")
Back to Journals » Journal of Inflammation Research » Volume 17
Development of a Prognosis Prediction Model for Pediatric Sepsis Based on the NLPR
Authors Wang H , Zhang R, Xu J, Zhang M, Ren X, Wu Y
Received 24 May 2024
Accepted for publication 24 October 2024
Published 28 October 2024 Volume 2024:17 Pages 7777—7791
DOI https://doi.org/10.2147/JIR.S479660
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Adam Bachstetter
Huabin Wang,1– 4 Rui Zhang,1,3,4 Jing Xu,1,3,4 Min Zhang,1,3,4 Xueyun Ren,1,3,4 Yuhui Wu5
1Department of Pediatrics, Affiliated Hospital of Jining Medical University, Jining Medical University, Jining, People’s Republic of China; 2Postdoctoral Mobile Station, Shandong University of Traditional Chinese Medicine, Jinan, People’s Republic of China; 3Jining Key Laboratory for Prevention and Treatment of Severe Infection in Children, Affiliated Hospital of Jining Medical University, Jining, People’s Republic of China; 4Shandong Provincial Key Medical and Health Discipline of Pediatric Internal Medicine, Affiliated Hospital of Jining Medical University, Jining, People’s Republic of China; 5Department of Pediatric Intensive Care Unit, Shenzhen Children’s Hospital, Shenzhen, People’s Republic of China
Correspondence: Xueyun Ren; Yuhui Wu, Email [email protected]; [email protected]
Objective: Identifying high-risk children with poor prognoses during the early stages of sepsis and providing timely and appropriate interventions are imperative. The objective of this study was to develop a prognostic prediction model for pediatric sepsis utilizing the neutrophil to lymphocyte and platelet ratio (NLPR).
Methods: A multivariable logistic regression analysis was conducted to investigate the association between the NLPR and in-hospital mortality among septic children upon admission. To minimize the potential confounding factors that could introduce bias, a propensity score matching analysis was employed. Subsequently, a nomogram prediction model was developed to assess the risk of in-hospital mortality in septic children, incorporating the NLPR as a key factor. The performance of this prediction model was then evaluated.
Results: A total of 230 septic children were enrolled in the study. Multivariate logistic regression analysis revealed that the NLPR was an independent risk factor for in-hospital mortality, with an odds ratio of 8.31 (95% CI 3.69– 18.68). The finding remained consistent after propensity score matching analysis. A nomogram prediction model was developed that incorporates the NLPR, arterial blood lactate level, and Pediatric Critical Illness Score (PCIS). Among the various models, this nomogram exhibited the highest area under the curve (AUC) value of 0.831. The calibration curve demonstrated good agreement between the predicted and observed outcomes. Decision curve analysis indicated that the prediction model outperformed the PCIS. Internal validation of the model yielded an AUC value of 0.824 and a kappa value of 0.420, indicating its reliability and accuracy.
Conclusion: The NLPR serves as an independent risk factor for in-hospital mortality among septic children. The nomogram prognostic prediction model could effectively guide clinicians in accurately predicting the prognosis of septic children, thus enabling timely and effective treatment interventions.
Keywords: pediatric sepsis, NLPR, prognosis, clinical prediction model
Introduction
Sepsis is a primary cause of mortality among children globally, with significant incidence and mortality rates. Statistics indicate that approximately 1.2 million new cases of pediatric sepsis occur annually,1 and sepsis affects approximately 4–8% of hospitalized children.2 A global study encompassing pediatric intensive care units (PICUs) from 128 medical institutions reported a mortality rate of 21–32% among children with severe sepsis.3 Sepsis may cause hemodynamic instability, disrupt cardiovascular function, decrease the cellular oxygen supply, attenuate catecholamine responsiveness, and trigger insulin resistance, all of which cumulatively contribute to elevated mortality rates.
