providers in Gondar city were collected based on the level care (health center, general hospital and specialized hospital). Then the number of healthcare providers was proportionally allocated to each healthcare level and systematic random sampling technique was applied to select healthcare providers within each stratum. The total number of healthcare professionals (2611) was divided by the required sample size (660) to determine a sampling fraction interval of 4. Then every 4th healthcare provider was included in the sample once the first participant selected.
Operational Definitions
In this study, we measured healthcare providers’ knowledge of AMD risk factors among healthcare providers who were aware of the condition. Healthcare provider were considered aware of AMD when they provided a positive response (yes) for the question, “Have you ever heard of age-related macular degeneration?” and being able to describe AMD, as “a condition caused by deterioration of the retina or part of the eye, leading to blurred central vision or blindness in elderly individuals”, were considered aware of AMD. Study participants who identified the two most consistently literature reported age related macular degeneration risk factors—age and cigarette smoking16,22,25,26 and/or one or more additional risk factor were classified as having adequate knowledge of AMD risk factors; otherwise knowledge was considered inadequate. Knowledge on AMD was assessed with seven question items adapted from previous studies.59,60 These question items encompass definitions of AMD, its causes, symptoms, risk factors, prevention strategies, treatments, and its types. Health providers who answered the knowledge questions correctly were awarded one point for each correct answer; otherwise, they received zero points. The possible knowledge score on AMD for each participant ranges from zero to seven, and the total knowledge score classified into61 good (80–100%), fair (60–79%), and poor (below 60%) based on Bloom’s cutoff point. Additionally, participants who had undergone an eye examination within the past year were categorized as having had a recent eye examination.62 Participants were considered to have a history of eye disease if they had been diagnosed with any type of eye disease by an eye care professional.62 In this study healthcare providers were those health professionals who had direct contact with patients (such as nurse, medical doctors) and those with indirect contact with services such as laboratory technologist and pharmacists.
Data Collection Tool and Procedures
A pre-tested structured questionnaire, adapted from previous studies,59,60 was used to collect data. The questionnaire consisted of three parts: socio demographic data, health related data and knowledge related questions about risk factors of AMD. The questionnaire was administered face-to-face using the English version of the questionnaire as it was challenging to make direct translation form English to Amharic (local language) and it the pretest indicated healthcare providers are rather well familiar with terms related to AMD in English than Amharic. The data were collected by three optometrists supervised by the principal investigators after a verbal informed consent was sought from each study participant.
Data Quality Assurance
A pretest was conducted with 30 healthcare providers (5% of the total sample size) from healthcare settings not included in the study. This was done to assess the consistency of the wording and to identify any relevant items that may have been overlooked in the questionnaire. A half day training was provided to data collectors by the researcher on how to collect the data. A close day-to-day supervision was made to ensure quality data and collected data were checked for completeness.
Ethical Considerations
The study was ethically approved by the University of Gondar Ethical Review Board (Ref# AV/S10914). Additionally, a letter of support was secured from the administrative offices of the Central Gondar Zonal Health Bureau. Each study participant provided informed verbal consent before participating in the study, ensuring they were fully informed to refuse or leave to participate in the study at any time without any consequences. As the study was deemed to involve minimal risk to participants and it was designed to gather anonymous data on non-sensitive topic the institutional review board decided verbal consent was sufficient to ensure participants’ rights and welfare without imposing unnecessary burden. This decision was approved by the University of Gondar IRB, which recognized the appropriateness of verbal consent for this study. The verbal consent process was documented thoroughly, ensuring that all participants were fully informed about the study’s aims and their rights. To maintain confidentiality, individual identifiers were excluded, and a computer with a password was use to secure data.
Statistical Analysis
Entered data to Microsoft excel 16 (Supplementary 1) and were reviewed for completeness and consistency before performing analysis with the R statistical software version 4.4.1.63 The univariable analysis was presented as percentages and frequencies, while continuous data were reported as means and standard deviations. A binary logistic regression model was employed to examine the relationship between knowledge of AMD risk factors and the independent variables. Initially, associations between knowledge and predictors were examined using bivariabel logistic regression to identify factors linked to the dependent variable. Subsequently, variables with a P-value < 0.2 in the bivariate logistic regression were included in a multivariable logistic regression model to assess significant associations. The Hosmer-Lemeshow goodness-of-fit test was used to assess model fit (p-value = 0.73). The strength of the association between the independent variables and the dependent variable was evaluated using adjusted odds ratios with 95% confidence intervals, with P-values < 0.05 considered statistically significant. In our analysis, we exclusively included healthcare providers who demonstrated an awareness of AMD, as specified in the operational definition.
Results
Participants Characteristics
A total of 607 healthcare providers, with a response rate of 92%, were participated in the study. The mean age of the study participants was 33.2 (±5.4) years. They had varied healthcare service experiences ranging from 1 to 37 years. Almost half of the participants (332) were male, and 68% (417) were married. A large majority of the healthcare providers (77.8%) worked in specialized hospitals (Table 1).
 |
Table 1 Sociodemographic Profiles of Healthcare Providers in Gondar City, Northwest Ethiopia (N= 607) |
Profession and Eye Healthcare Related Trainings of Study Participants
Nurses accounted for around 40% (263) of the study participants, while medical doctors represented a quarter (128) of the study participants. Less than one-third (165) of the study participants had received training related to eye health which ranges from as recent as one year to as long as 18 years since the training has been taken. Nearly equal proportions of participants received eye health-related training during their university/college education or through on-the-job training (Table 2).
