")
Back to Journals » Patient Preference and Adherence » Volume 18
Development and Validation of the Healthcare-Seeking Intention Questionnaire in Patients with Diabetic High-Risk Foot
Authors Wang H, Li N, Ye Y, Zhao N, Liu M, Xu M, Zhou Q
Received 23 May 2024
Accepted for publication 29 August 2024
Published 12 September 2024 Volume 2024:18 Pages 1873—1883
DOI https://doi.org/10.2147/PPA.S479644
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Honglin Wang,1,2,* Na Li,1,3,4,* Ying Ye,5 Nan Zhao,6 Meizi Liu,1 Min Xu,3 Qiuhong Zhou3,4
1Xiangya School of Nursing, Central South University, Changsha, People’s Republic of China; 2School of Health and Nursing, Guangzhou Huali College, Jiangmen, People’s Republic of China; 3Teaching and Research Section of Clinical Nursing, Xiangya Hospital of Central South University, Changsha, People’s Republic of China; 4National Clinical Research Center for Geriatric Disorders, Xiangya Hospital of Central South University, Changsha, People’s Republic of China; 5Department of Nursing, First People’s Hospital of Yunnan, Kunming, People’s Republic of China; 6School of Nursing, Zhengzhou Shuqing Medical College, Zhengzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qiuhong Zhou, Teaching and Research Section of Clinical Nursing, Xiangya Hospital of Central South University, Changsha, 410008, People’s Republic of China, Tel +8613786136512, Email [email protected]
Objective: Timely screening and intervention can prevent the development of the diabetic foot. However, delayed visits to the clinic are common among diabetic foot patients. The study aimed to develop and validate a questionnaire to assess healthcare-seeking behavior among patients with diabetic high-risk foot.
Methods: The questionnaire of healthcare-seeking intention for patients with diabetic high-risk foot was developed in two phases: (1) Developing the questionnaire: 1) questionnaire items were formulated after literature review, group discussion and semi-qualitative interview; 2) a two-round modified Delphi method was to examine the content validity and the degree of consistency in questionnaire items; 3) conducting pre-survey to revise the questionnaire items. (2) Assessing the internal reliability and construct validity.
Results: The final questionnaire consisted of five main themes and 28 items with a five-point rating. Cronbach’s alpha coefficients for the five dimensions were respectively 0.937 (relevant knowledge of diabetic foot), 0.669 (attitudes toward seeking care), 0.896 (social support for seeking care), 0.621 (efficacy in coping with foot symptoms), 0.871 (intention to seek care). The Scale-level Content Validity Index of the five parts was 1.00, 0.80, 1.00, 1.00, and 1.00, respectively. The Kaiser-Meyer-Olkin values for each dimension was greater than 0.7, and the p-value for Bartlett’s test of sphericity was less than 0.05.
Conclusion: This questionnaire showed good validity, internal consistency, and reliability. It provided a potentially useful instrument to evaluate healthcare-seeking intention among patients with diabetic high-risk foot.
Keywords: healthcare-seeking intention, questionnaire development, high-risk foot, patients
A Letter to the Editor has been published for this article.
Introduction
Diabetic foot (DF) is a serious complication of diabetes mellitus, with high levels of mortality, amputation, and recurrence, as well as high financial costs.1–3 A quarter of all people with diabetes may develop a DF.1 Approximately 80% of diabetes-related lower extremity amputations are preceded by foot ulcers,4 and these patients have lower survival rates.5 Individual factors and the burden of illness put this group at a significantly increased risk of depression or anxiety.6 Regular foot inspection can recognize skin damage.7 Managing risk factors of DF, timely foot screening and foot care can prevent the development of DF.8 However, timely access to medical care for DF patients is poor. The median pre-hospital delay time for patients with DF was 46.49 days.9 Many patients with DF in the early stages of the disease tried to initially manage foot problems themselves by cleaning and disinfecting the wound at home.10 Patient will to go primary health care if above treatment at home does not work. Unfortunately, they are often seen at a time when the best treatment is missed, resulting in a significant chance of amputation or non-healing wounds. Meanwhile, limited knowledge and awareness around DF, a lack of finance have an impact on timely healthcare-seeking.11 High-risk foot is the early stage of DF, which means that no foot ulcer has occurred but there are risk factors that predispose to ulceration.12 Consequently, it is very critical to assess the intention of patients with diabetic high-risk foot to seek medical attention at an early stage.