A prediction model is defined as a tool that anticipates the association between variables or risk factors and outcomes.4 Since its inception, prediction models have gained widespread clinical acceptance and have undergone rigorous development and validation, resulting in numerous publications in highly regarded peer-reviewed journals.5 Logistic or Cox regression is typically utilized to analyze the relationship between predictor variables and dichotomous outcomes. These models can take various forms, such as scoring systems, graphical score sheets, web calculators, mobile applications, and nomograms.
In primary-level hospitals, clinicians often lack a solid foundation in computer science and statistics, hindering their practical application of these models. To address this issue and enhance the usability of models for clinicians, modifications are sometimes made to convert these models into relatively simple scoring systems or to employ Classification and Regression Tree (CART) methods. While both approaches are effective and beneficial, they also have their drawbacks: converting predictive models into easily computable scoring systems by simplification may introduce biases, whereas CART typically requires very large datasets to generate reliable and generalizable models, often exhibiting lower accuracy compared to other methods.
A nomogram is a graphical tool that enables quick, approximate complex calculations without the need for a calculator or computer.6 It visually illustrates the impact of each independent variable on the outcome and assigns corresponding scores. By summing these scores, clinicians can infer the probability of the outcome. Nomograms offer several notable advantages compared to other clinical prediction models: (1) they are easily usable in settings remote from computers, particularly when the number of predictor variables is limited;7 (2) the relative significance of predictor variables is reflected by the length of lines in the nomogram; (3) they effectively handle interactions and nonlinear terms; and (4) they can represent complex models incorporating time-related predictor variables.8
The use of clinical prediction models for the prognosis of pediatric sepsis remains limited. Two risk prediction models, the pediatric sepsis biomarker risk model (PERSEVERE) and its revised version, PERSEVERE-II,9 have been developed using transcriptome analysis and CART, demonstrating a certain degree of accuracy in predicting the 28-day mortality risk among pediatric sepsis patients.10 However, widespread clinical implementation of these models is significantly hindered by their complex detection procedures and costly reagents.
During sepsis, the number of different types of immune cells varies depending on the stage of sepsis, the patient’s immune status, and the etiology of the infection.11 Therefore, clinical research based on the number or ratio of immune cells is promising.12–14 Although some biomarkers, such as miRNAs, have demonstrated promising predictive value in adult and pediatric sepsis, there is still a lack of simple and feasible detection indicators or predictive models that can be implemented in the vast majority of hospitals.15–18 The neutrophil to lymphocyte and platelet ratio (NLPR), as a novel prognostic indicator, has gradually gained attention in the medical community over the past two years. The NLPR incorporates the platelet count into the traditional neutrophil to lymphocyte ratio (NLR), and this organic combination is expected to further enhance its predictive value. This study aimed to assess whether the initial NLPR can effectively predict the risk of inpatient death in children with sepsis. Additionally, given the current lack of an effective nomogram for predicting the risk of mortality in pediatric patients with sepsis, this study aimed to establish and evaluate an NLPR-based nomogram to aid clinicians in decision-making.
Materials and Methods
Study Subjects
This study employed a retrospective cohort design to gather clinical data on children who were diagnosed with sepsis and admitted to the PICU of Shenzhen Children’s Hospital between January 2019 and September 2021. The Ethics Committee of Shenzhen Children’s Hospital granted approval for the study. As this study was conducted retrospectively, without influencing clinical decision-making and devoid of any personal or medical information capable of identifying individuals, the ethics committee dispensed with the requirement to obtain informed consent from parents or guardians. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013).
Inclusion and Exclusion Criteria
The criteria for patient inclusion were as follows: (1) met the diagnostic criteria for pediatric sepsis upon admission to the PICU;19 and (2) aged between 28 days and 18 years. (3) In the case of multiple admissions to the PICU, only the information from the first admission was included in the analysis.
The exclusion criteria for patients were as follows: (1) absence of blood routine information within the initial 24 hours of admission to the PICU; (2) diagnosis of hematological malignancies or those in the terminal stage of malignancy; (3) receiving organ transplants or who had used hormones, cytotoxic drugs, or immunosuppressants within the past two weeks; (4) a PICU stay of less than 24 hours; and (5) discontinued treatment, were voluntarily discharged, or transferred to another hospital.