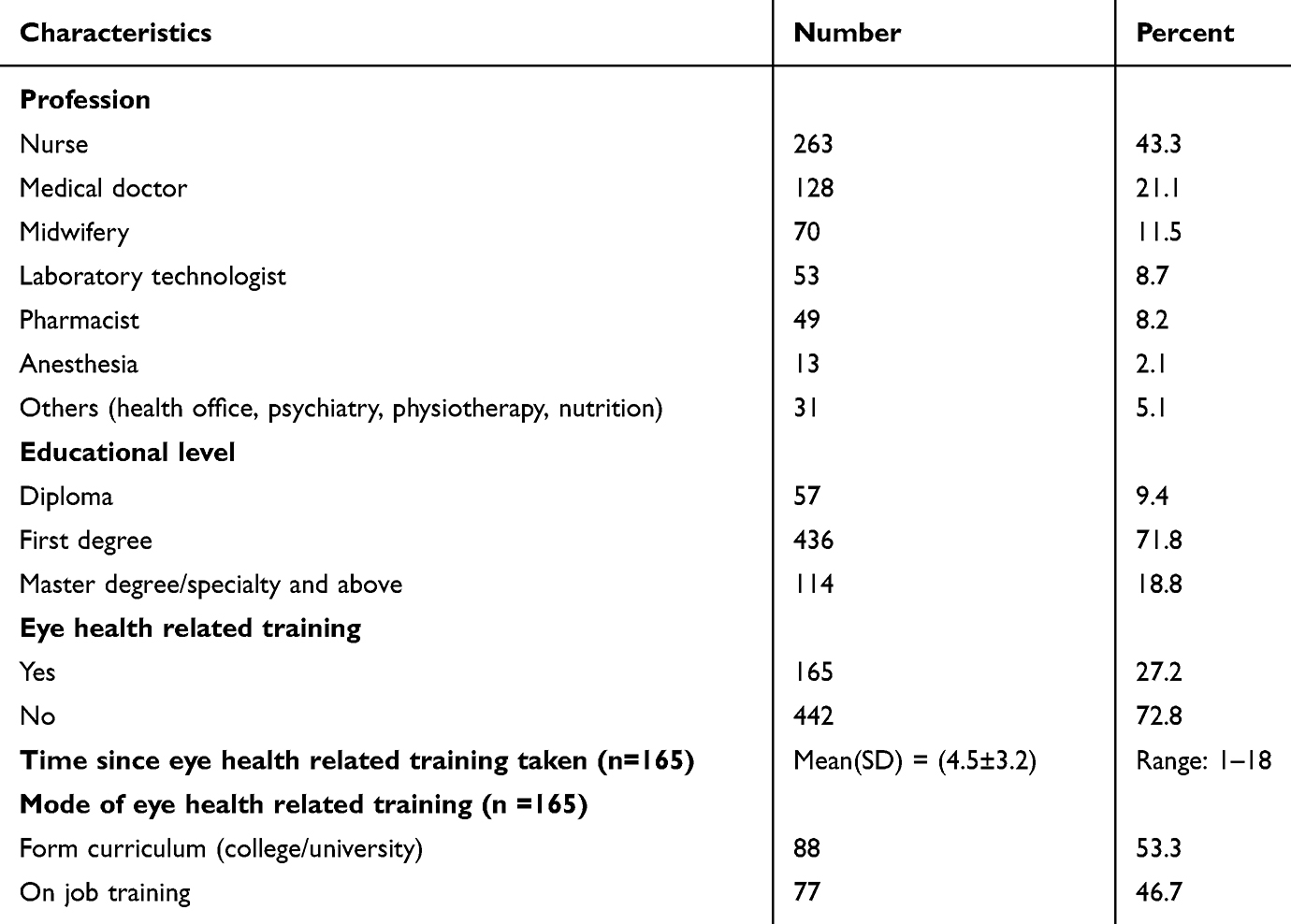 |
Table 2 Study Participants Profession and Eye Health Related Training at Gondar City, Northwest Ethiopia, 2024 (n = 607) |
General and Eye Health Related Status of the Study Participants
Two hundred thirty-six participants (38.9%) had a family history of hypertension, while only 5.6% reported having hypertension themselves. Additionally, one-third of the participants (182) had a family history of diabetes mellitus. Less than one-third (168) of the participants had undergone a general eye check-up in the past year, and approximately a quarter (94) had a confirmed eye health condition with refractive errors (45.7%) and conjunctivitis (26.6%) (Table 3).
 |
Table 3 General and Eye Health Status of Study Participants in Gondar City, Northwest Ethiopia, 2024 (n = 607) |
Knowledge on AMD Risk Factors
Among the study participants who were aware of age-related macular degeneration (350), 29.7% (95% CI: 25.0%, 34.8%) demonstrated adequate knowledge of its risk factors. The large majority of study participants demonstrated significant knowledge about older age (95.7%), diabetes mellitus (76.6%), cigarette smoking (72%), and hypertension (68%) as risk factors of AMD (Figure 1).
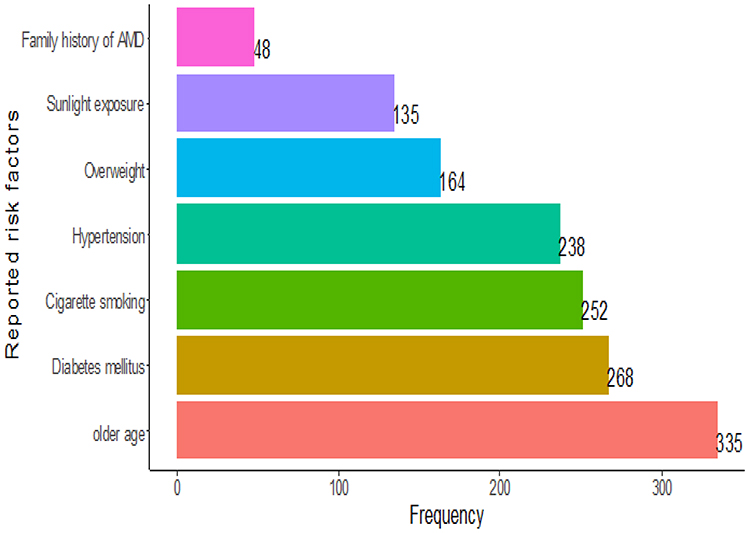 |
Figure 1 Types and frequency of reported risk factors of AMD by healthcare providers. |
However, more than one risk factors were also reported by study participants (Table 4).
