")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Development and Validation of an Agricultural Safety and Health Literacy Tool
Received 18 March 2025
Accepted for publication 2 July 2025
Published 17 July 2025 Volume 2025:18 Pages 4059—4070
DOI https://doi.org/10.2147/JMDH.S528979
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
Gyeong-Ye Lee,1 Ki-Soo Park1,2
1Department of Preventive Medicine, Institute of Medical Sciences, College of Medicine, Gyeongsang National University, Jinju, Republic of Korea; 2Department of Bio & Medical Big Data, Gyeongsang National University, Jinju, Republic of Korea
Correspondence: Ki-Soo Park, Department of Preventive Medicine, Institute of Medical Sciences, College of Medicine, Gyeongsang National University, 816 Beon-gil Jinju-daero 15, Jinju, 52727, Republic of Korea, Tel +82-55-772-8095, Fax +82-55-772-8099, Email [email protected]
Background: Health literacy in the workplace plays a crucial role in preventing work-related diseases and injuries. This study aims to develop and validate an instrument to measure Agricultural Safety and Health Literacy (ASHL) based on existing occupational health literacy tools.
Methods: The development of the instrument involved preliminary item development, expert evaluation, and preliminary testing. Cronbach’s α, a coefficient that measures the internal consistency of each item, was measured for reliability. Exploratory factor analysis and confirmatory factor analysis were performed to examine the construct validity, and predictive validity was evaluated using paired t-tests for changes in health literacy before and after education.
Results: The overall Cronbach’s α for the instrument was 0.92, indicating high reliability. In the exploratory factor analysis, five factors were extracted explaining 64.4% of the total variance. As a result of confirmatory factor analysis, the goodness-of-fit index (GFI) was shown as GFI=0.851, adjusted GFI=0.816, comparative fit index=0.901, normed fit index=0.835, root mean square error of approximation=0.071, and χ2/df=2.2. These results indicated acceptable model fit. The change in score from before to after the educational intervention was confirmed to have predictive validity with a significant increase in all areas (p< 0.005).
Conclusion: This study describes the development of an instrument for understanding ASHL for use in evaluating the health and safety of farmers. The developed instrument will be used in Korea to improve the health behavior of farmers and to prevent and manage various health problems that may occur in the agricultural working environment.
Keywords: agriculture, safety, health, literacy
Introduction
Health literacy refers to the ability to access health information, acquire the necessary details, comprehend the information, and judge its suitability in order to apply it for health management, disease prevention, and the use of medical services.1 It has also been defined as the cognitive and social skills that determine an individual motivation and capacity to access, understand, evaluate, and use health information to promote and maintain health.2–4
Health literacy is also essential for enhancing health and safety in the workplace. Occupational health status and behaviors are also related to health literacy, and in particular, health information comprehension in the workplace plays an important role in preventing work-related diseases and injuries.5 Rauscher and Myers6 defined Occupational Health Literacy (OHL) as the ability of workers to access, understand, appraise, and apply occupational health and safety information when making appropriate health decisions at work.
“Access” refers to the ability to obtain safety and health information, “understanding” to the ability to comprehend that information, “appraise” to the ability to assess the relevance of safety and health information and “apply” to the ability to utilize safety and health information.7
Meanwhile, a positive attitude was identified as an important factor in effectively processing and applying health-related information, and attitude was also considered to be an important factor in understanding occupational health information because workers with negative attitudes are more likely to fail to take effective disaster prevention measures. This relationship has been supported in previous studies.8,9
Occupational health literacy is associated with health outcomes such as well-being, subjective health status, and quality of life, and is also related to work ability.8,10–14 Employees who actively manage their health using a high level of understanding of occupational health information have improved job efficiency and better health status.15,16
Among occupational groups, agriculture is one of the most hazardous professions worldwide, with occupational injuries and diseases occurring at a much higher rate than the average for other professions.17–19 According to the International Labor Office of the United Nations, the cumulative incidence rate of occupational diseases due to chemical, biochemical, and physical hazards in the agricultural sector is 87.6 per 100,000 workers, among which 3.6 are due to biological hazards.19 Farmers are constantly exposed to physical, chemical, biological, and mechanical risks, the health outcomes of which can range from short-term injuries to long-term diseases. A lack of occupational health literacy can lead to work-related injuries, making the assessment of health knowledge the first step in protecting workers from potential occupational hazards.20
“Agricultural Safety and Health Literacy” (ASHL) is not a term commonly used in the existing literature, ASHL is a newly proposed conceptual framework developed in this study. It is defined here as an index for accurately recognizing risks that may arise in agricultural work environments, evaluating appropriate preventive measures or coping methods, and making the right health decisions. This concept is used to develop a tool for measuring the agricultural safety and health literacy of farmers.
