")
Back to Journals » Journal of Healthcare Leadership » Volume 17
Developing Primary Health Network Employee’s Capability in Health and Social Care Commissioning
Authors Liang Z , Martin A, Turner CL
Received 18 December 2024
Accepted for publication 28 May 2025
Published 3 June 2025 Volume 2025:17 Pages 241—258
DOI https://doi.org/10.2147/JHL.S511151
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Russell Taichman
Zhanming Liang,1 Amanda Martin,2 Catherine Louise Turner2
1College of Business, Law and Governance, James Cook University, Townsville, QLD, Australia; 2The Hunter New England and Central Coast Primary HealthNetwork, Broadmeadow, NSW, Australia
Correspondence: Zhanming Liang, College of Business, Governance & Law, James Cook University, Townsville, QLD, Australia, Email [email protected]
Introduction: Primary care has strategic importance in Australia’s complex health system, attracting one-third of the country’s health budget. Primary Health Networks (PHNs), established in 2015 to act as commissioners for non-hospital health and social care across Australia, enable a more comprehensive health planning approach to identify and prioritise service gaps and commission appropriate health services. Hence, building PHNs’ capability in health commissioning is critical to maximising health outcomes of the Australian population.
Objective: This study was conducted to identify the skill development needs of PHNs employees to lead and manage commissioning, and strategies to build commissioning capabilities across PHNs.
Methods: A multiphase mixed-method approach was used, including an anonymous online survey and two focus group discussions.
Results: The health commissioning practices of PHNs directly affect PHN staff’s confidence (Pearson’s r=0.484, p< 0.001) and self-perceived competence in their commissioning practices (Pearson’s r=0.335, p< 0.001). This study confirms that systematic upskilling commissioning among PHN employees, focusing on the commissioning cycle, complex healthcare environments, and data management, is required to improve their capabilities. This highlights the importance of organisational support in strengthening the six key factors for effective commissioning.
Discussion: The enhancement of PHNs’ capability in health commissioning should be centered around employees’ capability building guided by the proposed PHN health commissioning capability building model. Organisation investment in performance monitoring and enhancement, organisations’ multi-strategy approach towards internal support and development, and external learning and development opportunities are the three key pillars.
Conclusion: Enhancing robust commissioning processes and strengthening leadership capabilities in health commissioning are essential for PHNs to meet the evolving healthcare needs of the population. Effective commissioning requires skilled and confident teams, systematic upskilling, organisational support, and strategic approaches to address challenges, deliver high-quality primary care, and improve population health outcomes. Building PHNs’ commissioning capability requires a systematic and progressive skill development approach that prioritises a staff-centred model.
Keywords: commissioning, skills, competency, primary health, primary health networks, capacity building
Introduction
Australia was ranked third in overall healthcare system performance among OECD countries by the Commonwealth Fund in 2021.1,2 Some proven advantageous features of the Australian health system include universal health care coverage (Medicare), a mixture of public and private health insurance coverage, pharmaceutical benefit schemes, and comparatively well-coordinated primary health.3 Well-designed primary healthcare plays a key role in the provision of continuation of care and support for chronic disease management and is also key to a resilient healthcare system that is prepared for and responsive to crisis and challenges.2 The funding and organisation of primary healthcare varies across countries, such as the publicly funded but privately delivered system in the UK, publicly funded out-of-pocket from care recipients in Canada, mixed public and private provision in Australia, and primarily privately funded healthcare in the US. A well-trained workforce is required for these systems to function and be sustainable. Identifying skill gaps aligned with relevant core competencies ensures that the human resource aspect of each of these health systems operates to deliver appropriate care and services regardless of the sector - private, public, tertiary, or primary care.
Primary Health Networks in Australia
In Australia, primary health care, provided by a mixture of public and private businesses for profit and non-profit entities, includes care that is unrelated to hospital visits, such as medical services provided in general practice subsidised by Medicare or publicly funded community health and social services, mental health and drug and alcohol services, and maternal and child health services. In 2021–22, approximately 1/3 of the overall health spending was on primary health care.4 The Primary Health Networks were established in 2015 to address a number of challenges facing the the Australian primary care. These challenges included the complexity of funding arrangements and difficulties in the coordination of multilevel service providers, which signified a fragmented system that was difficult for consumers to navigate and access.5 To streamline non-hospital-based health services, enhance care coordination, and improve the effectiveness and efficiency of primary health care tailored to the needs of the community, 31 Primary Health Networks (PHN) were established across Australia in July 2015. Primary Health Networks are independent nonprofit organisations funded by the Australian Government.6,7 Primary Health Networks have a remit to act as services commissioners, meaning that unless significant market failure exists, they ‘do not provide health services but use a comprehensive health planning approach to identify and prioritise service gaps, and to commission appropriate health services’8 in the respective catchment areas.
Primary Health Network commissioning across Australia is guided by the Commissioning Framework (https://www.health.gov.au/our-work/phn/what-PHNs-do) established by the Australian Government Department of Health and Aging (DoHAC) to ensure approaches adopted for the PHN program deliver ‘consistent, comparable and measurable outputs and outcomes’.9 This framework has guided the development of commissioning frameworks adopted by individual PHN such as in Figure 1, a commissioning framework (https://thephn.com.au/what-we-do/commissioning-2) developed by the Hunter New England and Central Coast PHN – one of the largest PHNs in Australia. The ability of PHNs in fully implemented each dimension such as need assessment, annual planning, and prioritising, monitoring and evaluating commissioning activities is crucial to achieving health outcomes for the population that they serve. Assessing and prioritising local primary health needs is the fundamental first step of the commissioning cycle which provides evidence to guide PHNs in determining the type of services and associated outcomes needed, by which service providers and how such services should be funded. Hence, effective stakeholder partnerships and engagement are critical to commissioning health and social care.
 |
Figure 1 PHN commissioning framework. Note: Reprinted with permission from Primary Health Network. Available from: https://thephn.com.au/what-we-do/commissioning-2. |
Based on assessed and prioritised health needs, PHN commissioning focuses on three primary functions: 1) coordinating and integrating local health care services, 2) commission primary care services, and 3) building the capacity of local primary care service providers.10 Primary Health Networks commission local service providers to deliver services in a number of areas, such as mental health and suicide prevention, alcohol and other drugs, health services in aged care, Aboriginal and Torres Strait Island health, health workforce, emergency response, domestic, family, and sexual violence support, and medical urgent care.11 As an integral part of the health system, PHNs’ success rely on how well they work, how well they commission primary health services, and how well they work with other parts of the health system. Essential to this is the skills and structures in place to recruit, train, and build on the core competencies of the PHNs’ own workforces.