 |
Table 4 Reported Risk Factors (More Than One) for AMD and Frequency by Healthcare Providers in Gondar City, Northwest Ethiopia, 2024 (n = 350) |
Factors Associated with Knowledge of AMD Risk Factors
In the bivariable regression analysis, male sex, having a master’s degree or higher, healthcare service durations of less than five years, working in non-clinical healthcare professions (those with no direct involvement with patients), receiving eye health-related training, having an eye check-up in the past year, working in specialized hospitals, and having hypertension or diabetes mellitus were statistically associated with knowledge of AMD risk factors at p < 0.20. These variables were included in the multivariable logistic regression model to determine the independent predictors of knowledge about age-related macular degeneration risk factors.
In the multivariable logistic regression, knowledge of AMD risk factors was significantly affected by male sex, healthcare service durations of less than five years and over ten years, receiving eye health-related training, and having hypertension. Males were 68% more likely (AOR: 1.68; 95% CI: 1.16, 2.43) to be knowledgeable about the risk factors of AMD compared to their female counterparts, controlling for all other determinants. Healthcare providers with less than five years of healthcare experience were 1.86 times more likely to be knowledgeable about AMD risk factors (AOR: 1.86; 95% CI: 1.23, 2.88) compared to those with six to ten years of experience. Conversely, those with over ten years of healthcare service were 43% less likely to be knowledgeable about AMD risk factors (AOR: 0.57; 95% CI: 0.34, 0.95). Additionally, healthcare providers who received eye health-related training were 91% more likely to be knowledgeable about AMD risk factors (AOR: 1.91; 95% CI: 1.23, 2.83) compared to those who did not receive such training. Furthermore, healthcare providers with a history of confirmed hypertension and diabetes mellitus were 2.28 times (AOR: 2.28; 95% CI: 1.52, 3.44) and 2.48 times (AOR: 2.48; 95% CI: 1.02, 6.27) more likely, respectively, to be knowledgeable about AMD risk factors (Table 5).
 |
Table 5 Bivariable and Multivariable Logistic Regression Analysis to Identfiy Factors Association with Knowledge of AMD Risk Factors Among Healthcare Providers in Ethiopia (n=350) |
Discussion
This study explored the knowledge of healthcare providers regarding the risk factors for AMD in public health facilities in northern Ethiopia. The results revealed that only a small percentage of providers had sufficient knowledge about AMD risk factors. Several factors influenced AMD risk factor knowledge including gender, years of healthcare services, participation in eye health training, and history of hypertension and diabetes mellitus.
The study revealed that only one-third of healthcare providers had adequate knowledge about the risk factors for AMD. This limited understanding may stem from a lack of eye health training for these providers. In fact, less than one-third (27.2%) reported receiving eye health-related training during their College education or while on the job. Given the critical role play in delivering health information and medication counseling to patients, the limited knowledge about AMD is concerning. These gaps in understanding represent missed opportunities for early detection and preventive care, particularly in Ethiopia, which faces a triple burden of diseases where noncommunicable diseases account for approximately 35%64 and around 60% of the population relies on public health facilities for care. However, this finding is more encouraging compared to a nationwide cross-sectional study conducted in Poland, which revealed that more than half of adults did not know the risk factors for AMD.65 This difference may be attributed to varying levels of awareness and knowledge about AMD itself. The current study supports this notion, as 57.7% of healthcare providers reported being aware of AMD, with 60% demonstrating fair to good knowledge of the condition. In contrast, only 54.3% of Polish adults were aware of AMD. This highlights a notable discrepancy in awareness levels, suggesting that may have more access to relevant information and training compared to the general population. One possible explanation for the better outcomes in our study is that it involved who have a higher knowledge demand and experience in health-related fields. For instance, a study from Beijing, China, found that 35% of participants with health-related work experience identified smoking as AMD risk factor.66 This suggests that increased exposure to health education may significantly enhance knowledge of AMD risk factors among healthcare providers. Furthermore, the higher proportion of healthcare providers aware of AMD risk factors can be attributed to the study’s focus on medical professionals who could greater access to information about AMD risk factors from different sources of information. A study conducted in the USA among undergraduate and graduate students showed that participants were generally able to recognize the links between various cancers and health risk behaviors that have been extensively covered in the media.67 In contrast, the findings from the current study are lower than those reported in other research. For instance, a study on the warning signs and risk factors to stroke among Nigerian nursing undergraduate students found that approximately 53.2%68 of participants had a good understanding of stroke risk factors. Similarly, another study involving twenty optometrists in Australia indicated that 65%69 were knowledgeable about AMD risk factors. Several factors may explain these discrepancies. First, differences in training programs and educational curricula between countries could lead to varying levels of knowledge among healthcare providers. In Nigeria and Australia, nursing and optometry students may receive more comprehensive training focused on specific health conditions, including stroke and AMD. Additionally, the focus of their respective studies may have heightened awareness and interest in those particular conditions. Another possible explanation is the varying prevalence and public health emphasis on different diseases. In regions where stroke and AMD are more prevalent or widely discussed in media and public health campaigns, might be more motivated to stay informed about these conditions. Despite the small proportion of healthcare providers knowledgeable about the risk factors for AMD, it is notable that a high percentage of participants recognized older age (95.7%) and cigarette smoking (72%) as significant risk factors. Similar findings have been reported in other studies. For example, a study from Saudi Arabia showed that 66.2% of adults identified age and 25.7% identified smoking as risk factors for cataracts.70 In a survey conducted among 385 residents in Beijing, only 35% recognized smoking as AMD risk factor.66 Additionally, a study on the general population in Singapore found that 38.5% and 36.7% of respondents identified age and smoking as risk factors for AMD, respectively.71 These findings suggest a general awareness of key risk factors among participants, even if overall knowledge of AMD is limited. Several explanations may account for this awareness. First, older age and smoking are widely discussed in public health campaigns and media, which can enhance recognition; second, the association of these risk factors with other well-known health conditions, such as cardiovascular diseases and lung cancer, may reinforce their significance in the minds of healthcare providers and the public and personal experiences or the prevalence of related health issues within communities may also influence awareness.