Currently, few measures that assess early healthcare-seeking intention for patients with diabetic high-risk foot exist. Existing assessments of healthcare-seeking intention have focused on cancer patients, parents, cough patients and patients with psychological disorders.13–16 Nevertheless, these scales are not universal and cannot be applied to assess patients with diabetic high-risk foot. In addition, the development process of some questionnaires was not reported. To our knowledge, there is almost no high-quality tool specifically for assessing healthcare-seeking intention for patient with diabetic high-risk foot. The aim of this study was to develop and validate a questionnaire to assess the level of healthcare-seeking intention for people with diabetes at the onset of early foot symptoms.
The theory of Planned Behavior (TPB) was developed by Ajzen and is often used as an inquiry into certain behavioral intentions, which pointed out that human action is guided by three kinds of considerations (including behavioral beliefs, normative beliefs and control beliefs).17 It consists of five components, namely, attitude toward the behavior, subjective norm, perceived behavioral control, intention and behavior.18 TPB emphasizes that the more favorable the attitudes and subjective norm, the greater the perceived control, the stronger the person’s intention to perform the behavior, and if there is a sufficient degree of actual control over the behavior, people will perform their intentions when the opportunity arises.17 Yi et al19 investigated perceptions and acceptability of HPV vaccination for female adolescents based on TPB. Dadipoor et al20 applied TPB to construct a predictive model waterpipe smoking cessation. Meanwhile, behavior is also influenced by the relevant knowledge of the actor.21 Therefore, we used TPB to guide the development of the healthcare-seeking intention questionnaire, and in the process of questionnaire development, we also integrate the Knowledge-Belief-Behavior (KAP) Theory to explain the healthcare-seeking behavior.
Methods
The development and validation of the questionnaire on healthcare-seeking intention of diabetic high-risk foot patients occurred in two phases: (1) developing the questionnaire. (2) an assessment of internal reliability and construct validity. The detailed study design flow chart was shown in Figure 1.
 |
Figure 1 The study design flow chart. |
Phase 1: Developing the Questionnaire
The questionnaire development process involved the three stages: creating a pool of items, a two-round modified Delphi method, and pre-survey.
In the first stage, we constructed 21 items primarily based on the TPB, literature review and group discussion. And then we conducted semi-structured interviews. The interview outline included the seven aspects: 1) What do you think is DF? 2) What do you think are the symptoms (manifestations) of DF in the early stage? 3) When these symptoms occur in your foot, how do you respond to them? 4) What do you think are the advantages and disadvantages of going to the hospital for treatment when these foot symptoms occur? 5) Who are the people who would influence you to seek treatment in the hospital? 6) What are the other reasons that may influence you to seek treatment? 7) Under what circumstances would you choose to go to the hospital for treatment? And a convenience sampling method was used to interview patients with diabetic high-risk foot.22 The time of each interview was controlled at 30~40 minutes. We interviewed eleven participants, finding that the knowledge had a great influence on the behavior. At the same time, more studies proved that knowledge can have a direct or indirect impact on the behavioral intentions of individuals.23–25 KAP also proposed that healthy knowledge is a crucial basis for developing positive attitudes and further health behavior change.26 Therefore, we combined the TPB and KAP, and constructed the theoretical framework of this study (Figure 2).
 |
Figure 2 Theoretical framework of healthcare-seeking intention for patients with diabetic high-risk foot. |
In the second stage, we used two rounds of Delphi surveys to ask experts to rate each question for content. The electronic version of the questionnaire was sent to 16 experts, of whom the inclusion criteria were: ① research or clinical medical work in DF-related fields; ② clinical work experience ≥ 10 years or research experience ≥ 5 years; ③ associate senior title or above; ④ bachelor degree or above; ⑤ informed consent; and exclusion of those who did not complete within the corresponding time frame. Expert rated the items on a scale of 1 to 5 (1=very unimportant, and 5= very important). In addition, the familiarity of the questionnaire and the basis for judgment were assessed. We used the response rate to the questionnaire to reflect the extent of experts’ concern about the study, and authority coefficient (Cr) is used to indicate authority degree of expert opinion, which reflects the reliability of the findings.27
In the final stage, thirty patients with diabetic high-risk foot who met the inclusion and exclusion criteria were selected from urban communities for a pre-survey. Inclusion criteria for these patients were as follows: (i) diabetic patients with peripheral neuropathy and intact skin on the foot;22 (ii) those who could communicate normally; (iii) those who voluntarily participated in this study. We excluded those with serious physical diseases (such as cardiac, cerebral, or pulmonary diseases or tumors) or psychiatric diseases, those with neurological symptoms caused by other diseases (such as cervical spine and lumbar spine) and those who were being treated in hospital for foot problems. This phase collects the problems of patients in the process of filling out the items and make adjustments and changes to the items.