Health and Social Care Commissioning and Its Success
Commissioning initially emerged in the UK in the 1980s; like contracting, it has become a common model for engaging healthcare organisations in the provision of health and social care in many other countries.12 The fundamental difference between commissioning and contracting models is that commissioning includes a health needs assessment for a population, which determines the types of services to be commissioned by external service providers.13 Commissioning can be defined as ‘the process of translating aspirations and needs, by specifying and procuring services for the local population, into services for users’14 and ‘the process of assessing needs, planning and prioritising, purchasing and monitoring health services, to get the best health outcomes’ (NHS, 2023). Commissioning in the health and social care sectors aims to improve population health, reduce inequalities, enhance consumer experience,15 and ‘target gaps in health status, and improve health equity’.16
A rapid review of the impact of commissioning, conducted in 2016, found that the identified benefits of health commissioning in the UK, US, and some European countries are mainly on improved efficiencies of service funding and enhanced value of services.17 A clear policy framework of national and regional priorities that defines agreed targets for commissioning agencies and collaborative partnerships and engagement with local service providers in developing a needs assessment to ensure strategic priority alignments is said to be a critical success factor in health and social care commissioning.17,18 Knowledge of the employees involved in commissioning and the time invested in working collaboratively with service providers throughout the commissioning process is also key to ensuring that commissioned services meet identified needs and achieve planned outcomes.19 Other key success factors include the competencies of local commissioners and providers in local decision-making management, clear governance and accountability, project management and leadership.17,20
Building PHN’s Capacity – The Conceptual Framework
Capacity building refers to ‘an ongoing evidence-driven process to improve the ability of an individual, team, organisation, network, sector, or community to create measurable and sustainable results’21 and ‘the development of knowledge, skills, commitment, structures, systems, and leadership to enable effective health promotion’.22 In the healthcare context, organisational capacity refers to the level and potential of an organisation’s capability to deliver effective and efficient health services that meet patient expectations and the needs of the population it serves. It can also be understood as an organisation’s capability to capture external opportunities23 and rapidly translate knowledge/research evidence into health practice24 Hence, building an organisation’s capacity is about the enhancement of core internal aspects that affect the function of the organisation, such as resources, structure and processes, infrastructure, employees’ knowledge and skills, organisational culture, leadership, management and governance.25 In addition to focusing on developing individuals’ capabilities, organisations should enhance their abilities to address local health issues, improve practices and infrastructure, and enhance capabilities to engage in evidence-informed interventions.25,26 Potter and Brough (2004)26 described that systemic capacity-building is required to meet the capacity-building needs of the nine internal components presented in Figure 2.
 |
Figure 2 Conceptual framework for organisation capacity. Note: Data from Potter C and Brough R.26 |
Considering the functions of commissioning as discussed earlier and guided by the Potter and Brough (2004) framework, the following three pillars are fundamental to maximising health and social care commissioning outcomes: transparency and efficiency in the commissioning processes, efforts in encouraging innovative ideas, and investment in supporting and ensuring that PHN employees are equipped with the skills critical to fulfilling their responsibilities. Therefore, developing an understanding of the skill development needs of PHN employees responsible for and/or involved in designing, leading, and managing the commissioning process implemented by PHNs is the initial step in building the PHN’s commissioning capacity. Engaging employees in co-designing professional development opportunities can ensure that appropriate support and targeted professional development opportunities are offered27 which can systematically improve their capability and enhance PHN’s capacity. It is also critical to ensure the relevance of the design and to encourage employee commitment to skill development. Most importantly, improving employee capability takes many forms; skill development is only one of the many elements of transformational adult-learning.28,29 Therefore, organisations’ efforts to support and enable employees to excel in their jobs and embed capacity-building efforts in employees’ daily jobs cannot be overlooked.
Focus of the Project and Paper
The overall project aimed to clarify the role of PHN’s in building employees’ capability to design and lead the health and social care commissioning process by investigating the following research questions.
- Does PHNs’ current commissioning practices and capacities affect employees’ confidence in their commissioning practices and competence?
- What are the skill development needs of PHN employees in effectively leading and managing the commissioning process, and how can these skills be developed?
- What improvements are required for PHNs to develop and support their employees and improve the current PHN commissioning processes?
The identification of skill gaps and the building of capabilities beyond the clinical skills needed to deliver healthcare are the focus of the current study, particularly the exploration of the capabilities needed by those undertaking health and social care commissioning in the primary care sector of the Australian healthcare system.
Materials and Methods
The project adopted a mixed-method design, comprising an online survey and focus group discussions (FGDs). Both methods partially and fully investigated the research questions. The focus group discussions also played a role in verifying some of the information such as perception of current commissioning practices and strengths and required improvements identified in the online survey and added depth to the findings by delving into participants’ actual experiences. The online survey identified skills development needs of the participants which were further discussed at the focus group to guide confirming professional development and support direction.
Online Survey
An online survey was conducted in May 2024 using Qualtrics software. The survey participants were as follows.