Therefore, this study aimed to verify the validity and reliability of this approach by developing an ASHL instrument to assess and improve health information understanding in the agricultural sector. This product is expected to serve as an evaluation instrument for various safety and health projects in rural areas and to help manage the health and safety of farmers effectively.
Materials and Methods
Study Participants
The study population could read and write in Korean, were at least 19 years old, and had a minimum of one year of experience in agriculture. Farmers residing in four counties were recruited using a snowball sampling method. Participants were informed about the research purpose, methods, and their right to withdraw, and written consent was obtained before participation. It was important to have a sufficient number of participants in factor analysis. A previous study considered 200 subjects to be sufficient if the number of measurement variables did not exceed 40.21 Therefore, this study set the minimum sample size to 200, and 245 farmers ultimately participated in the survey.
And, the predictive validity was assessed to determine whether the education resulted in changes to the ASHL developed. A total of 31 farmers who participated in agricultural safety and disaster prevention education were surveyed, and their responses were collected both before the education and one week after to evaluate changes in ASHL.
Data was collected over one month in May 2024, following approval from the Institutional Review Board (IRB No, GIRB-A24-NY-0037). This study was conducted in accordance with the principles of the Declaration of Helsinki.
Instrument Development Process
The development of the instrument was conducted in four stages: drafting preliminary questions through literature review, reviewing the items with agricultural and health experts, conducting a preliminary survey, and executing the main survey (Figure 1).
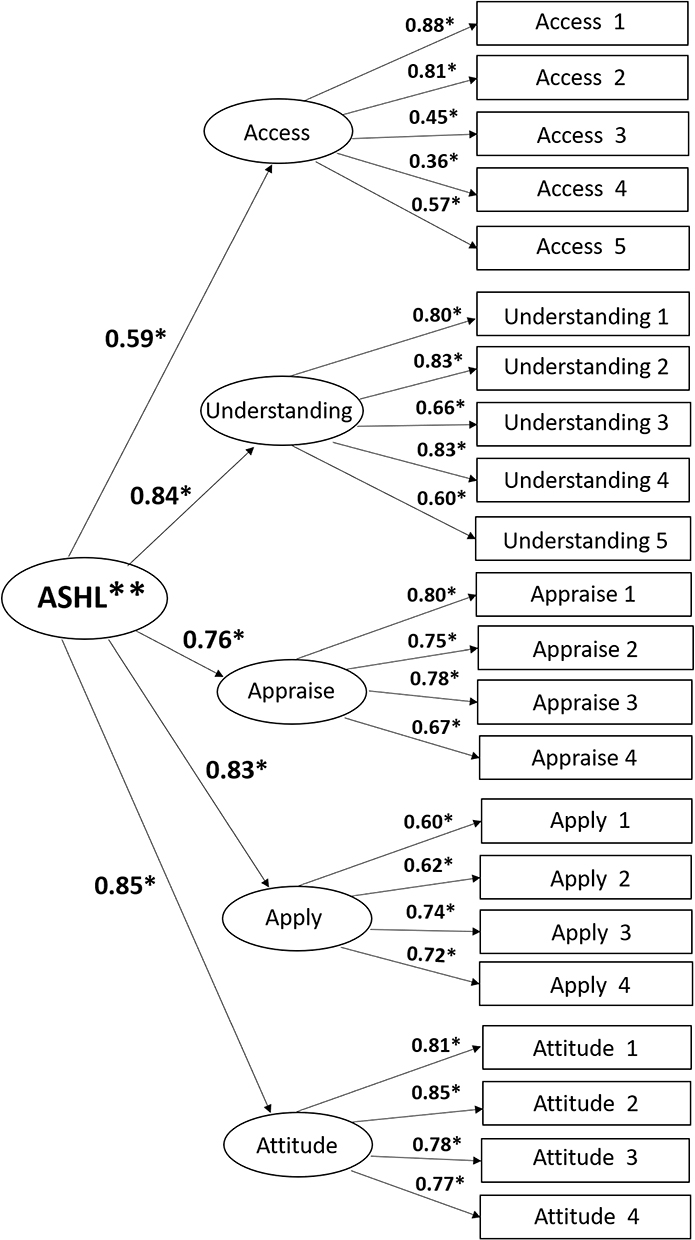 |
Figure 1 Confirmatory factor analysis result based on 22 items and 5 factors. *p<0.001. Abbreviation: ASHL, Agricultural Safety Health Literacy. |
Preliminary Items
The preliminary items for assessing agricultural safety and health literacy were initially developed by reviewing literature related to tools for occupational health literacy. This process involved selecting key individual-level items from the domain of Occupational Safety and Health Information.7 Specifically, the process included accessing, understanding, appraising, and applying health and safety information in agriculture, to which attitude was added as a factor. Attitude affects how individuals receive and apply health information.8 Thus, farmers with positive attitudes are more likely to understand health information accurately and use it effectively for preventive measures and coping strategies. An attitude of actively taking necessary actions to comply with safety guidelines and minimize risks is crucial for maintaining a safe working environment. Therefore, it was included in this study to provide a comprehensive evaluation of ASHL.
