")
Back to Journals » Journal of Inflammation Research » Volume 18
Development and Validation of a New Immune-Inflammatory-Nutritional Score to Predict Pathological Complete Response in Triple-Negative Breast Cancer Undergoing Neoadjuvant Chemotherapy: A Two-Center Study
Authors Wang S, Song Y , Ding J, Li M, Wang Y, Bai Y, Zi H, Sun J, Fan C, Chen H, Luo T, Wang T
Received 18 March 2025
Accepted for publication 23 June 2025
Published 16 July 2025 Volume 2025:18 Pages 9365—9378
DOI https://doi.org/10.2147/JIR.S526429
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Junhao Wang
Shuai Wang,1,* Yuting Song,2,* Jiajun Ding,1 Mengxuan Li,1 Yidi Wang,1 Yujie Bai,1 Haoyi Zi,1 Jianing Sun,1 Cong Fan,1 He Chen,1 Ting Luo,2 Ting Wang1
1Department of Thyroid, Breast and Vascular Surgery, Xijing Hospital, Fourth Military Medical University, Xi’an, Shaanxi, People’s Republic of China; 2Institute of Breast Health Medicine, Department of Medical Oncology, Cancer Center, Breast Center, West China Hospital, Sichuan University, Chengdu, Sichuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ting Wang, Department of Thyroid, Breast and Vascular Surgery, Xijing Hospital, Fourth Military Medical University, No. 127, Changle West Road, Xi’an, Shaanxi, 710032, People’s Republic of China, Email [email protected] Ting Luo, Institute of Breast Health Medicine, Department of Medical Oncology, Cancer Center, Breast Center, West China Hospital, Sichuan University, 37 Guoxue Alley, Wuhou District, Chengdu, Sichuan, 610000, People’s Republic of China, Email [email protected]
Purpose: To construct a novel immune-inflammatory-nutritional (IIN) score based on peripheral blood biomarkers related to inflammation, immunity, and nutrition, and to predict the efficacy of neoadjuvant chemotherapy (NAC) in patients with triple-negative breast cancer (TNBC).
Patients and Methods: We retrospectively selected 431 patients with TNBC from Xijing Hospital, and then randomly divided the patients into a training set and an internal validation set in a ratio of 7:3. An external validation set was included with 154 patients selected from West China Hospital of Sichuan University. In the training set, patients were divided into the pathological complete response (pCR) group and the non-pathological complete response group. Univariate logistic regression analysis and LASSO regression analysis were used to select biomarkers that affect the efficacy of NAC in TNBC patients and to construct the IIN score. A nomogram model was constructed based on the IIN score and clinical pathological characteristics to predict whether TNBC patients could achieve pCR after NAC before treatment. The predictive performance and clinical application value of the nomogram model were assessed using the receiver operating characteristic (ROC) curve, calibration curve, decision curve analysis, and confusion matrix.
Results: Through LASSO regression analysis, 6 biomarkers were ultimately identified to construct the scoring system. A nomogram model was constructed based on the IIN score and clinical pathological characteristics, and the ROC curve showed the areas under the curve to be 0.827, 0.786, and 0.754 in the training set, internal validation set, and external validation set, respectively. Calibration curves, decision curves, and confusion matrices all demonstrated that the nomogram model exhibited robust predictive performance and holds certain clinical application value.
Conclusion: The nomogram model based on the IIN score offers high predictive performance and can accurately predict the efficacy of NAC in TNBC patients before treatment, highlighting its clinical application potential.
Keywords: triple-negative breast cancer, immune-inflammatory-nutritional score, pathological complete response, neoadjuvant chemotherapy, nomogram
Introduction
Breast cancer is a malignant tumor that originates from epithelial cells of the mammary gland. According to the GLOBOCAN 2022 report, breast cancer has the highest incidence rate among women and is the leading cause of cancer-related mortality in females.1 Triple-negative breast cancer (TNBC) is the most aggressive subtype of breast cancer, characterized by the absence of expression of estrogen receptors, progesterone receptors, and human epidermal growth factor receptor 2 (HER2), accounting for approximately 12% to 17% of all breast cancer cases.2 Due to the absence of effective endocrine therapies and molecular-targeted treatments for TNBC, chemotherapy has become the primary treatment method in addition to surgery. Neoadjuvant chemotherapy (NAC) refers to the administration of chemotherapeutic drugs before surgery, which can reduce tumor volume and create opportunities for surgery, thereby improving patient prognosis. Studies have confirmed that patients who achieve pathological complete response (pCR) after NAC have better long-term outcomes.3 However, due to the heterogeneity of tumors, not all patients benefit from NAC. Some patients experience tumor progression during treatment, missing the optimal timing for surgical treatment. Therefore, predicting the efficacy of NAC through clinical indicators before treatment is of significant importance.
Recent studies have indicated that inflammation, immune function, and nutritional status are closely related to the occurrence and progression of tumors.4–6 Certain biomarkers related to inflammation, immunity, and nutrition, based on peripheral blood indicators, have significant value in predicting the efficacy of cancer treatment and prognosis.7–9 For instance, the neutrophil-to-lymphocyte ratio (NLR) is a typical peripheral blood inflammatory biomarker, and researchers have found that it has substantial value in predicting the efficacy of NAC and the prognosis of patients with esophageal squamous cell carcinoma.10 In TNBC, patients with a low NLR before NAC are more likely to achieve pCR and have a better long-term prognosis.11,12 The nutritional risk index (NRI) is a peripheral blood biomarker that reflects the body’s nutritional and immune status and can serve as a strong prognostic marker for patients with head and neck tumors.13 Additionally, the NRI can predict the prognosis of breast cancer patients, with patients having a high NRI exhibiting longer disease-free survival (DFS) and overall survival (OS).14 However, a single peripheral blood biomarker cannot fully reflect the patient’s inflammatory, immune function, and nutritional status. Combining these biomarkers may better reflect the actual situation. This study analyzed the relationship between peripheral blood biomarkers related to inflammation, immunity, and nutrition and the efficacy of NAC in patients with TNBC, with the aim of developing a new predictive model known as the immune-inflammatory-nutritional (IIN) score. Furthermore, a nomogram was constructed based on the IIN score and other clinical pathological features to predict treatment effects before NAC and guide clinical decision-making.