Data Collection and Processing
The extracted demographic data included age and sex. Laboratory test data, obtained from the Laboratory Department of Shenzhen Children’s Hospital, included peripheral blood leukocyte count, neutrophil count, lymphocyte count, monocyte count, platelet count, high-sensitivity c-reactive protein (hs-CRP), procalcitonin, creatine kinase isoenzymes (CKMB), serum potassium, serum sodium, serum calcium, arterial blood pH, arterial blood lactate, activated partial thromboplastin time (APTT), and fibrinogen. These initial values were recorded within 24 hours of admission to the PICU.
Comorbidities, including anemia, hypertension, liver dysfunction, renal dysfunction, and hypoproteinaemia, were diagnosed within the first 24 hours of PICU admission. The definitions of these comorbidities are detailed in Supplementary Table 1. Additional variables considered were the site of infection and the Pediatric Critical Illness Score (PCIS).20 The PCIS, comprising 10 indicators (heart rate, systolic blood pressure, respiration, oxygen partial pressure, pH, serum sodium, serum potassium, serum creatinine or urea nitrogen, hemoglobin, and gastrointestinal manifestations), ranged from 0 to 100, with lower scores indicating greater illness severity. The worst values of each PCIS measurement were recorded within the first 24 hours of the patient’s PICU stay.
For this study, the neutrophil to lymphocyte and platelet ratio (NLPR) was calculated using the following formula: NLPR = neutrophil count × 100/(lymphocyte count × platelet count). Less than 10% of the missing values for all variables were replaced with the mean or median value.
Grouping and Definition of Outcomes
The NLPR was dichotomized into a binary variable utilizing the optimal cutoff value derived from the receiver operating characteristic (ROC) curve. The optimal cutoff value is the maximization of the Youden index (sensitivity + specificity − 1). The results of the ROC analysis, presented in Supplementary Figure 1, demonstrate the predictive value of the NLPR for in-hospital mortality in children with sepsis. NLPR exhibited significant predictive ability (P < 0.001), with the area under the curve (AUC) values of 0.748. The NLPR exhibited an optimal cut-off value of 2.34, with a predictive sensitivity of 68.63% and specificity of 71.51%. Based on this cutoff, children with sepsis were categorized into two groups: a high NLPR group (NLPR > 2.34) and a low NLPR group (NLPR ≤ 2.34).
The primary outcome was inpatient mortality, defined as deaths occurring during hospitalization. The secondary outcome included 30-day mortality, defined as death within 30 days of PICU admission, as well as the need for mechanical ventilation and the duration of the PICU stay.
Statistical Analysis
Continuous variables with a normal distribution are expressed as the mean ± standard deviation. Student’s t test was used to compare differences between two groups. For continuous variables with a skewed distribution, the median (interquartile range) was reported, and the Mann‒Whitney U-test was employed for group comparisons. Categorical variables are presented as the number of cases (percentages), and differences between groups were analyzed using the chi-square test.
A stepwise backward approach was employed to screen covariates for inclusion in the multivariate logistic regression analysis. Covariate adjustment was performed using an extended model approach, with Model 1 incorporating demographics (age and sex), Model 2 adding laboratory tests (hs-CRP, procalcitonin, CKMB, serum potassium, serum sodium, serum calcium, arterial blood pH, arterial blood lactate, APTT, and fibrinogen), Model 3 further incorporating complications (anemia, hypertension, liver dysfunction, renal dysfunction, and hypoproteinaemia), and Model 4 adding the PCIS. The laboratory test results were dichotomized into binary variables based on the respective normal reference ranges.
The relative importance of each covariate in the multivariate logistic regression model was assessed by subtracting the degrees of freedom of the covariate from the Wald chi-square value. A larger difference indicates greater importance of the covariate in the logistic regression model.