Items to be included in ASHL were developed with reference to existing occupational health literacy instrument.22–24 The sub-domains consisted of access, understand, appraise, apply, and attitude. To assess agricultural safety and health literacy, a self-reported 4-point Likert scale was used. The response options were: 1 (Strongly disagree), 2 (Disagree), 3 (Agree), and 4 (Strongly agree), with higher scores indicating higher levels of agricultural safety and health literacy.
Item Review
The preliminary items developed were reviewed by three experts with extensive experience and expertise in agriculture and health. Expert opinion was held considering the scale face and content validity,25 in other words, these experts evaluated the appropriateness, clarity, and validity of the items for tool development, leading to necessary revisions and improvements. Specifically, items containing difficult terminology were modified, the order of items was adjusted for readability, and an ambiguous question regarding the use of agricultural safety and health services under the “Access” factor was removed. The final item set, refined through expert discussion, consisted of 27 items: access (5 items), understanding (8 items), appraise (4 items), apply (6 items), and attitude (4 items).
Pretest
Before conducting the main survey, a pretest was administered to 20 farmers living in the same county as the main survey, using 27 items to evaluate respondents’ reactions. During this process, items that were difficult to understand, had ambiguous meanings, or could reduce reliability and validity were revised or eliminated. Specifically, items that were unclear in the “understanding” category, such as comprehension of agricultural safety and health guidelines, proper use of protective equipment, and exercises for musculoskeletal disorder prevention, were removed. In the “apply” category, items related to explaining agricultural disaster prevention methods to others and recommending agricultural safety insurance to peers were also removed. As a result, the final questionnaire comprised five factors: access (5 items), understanding (5 items), appraise (4 items), apply (4 items), and attitude (4 items), totaling 22 items. This instrument was named the ASHL (Supplementary Table).
Main Survey
The main survey was conducted with 245 farmers to evaluate the appropriateness of the ASHL instrument. Based on the preliminary survey analysis, 22 final items were used for survey responses, and a comprehensive analysis was performed to validate the instrument.
Statistical Analysis
For data analysis, the statistical programs SPSS-Win version 25.0 and R version 4.3 with the lavaan package were used. SPSS was utilized for descriptive statistics, Cronbach’s α, exploratory factor analysis, and paired t-tests. The lavaan package in R was used for confirmatory factor analysis. Lavaan is an R package specialized for structural equation modeling.