This study reveals an interesting finding regarding gender differences in knowledge about the risk factors for AMD. Specifically, males were found to be 68% (AOR: 1.68; 95% CI: 1.16 −2.43) more likely to be knowledgeable about these risk factors compared to females with the same profile. Understanding the reasons behind this disparity could be valuable for developing targeted educational interventions aimed at increasing knowledge among females, ultimately enhancing awareness and prevention efforts for AMD across all demographics. The observed discrepancy in knowledge about AMD risk factors between males and females may be because males might be more attuned to lifestyle-related risk factors, such as smoking, which could further enhance their overall knowledge about risks of AMD. Understanding factors for this gender gap is essential for developing targeted educational initiatives aimed at bridging the knowledge gap and improving awareness of AMD among all demographics. Gender differences in knowledge of risk factors for other eye diseases have also been reported in other studies. For example, a study among final-year medical students in Saudi Arabia found that male students had higher knowledge scores regarding the risk factors for diabetic retinopathy compared to their female counterparts.72 Additionally, gender emerged as a significant factor influencing awareness of common eye disease risk factors such as glaucoma and AMD in a nationwide survey conducted in Poland among adults.65 Varying perceptions of risk may impact knowledge, as males might be more likely to seek out information about conditions they view as more relevant or threatening. A significant body of research on risk suggests that women and men have different perceptions of risk.73
The findings from this study revealed a significant trend in healthcare providers’ knowledge AMD risk factors based on their years of experience. Specifically, providers with less than five years of healthcare experience were 1.86 times more likely (AOR: 1.86, 95% CI: 1.23–2.88) to possess knowledge about AMD risk factors compared to those with six to ten years of experience. In contrast, providers with over ten years of experience were found to be 43% less likely (AOR: 0.57; 95% CI: 0.34–0.95) to be knowledgeable about these risk factors. This trend is consistent with findings from a cross-sectional study conducted among pediatricians in Jeddah, where 56.5% of junior residents were aware of risks of retinopathy of prematurity,74 compared to only 6% of consultants. Additionally, evidence from Ireland indicates that knowledge of stroke risk factors was lowest among individuals aged 65 and older.75 These observations suggest that newer healthcare providers may be more engaged with current educational resources and updates, while more experienced providers may benefit from targeted training to refresh their knowledge on evolving health risks. This finding suggests that newer healthcare providers may benefit from more recent training and exposure to current guidelines and research related to eye health, while those with greater experience might be relying on outdated information or may not have received ongoing education about conditions like AMD. In this study, the duration of eye health-related training ranged from 1 to 18 years. Addressing this knowledge gap through targeted continuing education programs could help ensure that all healthcare providers are well-informed about important risk factors for AMD. However, this observation contrasts with another study that found knowledge scores among optometry practitioners increased with years of clinical experience.76 This discrepancy highlights the need for further investigation into the factors influencing knowledge retention and updates among experienced providers, emphasizing the importance of continuous professional development in the rapidly evolving field of eye health. This emphasis on training aligns with findings from other studies. For instance, research from the Democratic Republic of Congo showed that who received training on breast cancer were 1.9 times more likely to be knowledgeable about its risk factors.77 Additionally, a qualitative study in Fiji among community health workers indicated significant improvements in knowledge about both diabetes and diabetic retinopathy following training.78 Similarly, a study of non-ophthalmic healthcare providers in Riyadh, Saudi Arabia, identified insufficient periodic training in eye care (69%) and a lack of retinal evaluation training (49.6%)79 as key reasons for low knowledge levels regarding the management of diabetic eye conditions. These insights collectively highlight the importance of ongoing education and specialized training in enhancing healthcare providers’ knowledge and competence in eye health. The findings reveal that healthcare providers with a history of confirmed hypertension and diabetes mellitus were significantly more likely to be knowledgeable about AMD risk factors. Specifically, those with a history of hypertension were 2.28 times more likely to possess this knowledge (AOR: 2.28; 95% CI: 1.52 to 3.44), while providers with diabetes mellitus were 2.48 times more likely (AOR: 2.48; 95% CI: 1.02 to 6.27). These results suggest that personal health experiences may enhance awareness and understanding of conditions linked to AMD. Providers with these chronic conditions may be more attuned to the associated risk factors and the importance of early detection, leading to improved patient education and advocacy. This underscores the potential value of integrating personal health experiences into professional development, which could further enhance healthcare providers’ ability to inform and support patients at risk for AMD. The presence of chronic diseases has been reported to correlate with awareness of AMD risk factors. It can be hypothesized that older adults, who are at greater risk for both chronic diseases and eye conditions, may seek eye care more frequently and receive education from their primary care physicians or ophthalmologists.80 Chronic conditions like diabetes, hypertension, and dyslipidemia are established risk factors for eye diseases.81 Therefore, individuals with these conditions may be more informed about the potential eye complications associated with them, increasing awareness on eye diseases and their associated factors. Additionally, studies have shown that the presence of chronic diseases is a key factor linked to awareness of common eye diseases and the risk factors for glaucoma and AMD.65
Strength and Limitations
This is the first study which address the gap in the literature on the knowledge of healthcare providers regarding AMD in Ethiopia. Our study population included a range of healthcare professions, including nurses, medical doctors, pharmacists, health officers, midwifers working at three healthcare levels (health center, general hospital and specialized hospitals). This increases the generalisability of these findings. However, there are some limitations which should be considered in the interpretation of findings from the study. Firstly, the outcome definition in our study is somewhat based on a stricter criteria than previous studies which may result in underestimation of our estimate. Secondly, the study might be subject to the recall as the data is based on self-report and social desirability bias as the healthcare providers’ may expectation of knowledge themselves as knowledge about the subject matter. This study was only limited to risk factors of AMD and it did not address prevention and management knowledge among healthcare providers. Another potential limitation is that the study only included public health facility healthcare providers, but we do not believe this would affect the representativeness of our study findings as majority of the healthcare providers working in private health facilities in the study are those who work in public health facilities.