Materials and Methods
Study Cohort
A retrospective analysis was conducted on breast cancer patients admitted to Xijing Hospital (institution 1) from January 2018 to December 2023, totaling 6967 cases. The inclusion criteria were as follows: pathological puncture specimens diagnosed as TNBC by immunohistochemistry (IHC) and fluorescence in situ hybridization (FISH); received complete NAC; had no acute or chronic inflammation, hematologic disorders, or autoimmune diseases before NAC; underwent blood routine and liver and kidney function tests within one week before NAC; and underwent surgical treatment after NAC. The exclusion criteria included: inability to tolerate NAC or incomplete NAC process; concurrent other systemic malignant tumors; and incomplete clinical data. After screening according to the inclusion and exclusion criteria, a total of 431 patients were included in the study. Subsequently, patients were randomly divided into a training set (n=303) and an internal validation set (n=128) in a ratio of 7:3 using R software package “caret”. From June 2021 to June 2023, 154 patients admitted to West China Hospital of Sichuan University (institution 2) were included in the external validation set. The specific screening process is illustrated in Figure 1. This study was approved by the ethics committee of Xijing Hospital, with the ethical number: KY-20232266-C-1. In addition, approval has been obtained from West China Hospital of Sichuan University (ethical number: 2020–427). Informed consent was obtained from each patient. This study strictly adhered to the Declaration of Helsinki.
 |
Figure 1 Flowchart for selecting the study population. Abbreviations: TNBC, triple-negative breast cancer; NAC, neoadjuvant chemotherapy; pCR, pathological complete response; non-pCR, non-pathological complete response. |
NAC Regimens and Efficacy Assessment
The NAC regimens, based on anthracycline and taxane classes, included the AC-T, TAC, and TC protocols. The AC-T regimen consisted of four cycles of doxorubicin (100mg/m2) and cyclophosphamide (600mg/m2), followed by four cycles of docetaxel (100mg/m2) or twelve cycles of paclitaxel (80mg/m2). The TAC regimen comprised six cycles of docetaxel (75mg/m2), doxorubicin (50mg/m2), and cyclophosphamide (500mg/m2). The TC regimen involved four cycles of docetaxel (75mg/m2) and cyclophosphamide (600mg/m2).
The NAC was followed by surgery, and the efficacy of the NAC was assessed through the surgical specimens. According to the pathology, the efficacy was divided into pCR and non-pathological complete response (non-pCR). pCR is defined as the absence of invasive cancer in the primary lesion of the breast (with the possibility of existence of ductal carcinoma in situ) and negative regional lymph nodes.15
Date Collection
Clinical and pathological data of patients were collected from the medical record system, including age, body mass index (BMI), family history of cancer, menstrual status, cT stage, cN stage, histological subtype, histological grade, HER2 expression level, Ki-67, p53 status, androgen receptor (AR) status, as well as hematological indicator data within one week before the first NAC. The HER2 expression level was categorized based on IHC and FISH as 0, 1+, and 2+ with FISH-negative; Ki-67 was considered low expression with positive cell count <30%, and high expression with ≥30%;16 p53 was considered positive if there was any staining in tumor cells, regardless of the number of positive cells; AR was considered negative with positive cell count <1%, and positive with ≥1%. The collected hematological indicators included neutrophil count, lymphocyte count, platelet count, monocyte count, hemoglobin level, and albumin level. A total of 11 peripheral blood biomarkers related to inflammation, immunity, and nutrition were included in this study, and the calculation formulas are provided in Table 1.
 |
Table 1 The Calculation Formulas of 11 Peripheral Blood Biomarkers Related to Inflammation, Immunity, and Nutrition |
IIN Score Construction
First, in the training set, univariate logistic regression analysis was performed to screen for biomarkers that affect the efficacy of NAC. Biomarkers with a P-value less than 0.05 were used for further analysis. Subsequently, the predictive value of these biomarkers was assessed using the least absolute shrinkage and selection operator (LASSO) regression analysis, which could minimize the risk of overfitting and address collinearity issues. The R software package “glmnet” was used to perform LASSO regression. A 10-fold cross-validation method was employed with deviance as the evaluation metric, ultimately selecting the lambda value corresponding to the minimum deviance for subsequent analysis. Finally, IIN score was calculated based on the biomarkers with non-zero coefficients. The formula for the IIN score was: IIN score = β1×Value1+β2×Value2+.+βn×Valuen, where β represents the regression coefficient of the corresponding biomarker, and Value represents the value of the corresponding biomarker. The IIN score for each patient was calculated. At the same time, the coefficients derived from the training set were used to calculate the patient IIN score in the internal and external validation sets to evaluate the effectiveness of the model.
Predictive Value of IIN Score
To explore whether the IIN score was associated with adverse clinical and pathological features, we compared the IIN score differences among subgroups of various clinical and pathological characteristics and presented the results in box plots. The receiver operating characteristic (ROC) curve was plotted based on the IIN score, and its predictive performance was evaluated according to the area under the curve (AUC).
Construction and Validation of Nomogram
In order to validate the IIN score as an independent factor influencing the efficacy of NAC, the IIN score was incorporated as a variable, in conjunction with other clinical and pathological parameters, for both univariate and multivariate logistic regression analyses. Variables that exhibit a P-value less than 0.05 in the multivariate logistic regression analysis were included in the construction of a nomogram. The predictive performance of the nomogram was illustrated using ROC curves and calibration curves. Decision curve analysis was utilized to evaluate the clinical value of the nomogram in practical applications.