To minimize the influence of confounding factors potentially leading to biased results, propensity score matching (PSM) analysis was employed. These propensity scores were determined based on the probabilities of different NLPR groups among pediatric patients and were estimated using a multivariate logistic regression model. A 1:1 matched nearest neighbor matching algorithm was applied, with a caliper value set at 0.05.
For the development of a nomogram prediction model for inpatient mortality risk in pediatric sepsis patients, R statistical software (version 4.1.0) was utilized, leveraging the rms package. In this nomogram prediction model, each independent variable’s value was assigned a score based on its contribution to the outcome variable (ie, the magnitude of the regression coefficient). Subsequently, the scores for all the independent variables were summed to obtain a total score. A functional transformation was then applied to establish a relationship between the total score and the probability of the outcome event, enabling the calculation of the probability of the outcome event for an individual patient.
To assess the discriminatory ability of the nomogram prediction model, we employed metrics such as the AUC, integrated discrimination improvement (IDI), and the net reclassification index (NRI). Additionally, we evaluated the calibration of the prediction model using a calibration plot and conducted internal validation through bootstrap resampling with 1000 repetitions. To compare the nomogram prediction model with the PCIS, we utilized decision curve analysis (DCA), which quantified the net benefit at different threshold probabilities, thus enabling an assessment of the clinical effectiveness of the prediction model. Statistical significance was determined using a P value < 0.05. The statistical analysis was performed using STATA V.16, SPSS V.24, and R V.4.1.0.
Results
General Information of the Enrolled Patients
The participant screening process for this study is outlined in Figure 1. A detailed examination of clinical data was conducted to compare the high NLPR group with the low NLPR group among children with sepsis. As presented in Table 1, the high NLPR group exhibited significant differences in several clinical parameters compared to the low NLPR group. Specifically, children in the high-NLPR group were more likely to be older (48 vs 9, P < 0.001) and to have a greater neutrophil count (7.37 vs 5.51, P = 0.024), procalcitonin level (10.05 vs 6.55, P = 0.010), anemia proportion (77.9% vs 61.8%, P = 0.011), liver dysfunction proportion (34.9% vs 20.1%, P = 0.013), and renal dysfunction proportion (18.6% vs 7.6%, P = 0.012). Conversely, the lymphocyte count (1.06 vs 2.76, P < 0.001), platelet count (91 vs 306, P < 0.001), serum calcium level (2.02 vs 2.12, P < 0.001), and fibrinogen level (2.11 vs 2.97, P < 0.001) were significantly lower in the high NLPR group than in the low NLPR group.
 |
Table 1 Comparison of Clinical Data Between Different NLPR Groups |
 |
Figure 1 Flowchart of the patient screening process. Abbreviation: PICU, pediatric intensive care unit. |
Regarding clinical outcomes, no statistically significant difference was observed in the ICU length of stay between the high NLPR group and low NLPR group (4.3 vs 4.5 days, P = 0.177). However, a greater proportion of children in the high NLPR group than in the low NLPR group required mechanical ventilation (59.3% vs 42.4%, P = 0.013). Furthermore, the 30-day mortality rate was significantly greater in the high NLPR group than in the low NLPR group (37.2% vs 9.0%, P < 0.001). Similarly, the in-hospital mortality rate was 3.7 times greater in the high NLPR group (40.7% vs 11.1%, P < 0.001).