- Core employees, with employee management responsibilities, from eight of the 11 PHNs in NSW/ACT, are responsible for the overall commissioning processes.
- Core employees, without employee management responsibilities, from eight of the 11 PHNs in NSW/ACT, who are involved in supporting the commissioning process.
In addition to collecting information on participants’ positions, number of years working in similar positions, and qualifications, the online survey also collected data from the following four sections:
- PHN’s current commissioning practices
- Evidence-based strategic planning (4 items)
- Stakeholder engagement in planning (6 items)
- Time investing in commissioning (3 items)
- Capability in commissioning (3 items)
- PHN employee’s self-confidence in
- Planning and commissioning practice (6 items)
- Self-confidence in assessing needs and using evidence (4 items)
- Professional development and support need of PHN employees (9 items)
- PHN employees’ self-assessed competence in demonstrating core behaviours essential to their roles (30 items).
The questions included in sections one–three were developed based on evidence from the literature and recommended health commissioning practices, as discussed in the introduction. The questions in section four included 30 management competency behavioural items from the validated MCAP tool.30,31 Four different scales were used in the survey (Table 1). All questions in the survey were developed to understand the PHN staff’s current practice and perception at the time of the survey, rather than the change of practice and competency overtime. The actual survey questionnaire is included as Appendix 1.
 |
Table 1 Four 7-Point Likert Scales Used in the Online Survey |
Focus Group Discussions
Online FGDs were held via Microsoft Teams in July 2024, with core management employees responsible for the overall commissioning processes and non-management employees who supported the commissioning process from different PHNs in the NSW/ACT. A detailed schedule for each FGD was developed using a rigorous process before conducting the focus group. The schedules of the two FGD are attached to the appendices. The process included
- Initial discussions between the facilitator, note taker, and project principal investigator prior to drafting each focus group schedule to ensure that all questions included in the schedule could comprehensively answer the research questions.
- seeking input from representatives of PHNs on the draft focus group schedule to ensure all questions are appropriate and relevant to the PHN context, and
- Final preparation meeting prior to each focus group to ensure that the team conducting the focus group was on the same page. This is particularly important to ensure rich discussions through skillful facilitation and accurate notetaking.
Key questions asked during the FGDs included
- Can you share your experiences with the commissioning work process from service providers that have worked well? As we talk through your examples, can you identify the factors that enable the various aspects of commissioning to work effectively?
- In your view, what do you think are the strengths of this commissioning process? What aspects need to be addressed? What do you think needs to be done to achieve such improvements?
- The commissioning process involved several steps. Which steps or aspects are more difficult to manage, based on your experience? What are your suggestions on what your PHN can do to make your job easier?
Sampling and Recruitment
Purposive sampling was used in this study. Seven of the 11 PHNs across the NSW and ACT in Australia agreed to participate in the study. Management and non-management employees working at the 11 PHNs were invited to participate in an online survey. The Australian Bureau of Statistics tool was used to calculate the minimum sample size being 52: (https://www.abs.gov.au/websitedbs/D3310114.nsf/home/Sample+Size+Calculator) with a 95% confidence interval, 5% margin of error, and the assumption that all staff have good understanding of PHN’s current planning, stakeholder engagement and commissioning practice. Further considering that 1) 30 or more samples were considered sufficient to answer the survey questions based on the Central Limit Theorem and 2) 30 is the minimum sample size for a Spearman correlation test to obtain reliable results, 52 or more valid completion of the survey should be regarded as adequate for the study. An Email invitation containing the participant information sheet and survey link was sent to potential participants by the commissioning manager (or equivalent) of each PHNs. Implied consent was obtained from each of the online survey participants by adding a informed consent page at the beginning of the online questionnaire. At the end of the online survey with PHN employees, the participants who completed the survey were asked whether they would like to participate in FGDs. Participants who ticked ‘yes, I would like to participate in one of the focus groups, were then directed to a separate online link, allowing them to provide their consent to participate in the FGD and their names, positions (management vs non-management), and Email addresses. This link also provides several dates and times for the proposed FGDs, allowing them to indicate their availability. The purpose of creating a separate link was to protect the anonymity of the survey responses. Once the date and time that suited the majority of PHN management employees or PHN non-management employees were identified, a calendar invitation, together with a link to a Microsoft Teams virtual meeting, was sent to management and non-management employees. The targeted number of participants for each FGDs was between 8 and 12, which is the ideal number for achieving data saturation and virtual FGD.32,33
Ethical Considerations
Ethics approval was received on 23 May 2024 from the James Cook University Human Research Ethics Committee (approval H9451; expiry 30 September 2024). For the online survey, no name or other identifiable personal details were collected making the survey completely anonymous. For the focus group discussion, no name, position title, or name of the organisation was recorded during the focus group discussions. Instead, a code was created for the focus group transcript to maintain participants’ anonymity. No payment or remuneration was provided for the FGD participation.
Data Collection and Analysis
After being downloaded from the Qualtrics website in Microsoft Excel, the survey data were checked for completion and errors. Questionnaires with missing data from one or more complete sections were excluded from analysis using IBM SPSS Statistics version 29.0. The mean of each question from all employees, management employees, and non-management employees was calculated. A t-test was performed to test the statistical significance of the mean scores of the management and non-management employees. Univariate analyses including tests for normality were performed. Correlations between PHN employees’ confidence in their own health commissioning practices, PHN employees’ self-assessed competency, and PHNs’ current and capacity in health commissioning practices were tested using Pearson’s correlation coefficient, with the alpha level of significance set at 0.05.