Statistical Analysis
Statistical analyses were performed using R 4.0.5. Categorical variables were described using frequencies and percentages, and comparisons between groups were made using the chi-square test or Fisher’s exact tests. Continuous variables with a normal distribution were described using the mean ± standard deviation (SD), and group comparisons were made using the t-test or one-way ANOVA. Continuous variables with a non-normal distribution were described using the median and interquartile range (IQR), and group comparisons were made using the Mann–Whitney U-test or Kruskal–Wallis H-test. A P-value less than 0.05 was considered to indicate statistical significance.
Results
Baseline Characteristics
The baseline characteristics of the training set, internal validation set, and external validation set are presented in Table 2. The average age of the patients in the training set was 47.86±10.61 years, with 123 cases (40.6%) achieving pCR; the average age of the patients in the internal validation set was 48.05±10.59 years, with 47 cases (36.7%) achieving pCR. In the external validation set, the average age of the patients was 48.64±10.78 years, with 59 cases (38.3%) achieving pCR. There was no difference in the pCR rates among the three cohorts (P=0.730).
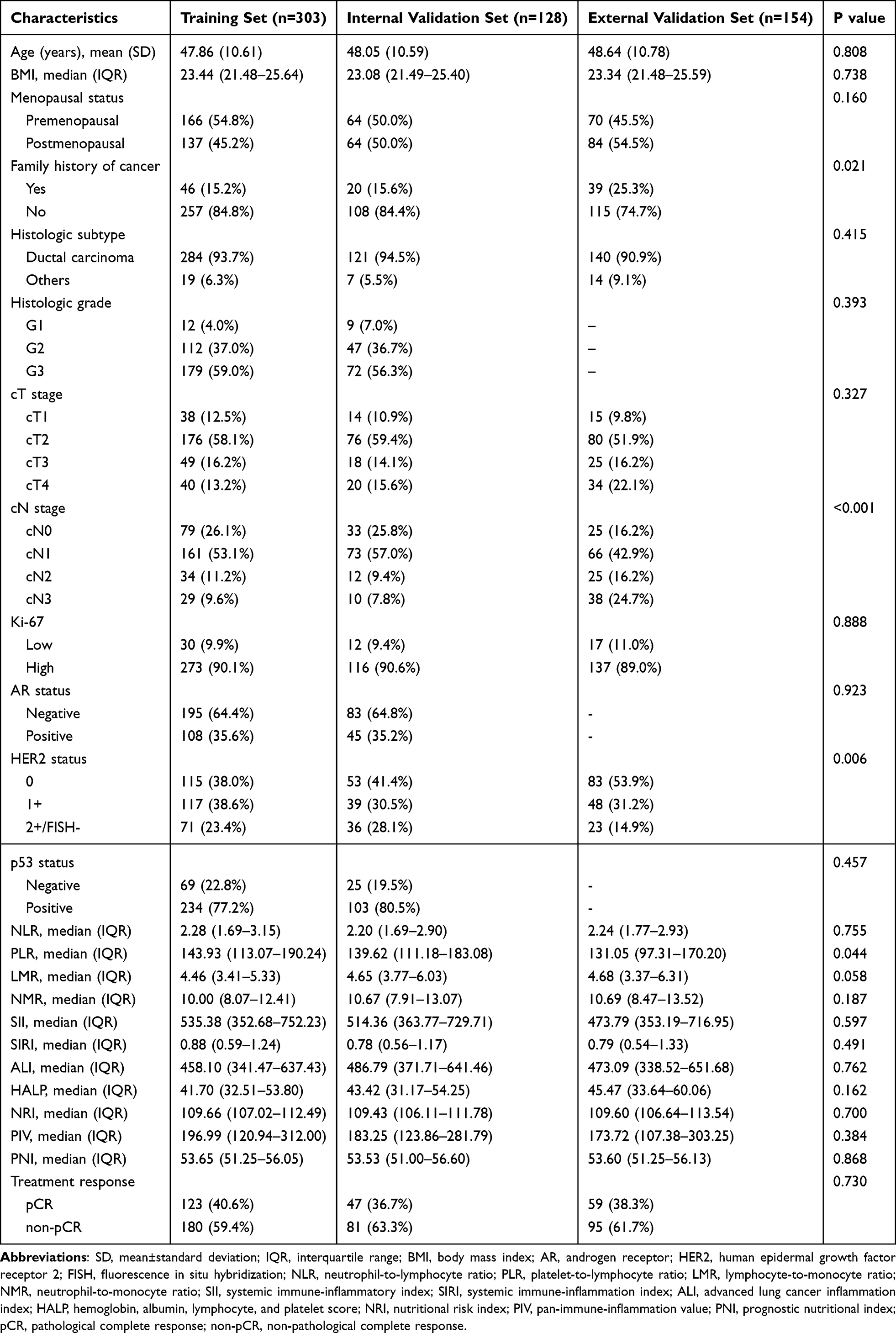 |
Table 2 Clinical Characteristics of Patients in This Study |
IIN Score
Univariate logistic regression analysis was performed on 11 peripheral blood biomarkers related to inflammation, immunity, and nutrition. The results indicated that 8 biomarkers were associated with the efficacy of NAC (Table 3). Further LASSO regression analysis revealed that 6 biomarkers with non-zero coefficients were closely related to achieving pCR after NAC (Figure 2A and B). These 6 biomarkers were NLR, lymphocyte-to-monocyte ratio (LMR), systemic immune-inflammation index (SIRI), hemoglobin, albumin, lymphocyte, and platelet score (HALP), NRI, and pan-immune-inflammation value (PIV). The IIN score was calculated as follows: IIN score = NLR×0.00124-LMR×0.11805-SIRI×0.11408+HALP×0.11070-NRI×0.03192+PIV×0.01507 (Figure 2C). Spearman correlation analysis was conducted on the biomarkers included in the IIN score, and a heatmap was plotted, showing that there was no high correlation among these 6 biomarkers, with correlation coefficients all within the range of −0.7 and 0.7 (Figure 2D). Clinical correlation analysis results indicated significant differences in the IIN score between cT stage (Figure 3). Patients with earlier cT stage had relatively higher IIN score, while those with later stage had relatively lower IIN score. This suggests that the IIN score was correlated with adverse tumor characteristics. The ROC curve based on the score had AUC values of 0.766, 0.734, and 0.723 in the training set, internal validation set, and external validation set, respectively, indicating that the IIN score had a relatively high predictive ability (Figure 4B–D). Additionally, we constructed prediction models using single biomarkers (Figure S1). The results demonstrated that the IIN score significantly enhanced predictive performance. This provided compelling evidence supporting the practical application of the IIN score.