Cronbach’s α was measured to determine internal consistency, with values above 0.7 considered acceptable, above 0.8 good, and above 0.9 excellent.26
To examine the construct validity of the instrument, exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) were conducted. EFA was used to determine which factors each item in the ASHL questionnaire belonged to and to explore the structural relationships between factors, thus assessing the conceptual validity of the questionnaire. Principal component analysis was performed for EFA, and the Kaiser-Meyer-Olkin (KMO) measure and Bartlett’s test of sphericity were calculated to determine the suitability of the model for factor analysis. Generally, a KMO value of 0.80 or higher and a p-value <0.05 for Bartlett’s test indicate that the model is suitable for factor analysis.27 The varimax orthogonal rotation method was used to aid in interpreting the factors by rotating the explanatory axis of the variables.
CFA was applied to verify construct validity by ensuring that each factor accurately measured its respective sub-items. CFA was used to validate the factor structure derived from exploratory factor analysis, and structural equation modeling (SEM) tools were employed to evaluate model fit. Model fit was assessed using indices such as the goodness of fit index (GFI), adjusted goodness-of-fit index (AGFI), normed fit index (NFI), comparative fit index (CFI), and root mean square error of approximation (RMSEA). A GFI, AGFI, NFI, or CFI of 0.9 was considered good, while values above 0.8 were recommended. RMSEA values below 0.08 were advised, and the chi-square divided by degrees of freedom (χ2/df) was considered good if below 3.28,29
Predictive validity refers to measuring an external criterion in the future to examine its correlation. The developed scale was evaluated by comparing pre- and post-education groups to determine whether health literacy changed. To assess changes before and after the educational intervention, a paired t-test was conducted. This analysis confirmed whether the ASHL instrument could effectively predict improvements in farmers’ safety and health literacy after the educational intervention.
Results
General Characteristics of Participants
The general characteristics of the participants are shown in Table 1. Women accounted for 84.9% of the total participants, representing the majority. The largest age group was those in their 60s (56.7%), with an average age of 62.1 years. Regarding education level, 65.7% of participants had graduated from high school or higher. The marital status of 91.4% of participants was married. The average farming period was 25.6 years, with 23.3% having between 15 and 20 years of experience, and 23.7% having over 20 years of experience, indicating that most participants had extensive experience. The proportion of participants engaged in additional jobs outside of agriculture was 65.3%. The largest group of farmers (51.0%) was engaged in open-field farming, including rice paddies and dry fields. Regarding medical history, 64.1% of participants reported having a disease. Among major chronic diseases, hypertension was the most common (31.4%), followed by diabetes (11.4%), arthritis (31.4%), and other conditions (11.0%).
 |
Table 1 General Characteristics (N=245) |
Reliability Test
The overall Cronbach’s α for the ASHL scale was 0.92, indicating high reliability. Examining sub-factors, the Cronbach’s α for the access domain was 0.75. When each of the five items in this factor was individually removed, Cronbach’s α ranged between 0.65 and 0.77, indicating that no items reduced reliability. The understanding domain had a Cronbach’s α of 0.82, with values ranging from 0.76 to 0.81 when each of the five items was removed, confirming the suitability of all items. The appraise domain had a Cronbach’s α of 0.83, and when each of the four items was individually removed, values ranged from 0.77 to 0.82, ensuring all items were appropriate. The apply domain had a Cronbach’s α of 0.77, and removing each of its items resulted in values between 0.71 and 0.72, verifying their reliability. Lastly, the attitude domain had a Cronbach’s α of 0.88, with values ranging from 0.84 to 0.85 when individual items were removed, confirming that all items were suitable Thus, the overall reliability of the scale was high (Table 2).
 |
Table 2 Reliability of Agricultural Safety Health Literacy Instrument |
Validity Test
The resulting EFA for the 22 items of the Agricultural Safety and Health Literacy scale are shown in Table 3. The Bartlett’s test of sphericity was significant (p<0.001), confirming the suitability of the factor analysis, and the KMO measure was 0.904, exceeding the 0.80 threshold, which indicates adequacy. Based on eigenvalues greater than 1.0, five factors were extracted, accounting for 64.4% of the total variance. These five factors were: access (5 items), understanding (5 items), appraise (4 items), apply (4 items), and attitude (4 items).
 |
Table 3 Exploratory Factor Analysis of 22 Items on Agricultural Safety Health Literacy |
After conducting exploratory factor analysis, confirmatory factor analysis (CFA) was performed using the maximum likelihood method to estimate parameter values for the measurement model.