Conclusion
With over 70% of the healthcare providers having low knowledge of AMD risk factors, there is a dire need for public health educational programs to improve the level of knowledge about AMD in the healthcare provider population. Despite the ever increasing burden of AMD understanding among healthcare providers is limited. Only one out of three healthcare providers have sufficient knowledge regarding AMD risk factors. Improvements in AMD risk factor knowledge among healthcare providers can be brought about by incorporating this topic into the curriculum and continuing education courses supported with period refreshment trainings. Integrating advice for people with chronic diseases such as DM and hypertension could help to increases risk factors of knowledge on AMD. Further studies are recommended to examine the reasons for gender gap in risk knowledge related to AMD. Furthermore, evaluating the practice of eye checkup for AMD among healthcare providers is recommended and how risk factor knowledge affect eye checkup practices, and the extent of awareness on management and prevention of AMD should be investigated among this segment of the population including the sources of information.
Abbreviations
AMD, Age – Related Macular Degeneration; AOR, Adjusted Odds Ratio; DM, Diabetes Mellitus; COR, Crude Odds Ratio; CI, Confidence Interval; HTN, Hypertension; USD, United States Dollar.
Data Sharing Statement
Data can be obtained upon reasonable request. The datasets used and/or analyzed in this study are available from the corresponding author upon request.
Ethics Approval and Informed Consent
The study was carried out following the ethical standards of the University of Gondar, in accordance with local laws and institutional guidelines (Ref# AV/S10914), as well as the World Medical Association’s Declaration of Helsinki. The participants gave verbal consent to take part in the study before engaging in the research. As the study was deemed to involve minimal risk to the study participants and was designed to gather anonymous data on non-sensitive topics, the institutional review board decided verbal consent was sufficient to ensure participants’ rights and welfare without imposing unnecessary burden. This decision was approved by the University of Gondar IRB, which recognized the appropriateness of verbal consent in for this study. The verbal consent process was documented thoroughly, ensuring that all participants were fully informed about the study’s aims and their rights.
Acknowledgments
The authors thank all data collectors and supervisors for their dedicated work in the data collection. We acknowledge the study participants for their valuable time to take part in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The was no financial support for this research.
Disclosure
The authors declare that the research was conducted without any commercial or financial relationships that could be perceived as a potential conflict of interest.
References
1. Blasiak J, Sobczuk P, Pawlowska E, Kaarniranta K. Interplay between aging and other factors of the pathogenesis of age-related macular degeneration. Ageing Res Rev. 2022;81:101735. doi:10.1016/j.arr.2022.101735
2. Fleckenstein M, Keenan TD, Guymer RH, et al. Age-related macular degeneration. Nature Reviews Disease Primers. 2021;7(1):31. doi:10.1038/s41572-021-00265-2
3. Lim LS, Mitchell P, Seddon JM, Holz FG, Wong TY. Age-related macular degeneration. Lancet. 2012;379(9827):1728–1738. doi:10.1016/S0140-6736(12)60282-7
4. Wong WL, Su X, Li X, et al. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: a systematic review and meta-analysis. Lancet Glob Health. 2014;2(2):e106–e16. doi:10.1016/S2214-109X(13)70145-1
5. Stahl A. The diagnosis and treatment of age-related macular degeneration. Dtsch Arztebl Int. 2020;117(29–30):513. doi:10.3238/arztebl.2020.0513
6. Flaxman SR, Bourne RR, Resnikoff S, et al. Global causes of blindness and distance vision impairment 1990–2020: a systematic review and meta-analysis. Lancet Glob Health. 2017;5(12):e1221–e34. doi:10.1016/S2214-109X(17)30393-5
7. Joachim N, Mitchell P, Kifley A, Rochtchina E, Hong T, Wang JJ. Incidence and progression of geographic atrophy: observations from a population-based cohort. Ophthalmology. 2013;120(10):2042–2050. doi:10.1016/j.ophtha.2013.03.029
8. Zimmer Z, Jagger C, Chiu C-T, Ofstedal MB, Rojo F, Saito Y. Spirituality, religiosity, aging and health in global perspective: a review. SSM-Population Health. 2016;2:373–381. doi:10.1016/j.ssmph.2016.04.009
9. Mane A, Khandekar S, Fernandez K. India’s ageing population: geriatric care still in infancy. J Gerontol Geriatr Res. 2014;3:186.
10. United Nations Department of Economic and Social Affairs Population Division (2024). World population prospects 2024: ten key messages. 2024. Available from: https://www.un.org/development/desa/pd/.