Two focus groups were conducted using Microsoft Teams (TEAMs), with video recording and transcription enabled. Key points from the discussions on each question were captured through note taking. Transcriptions were used to verify the notes and check for possible missing key points. Both the focus groups were conducted by a professional facilitator. The principal researcher (ZL) attended both focus groups as observer and for quality assurance. One research officer (LK) also played the role of notetaker. Each focus group took approximately 120 minutes to complete. Consolidated criteria for reporting qualitative research (COREQ) were applied to meet the recommended qualitative data reporting standards.34 Participants were provided with the opportunity to request a copy of the notes taken from the FG for further comments. Thematic analysis was then conducted on the key points captured from the focus group to develop concepts, categories, and themes guided by Braun and Clarke’s (2019) six-phase reflexive thematic analysis.35
Results – Online Survey
In total, 62 participants completed the survey excluding two who did not complete more than half of the survey questions, which yielded a response rate of approximately 35.6%. Among the 62 participants, 24 were management employees and 38 were non-management employees.
PHNs and Employee’s Planning and Commissioning Practices
Participants were provided with 26 items to rank, using the 7-point agreement scale, in relation to PHNs’ evidence-based strategic planning, stakeholder engagement in planning, time invested in commissioning and capability in commissioning, and PHN employees’ self-confidence in planning and commissioning practice, assessing needs, and using evidence. Figure 3 presents the mean scores for each section for management employees, non-management employees, and all employees. The results show that the mean score received for each of the sections from management employees was consistently higher than that from non-management employees. The differences between these two groups of participants were not statistically significant, except in section two - PHNs’ stakeholder engagement in planning (P0.019).
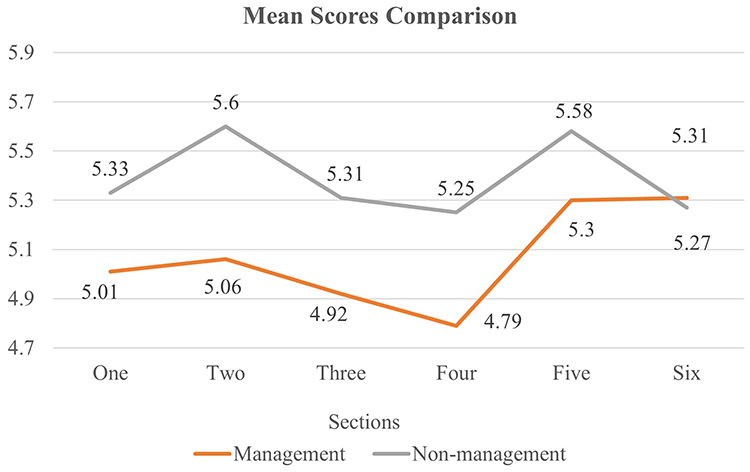 |
Figure 3 Mean scores comparative view. Section one PHN’s Evidence-based strategic planning. Section two PHN’s stakeholder engagement in planning. Section three PHN’s time investing in commissioning. Section four PHN’s capability in commissioning. Section five Self-confidence in own planning and commissioning practice. Section six Self-confidence in assessing needs and using evidence. |
To best understand the PHN employees’ views of the current PHN and their own commissioning practices, agreement (agree or strongly agree) from the proportion of employees may be more accurate. Figure 4 presents the proportion of management and non-management employees who collectively agreed or strongly agreed with the statements in each section ranging between 15.8–28.9% for management employees and 29.1% - 37.5% for non-management employees.
 |
Figure 4 Proportion of participants chose a score of 6 or 7. Section one PHN’s Evidence-based strategic planning. Section two PHN’s stakeholder engagement in planning. Section three PHN’s time investing in commissioning. Section four PHN’s capability in commissioning. Section five Self-confidence in own planning and commissioning practice. Section six Self-confidence in assessing needs and using evidence. |
Correlation Between PHN’s Health Commissioning Practices, PHN Employee’s Confidence and Self-Perceived Competence
Pearson’s correlation tests confirmed that the following did not have a significant effect on PHN employees’ confidence in their commissioning practices and self-perceived competency.
- With or without a master’s degree, the Mann–Whitney U-test p-value was 0.572 vs 0.472, respectively.
- Number of years working at a PHN: Pearson’s p-value of 0.677 vs 0.119 (management employees) or 0.885 (non-management employees)
- With or without management responsibilities: Pearson’s p value of 0.752 vs Mann–Whitney U-test of 0.753.
Pearson’s correlation tests confirmed a significant positive correlation between a PHN’s current commissioning practice and PHN employees’ confidence in their own commissioning practice and competency with p-value <0.001 and 0.012 respectively. Details scores of the tests are detailed in Table 2. When testing the correlations for management and non-management employees separately, the results vary.
 |
Table 2 Correlation Matrix |
Pearson’s correlation test further showed a significantly positive correlation between PHN employees’ average scores for self-assessed competency and average scores for confidence in their own health commissioning practices (P <0.001). When testing the correlation between management and non-management employees, a significant positive correlation remains. Figure 5 shows the positive correlations between three factors: PHN practice, PHN employees’ confidence in their own practice, and competency.
 |
Figure 5 PHN’s capacity affecting PHN employee’s perception. Abbreviation: PHN, Primary Health Networks. |
Importance of Professional Development and Support
Participants were also asked to indicate the importance of each of the ten professional development and support to improve their performance in their current role and/or for future career advancement at PHN. The following five among the provided choices were perceived as important or very important by no less than 2/3 of participants:
- A series of comprehensive training progressively developing skills relevant to health commissioning (77%).
- Regular team meetings to share ideas, discuss problems, and identify solutions (75%).
- Allocating self-study time in my workload (75%).
- Regular coaching by experienced colleague at my PHN (69%).
- More opportunities to attend networking activities (ie network meetings, communities of practice, and curated learning where employees from other PHNs are present) (66%).
- Targeted training using a problem-based approach provided externally (63%).
