")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 18
Development of a Cutaneous Horn on a Lower Extremity with Granuloma Annulare: A Rare Co-Occurrence
Authors Bu X, Feng L , Guo J, Yu R, Bi X
Received 2 February 2025
Accepted for publication 17 July 2025
Published 19 July 2025 Volume 2025:18 Pages 1753—1756
DOI https://doi.org/10.2147/CCID.S520386
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Michela Starace
Xiaolin Bu,1,* Liwei Feng,2,* Jing Guo,3 Rongzhu Yu,2 Xinling Bi4
1Laboratory of Laser and Medical Innovation Application, Department of Dermatology, Gongli Hospital of Shanghai Pudong New Area, Shanghai, People’s Republic of China; 2School of Gongli Hospital Medical Technology, University of Shanghai for Science and Technology, Shanghai, People’s Republic of China; 3Postgraduate Training Base at Shanghai Gongli Hospital, Ningxia Medical University, Shanghai, People’s Republic of China; 4Department of Dermatology, Changhai Hospital, Naval Medical University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xinling Bi, Department of Dermatology, Changhai Hospital, Naval Medical University, 168 Changhai Road, YangPu District, Shanghai, People’s Republic of China, Email [email protected]
Abstract: A 65-year-old Asian male presented with a circular skin lesion on the flexor aspect of the right calf that first appeared at age 13 and gradually expanded peripherally. Six months prior to presentation, a dark brown, horn-like keratotic lesion with a hard texture emerged on the annular lesion, growing progressively without pain or pruritus. The cutaneous horn was surgically excised, and the annular lesion underwent biopsy. Pathological findings revealed abundant mucin in dermal collagen, dense histiocyte infiltration, and focal mild collagen degeneration, confirming a diagnosis of granuloma annulare complicated by a cutaneous horn.
Keywords: cutaneous horn, granuloma annulare, keratotic
Introduction
Granuloma annulare (GA) is an inflammatory, non-infectious granulomatous skin disease characterized by annular plagues or nodular lesions, primarily involving the dermis and subcutaneous tissue.1 A cutaneous horn is a cone-shaped hyperkeratotic lesion, most commonly observed in sun-exposed areas.2 However, its development on the lower extremities remains rare. Clinically, cutaneous horns are diagnosed based on underlying lesions, which may include viral warts, keratoacanthoma, seborrheic keratosis, actinic keratosis, squamous cell carcinoma, or basal cell carcinoma.3 To date, few cases of cutaneous horn complicating GA on the calf have been reported. Here, we describe a unique case of a cutaneous horn arising from GA on the calf.
Case Report
A 65-year-old male presented with a worsening skin lesion that had persisted for 52 years. The initial annular lesion on the flexor aspect of the right calf developed during adolescence, expanding slowly without medical intervention. Six months before evaluation, a hyperkeratotic lesion emerged on the annular lesion, increasing in size gradually. The patient reported no subjective symptoms. A former train driver with a 30-year career, he had no family history of similar dermatological conditions.
Physical examination revealed a large, golden-yellow, cone-shaped cutaneous horn (1.5 cm in length, 0.5 cm base width) localized on the annular lesion of the right calf flexor surface. The horn had smooth margins, and the surrounding skin exhibited a 3.0-cm-diameter annular plague with dark red-brown pigmentation (Figure 1). No similar lesions were noted elsewhere.
 |
Figure 1 Cutaneous horn arising from granuloma annulare on the right calf flexor surface. |
The horn was surgically excised, and a biopsy of the annular plague was performed. Histopathology of the plague showed abundant mucin in dermal collagen spaces, dense histiocyte infiltration, and focal mild collagen degeneration (Figure 2). The horn’s epidermis displayed hill-like protuberances with hyperkeratosis and parakeratosis, forming columnar lesions (Figure 3). No malignant features were observed. After a 3-year follow-up, there was no recurrence, and the annular plague significantly regressed.