 |
Table 3 Univariate Logistic Analysis of 11 Biomarkers Between pCR Patients and Non-pCR Patients in the Training Set |
 |
Figure 2 Construction of the IIN score. (A) Partial likelihood deviance for LASSO coefficient profiles. (B) LASSO coefficient profiles of 8 biomarkers related to inflammation, immunity, and nutrition. (C) The 6 biomarkers involved in the construction of the score. (D) Heatmap of the correlations of the 6 biomarkers. Abbreviations: IIN, immune-inflammatory-nutritional; LASSO, Least absolute shrinkage and selection operator; NLR, neutrophil-to-lymphocyte ratio; LMR, lymphocyte-to-monocyte ratio; SIRI, systemic immune-inflammation index; HALP, hemoglobin, albumin, lymphocyte, and platelet score; NRI, nutritional risk index; PIV, pan-immune-inflammation value. |
 |
Figure 3 Differential analysis of the distribution of the IIN score in different clinicopathologic features. Abbreviations: IIN, immune-inflammatory-nutritional; BMI, body mass index; HER2, human epidermal growth factor receptor 2; AR, androgen receptor. |
 |
Figure 4 Construction and validation of the nomogram. (A) Development of the nomogram in the training set, incorporating cT stage, Ki-67 and IIN score. Receiver operating characteristic curves of the IIN score and the nomogram model in the training set (B), internal validation set (C), and external validation set (D). Abbreviations: IIN, immune-inflammatory-nutritional; AUC, area under the curve. |
Nomogram
In the training set, the score, along with other clinical and pathological parameters, was subjected to univariate and multivariate logistic regression analyses. The univariate results indicated that cT stage, cN stage, Ki-67, and the IIN score were associated with achieving pCR after NAC (Table 4). The multivariate analysis revealed that cT stage, Ki-67, and the IIN score were independent factors affecting the efficacy of NAC (Table 5). A nomogram model was constructed based on these three independent factors (Figure 4A). The ROC curve demonstrated that the AUC values of the nomogram model were 0.827, 0.786, and 0.754 for the training set, internal validation set, and external validation set, respectively (Figure 4B–D). Calibration curve also showed that the predicted outcomes by the nomogram model were highly consistent with the actual outcomes (Figure 5A–C). Overall, the nomogram model constructed based on the IIN score and clinical pathological characteristics exhibited certain discrimination and calibration capabilities. Furthermore, by quantifying the net benefits at different threshold probabilities, we conducted decision curve analysis to evaluate the clinical utility of the nomogram model. The decision curve indicated that the nomogram model provided high net benefits for patients (Figure 5D–F). We also plotted a confusion matrix to further visualize the predictive performance of the nomogram model (Figure 5G–I). Table 6 detailed the predictive performance of the IIN score and the nomogram model across the three cohorts.
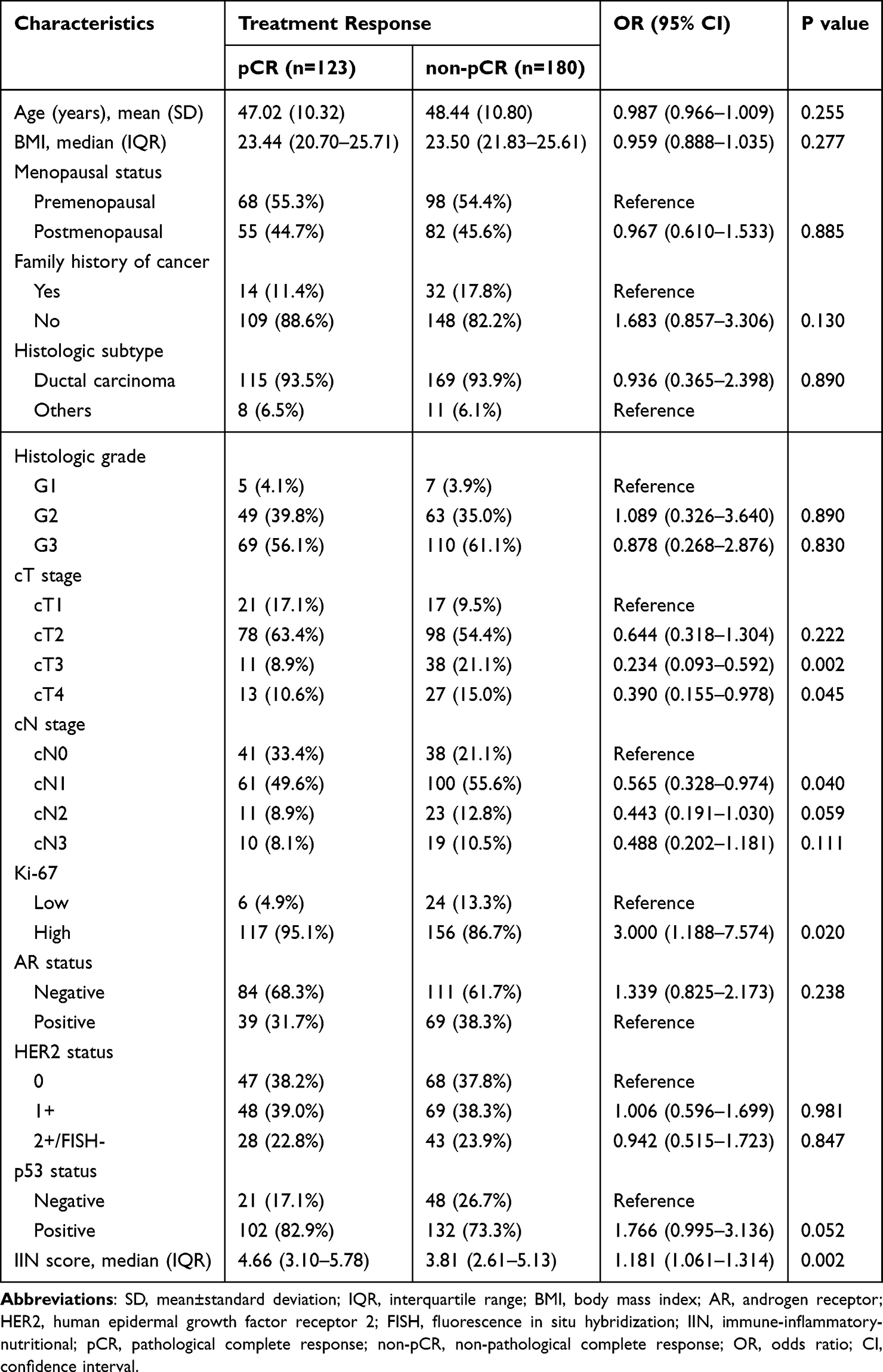 |
Table 4 Univariate Logistic Analysis of Patients with pCR Versus Those Without in the Training Set |
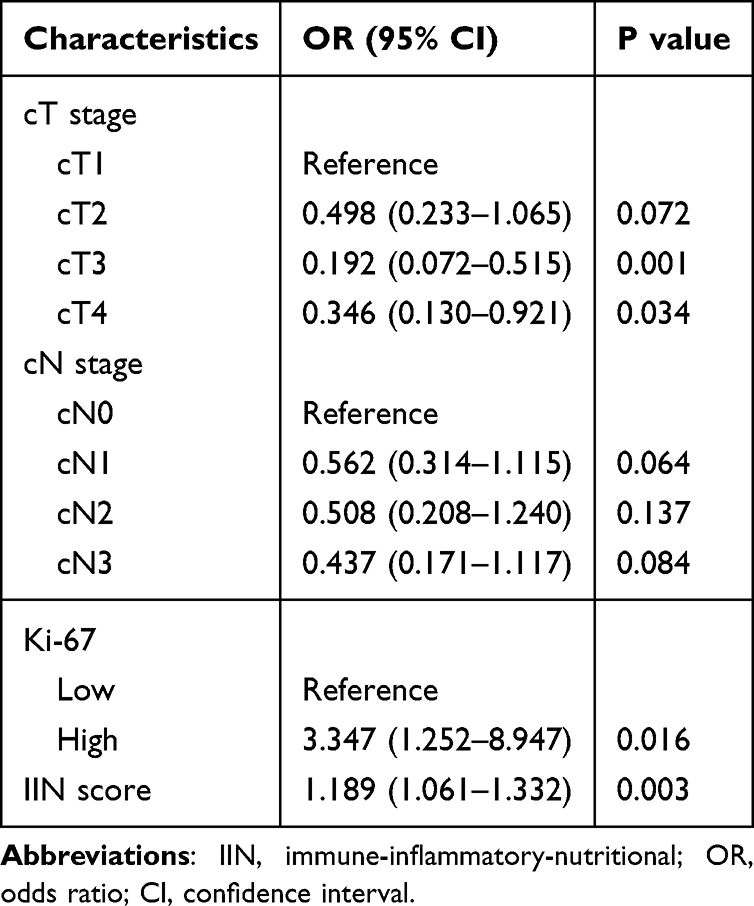 |
Table 5 Multivariate Logistic Analysis of Patients with pCR Versus Those Without in the Training Set |
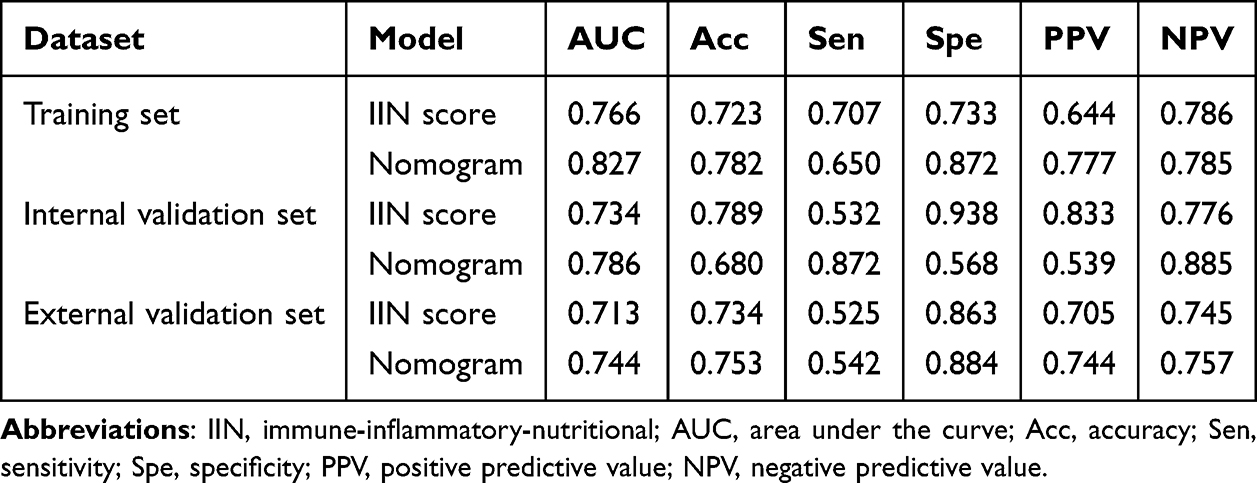 |
Table 6 Predictive Performance of the Two Models in the Training Set, Internal Validation Set and External Validation Set |
 |
Figure 5 Calibration curves for the nomogram in the training set (A), internal validation set (B), and external validation set (C). Decision curve analysis for the nomogram in the training set (D), internal validation set (E), and external validation set (F). Confusion matrix for the nomogram in the training set (G), internal validation set (H), and external validation set (I). Abbreviations: pCR, pathological complete response; non-pCR, non-pathological complete response. |
Discussion
NAC has become the standard treatment for downstaging and downsizing in breast cancer. Patients who achieve pCR after NAC have longer DFS and OS.17 Moreover, patients with pCR can also benefit from breast-conserving surgery, and may even forgo surgery without the need for mastectomy.18,19 However, the gold standard for pCR assessment depends on the pathological results of the surgical specimen after NAC. Accurately predicting the efficacy of NAC before surgery can not only identify the population likely to benefit from NAC but also enable patients to benefit from different surgical strategies. This provides significant value for clinical diagnosis and treatment.