Competence in Demonstrating Various Skills
Thirty behavioural items associated with evidence-based decision-making, leadership, change management, operation and resource management, and personal and interpersonal skills were provided to participants to rank based on their perceived competence level. Overall, the mean scores for the 30 behavioural items ranged between 3.88 and 6.5 for management employees and between 4.38 and 6.58 for non-management employees (Figure 6). There was no significant difference between the mean scores received for management and non-management employees for each of the 30 behavioural items, with the Mann p-value ranging from 0.213 to 1.
 |
Figure 6 Self-assessed competence level of behavioral items. |
To understand the self-perceived strengths and weaknesses of the employees, the proportion of management (ranging between 28% and 91%) and non-management employees (ranging between 25% and 100%) who chose a score of 6 (competent) or 7 (very competent) was calculated (Figure 7). There was no difference in the proportion of management and non-management employees choosing 6 or 7 for each of the 30 items, with a Mann’s p-value ranging between 0.095 and 1.
 |
Figure 7 Proportion of employee choosing the score of 6 (competent) or 7 (very competent). |
Overall, ten items were given a score of 6 or 7 by less than 50% of management and non-management employees respectively as detailed in Table 3, which could be perceived as skill weaknesses. Behavioral items 5, 10 and 16 received a score of 6 or 7 from less than 1/3 of the employee.
 |
Table 3 Skills Weaknesses |
Two more weaknesses are relevant to management employees:
Beh Item 28 Effective balance consultation and decisiveness in decision-making (47%)
Beh Item 30 Evaluate the processes and outcomes of change (47%)
Five items as detailed in Table 4 were given a score of 6 or 7 by more than 80% of both management and non-management employees which can be perceived as skill strength.
 |
Table 4 Skill Strengths |
Results – Focus Group Discussion
Two focus groups were conducted between late June and early July 2024. Ten PHN employees who managed commissioning with employee management responsibilities attended one focus group. Eight PHN employees involved in commissioning work without employee management responsibilities participated in the second focus group.
Key Factors for Effective Commissioning
PHN employees in both focus groups were asked to identify the factors that enabled various aspects of commissioning to work effectively. Participants were reminded of each key step in the commissioning cycle during the discussion and were prompted with a broad range of topics, such as relationships, teams, management and leadership, organisational factors, and stakeholder engagement. In total, 23 factors were discussed, based on their similarity in relation to different aspects of commissioning, and the key factors mentioned by both FGs were put into seven themes relevant to the key functions of commissioning, as detailed in Table 5.
 |
Table 5 Key Factors for Effective Commissioning |
Challenges and Difficulties During the Commissioning Process
During the focus group discussions, participants were asked to share the challenges and difficulties encountered during the commissioning process. Participants were reminded of each key step in the commissioning cycle, particularly those related to tendering, co-designing, implementation, and working with, and engaging with, key stakeholders. Participants were also encouraged to explore the causes of these difficulties. In total, 12 challenges/difficulties were raised in both focus groups. Based on their similarities in relation to different aspects of healthcare commissioning, they were divided into five themes, as detailed in Table 6.
 |
Table 6 Challenges and Difficulties in Health Commissioning |
Discussion
The establishment of Primary Health Networks (PHNs) in Australia represents a significant reform in primary care enhancing local planning and prioritisation of healthcare needs. By leveraging the expertise of local services, PHNs facilitate the development of targeted, community-based care solutions.3,5 Effective commissioning of PHNs is vital for the prevention and management of chronic diseases, leading to improved health outcomes and a reduction in the demand for costly acute care services. The study clearly demonstrates how PHNs’ commissioning practices and efforts in developing the capacity of commissioning affect employees’ confidence in their capabilities, practices, and demonstration of the required skills. This strongly supports the organisational capacity development theory proposed by Potter and Brough (2004)26 as mentioned earlier. The development of external skills alone is inadequate to develop employee capabilities. Organisational efforts in supporting employees’ skill development and enabling employees to demonstrate and apply their skills are equally important.25 Improving employees’ confidence in their own work has positive links to improved job satisfaction and morale, which are important for improving retention and prevent burn out.36,37 Maximised support and professional development opportunities can positively affect employees’ self-confidence which ultimately affects their own performance.37,38 On the other hand, improved employee capability has a direct and positive effect on an organisation’s capacity to provide high quality services.25
Although there were consistent differences in the results between management and non-management employees in each survey section, the trend of the scores in each section was very similar between the two groups of employees. Such differences are not significant, indicating that there is a minimum impact of qualifications, years of service, and whether or not the individual has line management responsibilities on employees’ confidence in their own practice and self-perceived competencies. Based on the organisational capacity development theory discussed earlier, the findings support the idea that consistent and transparent organisation-wide policies and mechanisms to support and develop employee capabilities are fundamental to employee performance improvement.22,25,26 Management employees tended to give a lower score to current PHN commissioning practices related to strategic planning and stakeholder engagement compared to non-management employees. One possible explanation is that management employees might have been exposed to additional training and development opportunities, given the scope of their roles. This could include ad hoc development opportunities such as participation in strategic planning sessions or general interactions with boards, strategic partners, and system-wide engagement, which present a broader view of the local health ecosystem. Potentially, this system-wide influence or additional training and development has led management employees to develop critical and analytical skills and a better understanding of the impacts of the commissioning process as a whole. ‘You do not know what you don’t know’ may also be an explanation for non-management employees who hold more positive views of the current PHN’s practice, indicating that knowledge improvement may be required before skill development can be achieved.