Phase 2: An Assessment of Reliability and Validity
Six experts were selected to evaluate the content validity of the final questionnaire, namely, experts evaluated the relevance of the items (1=not relevant, 2=weakly relevant, 3=strongly relevant, 4=very relevant). The experts were selected based on the same criteria as the expert correspondence. Furthermore, based on Kendall’s sample size calculation28 (the sample size of the reliability and validity test is 5~10 times of the number of evaluation tool items), we used convenience sampling methods to select 200 patients with diabetic high-risk foot from urban communities to conduct reliability and validity tests of the questionnaire. Patient selection criteria for this stage were consistent with those for patients in the pre-survey. The final questionnaire was distributed on site for the participants to fill out voluntarily. Meanwhile, socio-demographic information of the participants was collected, such as gender, age, education level, marital status, economic status, and duration of diabetes. The study leader checked the quality of the questionnaires while retrieving them, and if there were any omissions, promptly asked the participants to add them and actively answered their doubts.
Statistical Analysis
After the questionnaires were returned, they were checked and entered into Microsoft Office Excel by two researchers. All statistical analyses were performed using IBM SPSS for version 26.0. Statistical descriptions were expressed as means, standard deviations, frequencies and percentages. Then we analyzed the coefficient of expert positivity, the degree of expert opinion concentration, the degree of expert opinion coordination, and the degree of expert opinion authority. Meanwhile, items with mean importance score > 3.5 and coefficient of variation (CV) < 0.25 were retained as guidelines29 in two rounds of Delphi, and items were selected by combining literature review and subject panel discussion. The item analysis was conducted using the Critical Ratio (CR) method, correlation coefficient method, and reliability analysis method. In this study, six experts specializing in the field of DF used a 4-point relevance rating scale to evaluate the questionnaire, calculating the Item-level Content Validity Index (I-CVI) and the Scale-level Content Validity Index (S-CVI). An I-CVI of ≥0.78 and S-CVI of ≥0.70 are deemed acceptable.30 An exploratory factor analysis was conducted to evaluate the structural validity of the questionnaire. Factor analysis was determined based on the magnitude of the Kaiser-Meyer-Olkin (KMO) measure. Internal reliability was tested using Cronbach’s alpha (Cronbach’s α).
Ethics Statement
Prior to the start of the survey, we explained the purpose and content of the study to the participants and obtained their verbal consent, which was acceptable and approved by the Ethics Committee of Xiangya Hospital, Central South University (Reference number 202306127). And the study entirely complied with the Declaration of Helsinki.
Results
Phase 1: Developing the Questionnaire
We conducted semi-structured interviews with eleven patients with diabetic high-risk foot. The mean age of these patients was 70.09±5.68 years. And the average duration of diabetes was 13.27±9.11 years. According to semi-structured interviews, there were five dimensions were initially developed as well as 36 items, namely, relevant knowledge of diabetic foot (A,7 items), attitudes toward seeking care (B,15 items), social support for seeking care (C,6 items), efficacy in coping with foot symptoms (D,4 items), intention to seek care (E,4 items).
Sixteen experts reviewed our questionnaires. Among the experts, 9 were nurses and 7 were doctors. Male and female accounted for 25% and 75%, respectively, with an average age of 48.63 ± 8.17, and an average work year of 26.75 ± 10.56. Experts with senior professional post titles accounted for 93.70%. The response rates were both 100% in two rounds of Delphi method. Meanwhile, the Cr of Delphi round 1 was 0.93 and Delphi round 2 was 0.97. Experts suggested adding 10, deleting 9, and revising 6 items in round 1 and deleting 1, merging 2, revising 2 items in round 2. Finally, there were five dimensions and 35 items, namely, relevant knowledge of diabetic foot (A,11 items), attitudes toward seeking care (B,9 items), social support for seeking care (C,6 items), efficacy in coping with foot symptoms (D,5 items), intention to seek care (E,4 items). Table 1 showed Kendall’s W for two rounds.