Immune and inflammatory responses play a crucial role in the occurrence and progression of cancer.20,21 The cytokine microenvironment created by cytotoxic T cells and helper T cells can inhibit the growth of tumor cells.22 The tumor-associated microenvironment attracts the recruitment of tumor-associated neutrophils by secreting chemokines, cytokines, and hydrogen peroxide, then reshapes the extracellular matrix or releases matrix metalloproteinases 8/9, thereby affecting tumor progression. Tumor-associated neutrophils can also interact with CD8+ T cells to induce immune suppression or activation, promoting tumor progression.23,24 In addition, tumor-associated macrophages also promote the occurrence and development of cancer through immune suppression, extracellular matrix reconstruction, and angiogenesis.25 Monocytes can regulate tumor metastasis by stimulating the aggregation of natural killer cells and enhancing immune surveillance.26
It is widely acknowledged that liquid biopsy is the optimal choice for predicting the therapeutic response of malignant tumors or monitoring long-term recurrence and metastasis. The key step in liquid biopsy is the isolation of tumor-associated substances from blood or other body fluids, which helps to overcome population bias and reduce analysis time.27 Peripheral blood testing is widely applied in clinical settings due to its low cost, convenience, stability, and high reproducibility. Studies have confirmed that certain inflammatory, immune, and nutritional biomarkers in peripheral blood are closely related to the efficacy and prognosis of cancer treatment. The systemic immune-inflammatory index is associated with the prognosis of colorectal and liver cancer patients and can serve as a potential prognostic predictor.28,29 Platelet-to-lymphocyte ratio (PLR) is related to the efficacy of NAC in gastric cancer patients, with better treatment outcomes observed in patients with a low PLR before treatment.9,30 However, the predictive power of a single biomarker is limited, making the integration of multiple markers essential. We collected 11 peripheral blood biomarkers related to inflammation, immunity, and nutrition, and ultimately selected 6 to construct the IIN score. To the best of our knowledge, this was the first study to integrate multiple biomarkers into the IIN score to predict the efficacy of NAC in TNBC patients.
The IIN score is composed of 6 biomarkers, namely NLR, LMR, SIRI, HALP, NRI and PIV. Elevated NLR indicates a reduction in lymphocytes, an increase in neutrophils, or both, reflecting a relatively weak immune system that is unable to suppress the progression of cancer. Numerous studies have demonstrated that NLR is correlated with the efficacy and prognosis of NAC in TNBC patients, which is consistent with our findings.11,31 LMR, representing the ratio of peripheral white blood cell count to monocyte count, is one of the best markers, since high LMR levels synergize with chemotherapy drugs to increase drug sensitivity and improve the efficacy of NAC.32 Our study suggested that TNBC patients with high LMR levels before NAC were more likely to achieve pCR. Currently, no studies have reported the impact of LMR levels on the efficacy of NAC in TNBC patients. However, studies have confirmed that LMR levels are an independent factor affecting the efficacy and prognosis of NAC in breast cancer patients.33 SIRI, a composite inflammatory biomarker based on neutrophil count, monocyte count, and lymphocyte count, has been shown in previous studies to predict the efficacy and prognosis of NAC in breast cancer patients.34,35 We found that in TNBC, patients with low SIRI levels before NAC had better treatment outcomes. HALP is a composite indicator that comprehensively assesses the nutritional status and inflammatory stress response of the body. Previous studies have reported that TNBC patients with low HALP levels before NAC have a lower pCR rate and worse prognosis.36 Our study also confirmed this. Nutritional status is closely related to immune function and the development of tumors. NRI, which includes changes in patient weight, can effectively reflect the nutritional status of patients. NRI is an independent factor affecting the prognosis of breast cancer patients, and there are fewer reports on its relationship with the efficacy of NAC.37 Our study suggested that NRI could predict the efficacy of NAC in TNBC patients, with patients with high NRI levels more likely to achieve pCR. PIV, which includes all pro-inflammatory cells in the peripheral blood cell count in its calculation formula, can more accurately simulate and reflect inflammatory stress. In breast cancer patients undergoing NAC, patients with low PIV before treatment have better treatment outcomes and prognosis than those with high PIV.38 We also confirmed the predictive value of PIV in TNBC. In our study, univariate and multivariate logistic regression analyses indicated that the IIN score was an independent factor affecting the efficacy of NAC in TNBC patients. A nomogram model based on the IIN score and other clinically and pathologically independent predictive features showed high predictive ability with the ROC curve. Calibration curves, decision curves, and confusion matrices all indicated that the nomogram model has robust predictive performance and certain clinical application value.