Associations Between the NLPR and in-Hospital Mortality
As demonstrated in Table 2, the stepwise expanded multivariable logistic regression model revealed a significant association between elevated NLPR and increased in-hospital mortality among children with sepsis. This association remained consistent across all models, with ORs ranging from 7.28 to 8.31. Comparable results were observed for the relationship between the NLPR and 30-day mortality, with ORs ranging from 6.19 to 8.39. Table 3 further illustrates that when the NLPR is treated as a continuous variable, each increase per standard deviation is associated with a 37.0% increase in in-hospital mortality and a 40.8% increase in 30-day mortality, both of which are statistically significant at P < 0.05.
 |
Table 2 Stepwise Expanded Multifactorial Logistic Regression Model (NLPR as a Dichotomous Variable) |
 |
Table 3 Stepwise Expanded Multifactorial Logistic Regression Model (NLPR as a Continuous Variable) |
According to the multivariable logistic regression analysis, the ORs for all covariates in Model 4 for in-hospital mortality are presented in Supplementary Table 2. After adjusting for covariates, arterial blood lactate (OR 3.44, 95% CI 1.49–7.91), PCIS (OR 0.93, 95% CI 0.89–0.97), and NLPR (OR 8.31, 95% CI 3.69–18.39) were identified as independent risk factors for in-hospital mortality among children with sepsis.
The Wald chi-square value and degree of freedom statistical results are presented in Figure 2, which only displays covariates with a difference greater than 0. These results indicate that the NLPR is the most significant covariate for predicting in-hospital mortality, followed by the PCIS and arterial blood lactate.
 |
Figure 2 Importance of covariates in the multivariable logistic regression model for the risk of in-hospital mortality in children with sepsis. Abbreviations: hs-CRP, high-sensitivity c-reactive protein; CKMB, creatine kinase isoenzymes; PCIS, pediatric critical illness score. |
PSM Results
Based on the baseline characteristics table, variables with statistically significant differences between the high and low NLPR groups were selected for propensity score generation. These variables included age, procalcitonin, serum calcium, fibrinogen, anemia, liver dysfunction, and renal dysfunction. Neutrophils, lymphocytes, and platelets were excluded from propensity score generation due to their involvement in the NLPR calculation. Matching was conducted using a 1:1 ratio, and the overall quality of the matched samples was assessed by comparing propensity scores between the groups (see Supplementary Figure 2).
As shown in Table 4, 55 patients were matched in each group, and all covariates were balanced between the two groups. The 30-day mortality rate (30.9% vs 9.1%, P = 0.004) and in-hospital mortality rate (34.5% vs 10.9%, P = 0.003) were significantly greater in the high NLPR group than in the low NLPR group.
 |
Table 4 Comparison of Variables After Propensity Score Matching |
Sensitivity Analysis
To assess the reliability of the findings following PSM, sensitivity analysis was conducted by including various covariates. In the context of multivariable logistic regression, arterial blood lactate and the PCIS were identified as potential confounders of the association between the NLPR and in-hospital mortality. Consequently, these two variables were incorporated into the PSM analysis. Post-PSM, the covariate distribution was balanced between the two groups, as shown in Supplementary Figure 3 and Table 3. We found that the results remained consistent and stable, indicating the robustness of our findings.
The immune microenvironment and the composition of immune cells are influenced by age. Therefore, in the context of this study, it is crucial to investigate whether the predictive value of immune cell composition for prognosis varies across different age subgroups. Based on the median age, we divided the subjects into a younger group (≤16 months) and an older group (>16 months). Initially, we conducted ROC analysis to compare the predictive value of NLPR in both the younger and older groups. The results (AUC were all greater than 0.7), presented in the Supplementary Table 4, indicate that both the single indicator NLPR and the composite indicator PCIS exhibit good predictive value in both age groups.
Then, we conducted stratified analyses and interaction tests based on age and site of infection. In the stratified analysis by age, the P-value for the interaction test was 0.684. For respiratory infections, the P-value for the interaction test was 0.294; for digestive system infections, it was 0.157; and for blood system infections, the P-value for the interaction test was 0.737. Thus, the predictive value of NLPR for mortality is not affected by different age groups or sites of infection.