11. Lissanewerk A, Hailu S, Minda A, Bekele M. Prevalence of age related macular degeneration and associated factors at a tertiary eye care center in Addis Ababa, Ethiopia. Ethiopian J Public Health Nutrition. 2021;4(2):118–122.
12. Abebe D, Tsegaw A. Pattern of vitreo-retinal diseases at University of Gondar tertiary eye care and training center, North-West Ethiopia. PLoS One. 2022;17(4):e0267425. doi:10.1371/journal.pone.0267425
13. Gebremichael G. Age related macular degeneration among patients visiting Jimma University department of ophthalmology, South West Ethiopia. EC Ophthalmol. 2022;13:98–107.
14. Tegegn MT, Assaye AK, Mersha GA. Proportion, causes and associated factors of blindness among adult patients attending tertiary eye care and training center in Ethiopia. Clin Optom. 2021;Volume 13:83–91. doi:10.2147/OPTO.S295626
15. Coleman HR, Chan -C-C, Ferris FL, Chew EY. Age-related macular degeneration. Lancet. 2008;372(9652):1835–1845. doi:10.1016/S0140-6736(08)61759-6
16. Thomas CJ, Mirza RG, Gill MK. Age-related macular degeneration. Med Clin North Am. 2021;105(3):473–491. doi:10.1016/j.mcna.2021.01.003
17. Fine SL, Berger JW, Maguire MG, Ho AC. Age-related macular degeneration. N Engl J Med. 2000;342(7):483–492. doi:10.1056/NEJM200002173420707
18. Evans JR. Risk factors for age-related macular degeneration. Prog Retinal Eye Res. 2001;20(2):227–253. doi:10.1016/S1350-9462(00)00023-9
19. Mitchell P, Liew G, Gopinath B, Wong TY. Age-related macular degeneration. Lancet. 2018;392(10153):1147–1159. doi:10.1016/S0140-6736(18)31550-2
20. Lynch AM, Patnaik JL, Cathcart JN, et al. Colorado age-related macular degeneration registry: design and clinical risk factors of the cohort. Retina. 2019;39(4):656–663. doi:10.1097/IAE.0000000000002023
21. Hernández-Zimbrón LF, Zamora-Alvarado R, Ochoa-de la paz L, et al. Age‐related macular degeneration: new paradigms for treatment and management of AMD. Oxid Med Cell Longev. 2018;2018(1):8374647. doi:10.1155/2018/8374647
22. Tomany SC, Wang JJ, Van leeuwen R, et al. Risk factors for incident age-related macular degeneration: pooled findings from 3 continents. Ophthalmology. 2004;111(7):1280–1287. doi:10.1016/j.ophtha.2003.11.010
23. Heesterbeek TJ, Lorés‐Motta L, Hoyng CB, Lechanteur YT, den Hollander AI. Risk factors for progression of age‐related macular degeneration. Ophthalmic Physiol Opt. 2020;40(2):140–170. doi:10.1111/opo.12675
24. Seddon JM, Willett WC, Speizer FE, Hankinson SE. A prospective study of cigarette smoking and age-related macular degeneration in women. JAMA. 1996;276(14):1141–1146. doi:10.1001/jama.1996.03540140029022
25. Age-Related Eye Disease Study Research Group. Risk factors for the incidence of advanced age-related macular degeneration in the age-related eye disease study (AREDS): AREDS report no. 19. Ophthalmology. 2005;112(4):533–9.e1. doi:10.1016/j.ophtha.2004.10.047
26. Flaxel CJ, Adelman RA, Bailey ST, et al. Age-related macular degeneration preferred practice pattern®. Ophthalmology. 2020;127(1):P1–P65. doi:10.1016/j.ophtha.2019.09.024
27. Schick T, Ersoy L, Lechanteur YT, et al. History of sunlight exposure is a risk factor for age-related macular degeneration. Retina. 2016;36(4):787–790. doi:10.1097/IAE.0000000000000756
28. Sui GY, Liu GC, Liu GY, et al. Is sunlight exposure a risk factor for age-related macular degeneration? A systematic review and meta-analysis. Br J Ophthalmol. 2013;97(4):389–394. doi:10.1136/bjophthalmol-2012-302281
29. Modenese A, Gobba F. Macular degeneration and occupational risk factors: a systematic review. Int Arch Occupational Environm Health. 2019;92(1):1–11. doi:10.1007/s00420-018-1355-y
30. Moon BG, Joe SG, Hwang J-U, Kim HK, Choe J, Yoon YH. Prevalence and risk factors of early-stage age-related macular degeneration in patients examined at a health promotion center in Korea. J Korean Med Sci. 2012;27(5):537. doi:10.3346/jkms.2012.27.5.537
31. Ersoy L, Ristau T, Lechanteur YT, et al. Nutritional risk factors for age‐related macular degeneration. Biomed Res Int. 2014;2014(1):413150. doi:10.1155/2014/413150
32. Chew EY, Lindblad AS, Clemons T; Group A-REDSR. Summary results and recommendations from the age-related eye disease study. Arch Ophthalmol. 2009;127(12):1678–1679. doi:10.1001/archophthalmol.2009.312
33. Age-Related Eye Disease Study 2 (AREDS2) Research Group. Lutein + zeaxanthin and omega-3 fatty acids for age-related macular degeneration: the age-related eye disease study 2 (AREDS2) randomized clinical trial. JAMA. 2013;309(19):2005–2015. doi:10.1001/jama.2013.4997
34. Chakravarthy U, Wong TY, Fletcher A, et al. Clinical risk factors for age-related macular degeneration: a systematic review and meta-analysis. BMC Ophthalmol. 2010;10(1):1–13. doi:10.1186/1471-2415-10-31
35. Brody BL, Gamst AC, Williams RA, et al. Depression, visual acuity, comorbidity, and disability associated with age-related macular degeneration. Ophthalmology. 2001;108(10):1893–1900. doi:10.1016/S0161-6420(01)00754-0