Since the five factors of ASHL are sub-factors of the overall concept, they are expected to be positively correlated, and each individual item was assumed to independently measure its corresponding sub-dimension. The confirmatory factor analysis results for the five-factor model showed the following key indices: Goodness of Fit Index (GFI)=0.851, Adjusted Goodness-of-Fit Index (AGFI)=0.816, Comparative Fit Index (CFI)=0.901, Normed Fit Index (NFI)=0.835, Root Mean Square Error of Approximation (RMSEA)=0.071, and chi-square divided by degrees of freedom (χ2/df) =2.2. These results indicate good fit (CFI, RMSEA, χ2/df) or at least acceptable fit (GFI, AGFI, NFI) (Table 4).
 |
Table 4 Model Fit in Confirmatory Factor Analysis |
Additionally, the standardized regression coefficients for the five factors and 22 individual items of ASHL ranged from 0.36 to 0.88, and all path coefficients were statistically significant at the p<0.001 level (Figure 1).
The predictive validity of the developed ASHL was assessed by measuring changes before and after education. In the “Access” domain, the average score increased from 2.5 before training to 2.7 after training (p=0.004), indicating that the training effectively improved information access skills. In the “Understanding” domain, the average score increased from 3.1 to 3.4 (p=0.002), demonstrating that the training contributed to enhancing comprehension skills. In the “Appraise” domain, scores rose from an average of 2.6 before training to 3.3 after training (p<0.001), suggesting that the training significantly improved the ability to evaluate information. For the “Apply” domain, the average score increased from 2.8 to 3.1 (p=0.005), indicating that the training positively influenced the ability to utilize information. Finally, in the “Attitude” domain, the score improved from 3.2 to 3.5 (p<0.001), suggesting that the training led to a positive change in farmers’ attitudes toward health and safety information (Figure 2).
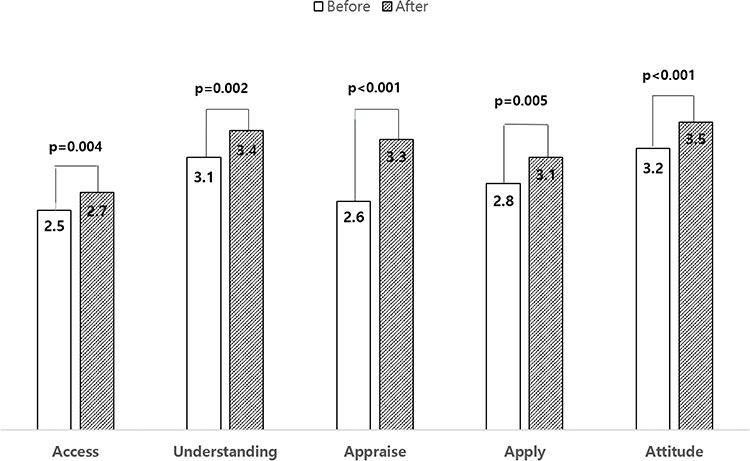 |
Figure 2 Comparison before and after education to evaluate the predictive validity. |
Discussion
This study developed a new instrument to measure ASHL based on existing occupational health and safety literacy assessment instruments. The developed tool was designed to evaluate how well farmers understand and apply safety and health-related information in agricultural work. The ASHL instrument consists of five factors: Access (5 items), Understanding (5 items), Appraise (4 items), and Apply (4 items), with an additional Attitude factor (4 items) that plays a crucial role in health-related decision making, for a total of 22 items. The entire questionnaire was structured using a 4-point Likert scale, where higher scores indicate a higher level of literacy.