 |
Table 1 The Coordination Degree and Significance Test of Delphi Method |
Phase 2: An Assessment of Reliability and Validity
200 questionnaires were distributed to patients with diabetic high-risk foot in urban communities. We detailed the purpose and significance of this study to participants at the beginning of the survey, and conducted face-to -face questionnaire collection, but 16 participants opted out during the questionnaire completion process. Therefore, 184 of recovered questionnaires were valid, and the response rate was 92.0% in the study. Table 2 showed the demographic characteristic of participants.
 |
Table 2 General Characteristics of Survey Participants (N=184) |
Item Analysis
CR method and correlation coefficient method were used to item analysis (Table 3). Participants were ranked in descending order based on their total score, with 27% as the critical rate. Participants with total scores in the top 27% were considered as the high group and those with total scores in the bottom 27% were considered as the ground group.31 Analysis was performed using independent samples t-test. Based on the principle that items with CR values < 3 or insignificant p-values should be deleted,32 we deleted D2. Then we calculated the correlation coefficient between score per item and the total score by Pearson correlation coefficient method. And according to the principle that items with correlation coefficient r <0.4 or insignificant p-values should be deleted,33 we deleted B7, D3.
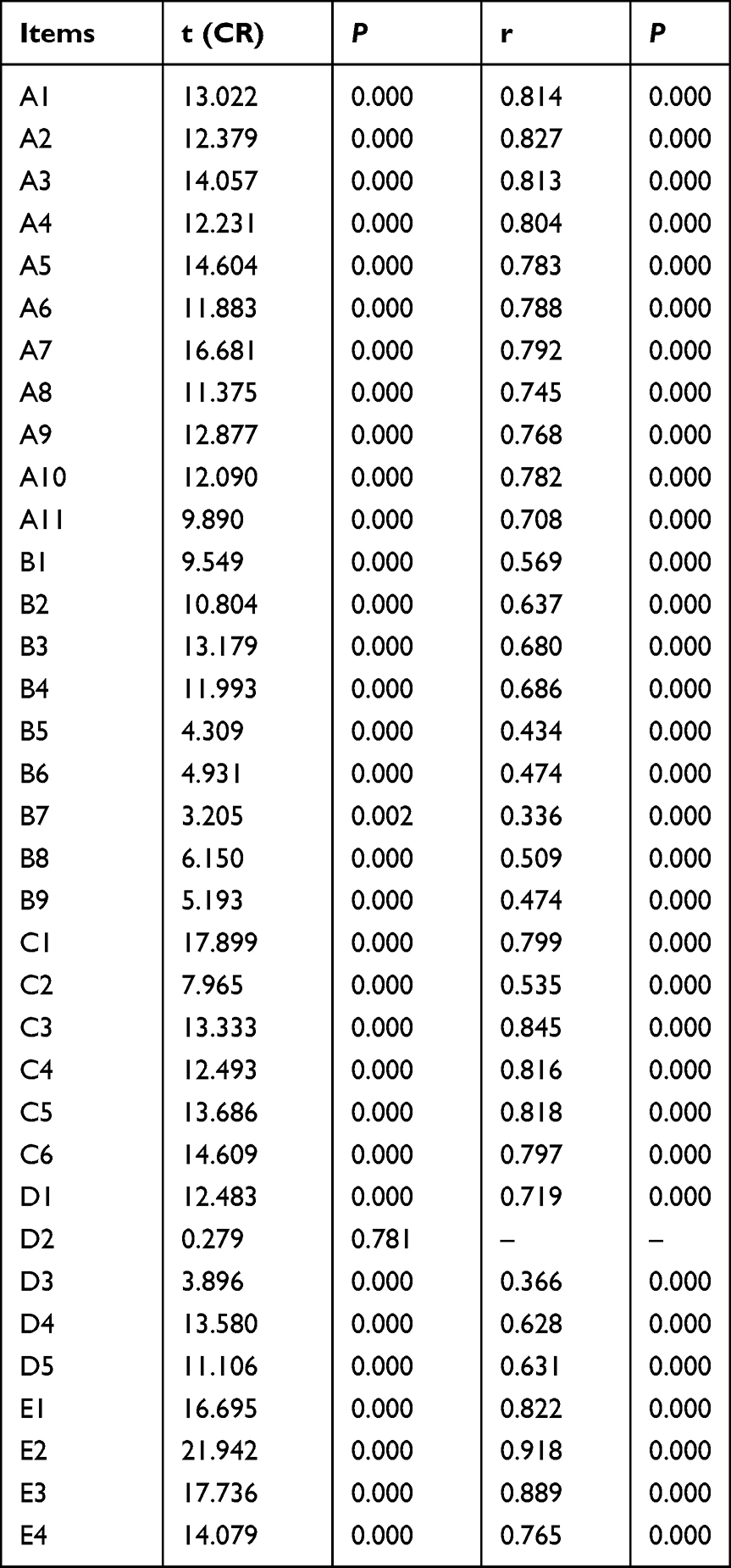 |
Table 3 Item Analysis Result of the Questionnaire |
The questionnaire, after the aforementioned screening, underwent further item screening using reliability analysis. The Cronbach’s α coefficient for each dimension of the questionnaire, the corrected item-total correlation (CITC), and the Cronbach’s α coefficient if item deleted (CAID) were calculated, as shown in Table 4. Based on the principle of deleting items where CITC < 0.4 and CAID is greater than the overall Cronbach’s α coefficient, items B5, B9, B6, and C2 were removed.