However, our study has several limitations. Firstly, this study was retrospective, which introduces a certain degree of bias. Secondly, while the IIN score could predict the efficacy of NAC in TNBC patients, its predictive value for patient prognosis remained unclear. Therefore, we plan to conduct a multicenter prospective study with long-term follow-up of patients to further explore the impact of peripheral blood biomarkers related to inflammation, immunity, and nutrition on the efficacy and prognosis of NAC in TNBC patients.
Conclusion
In summary, we have integrated 6 peripheral blood biomarkers related to inflammation, immunity, and nutrition to construct the IIN score. This score is an independent factor affecting the efficacy of NAC in patients with TNBC. A nomogram model based on IIN score can accurately predict whether TNBC patients will achieve pCR after NAC, which has guiding significance for the formulation of clinical decisions by physicians. However, additional prospective studies are warranted.
Data Sharing Statement
All data supporting the results reported in this study are available from the corresponding author upon request.
Acknowledgments
We are grateful to the doctors and participants who participated in this study.
Funding
This work was supported by the Cultivation Boost Project of Xijing Hospital (No. XJZT24LY09) and the Shaanxi Province Natural Science Basic Research (No. 2023-JC-QN-0965, No. 2023-JC-QN-0982).
Disclosure
No potential conflict of interest was reported by the authors.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Bianchini G, De Angelis C, Licata L, et al. Treatment landscape of triple-negative breast cancer - expanded options, evolving needs. Nat Rev Clin Oncol. 2022;19(2):91–113. doi:10.1038/s41571-021-00565-2
3. Klein J, Tran W, Watkins E, et al. Locally advanced breast cancer treated with neoadjuvant chemotherapy and adjuvant radiotherapy: a retrospective cohort analysis. BMC Cancer. 2019;19(1):306. doi:10.1186/s12885-019-5499-2
4. Kiely M, Lord B, Ambs S. Immune response and inflammation in cancer health disparities. Trends Cancer. 2022;8(4):316–327. doi:10.1016/j.trecan.2021.11.010
5. Mirza AH, Thomas G, Ottensmeier CH, et al. Importance of the immune system in head and neck cancer. Head Neck. 2019;41(8):2789–2800. doi:10.1002/hed.25716
6. Wiseman MJ. Nutrition and cancer: prevention and survival. Br J Nutr. 2019;122(5):481–487. doi:10.1017/S0007114518002222
7. Jung SH, Hao J, Shivakumar M, et al. Development and validation of a novel strong prognostic index for colon cancer through a robust combination of laboratory features for systemic inflammation: a prognostic immune nutritional index. Br J Cancer. 2022;126(11):1539–1547. doi:10.1038/s41416-022-01767-w
8. Xie H, Ruan G, Ge Y, et al. Inflammatory burden as a prognostic biomarker for cancer. Clin Nutr. 2022;41(6):1236–1243. doi:10.1016/j.clnu.2022.04.019
9. Skórzewska M, Pikuła A, Gęca K, et al. Systemic inflammatory response markers for prediction of response to neoadjuvant chemotherapy in patients with advanced gastric cancer. Cytokine. 2023;172:156389. doi:10.1016/j.cyto.2023.156389
10. Hoshino S, Takeuchi M, Kawakubo H, et al. Neutrophil-to-lymphocyte ratio change predicts histological response to and oncological outcome of neoadjuvant chemotherapy for esophageal squamous cell carcinoma. Esophagus. 2022;19(3):426–435. doi:10.1007/s10388-021-00901-6
11. Kusama H, Kittaka N, Soma A, et al. Predictive factors for response to neoadjuvant chemotherapy: inflammatory and immune markers in triple-negative breast cancer. Breast Cancer. 2023;30(6):1085–1093. doi:10.1007/s12282-023-01504-y
12. Qiu X, Song Y, Cui Y, et al. Increased neutrophil-lymphocyte ratio independently predicts poor survival in non-metastatic triple-negative breast cancer patients. IUBMB Life. 2018;70(6):529–535. doi:10.1002/iub.1745
13. Yiu CY, Liu CC, Wu JY, et al. Efficacy of the geriatric nutritional risk index for predicting overall survival in patients with head and neck cancer: a meta-analysis. Nutrients. 2023;15(20):4348. doi:10.3390/nu15204348
14. Chen L, Qi Y, Kong X, et al. Nutritional risk index predicts survival in patients with breast cancer treated with neoadjuvant chemotherapy. Front Nutr. 2021;8:786742. doi:10.3389/fnut.2021.786742
15. Wang-Lopez Q, Chalabi N, Abrial C, et al. Can pathologic complete response (pCR) be used as a surrogate marker of survival after neoadjuvant therapy for breast cancer?. Crit Rev Oncol Hematol. 2015;95(1):88–104. doi:10.1016/j.critrevonc.2015.02.011
16. Nielsen TO, Leung S, Rimm DL, et al. Assessment of Ki67 in breast cancer: updated recommendations from the international Ki67 in breast cancer working group. J Natl Cancer Inst. 2021;113(7):808–819. doi:10.1093/jnci/djaa201
17. van Mackelenbergh MT, Loibl S, Untch M, et al. Pathologic complete response and individual patient prognosis after neoadjuvant chemotherapy plus anti-human epidermal growth factor receptor 2 therapy of human epidermal growth factor receptor 2-positive early breast cancer. J Clin Oncol. 2023;41(16):2998–3008. doi:10.1200/JCO.22.02241
18. Goetz MP, Gradishar WJ, Anderson BO, et al. NCCN guidelines insights: breast cancer, version 3.2018. J Natl Compr Canc Netw. 2019;17(2):118–126. doi:10.6004/jnccn.2019.0009
19. Kuerer HM, Smith BD, Krishnamurthy S, et al. Eliminating breast surgery for invasive breast cancer in exceptional responders to neoadjuvant systemic therapy: a multicentre, single-arm, Phase 2 trial. Lancet Oncol. 2022;23(12):1517–1524. doi:10.1016/S1470-2045(22)00613-1
20. Singh R, Mishra MK, Aggarwal H. Inflammation, immunity, and cancer. Mediators Inflamm. 2017;2017:6027305. doi:10.1155/2017/6027305
21. Greten FR, Grivennikov SI. Inflammation and cancer: triggers, mechanisms, and consequences. Immunity. 2019;51(1):27–41. doi:10.1016/j.immuni.2019.06.025
22. Disis ML. Immune regulation of cancer. J Clin Oncol. 2010;28(29):4531–4538. doi:10.1200/JCO.2009.27.2146
23. Ocana A, Nieto-Jiménez C, Pandiella A, et al. Neutrophils in cancer: prognostic role and therapeutic strategies. Mol Cancer. 2017;16(1):137. doi:10.1186/s12943-017-0707-7