The instrument was developed through a review of occupational health and safety literacy literature and validated by agricultural health and safety experts, which likely strengthened its face and content validity.22,28 The resulting EFA confirmed that the 22 items were appropriately categorized into the intended five factors. These domains align with the study by Suthakorn,23 which developed a tool to assess occupational health literacy in Thailand, as well as Friedrich et al,24 which validated a measurement tool applicable to various occupational groups in Germany. This alignment suggests that the tool effectively captures the conceptual structure of personal-level occupational health literacy as defined in occupational safety and health information frameworks.7
Becker30 asserted that health behavior is directly influenced by an individual’s attitude. By incorporating the attitude domain into the developed ASHL in addition to the four domains from previous studies,6 this instrument highlights the significance of attitude in health behavior change and broadens its conceptual framework. The inclusion of the “attitude” domain in the ASHL instrument is supported by recent evidence highlighting the role of safety knowledge and personal health experiences in shaping farmers’ protective behaviors. For instance, Imran et al31 demonstrated that attitude significantly influenced pesticide safety practices among fruit and vegetable farmers in Pakistan.
Previous health literacy tools developed in similar research across different fields5 were generally applicable to all occupations but struggled to reflect the unique working environment of agriculture. This study, by incorporating the characteristics of agricultural work, ensures that the ASHL not only assesses farmers’ ability to access, understand, appraise, and apply health and safety information, but also emphasizes improving health behavior through a positive attitude. Ultimately, this instrument will play a critical role in promoting the health and safety of farmers.
To further validate the factor structure derived from EFA, confirmatory factor analysis was used to evaluate model fit, showing that the key indices were acceptable to good.24 This study reported favorable results for the CFI and RMSEA, although this study showed slightly lower values for the GFI and AGFI. However, since the key indices indicated at least acceptable or good fit, it is believed that each domain appropriately represents a sub-dimension of the overarching concept. Furthermore, including the additional attitude factor in this study, beyond the traditional four factors used in previous research, might provide a more comprehensive assessment.
The overall Cronbach’s α for all 22 items of the five factors was 0.92, indicating high reliability.26 The reliability of all five factors remained above 0.7, demonstrating that the tool provides a consistent evaluation across multiple aspects. This supports the reliability of the Agricultural Safety and Health Literacy assessment instrument, suggesting its validity. The high reliability measured in this study enhances its applicability in real-world settings. Utilizing the developed tool in educational programs aimed at improving Agricultural Safety and Health Literacy is expected to yield more reliable assessment results.
The predictive validity of the tool was confirmed by measuring score changes before and after the educational intervention. Overall, all factors in ASHL showed positive changes from before to after education. However, the relatively low score in the “Access” domain highlights the need for additional support to enhance information accessibility for farmers. Future research should explore specific strategies to improve access and develop diverse educational approaches to continuously enhance farmers’ overall health and safety literacy.
This study had several limitations. First, since the survey was conducted on farmers from four cities and counties, the sample may not be representative of the entire farming population. Future studies should expand the study area to ensure broader representation of farmers. Second, given that the majority of participants were female farmers, the results may be subject to bias. Female farmers tend to participate more actively in agricultural training programs, but future studies should include a more diverse sample, particularly male farmers. Third, since this study used a newly developed tool, its predictive validity has not been compared with existing standardized tools. Future research should consider longitudinal validation to determine whether ASHL can predict long-term health outcomes in agricultural workers. Additionally, it would be meaningful to explore the applicability of the tool in diverse international agricultural settings.
Nonetheless, this study demonstrated that the developed tool had good reliability and validity, and significant changes were observed before and after training. This confirmed that the instrument was successfully developed as intended by the researchers. Furthermore, the instrument was designed with survey items that reflect the unique agricultural context in Korea while maintaining a relatively small number of items.
Conclusions
This study was the first to develop and validate an instrument for assessing ASHL, making a significant contribution. The developed instrument is expected to play an essential role in improving farmers’ health behaviors and preventing and effectively managing various health issues that may arise in agricultural work environments.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
Ethical approval was obtained from the institutional review board in Gyeongsang National University, Korea (Reference number: GIRB-A24-NY-0037). All participants provided written informed consent. This study was conducted in accordance with the principles of the Declaration of Helsinki.