 |
Table 4 Reliability Analysis Results of the Questionnaire |
Reliability Analysis
Cronbach’s α coefficients for the five dimensions were respectively 0.937 (relevant knowledge of diabetic foot), 0.669 (attitudes toward seeking care), 0.896 (social support for seeking care), 0.621 (efficacy in coping with foot symptoms), 0.871 (intention to seek care).
Validity Analysis
After being evaluated by 6 experts, each I-CVI was above 0.78, and the S-CVI values for the five dimensions: relevant knowledge of diabetic foot, attitudes toward seeking care, social support for seeking care, efficacy in coping with foot symptoms, intention to seek care, were 1.00, 0.80, 1.00, 1.00, and 1.00, respectively. Table 5 displayed the results.
 |
Table 5 Content Validity Analysis Results of the Questionnaire |
Due to the inability to aggregate scores across dimensions in the questionnaire devised for this study, exploratory factor analysis was precluded. Consequently, each dimension underwent KMO test and sphericity test. The results showed that the KMO values for each dimension was greater than 0.7, and the p-value for Bartlett’s test of sphericity was less than 0.05, indicating that the dimensions have good construct validity.31
Discussions
The prevention and treatment of DF has always been the focus and difficulty in clinical practice. Many studies7,8,34,35 have demonstrated that timely and targeted treatment measures in the early stages of DF can effectively improve the clinical outcomes of patients. According to the TBP, patients’ healthcare-seeking behavior is directly influenced by their intention to seek medical care.18 However, no assessment tool has been reported for evaluating the healthcare-seeking intention of diabetic high-risk foot patients. Therefore, it is necessary to develop an effective and scientific assessment tool.
This study was guided by the TBP and the KAP, combining with literature review, group discussion, and semi-structured interviews constructed the pool items. And items of the scale were selected and refined through two rounds of expert consultations. Since the response rates of the experts were both 100%, the authority coefficients of the experts were 0.93 and 0.97, and the Kendall’s W were 0.145 and 0.133 (P<0.001), we concluded that the experts had a good representation, a high degree of positivity and authority, and that consensus among the experts was statistically significant.
Cronbach’s α was calculated to examine internal consistency of the scale. The results revealed that Cronbach’s α coefficients of all dimensions were in the range of 0.62~0.94, indicating that the internal consistency of the scale was satisfactory.36 Validity refers to the extent to which the scale a scale accurately captures the constructs under investigation, including content validity and construct validity. According to our results, each I-CVI was above 0.78 and S-CVI was above 0.80, showing that the questionnaire items were accurate and comprehensive.37 Although the KMO values in this study were all greater than 0.7, and the sphericity test was significant, the questionnaire developed for this study did not allow for the aggregation of scores across dimensions. While traditional exploratory factor analysis typically requires the total score of the questionnaire as a latent variable, and confirmatory factor analysis model requires endogenous latent variables. Therefore, it was not appropriate to conduct either exploratory or confirmatory factor analyses on this questionnaire.