Informal or formal training is only one of the many means of developing the required skills of employees and building their capabilities to excel in their roles.28,29 This study argues that investing in developing PHN employees’ overall understanding of the commissioning process is needed, coupled with a focus on developing a comprehension of the health system to allow a strategic understanding of what is being achieved by the PHN and its system partners through health and social care commissioning. PHN employees further emphasised the needs for systematic and progressive training and skill development opportunities to be made available to them. Ad hoc training may help develop an understanding of specific topics or skills, but it may not be adequate to meet the overall skill development requirements.39 To excel in a particular role, the application of specific and appropriate skill sets is essential. PHN employees are required to possess excellent communication and interpersonal skills when working with consumers and health professionals from various backgrounds.19 Competence was clearly captured in the self-assessments completed by both management and non-management employees. In addition to setting performance indicators and evaluating commissioned work, the focus of training and development for PHN employees should include data and information management, developing and managing budgets, monitoring financial performance by analysing a variety of financial data, applying risk management concepts and techniques, and applying relevant legislation, ethical principles, and accountability frameworks specific to healthcare settings.
Skills should be developed with a good understanding of what they are for, and how they should be adapted to different situations. In addition to systematic training and skill development, this study confirms the importance of organisational efforts in building employee capability.39,40 These efforts may include regular coaching by PHN colleagues, learning from each other by sharing ideas, discussing problems, identifying solutions at regular team meetings, and attending networking events with the employees of other PHNs. Including self-study time in employee workload was also consistently viewed by PHNs as important professional development.
Further, considering the discovery of the correlation between an organisation’s current practice, employee confidence in their own practices, and self-perceived competency, as detailed in Figure 5, a new model for building PHN’s health commissioning capacity placing employee at the centre of all efforts, is proposed in Figure 8. Employees are the backbone of quality service provision. Hence, policies, procedures, and investments should be designed around how best to support, guide, and build employee capabilities.
 |
Figure 8 PHN Health Commissioning Capacity Building Model. |
Successful commissioning starts with the identification of local needs, developing a good understanding of local service providers’ capacity, and ends with generating evidence to evaluate the outcomes of the commissioned work.19 Hence, organisational capacity in planning, evaluation, and key stakeholder engagement and consultations is an indicator of health commissioning success.13,41 The regular review of the Primary Health Networks of their own core health commissioning practice against a standardised set of commissioning competencies which includes key domains of data collection and evaluation processes, key stakeholder and community engagement strategies, and community-based needs assessment, is an important step for quality assurance and improvement. Employees who manage or are involved in commissioning should be engaged in the review process to ensure that their experiences and opinions are captured.
In the current economic climate and considering the financial constraints faced by our health system, healthcare organisations are pressured to improve service quality and efficiency.42 Continuous quality improvement involves regular monitoring of service processes and evaluation of service outcomes, which rely on the establishment of relevant performance indicators and the determination of appropriate data collection and analysis processes.43 However, the ability of Primary Health Networks to set performance indicators and evaluate the outcomes of commissioned works has not been well recognised. This study indicates that the support and guidance of PHN employees can be improved in these aspects. This is reflected in the low level of confidence among a large proportion of PHN employees in their ability to set performance measures and use performance indicators to evaluate the outcomes of commissioned work. Primary Health Networks’ efforts in setting and applying quality indices and benchmarks to set performance standards and inform continuous quality improvement are needed to build PHNs’ capacity for commissioning health and social care. To improve service quality and develop maturity over time, all levels of the organisation must be mobilised to share responsibilities.44,45
As health and social care commissioners, a key aspect of PHN’s responsibilities is working with a large number of local service providers to co-design services that can meet the primary healthcare needs of the local population.6,19 Primary Health Network employees are required to possess excellent communication and interpersonal skills when working with consumers and health professionals from various backgrounds. Competence was clearly captured in the self-assessments completed by both management and non-management employees. In addition to setting performance indicators and evaluating commissioned work, the focus of training and development for PHN employees should include data and information management, developing and managing budgets, monitoring financial performance by analysing a variety of financial data, applying risk management concepts and techniques, and applying relevant legislation, ethical principles, and accountability frameworks specific to healthcare settings.
The study also highlighted both successful practices and significant challenges in commissioning processes and suggested the following critical factors for successful health commissioning.
- clear procurement processes,
- effective and regular communication with service providers,
- flexibility in funding and contractual arrangements,
- fostering stakeholder relationships, and building partnerships and leveraging resources,
- involving community members in needs assessments, and
- well established performance and outcomes expectations.
Commissioning primary care services can be difficult because service outcomes may be difficult to specify and measure, particularly when paired with rigid funding models, time constraints, and finite financial resources.17,18 Primary Health Networks might be challenged to select the right service providers with the capacity to provide quality service delivery that meets identified local needs.19 Addressing communication gaps and funding constraints and enhancing governance are essential for improving commissioning outcomes. Capacity building through comprehensive training to support the novice commissioner in developing a level of advanced practice in healthcare commissioning and fostering greater collaboration across the PHN network can further strengthen the effectiveness and sustainability of commissioning efforts in primary health networks.
It is important to acknowledge the limitations of this study. First, while all staff members from participating PHNs were encouraged to engage in the online survey and focus group discussions, there may have been self-selection bias. This could have occurred due to the absence of compensation for the time and effort involved in participating. Staff members with a particular interest in improving commissioning practices or those with specific experiences to share may have been more likely to volunteer. Second, the study was limited to PHNs from only two out of the seven Australian states and territories, which may restrict the generalizability of the findings to other PHNs or different contexts. Third, the identification of current PHN practices relied solely on self-reported (subjective) data, which could introduce bias, particularly in evaluating one’s own competencies”.