Consent for Publication
Yes
Acknowledgments
We are deeply grateful to the farmers who kindly participated in the survey. Our special thanks also go to Prof. HS Song and Prof. YM Ha for their expert guidance in the assessment of face and content validity of the instrument.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by a grant from the Agricultural Science and Technology Research and Development Project (RS-2022-RD010387), Rural Development Administration, Republic of Korea.
Disclosure
The authors declare no competing interest in this work.
References
1. Sørensen K, Van den Broucke S, Fullam J, et al; (HLS-EU) Consortium Health Literacy Project European. Health literacy and public health: a systematic review and integration of definitions and models. BMC Public Health. 2012;12:80. doi:10.1186/1471-2458-12-80
2. Peerson A, Saunders M. Health literacy revisited: what do we mean and why does it matter? Health Promot Int. 2009;24:285–296. doi:10.1093/heapro/dap014
3. Malloy-Weir LJ, Charles C, Gafni A, Entwistle VA. Empirical relationships between health literacy and treatment decision making: a scoping review of the literature. Patient Educ Couns. 2015;98:296–309. doi:10.1016/j.pec.2014.11.004
4. Bröder J, Chang P, Kickbusch I, Levin-Zamir D. IUHPE position statement on health literacy: a practical vision for a health literate world. Glob Health Promot. 2018;25(4):79–88. doi:10.1177/1757975918814421
5. Ehmann AT, Ög E, Rieger MA, Siegel A. Work-related health literacy: a scoping review to clarify the concept. Int J Environ Res Public Health. 2021;18(19):9945. doi:10.3390/ijerph18199945
6. Rauscher KJ, Myers DJ. Occupational health literacy and work-related injury among U.S. adolescents. Int J Inj Contr Saf Promot. 2014;21(1):81–89. doi:10.1080/17457300.2013.792288
7. Jørgensen MB, Larsen AK. Occupational health literacy: healthy decisions at work. In: Okan O, Bauer U, Levin-Zamir D, Pinheiro P, Sørensen K, editors. International Handbook of Health Literacy: Research, Practice and Policy Across the Life-Span. Bristol, UK: Policy Press; 2019:347–358.
8. Friedrich J, Rupp M, Feng YS, Sudeck G. Occupational health literacy and work ability: a moderation analysis including interpersonal and organizational factors in healthy organizations. Front Public Health. 2024;12:1243138. doi:10.3389/fpubh.2024.1243138
9. Wang J, Mo C, Sheng Q, et al. Association of length of service and job category with occupational health literacy of port employees in Shenzhen, China. BMC Public Health. 2023;23:1223. doi:10.1186/s12889-023-15769-7
10. Tokuda Y, Doba N, Butler JP, Paasche-Orlow MK. Health literacy and physical and psychological wellbeing in Japanese adults. Patient Educ Couns. 2009;75(3):411–417. doi:10.1016/j.pec.2009.03.031
11. Zheng M, Jin H, Shi N, et al. The relationship between health literacy and quality of life: a systematic review and meta-analysis. Health Qual Life Outcomes. 2018;16(1):201. doi:10.1186/s12955-018-1031-7
12. Fiedler S, Pfaff H, Soellner R, Pförtner TK. Exploring the association between health literacy and psychological well-being among industry managers in Germany. J Occup Environ Med. 2018;60(8):743–753. doi:10.1097/JOM.0000000000001324
13. Ehmann AT, Groene O, Rieger MA, Siegel A. The relationship between health literacy, quality of life, and subjective health: results of a cross-sectional study in a rural region in Germany. Int J Environ Res Public Health. 2020;17(5):1683. doi:10.3390/ijerph17051683
14. Lindert L, Choi KA, Pfaff H, Zeike S. Health literacy at work - individual and organizational health literacy, health supporting leadership and employee wellbeing. BMC Health Serv Res. 2023;23(1):736. doi:10.1186/s12913-023-09766-0