The final questionnaire covered 5 dimensions. “Relevant knowledge of diabetic foot” (dimension A) mainly contained the definition, etiology, early symptoms, treatment and nursing of DF. Studies revealed that heightened levels of knowledge foster favorable attitudes and perceived behavioral control, consequently leading to elevated levels of intentions.38,39 As a result, this dimension identifies patients with inadequate disease knowledge and prompts healthcare professionals to enhance health education, thereby improving patients’ intention to seek treatment. “Attitudes toward seeking care” (dimension B) estimated the impact that patients perceive healthcare-seeking to have on their lives, encompassing daily life plans, work, family, and travel. Attitude is a strong predictor of healthcare-seeking intentions.40 If patients hold a proactive belief in the potential of early medical intervention to DF, their intention to seek medical care is heightened. Thus, approaches could highlight the beneficial results of early medical care such as showcasing successful prevention cases. “Social support for seeking care” (dimension C) accessed the people or groups that affected patients’ healthcare-seeking decisions, such as family, friends, neighbors, and diabetic patients. Individuals are more inclined to engage in a specific behavior when it receives encouragement and support from significant social influences.39 This suggests that healthcare providers can promote early healthcare-seeking behaviors by involving patient families in health promotion and harnessing peer influence.“Efficacy in coping with foot symptoms” (dimension D) evaluated patients’ ability to manage foot problems. Sheeran et al41 pointed out that coping efficacy could promote healthy behavior changes. However, Tao et al29 found that patients’ coping efficacy might hinder their intention to seek medical care. Therefore, it is crucial to enhance health education about risk screening, foot care, timing of visits, further to cultivate the correct attitude and skills for health behavior. “Intention to seek care” (dimension E) measured the patients’ implementation willingness, as well as their self-management ability. The intention to seek care is correlated with many factors such as knowledge, attitude, social support, coping efficacy and so on. For patients with a low level of healthcare-seeking intention, medical staff should analyze their obstacles and formulate targeted program.
In a word, the questionnaire developed in this study measured the intention of healthcare-seeking for patients with diabetes at the onset of early foot symptoms from multiple perspectives, which had strong clinical practice significance and guidance. However, there are some limitations noteworthy to mention. First, since we assessed the intention of healthcare-seeking for diabetic patients with high-risk foot at a given point in time using the scale, longitudinal data is suggested to collect to investigate its test–retest reliability, responsiveness and interpretability. Second, although we developed a new scale to measure the intention of healthcare-seeking among Chinese diabetic patients with high-risk foot, further research is required to confirm the usefulness of the scale in other countries. Further research is needed to refine the scale to increase the generalization of the current results.
Conclusion
Our study created the first measurement tool to evaluate the intention of healthcare-seeking for patients with diabetes at the onset of early foot symptoms. Five dimensions were revealed, namely “relevant knowledge of diabetic foot”, “attitudes toward seeking care”, “social support for seeking care”, “efficacy in coping with foot symptoms” and “intention to seek care. Among them, knowledge, attitude, social support, and coping efficacy are important predictors of healthcare-seeking intention and interact with each other, as well as directly or indirectly influence patients’ healthcare-seeking behavior. We confirmed that the tool has good validity, internal consistency and reliability. Therefore, it is recommended that healthcare workers should apply the questionnaire to the evaluation of patients with diabetic high-risk foot, so as to further promote the patient’s active search for medical care.
Acknowledgments
We would like to thank all the patients who participated in the study. The abstract of the preliminary findings will be presented at WCET® & ASCN UK Joint Congress conference on September 29, 2024. The official link to the conference is WCET-ASCN UK 2024 Joint Congress, more details can be found here.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was financially supported by the Natural Science Foundation of Hunan Province (2023JJ70063) and Center South University Graduate Student Independent Exploration and Innovation Program (512340016).
Disclosure
There is no conflict of interest in the study.