36. Schultz NM, Bhardwaj S, Barclay C, Gaspar L, Schwartz J. Global burden of dry age-related macular degeneration: a targeted literature review. Clin Ther. 2021;43(10):1792–1818. doi:10.1016/j.clinthera.2021.08.011
37. Gopinath B, Liew G, Burlutsky G, Mitchell P. Age-related macular degeneration and 5-year incidence of impaired activities of daily living. Maturitas. 2014;77(3):263–266. doi:10.1016/j.maturitas.2013.12.001
38. Tsang JY, Wright A, Carr MJ, et al. Risk of falls and fractures in individuals with cataract, age-related macular degeneration, or glaucoma. JAMA Ophthalmol. 2024;142(2):96–106. doi:10.1001/jamaophthalmol.2023.5858
39. Casten RJ, Rovner BW. Update on depression and age-related macular degeneration. Curr Opin Ophthalmol. 2013;24(3):239–243. doi:10.1097/ICU.0b013e32835f8e55
40. Lane J, Rohan EM, Sabeti F, et al. Impacts of impaired face perception on social interactions and quality of life in age-related macular degeneration: a qualitative study and new community resources. PLoS One. 2018;13(12):e0209218. doi:10.1371/journal.pone.0209218
41. Wood JM, Black AA, Mallon K, Kwan AS, Owsley C. Effects of age-related macular degeneration on driving performance. Invest Ophthalmol Visual Sci. 2018;59(1):273–279. doi:10.1167/iovs.17-22751
42. Woo SJ, Park KH, Ahn J, et al. Cognitive impairment in age-related macular degeneration and geographic atrophy. Ophthalmology. 2012;119(10):2094–2101. doi:10.1016/j.ophtha.2012.04.026
43. Choi S, Jahng WJ, Park SM, Jee D. Association of age-related macular degeneration on Alzheimer or Parkinson disease: a retrospective cohort study. Am J Ophthalmol. 2020;210:41–47. doi:10.1016/j.ajo.2019.11.001
44. McGuinness MB, Karahalios A, Finger RP, Guymer RH, Simpson JA. Age-related macular degeneration and mortality: a systematic review and meta-analysis. Ophthalmic Epidemiol. 2017;24(3):141–152. doi:10.1080/09286586.2016.1259422
45. Di Carlo E, Augustin AJ. Prevention of the onset of age-related macular degeneration. J Clin Med. 2021;10(15):3297. doi:10.3390/jcm10153297
46. Jonas JB, Bourne RR, White RA, et al. Visual impairment and blindness due to macular diseases globally: a systematic review and meta-analysis. Am J Ophthalmol. 2014;158(4):808–815. doi:10.1016/j.ajo.2014.06.012
47. Apte RS; Apte RS. Age-related macular degeneration. N Engl J Med. 2021;385(6):539–547. doi:10.1056/NEJMcp2102061
48. Tran E, Nayeni M, Shah N, Malvankar-Mehta MS. The effects of age-related macular degeneration on work productivity: a meta-analysis. Eur J Ophthalmol. 2024;34(3):641–648. doi:10.1177/11206721231185808
49. Chew EY, Clemons TE, Agrón E, et al. Ten-year follow-up of age-related macular degeneration in the age-related eye disease study: AREDS report no. 36. JAMA Ophthalmol. 2014;132(3):272–277. doi:10.1001/jamaophthalmol.2013.6636
50. Apte RS, Chen DS, Ferrara N. VEGF in signaling and disease: beyond discovery and development. Cell. 2019;176(6):1248–1264. doi:10.1016/j.cell.2019.01.021
51. Martin DF, Maguire MG, Fine SL, et al. Ranibizumab and bevacizumab for treatment of neovascular age-related macular degeneration: two-year results. Ophthalmology. 2012;119(7):1388–1398. doi:10.1016/j.ophtha.2012.03.053
52. Heier JS, Brown DM, Chong V, et al. Intravitreal aflibercept (VEGF trap-eye) in wet age-related macular degeneration. Ophthalmology. 2012;119(12):2537–2548. doi:10.1016/j.ophtha.2012.09.006
53. Hoeben M, Langelaan M, Klevering J, Keunen JE, van Rens GH. Low vision rehabilitation for better quality of life in visually impaired adults. Cochrane Database Syst Rev. 2020;1(1). doi:10.1002/14651858.CD006543.pub2
54. Group A-REDSR. A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report No. 8. Arch Ophthalmol. 2001;119(10):1417–1436. doi:10.1001/archopht.119.10.1417
55. Study A-RED, Group R. Lutein+ zeaxanthin and omega-3 fatty acids for age-related macular degeneration: the age-related eye disease study 2 (AREDS2) randomized clinical trial. 2013.
56. Salimiaghdam N, Riazi-Esfahani M, Fukuhara PS, Schneider K, Kenney MC. Age-related macular degeneration (AMD): a review on its epidemiology and risk factors. Open Ophthalmol J. 2019;13(1):90–99. doi:10.2174/1874364101913010090
57. Scheffer M, Menting J, Boeije H, van Nispen R, van Dulmen S. Understanding healthcare communication in age-related macular degeneration care: a mixed-methods review of patients’ perspectives. Survey Ophthalmol. 2024;69(4):646–660. doi:10.1016/j.survophthal.2024.03.002
58. Wang Y, Zhong Y, Zhang L, et al. Global incidence, progression, and risk factors of age-related macular degeneration and projection of disease statistics in 30 years: a modeling study. Gerontology. 2022;68(7):5721–5735. doi:10.1159/000518822
59. Shamous T, Obeid K, Salman A. Knowledge and awareness about age-related macular degeneration among students of the Syrian Private University. 2022.