Conclusions
Primary Health Networks, in their role as health care commissioners, are responsible for ensuring that robust commissioning processes are in place to achieve health outcomes of the Australian population. Enhancing leadership capability in health commissioning across PHNs is a worthwhile investment in meeting changing healthcare needs of the population. The confirmation of the positive influence of PHN’s current commissioning practices on staff confidence in their own practices and self-perceived competency reinforces PHNs’ important role in enhancing employees’ capability in managing or being involved in the health commissioning process. This can be achieved by adopting consistent and transparent organisation-wide policies and support mechanisms such as mentoring, coaching and investing in professional development. The study also highlights the need to adopt a flexible, blended approach to adult learning to systematically build skills in healthcare commissioning. Primary Health Networks should be encouraged to prioritise capacity-building initiatives focusing on data management, stakeholder engagement, and performance evaluation. Successful practices should also include clear procurement processes and strategic and analytical thinking and encourage a deep understanding of the complexities of the Australian healthcare system. Comprehensive training and continuous quality improvement efforts to address commissioning challenges such as rigid funding models, communication gaps, and resource constraints are required. All these efforts are critical to fostering advanced commissioning practices and ensuring the delivery of high-quality primary care services tailored to local needs.
Abbreviations
FGD, Focus Group Discussion; PHN, Primary Health Networks.
Acknowledgments
We are grateful for the funding and support provided by Hunter New England and Central Coast Primary Health Networks. The authors would like to acknowledge: 1) Lee Koh for assistance throughout the project, including developing the ethics application, setting up the online survey, and taking notes during the focus groups; 2) Anne Smyth for facilitating the focus groups and contributions made in developing the focus group schedules; and 3) Emily Grahn for the survey data analysis. The authors thank all focus group participants who shared their insights and experiences.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Ms Amanda Martin is an employee of Hunter New England and Central Coast Primary Health Network. Mrs Catherine Turner is an employee of Hunter New England and Central Coast Primary Health Network. The authors report no other conflicts of interest in this work.
References
1. Schneider EC, Shah A, Doty MM, Tikkanen R, Fields K, Williams RD. II mirror, mirror 2021 — reflecting poorly: health care in the U.S. Compared to other high-income countries. Commonwealth Fund. 2021. doi:10.26099/01DV-H208
2. Australian Institute of Health and Welfare. Health system overview. Australian Institute of Health and Welfare; Updated June 17, 2024a, Available from: https://www.aihw.gov.au/reports/australias-health/health-system-overview.
3. World Health Organisation. Primary Health Care. World Health Organisation. 2023. Available from: https://www.who.int/news-room/fact-sheets/detail/primary-health-care.
4. Australian Institute of Health and Welfare. Primary health care. Australian Institute of Health and Welfare. Updated March 1, 2024b, Available from: https://www.aihw.gov.au/reports-data/health-welfare-services/primary-health-care/overview.
5. Silburn K, Lewis V. Commissioning for health and community sector reform: perspectives on change from Victoria. Aust J Primary Health. 2020;26(4):332–337. doi:10.1071/PY20011
6. Australian Government Department of Health and Aged Care. PHN Strategy 2023-2024. Australian government department of health and aged care. April 10, 2024a, Updated August 27, 2024, Available from: https://www.health.gov.au/resources/publications/primary-health-networks-phn-strategy-2023-24.
7. Bates S, Harris-Roxas B, Wright M. Understanding the costs of co-commissioning: early experiences with co-commissioning in Australia. Aust J Public Admin. 2023;82(462):–487. doi:10.1111/1467-8500.12599
8. Hunter New England and Central Coast Primary Health Networks. HNECC PHN commissioned services toolkit. hunter new england and central coast primary health networks. Updated May, 2024, Available from: https://hneccphn.imgix.net/assets/src/uploads/images/HNECC-PHN-Commissioned-Services-Toolkit-May-2024-Rev.pdf.
9. Australian Government Department of Health. A commissioning overview in the PHN context. 2019. Available from: https://www.health.gov.au/sites/default/files/documents/2021/06/primary-health-networks-phns-commissioning-information-sheet-overview.pdf.
10. Australian Government Department of Health and Aged Care. Primary health networks. Australian Government Department of Health and Aged Care. Updated June 2, 2023, Available from: https://www.health.gov.au/our-work/phn.
11. Australian Government Department of Health. 2018. Change management and commissioning competencies guidance. Australian government department of health. Available from: https://www.health.gov.au/resources/publications/primary-health-networks-phns-change-management-and-commissioning-competencies-guidance-and-toolkit.
12. Bovaird T, Dickinson H, Allen K. Commissioning across government: review of evidence. Third Sector Research Centre research report. 2012. Available from: http://epapers.bham.ac.uk/1785/1/RR86_Commissioning_across_government_-_Bovaird_Aug_2012.pdf.
13. Regmi K, Mudyarabikwa O. A systematic review of the factors - barriers and enablers - affecting the implementation of clinical commissioning policy to reduce health inequalities in the national health service (NHS), UK. Public Health. 2020;186:271–282. doi:10.1016/j.puhe.2020.07.027
14. Department of Health (DH). Commissioning Framework for Health and Well-Being. London: DH; 2007.
15. The King’s Fund. Challenges and Lessons for Good Practice: Review of the History and Development of Health Service Commissioning. Prepared for Australian Government Department of Health; 2016.
16. Westen Australia Primary Health Alliance. Commissioning for better health. Western Aust Primary Health Network. 2019. https://www.wapha.org.au/wp-content/uploads/2019/04/Commissioning-for-Better-Health.pdf.
17. Gardner K, Powell DG, Edwards K, et al. A rapid review of the impact of commissioning on service use, quality, outcomes and value for money: implications for Australian policy. Aust J Primary Health. 2016;22(1):40–49. doi:10.1071/PY15148
18. McDermott I, Checkland K, Moran V, Warwick-Giles L. Achieving integrated care through commissioning of primary care services in the English NHS: a qualitative analysis. BMJ Open. 2019;9(4):e027622. doi:10.1136/bmjopen-2018-027622
19. Bates S, Wright M, Harris-Roxas B. Strengths and risks of the primary health network commissioning model. Aust Health Rev. 2022;46(5):586–594. doi:10.1071/AH21356
20. Dickinson H, Glasby J, Nicholds A, Sullivan H. Making sense of joint commissioning: three discourses of prevention, empowerment and efficiency. BMC Health Serv Res. 2013;13(Suppl 1):S6. doi:10.1186/1472-6963-13-S1-S6
21. US Agency for International Development. Organisational capacity building framework: a foundation for stronger, more sustainable HIV/AIDS programs, organisations and networks. Technical Brief. US Agency for International Development. January, 2011. Available from: https://msh.org/wp-content/uploads/2013/08/as2_technical_brief_2_final.pdf.