References
1. Armstrong DG, Boulton A, Bus SA. Diabetic Foot Ulcers and Their Recurrence. N Engl J Med. 2017;376(24):2367–2375. doi:10.1056/NEJMra1615439
2. Lazzarini PA, Hurn SE, Kuys SS, et al. The silent overall burden of foot disease in a representative hospitalised population. Int Wound J. 2017;14(4):716–728. doi:10.1111/iwj.12683
3. Lazzarini PA, Pacella RE, Armstrong DG, van Netten JJ. Diabetes-related lower-extremity complications are a leading cause of the global burden of disability. Diabet Med. 2018;35(9):1297–1299. doi:10.1111/dme.13680
4. Hingorani A, LaMuraglia GM, Henke P, et al. The management of diabetic foot: a clinical practice guideline by the Society for Vascular Surgery in collaboration with the American Podiatric Medical Association and the Society for Vascular Medicine. J Vasc Surg. 2016;63(2 Suppl):3S–21S. doi:10.1016/j.jvs.2015.10.003
5. Forde H, Wrigley S, O’Murchadha LT, et al. Five-year outcomes of patients attending a diabetic foot clinic in a tertiary referral centre. Ir J Med Sci. 2020;189(2):511–515. doi:10.1007/s11845-019-02108-2
6. Ahmad A, Abujbara M, Jaddou H, Younes NA, Ajlouni K. Anxiety and depression among adult patients with diabetic foot: prevalence and associated factors. J Clin Med Res. 2018;10(5):411–418. doi:10.14740/jocmr3352w
7. Craus S, Mula A, Coppini DV. The foot in diabetes - a reminder of an ever-present risk. Clin Med. 2023;23(3):228–233. doi:10.7861/clinmed2022-0489
8. Schaper NC, van Netten JJ, Apelqvist J, et al. Practical guidelines on the prevention and management of diabetes-related foot disease (IWGDF 2023 update). Diabetes Metab Res Rev. 2023;40(3):e3657. doi:10.1002/dmrr.3657
9. Yan J, Liu Y, Zhou B, Sun M. Pre-hospital delay in patients with diabetic foot problems: influencing factors and subsequent quality of care. Diabet Med. 2014;31(5):624–629. doi:10.1111/dme.12388
10. Crocker RM, Tan TW, Palmer K, Marrero DG. The patient’s perspective of diabetic foot ulceration: a phenomenological exploration of causes, detection and care seeking. J Adv Nurs. 2022;78(8):2482–2494. doi:10.1111/jan.15192
11. Ogunlana MO, Govender P, Oyewole OO, et al. Qualitative exploration into reasons for delay in seeking medical help with diabetic foot problems. Int J Qual Stud Health Well-Being. 2021;16(1):1945206. doi:10.1080/17482631.2021.1945206
12. Jin L, Xiaoyong Y, Geheng Y, et al. Construction of the standardized process of at-risk foot screening, stratification and intervention for diabetic patients. Chin J Diabetes Mellitus. 2017;09(05):281–285.
13. Addisu Y, Birhanu Z, Tilahun D, Assefa T. Predictors of treatment seeking intention among people with cough in East Wollega, Ethiopia based on the theory of planned behavior: a community based cross-sectional study. Ethiop J Health Sci. 2014;24(2):131–138. doi:10.4314/ejhs.v24i2.5
14. Chan WI, Batterham P, Christensen H, Galletly C. Suicide literacy, suicide stigma and help-seeking intentions in Australian medical students. Australas Psychiatry. 2014;22(2):132–139. doi:10.1177/1039856214522528
15. Hunter MS, Grunfeld EA, Ramirez AJ. Help-seeking intentions for breast-cancer symptoms: a comparison of the self-regulation model and the theory of planned behaviour. Br J Health Psychol. 2003;8(Pt 3):319–333. doi:10.1348/135910703322370888
16. Thurston IB, Phares V, Coates EE, Bogart LM. Child problem recognition and help-seeking intentions among black and white parents. J Clin Child Adolesc Psychol. 2015;44(4):604–615. doi:10.1080/15374416.2014.883929
17. Ajzen I. Constructing a TpB questionnaire: conceptual and methodological considerations. Office of Information Technologies. 2002.
18. Ajzen I. The Theory of Planned Behavior. Organ Behav Hum Decis Process. 1991;50(2):179–211. doi:10.1016/0749-5978(91)90020-T
19. Yi Y, Xiu S, Shi N, et al. Perceptions and acceptability of HPV vaccination among parents of female adolescents 9–14 in China: a cross-sectional survey based on the theory of planned behavior. Hum Vaccin Immunother. 2023;19(2):2225994. doi:10.1080/21645515.2023.2225994
20. Dadipoor S, Heydari G, Abu-Rmeileh NM, et al. A predictive model of waterpipe smoking cessation among women in southern Iran: application of the theory of planned behavior. BMC Public Health. 2023;23(1):1151. doi:10.1186/s12889-023-16053-4
21. Wang K, Zhang L. The impact of ecological civilization theory on university students’ pro-environmental behavior: an application of knowledge-attitude-practice theoretical model. Front Psychol. 2021;12:681409. doi:10.3389/fpsyg.2021.681409
22. Care DFBO. Chinese guidelines for the diagnosis and treatment of diabetic foot. Nat Med J China. 2017;4:251–258.
23. Huang S, Hu Y, Fu B, et al. Help-seeking intentions for depression and associated factors among Chinese perinatal women: a cross-sectional study. Int J Environ Res Public Health. 2023;20(3):2288.