60. Khan MA, Mahmood A, Saeed M, Ali SA, Imtiaz F. Age-related macular degeneration understanding and awareness in Pakistan: a realistic epidemiological survey. 2023.
61. Bloom BS. Learning for mastery. instruction and curriculum. regional education laboratory for the Carolinas and Virginia, topical papers and reprints, number 1. Evaluation Comment. 1968;1(2):n2.
62. Assem AS, Tegegne MM, Alemu DS, Woredekal AT, Tefera TK. Knowledge about diabetic retinopathy, eye check-up practice and associated factors among adult patients with diabetes mellitus attending at debark hospital, Northwest Ethiopia. BMC Ophthalmol. 2020;20(1):1–11. doi:10.1186/s12886-020-01730-4
63. R Core Team (2024). _R: a language and environment for statistical computing_. R Foundation forStatistical Computing, Vienna, Austria. Available from: https://www.R-project.org/.
64. Ethiopian Ministry of Health. Fact Sheet- Ethiopia 2020. Available from: https://www.moh.gov.et/index.php/en/fact-sheets?language_content_entity=en.
65. Kamińska A, Pinkas J, Wrześniewska-Wal I, Ostrowski J, Jankowski M. Awareness of common eye diseases and their risk factors-A nationwide cross-sectional survey among adults in Poland. Int J Environ Res Public Health. 2023;20(4).
66. Zhang CX, Zhang GM, Ma N, Xia S, Yang JY, Chen YX. Awareness of Age-related macular degeneration and its risk factors among Beijing residents in China. Chin Med J. 2017;130(2):155–159. doi:10.4103/0366-6999.197994
67. Merten JW, Parker A, Williams A, King JL, Largo-Wight E, Osmani M. Cancer risk factor knowledge among young adults. J Cancer Educ. 2017;32(4):865–870. doi:10.1007/s13187-016-1093-3
68. Kankaya H, Yesilbalkan OU. Awareness of risk factors and warning signs of stroke among nursing students: results from questionnaire. Niger J Clin Pract. 2021;24(5):729–734. doi:10.4103/njcp.njcp_181_19
69. Gocuk SA, Lee JH, Keller PR, et al. Clinical audit as an educative tool for optometrists: an intervention study in age-related macular degeneration. Ophthalmic Physiol Opt. 2021;41(1):53–72. doi:10.1111/opo.12754
70. Ghulaysi S, Abuallut I, Alaqsam AA, et al. Exploring awareness of cataract and associated risk factors: a cross-sectional study among the adult population in Jazan, Saudi Arabia. Medicine. 2024;103(25):e38335. doi:10.1097/MD.0000000000038335
71. Sanjay S, Neo HY, Sangtam T, et al. Survey on the knowledge of age-related macular degeneration and its risk factors among Singapore residents. Clin Exp Ophthalmol. 2009;37(8):795–800. doi:10.1111/j.1442-9071.2009.02153.x
72. Al Wadaani FA. The knowledge attitude and practice regarding diabetes and diabetic retinopathy among the final year medical students of king faisal university medical College of Al Hasa region of Saudi Arabia: a cross sectional survey. Niger J Clin Pract. 2013;16(2):164–168. doi:10.4103/1119-3077.110133
73. Gustafson PE. Gender differences in risk perception: theoretical and methodological perspectives. Risk Anal. 1998;18(6):805–811. doi:10.1023/B:RIAN.0000005926.03250.c0
74. Al Attas K, Roblah T, AlSwealh S. Knowledge of retinopathy of prematurity among pediatricians in King Abdulaziz University hospital in Jeddah: a cross-sectional study. BMC Ophthalmol. 2023;23(1):99. doi:10.1186/s12886-023-02829-0
75. Hickey A, Holly D, McGee H, Conroy R, Shelley E. Knowledge of stroke risk factors and warning signs in Ireland: development and application of the stroke awareness questionnaire (SAQ). Int J Stroke. 2012;7(4):298–306. doi:10.1111/j.1747-4949.2011.00698.x
76. Saravanan S, Negiloni K, Asokan R. Assessment of knowledge, attitude, and practice of glaucoma among different cadres of optometrists. Indian J Ophthalmol. 2022;70(6):2014–2019. doi:10.4103/ijo.IJO_3168_21
77. Sulu SMM, Mukuku O, Sulu AMS, Massamba BL, Wembonyama SO. Knowledge of risk factors and early detection methods toward breast cancer among healthcare workers in Kinshasa, Democratic Republic of the Congo. Cancer Rep. 2024;7(4):e2067. doi:10.1002/cnr2.2067
78. Ram S, Mohammadnezhad M, Ram K, Dalmia P, Pal M. Impact of diabetic retinopathy awareness training on community health workers’ knowledge and referral practices in Fiji: a qualitative study. Rural Remote Health. 2022;22(2):6976. doi:10.22605/RRH6976
79. Abu-Amara TB, Al Rashed WA, Khandekar R, et al. Knowledge, attitude and practice among non-ophthalmic health care providers regarding eye management of diabetics in private sector of Riyadh, Saudi Arabia. BMC Health Serv Res. 2019;19(1):375. doi:10.1186/s12913-019-4216-9
80. Voleti VB, Hubschman JP. Age-related eye disease. Maturitas. 2013;75(1):29–33. doi:10.1016/j.maturitas.2013.01.018
81. SanGiovanni JP, Chew EY, Clemons TE, et al. The relationship of dietary lipid intake and age-related macular degeneration in a case-control study: AREDS report no. 20. Arch Ophthalmol. 2007;125(5):671–679.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.