Establishment and Evaluation of a Nomogram Prediction Model
In the context of multivariable logistic regression analysis, this study identified independent risk factors for in-hospital mortality in children with sepsis, including arterial blood lactate, the PCIS, and the NLPR. Utilizing these three variables, a nomogram prediction model was developed to assess the risk of in-hospital mortality in this patient population (Figure 3). The nomogram assigns a score to each variable based on its contribution to the outcome, taking into account the NLPR, hyperlactatemia (defined as lactate ≥ 2 mmol/L), and the PCIS. These scores are then summed to obtain a total score, which is subsequently used to calculate the probability of in-hospital mortality through a functional relationship between the total score and the probability of the outcome event. Given the skewed distribution of the NLPR data, it was treated as a dichotomous variable within the prediction model.
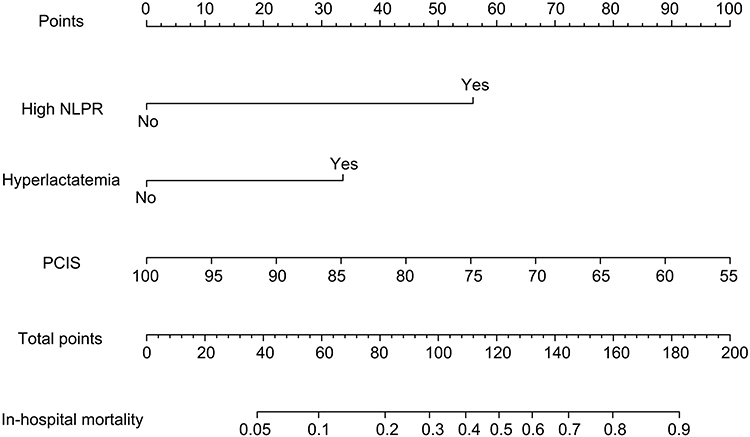 |
Figure 3 Nomogram prediction model for the risk of in-hospital mortality in children with sepsis. Abbreviation: PCIS, pediatric critical illness score. |
When evaluating the discriminatory performance of the models, five distinct models were constructed: Predictive Model 1 included only the PCIS, Predictive Model 2 included the PCIS combined with lactate, Predictive Model 3 included the NLPR combined with lactate, Predictive Model 4 included both the NLPR and PCIS, and Predictive Model 5, our nomogram prediction model, integrated all three variables: the NLPR, PCIS, and lactate. As demonstrated in Figure 4A, Predictive Model 5 exhibited the highest AUC value of 0.831 (95% CI 0.776–0.877), followed by Predictive Model 3 (AUC 0.779, 95% CI 0.720–0.831), Predictive Model 2 (AUC 0.762, 95% CI 0.701–0.815), Predictive Model 4 (AUC 0.761, 95% CI 0.700–0.814), and Predictive Model 1 (AUC 0.738, 95% CI 0.676–0.793).
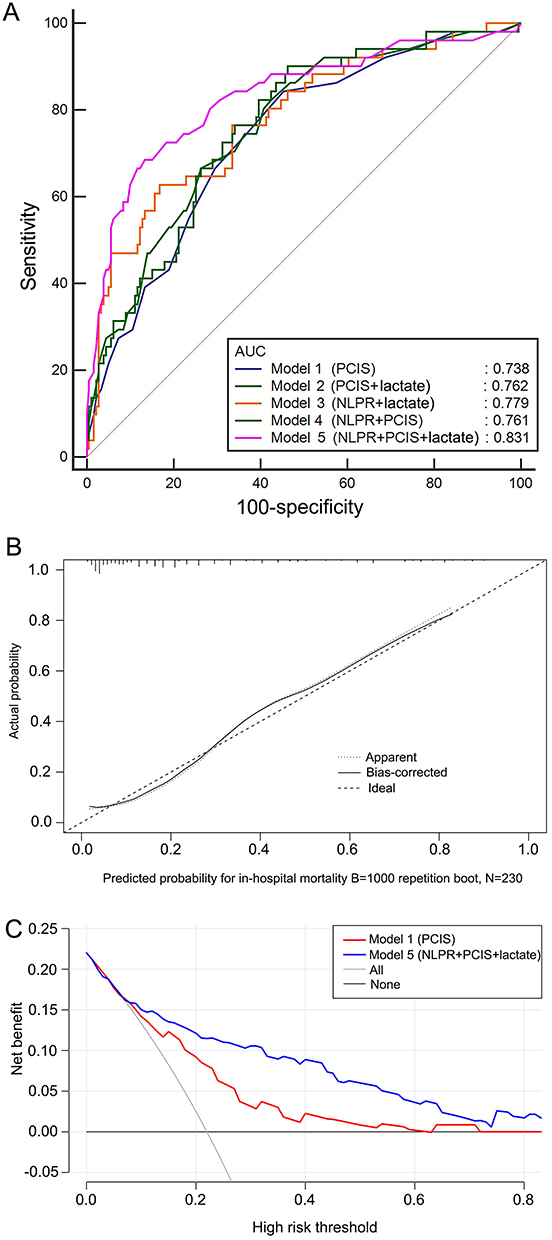 |
Figure 4 Evaluation of mortality prediction models for children with sepsis. (A) Receiver operating characteristic curve; (B) calibration plot; (C) decision curve analysis. Abbreviation: PCIS, pediatric critical illness score. |
The differences in AUC values were statistically significant for Predictive Model 5 versus Predictive Model 1 (0.093, 95% CI 0.024–0.162, P = 0.008), Predictive Model 5 versus Predictive Model 2 (0.069, 95% CI 0.012–0.127, P = 0.019), Predictive Model 5 versus Predictive Model 3 (0.052, 95% CI 0.001–0.103, P = 0.045), and Predictive Model 5 versus Predictive Model 4 (0.070, 95% CI 0.008–0.133, P = 0.027). These findings indicate that our nomogram prediction model demonstrates superior discriminatory performance.