22. Smith BJ, Tang KC, Nutbeam D. WHO health promotion glossary: new terms. Health Promotion Int. 2006;21(4):340–345. doi:10.1093/heapro/dal033
23. DeCorby-Watson K, Mensah G, Bergeron K, Abdi S, Rempel B, Manson H. Effectiveness of capacity building interventions relevant to public health practice: a systematic review. BMC Public Health. 2018;18(1):684. doi:10.1186/s12889-018-5591-6
24. King O, West E, Alston L, et al. 2024. Models and approaches for building knowledge translation capacity and capability in health services: a scoping review. Implement Sci. 2024;19(7):1–44. doi:10.1186/s13012-024-01336-0
25. Bergeron K, Abdi S, DeCorby K, Mensah G, Rempel B, Manson H. Theories, models and frameworks used in capacity building interventions relevant to public health: a systematic review. BMC Public Health. 2017;17(1):914. doi:10.1186/s12889-017-4919-yBackhouse
26. Potter C, Brough R. Systemic capacity building: a hierarchy of needs. Health Policy Plan. 2004;19(5):336–345. doi:10.1093/heapol/czh038
27. Kelly N, Brophy C, Scharoun L, Finger M, Meth D. Co-design for staff professional learning within universities: a case study. J Appl Res Higher Educ. 2024;16(2):315–327. doi:10.1108/JARHE-12-2022-0381
28. Yabrough JR. Adapting adult learning theory to support innovative, advanced, online learning -- WVMD model. Res Higher Educ J. 2018;35:1–15.
29. Mukhalalati B, Taylor A. Adult learning theories in context: a quick guide for healthcare professional educators. J Med Educ Curric Dev. 2019;6. doi:10.1177/2382120519840332
30. Liang Z, Howard P, Leggat S, Bartram T. Development and validation of health service management competencies. J Health Organ Manage. 2018;32(2):157–175. doi:10.1108/JHOM-06-2017-0120
31. Howard P, Liang Z, Leggat S, Karimi L. Validation of a management competency assessment tool for health service managers. J Health Organ Manage. 2018;32(1):113–134. doi:10.1108/JHOM-08-2017-0223
32. Hennink MM, Kaiser BN, Weber MB. What influences saturation? Estimating sample sizes in focus group research. Qual Health Res. 2019;29(10):1483–1496. doi:10.1177/1049732318821692
33. Hennink M, Kaiser BN. Sample sizes for saturation in qualitative research: a systematic review of empirical tests. Soc Sci Med. 2022;292:114523. doi:10.1016/j.socscimed.2021.114523
34. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
35. Braun V, Clarke V, Hayfield N, Terry G. Thematic Analysis. In: Liamputtong P, editor. Handbook of Research Methods in Health Social Sciences. Singapore: Springer; 2019:843–860.
36. Zhenjing G, Chupradit S, Ku KY, Nassani AA, Haffar M. Impact of employees’ workplace environment on employees’ performance: a multi-mediation model. Front Public Health. 2020;10:890400. doi:10.3389/fpubh.2022.890400
37. Lin CP, Liu CM, Chan HT. Developing job performance: mediation of occupational commitment and achievement striving with competence enhancement as a moderator. Personnel Rev. 2021;51(2):750–769. doi:10.1108/PR-04-2020-0296
38. Diamantidis AD, Chatzoglou P. Factors affecting employee performance: an empirical approach. Int J Product Perform Manage. 2019;68(1):171–193. doi:10.1108/IJPPM-01-2018-0012
39. Brommeyer M, Whittaker M, Liang Z. Organisational factors driving the realization of digital health transformation benefits from health service managers: a qualitative study. J Healthcare Leadership. 2024;16:455–472. doi:10.2147/JHL.S487589
40. Liang Z, King J, Nagle C, Pain T, Mallett AJ. Empower and build the capabilities of mid-level health service managers to lead and support the health workforce – a study protocol. Int J Environ Res Public Health. 2024;21(8):994. doi:10.3390/ijerph21080994
41. NHS England. Commissioning. Available from: https://www.england.nhs.uk/commissioning/#:~:text=What%20is%20commissioning?,get%20the%20best%20health%20outcomes.
42. Angerer A, Stahl J, Krasniqi E, Banning S. The management perspective in digital health literature: systematic review. JMIR mHealth uHealth. 2022;10(11):e37624. doi:10.2196/376242
43. Hill JE, Stephani AM, Sapple P, Clegg AJ. The effectiveness of continuous quality improvement for developing professional practice and improving health care outcomes: a systematic review. Implementation Sci. 2020;15(1):1–14. doi:10.1186/s13012-020-0975-2
44. Backhouse A, Ogunlayi F. Quality improvement into practice. BMJ. 2020;368:m865. doi:10.1136/bmj.m865
45. Wendwessen N, Dereje T, Gize A. Factors affecting the implementation of continuous quality improvement in health facilities in Southern nation and nationalities peoples region (SNNPR), Ethiopia. J Multidisciplin Healthcare. 2020;13:855–862. doi:10.2147/JMDH.S260285
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Differences in Necessary Competencies, Skills, and Performance Abilities Among Thai Board-Certified Occupational Medicine Physicians and Basic Occupational Medicine Certified Physicians
Sasanawin P, Surawattanasakul V, Prasan S, Banomyong K
Journal of Multidisciplinary Healthcare 2025, 18:1423-1432
Published Date: 8 March 2025