24. Fekih-Romdhane F, Chebbi O, Sassi H, Cheour M. Knowledge, attitude and behaviours toward mental illness and help-seeking in a large nonclinical Tunisian student sample. Early Interv Psychiatry. 2021;15(5):1292–1305. doi:10.1111/eip.13080
25. Branquinho M, Canavarro MC, Fonseca A. Postpartum Depression in the Portuguese population: the role of knowledge, attitudes and help-seeking propensity in intention to recommend professional help-seeking. Community Ment Health J. 2020;56(8):1436–1448. doi:10.1007/s10597-020-00587-7
26. Alzghoul BI, Abdullah NA. Pain management practices by nurses: an application of the knowledge, attitude and practices (KAP) model. Glob J Health Sci. 2015;8(6):154–160. doi:10.5539/gjhs.v8n6p154
27. Yang Y, Ye Q, Yao M, Yang Y, Lin T. Development of the Home-Based Fall Prevention Knowledge (HFPK) questionnaire to assess home-based fall prevention knowledge levels among older adults in China. BMC Public Health. 2022;22(1):2071. doi:10.1186/s12889-022-14546-2
28. Ma H, Hu M, Wan J. Validation of the Chinese version of the kidney transplant understanding tool in Chinese patients. Nurs Open. 2023;10(5):2991–2998. doi:10.1002/nop2.1544
29. He T. Development of Weight Management Behavior Scale for Patient with Chronic heart Failure Based on the Theory of Planned Behavior. University of South China; 2020.
30. Hou S, Wang X, Zhao Z, et al. A scale for measuring electronic patient engagement behaviors: development and validation. Patient Prefer Adherence. 2024;18:917–929. doi:10.2147/PPA.S444633
31. Wu M. Questionnaire Statistical Analysis Practice SPSS Operation and Application. Chongqing: Chongqing University Press; 2010.
32. Wu X, Cai S, Zhou Y, Lan Y, Lin Y. Development, reliability and validity of the medication literacy scale for parents of children with epilepsy. Patient Prefer Adherence. 2024;18:165–176. doi:10.2147/PPA.S446081
33. Graystone R. Prevent compassion fatigue and burnout with a magnet culture. J Nurs Adm. 2019;49(5):231–233. doi:10.1097/NNA.0000000000000743
34. Apelqvist J, Ragnarson-Tennvall G, Persson U, Larsson J. Diabetic foot ulcers in a multidisciplinary setting. An economic analysis of primary healing and healing with amputation. J Intern Med. 1994;235(5):463–471. doi:10.1111/j.1365-2796.1994.tb01104.x
35. McDermott K, Fang M, Boulton A, Selvin E, Hicks CW. Etiology, epidemiology, and disparities in the burden of diabetic foot ulcers. Diabetes Care. 2023;46(1):209–221. doi:10.2337/dci22-0043
36. Minglong M. Statistical Analysis of Questionnaires: Operation and Application of SPSS. Chongqing: Chongqing University Publishing; 2010:158–193.
37. Shi J, Mo X, Sun Z. Content validity index in scale development. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2012;37(2):152–155. doi:10.3969/j.issn.1672-7347.2012.02.007
38. Hu Z, Sun Y, Ma Y, et al. Examining primary care physicians’ intention to perform cervical cancer screening services using a theory of planned behavior: a structural equation modeling approach. Front Public Health. 2022;10:893673. doi:10.3389/fpubh.2022.893673
39. Lee JY, Shin YJ. Using the theory of planned behavior to predict Korean college students’ help-seeking intention. J Behav Health Serv Res. 2022;49(1):76–90. doi:10.1007/s11414-020-09735-z
40. Pan L, Zhang X, Wang S, et al. Determinants associated with self-management behavior among type 2 diabetes patients in China: a structural equation model based on the theory of planned behavior. Int J Clin Health Psychol. 2023;23(1):100332. doi:10.1016/j.ijchp.2022.100332
41. Sheeran P, Maki A, Montanaro E, et al. The impact of changing attitudes, norms, and self-efficacy on health-related intentions and behavior: a meta-analysis. Health Psychol. 2016;35(11):1178–1188. doi:10.1037/hea0000387
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.