24. Wu L, Saxena S, Singh RK. Neutrophils in the Tumor Microenvironment. Adv Exp Med Biol. 2020;1224:1–20.
25. Noy R, Pollard JW. Tumor-associated macrophages: from mechanisms to therapy. Immunity. 2014;41(1):49–61. doi:10.1016/j.immuni.2014.06.010
26. Olingy CE, Dinh HQ, Hedrick CC. Monocyte heterogeneity and functions in cancer. J Leukoc Biol. 2019;106(2):309–322. doi:10.1002/JLB.4RI0818-311R
27. Tellez-Gabriel M, Knutsen E, Perander M. Current status of circulating tumor cells, circulating tumor DNA, and exosomes in breast cancer liquid biopsies. Int J Mol Sci. 2020;21(24):9457. doi:10.3390/ijms21249457
28. Menyhart O, Fekete JT, Győrffy B. Inflammation and colorectal cancer: a meta-analysis of the prognostic significance of the systemic immune-inflammation index (SII) and the systemic inflammation response index (SIRI). Int J Mol Sci. 2024;25(15):8441. doi:10.3390/ijms25158441
29. Hu B, Yang XR, Xu Y, et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin Cancer Res. 2014;20(23):6212–6222. doi:10.1158/1078-0432.CCR-14-0442
30. Tang C, Cheng X, Yu S, et al. Platelet-to-lymphocyte ratio and lymphocyte-to-white blood cell ratio predict the efficacy of neoadjuvant chemotherapy and the prognosis of locally advanced gastric cancer patients treated with the oxaliplatin and capecitabine regimen. Onco Targets Ther. 2018;11:7061–7075. doi:10.2147/OTT.S176768
31. Kim JH, Son NH, Lee JS, et al. Time-sequencing of the neutrophil-to-lymphocyte ratio to predict prognosis of triple-negative breast cancer. Cancers. 2021;13(14):3472.
32. Vacchelli E, Eggermont A, Fridman WH, et al. Trial watch: immunostimulatory cytokines. Oncoimmunology. 2013;2(7):e24850. doi:10.4161/onci.24850
33. Meng X, Wang X, Jiang C, et al. Correlation analysis of lymphocyte-monocyte ratio with pathological complete response and clinical prognosis of neoadjuvant chemotherapy in patients with breast cancer. Transl Oncol. 2022;18:101355. doi:10.1016/j.tranon.2022.101355
34. Dong J, Sun Q, Pan Y, et al. Pretreatment systemic inflammation response index is predictive of pathological complete response in patients with breast cancer receiving neoadjuvant chemotherapy. BMC Cancer. 2021;21(1):700. doi:10.1186/s12885-021-08458-4
35. Zhang S, Cheng T. Prognostic and clinicopathological value of systemic inflammation response index (SIRI) in patients with breast cancer: a meta-analysis. Ann Med. 2024;56(1):2337729. doi:10.1080/07853890.2024.2337729
36. Lou C, Jin F, Zhao Q, et al. Correlation of serum NLR, PLR and HALP with efficacy of neoadjuvant chemotherapy and prognosis of triple-negative breast cancer. Am J Transl Res. 2022;14(5):3240–3246.
37. Lin F, Xia W, Chen M, et al. A prognostic model based on nutritional risk index in operative breast cancer. Nutrients. 2022;14(18):3783. doi:10.3390/nu14183783
38. Şahin AB, Cubukcu E, Ocak B, et al. Low pan-immune-inflammation-value predicts better chemotherapy response and survival in breast cancer patients treated with neoadjuvant chemotherapy. Sci Rep. 2021;11(1):14662. doi:10.1038/s41598-021-94184-7
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Predictive Value of Pretreatment Neutrophil to Albumin Ratio in Response to Neoadjuvant Chemotherapy of Breast Cancer
Deng YX, Zhao YJ, Nong QH, Qiu HM, Guo QL, Hu H
Breast Cancer: Targets and Therapy 2024, 16:393-402
Published Date: 23 July 2024
Promising Response to Neoadjuvant Chemotherapy Plus Immunotherapy in Metaplastic Breast Carcinoma
Tan Q, Li N, Wang Y, Du T, Liang G, Zhao Z, Tang J, Wu H
Breast Cancer: Targets and Therapy 2025, 17:447-454
Published Date: 23 May 2025