15. Stassen G, Grieben C, Hottenrott N, Rudolf K, Froböse I, Schaller A. Associations between health-related skills and young adults’ work ability within a structural health literacy model. Health Promot Int. 2021;36(4):1072–1083. doi:10.1093/heapro/daaa099
16. Fowles JB, Terry P, Xi M, Hibbard J, Bloom CT, Harvey L. Measuring self-management of patients’ and employees’ health: further validation of the Patient Activation Measure (PAM) based on its relation to employee characteristics. Patient Educ Couns. 2009;77(1):116–122. doi:10.1016/j.pec.2009.02.018
17. Walker-Bone K. Musculoskeletal disorders in farmers and farm workers. Occup Med. 2002;52(8):441–450. doi:10.1093/occmed/52.8.441
18. Rim K, Lim C. Biologically hazardous agents at work and efforts to protect workers’ health: a review of recent reports. Saf Health Work. 2014;5(2):43–52. doi:10.1016/j.shaw.2014.03.006
19. Nguyen THY, Bertin M, Bodin J, Fouquet N, Bonvallot N, Roquelaure Y. Multiple exposures and coexposures to occupational hazards among agricultural workers: a systematic review of observational studies. Saf Health Work. 2018;9(3):239–248. doi:10.1016/j.shaw.2018.04.002
20. Wong BK. Building a health literate workplace. Workplace Health Safety. 2012;60(8):363–369. doi:10.1177/216507991206000806
21. Devellis R. Scale Development: Theory and Applications. Los Angeles: Sage; 2012:80.
22. Azizi N, Karimy M, Abedini R, et al. Development and validation of the health literacy scale for workers. Int J Occup Environ Med. 2019;1:30–39. doi:10.15171/ijoem.2019.1498
23. Suthakorn W, Songkham W, Tantranont K, Srisuphan W, Sakarinkhul P, Dhatsuwan J. Scale development and validation to measure occupational health literacy among Thai informal workers. Saf Health Work. 2020;11(4):526–532. doi:10.1016/j.shaw.2020.06.003
24. Friedrich J, Münch AK, Thiel A, Voelter-Mahlknecht S, Sudeck G. Occupational Health Literacy Scale (OHLS): development and validation of a domain-specific measuring instrument. Health Promot Int. 2023;38(1):daac182. doi:10.1093/heapro/daac182
25. Imran M, Aziz A, Hamid SNA. Determinants of SME export performance. Int J Data and Netw Sci. 2017;1:39–58. doi:10.5267/j.ijdns.2017.1.007
26. Peterson RA. A meta-analysis of Cronbach’s coefficient alpha. J Consum Res. 1994;21(2):381–391. doi:10.1086/209405
27. Yang C, Chen Y, Zhao X. Emotional labor: scale development and validation in the Chinese context. Front Psychol. 2019;10:2095. doi:10.3389/fpsyg.2019.02095
28. Shahsavari H, Bakhshi F, Khosravi A, Najafi Z, Ghorbani A. Perceived professional preparedness of senior nursing students’ instrument: development and psychometric evaluation. Nurse Educ Today. 2020;93:104533. doi:10.1016/j.nedt.2020.104533
29. Ye ZJ, Liang MZ, Li PF, et al. New resilience instrument for patients with cancer. Qual Life Res. 2018;27(2):355–365. doi:10.1007/s11136-017-1736-9
30. Becker MH. The tyranny of health promotion. Public Health Rev. 1986;14(1):15–23.
31. Imran M, Mustafa G, Rehman SU, Yasri Y. The interplay of safety knowledge, attitude and health experience in adoption of protective pesticide behavior: evidence from Pakistani fruit and vegetable farmers. J Agribus Dev Emerg Econ. 2024. doi:10.1108/JADEE-05-2024-0148
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Think Before You Take: Understanding Adult Medication Literacy in Saudi Arabia
Alhomoud F, Alsaeed W, Alzainaldain F, Alelq K, Alhomoud FK, Alamer KA, Alsultan MM, Alqarni YS, Alshehail B, Alhifany AA
Patient Preference and Adherence 2025, 19:1973-1990
Published Date: 10 July 2025