 |
Figure 2 (a) Superficial dermis of GA lesion showing mucin deposition and histiocytes in collagen gaps; (b) Histiocyte-lymphocyte infiltration and focal mild collagen degeneration. H&E stain, original magnification (a) ×200, (b) ×100. |
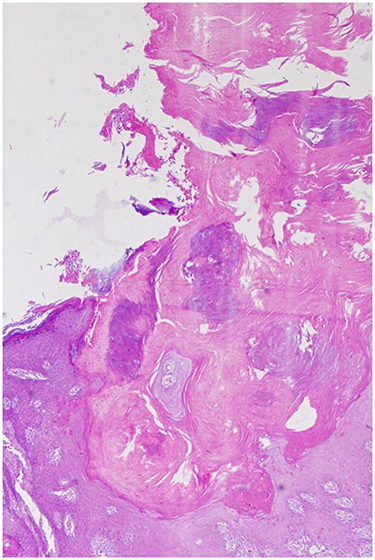 |
Figure 3 Cutaneous horn demonstrating lamellar parakeratosis columns. H&E stain, original magnification ×50. |
Discussion
Cutaneous horns are clinical diagnoses encompassing various benign and malignant underlying lesions. Literally defined as overgrowths of the skin’s superficial layer,4 they are more prevalent in Caucasians, rare in Asians, and extremely uncommon in Africans—likely due to pigmented skin photoprotection. Etiologic factors include chronic sun exposure and immunodeficiency.5
Typically occurring in individuals over 50 years without gender predilection, cutaneous horns usually involve sun-exposed areas.6 Notably, our patient’s horn developed in a non-exposed site (calf flexor), a location with few reported cases. While most horns grow slowly over years to decades, this case exhibited rapid progression (6 months), highlighting clinical variability in growth kinetics.7
GA is an idiopathic benign granulomatous disorder characterized by annular dermal plagues or plaques, commonly affecting the lateral/dorsal hands and feet. It often presents symmetrically in extremities and the trunk, typically asymptomatic but occasionally pruritic.8 Etiologies include immune dysregulation, heredity, viral infection, drugs, stress, insect bites, and trauma. Similar to cutaneous horns, GA may correlate with sun exposure. Pathologically, focal collagen degeneration and palisading granulomas are diagnostic, consistent with our case. Most GAs resolve within 2 years, though rare cases persist for decades—unusually, our patient’s lesion lasted over 50 years.
The co-occurrence of a cutaneous horn on long-standing GA is unique. Cutaneous horns rarely involve non-sun-exposed sites, and their association with GA is scarcely documented. The pathogenesis here remains unclear, but prolonged GA may have contributed to horn development. Histopathological studies of 222 cutaneous horn cases showed 58.56% were premalignant/malignant, with actinic keratosis (83.84%) and squamous cell carcinoma (93.75%) as leading underlying pathologies.9 Given the high prevalence of premalignant/malignant lesions beneath cutaneous horns, surgical excision with histopathological evaluation is imperative.9
Conclusion
This case emphasizes the need for heightened vigilance in long-standing GA, underscoring the importance of comprehensive diagnostic workup for cutaneous horns, regardless of anatomical location.
Ethics Approval and Consent to Participate
Written informed consent has been provided by the patient to have the case details and any accompanying images published. Approval was provided by Medical Research Ethics Committee of Gongli Hospital of Shanghai Pudong New Area. Publication of details of the case does not require the agency’s approval.
Consent for Publication
We have obtained informed consent from the patient and signed an informed consent form.
Funding
Key Discipline Construction Project of Pudong New Area Health Commission (PWZzb2022-01); Laser and Medical Innovation Capability Enhancement Program of Shanghai Pudong Gongli Hospital (JGYX2024A-06). The financial donors had no role in the design and conduct of the study, collection, management, analysis and interpretation of the data; preparation, review, or approval of the manuscript; and the decision to submit the manuscript for publication.
Disclosure
The authors have no conflicts of interest to declare for this work.
References
1. Bagci B, Karakas C, Kaur H, et al. Histopathologic aspects of malignancy-associated granuloma annulare: a single institution experience. Dermatopathology. 2023;10(1):95–103. doi:10.3390/dermatopathology10010015
2. Wan L, Park A, Arastu K, et al. Shedding new light on cutaneous horns: a comprehensive review and pitfall of management. Indian J Dermatol. 2025;70(1):50. doi:10.4103/ijd.ijd_331_24
3. Abhaypal K, Anjum N, Singh M, et al. Cutaneous horn: a masquerade to underlying keratotic basal cell carcinoma. Cureus. 2022;14(12):e32427. doi:10.7759/cureus.32427
4. Yang JH, Kim DH, Lee JS, et al. A case of cutaneous horn originating from keratoacanthoma. Ann Dermatol. 2011;23:89–91. doi:10.5021/ad.2011.23.1.89
5. Sidram V, Chndrakumar P, Varun M, et al. A rare case of cutaneous horn of scalp with squamous cell carcinoma in an elderly male. A case report. Int J Adv Case Rep. 2014;1:107–109.
6. Gupta R, Lavania P, Bansal VK, et al. Cutaneous horn developing over a verrucous carcinoma: a rare entity with an unusual presentation. Int Surg J. 2016;3:988–990. doi:10.18203/2349-2902.isj20161185
7. Masic T, Babajic E, Dizdarevic D, et al. A giant cutaneous horn. Med Arh. 2010;64(6):375–376.
8. Lapidus AH, Lee S, Khandewal T, et al. Subcutaneous granuloma annulare: a systematic review of a rare and underdiagnosed disease. Int J Dermatol. 2025;64(2):246–255. doi:10.1111/ijd.17419
9. Mantese SA, Diogo PM, Rocha A, et al. Cutaneous horn: a retrospective histopathological study of 222 cases. An Bras Dermatol. 2010;85:157–163. doi:10.1590/S0365-05962010000200005
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.