As demonstrated in Table 5, the categorical NRI and IDI values of the nomogram prediction model (Predictive Model 5) exceeded zero compared to those of Predictive Models 2, 3, and 4. This indicates that the established nomogram prediction model demonstrates superior predictive performance and a greater proportion of accurate classifications.
 |
Table 5 Comparison of NRIs Among Different Mortality Prediction Models for Hospitalized Children with Sepsis |
As depicted in Figure 4B, the calibration curve exhibited excellent concordance between the predicted and observed probabilities of in-hospital mortality for pediatric sepsis patients. The calculated Brier score of 0.118, which is below the threshold of 0.3, further confirms the strong alignment between the nomogram prediction model and actual observations. To further assess the clinical utility of the nomogram prediction model (Predictive Model 5), a decision curve was constructed and compared with the PCIS (Predictive Model 1). As shown in Figure 4C, the nomogram prediction model curve consistently surpassed the PCIS curve across a range of threshold probabilities, indicating a superior clinical net benefit.
To ensure the robustness of the nomogram prediction model, internal validation was conducted using bootstrap resampling with 1000 iterations. The validation results revealed an AUC value of 0.824 and a kappa value of 0.420 for predicting in-hospital mortality among pediatric sepsis patients. These findings confirm the model’s good discriminatory power and consistency during internal validation.
Discussion
Immune cells play a pivotal role in the etiology and progression of sepsis.21,22 In the present study, we investigated organically integrated immune cells (specifically, neutrophils, lymphocytes, and platelets) that are relevant to sepsis, revealing the intricate relationships between immune cells and coagulation systems within the inflammatory cascade of sepsis. Our findings revealed that the initial NLPR upon admission to the PICU serves as an independent predictor of in-hospital mortality among children with sepsis and is the most significant covariate for hospital mortality prediction. Notably, even after adjusting for all covariates between the two groups using PSM analysis, the 30-day and in-hospital mortality rates remained significantly greater in the high NLPR group than in the low NLPR group. Finally, we constructed a nomogram prediction model that incorporated the NLPR, arterial blood lactate level, and PCIS. This model demonstrated excellent accuracy, consistency, and clinical utility, thus providing valuable guidance for clinical decision-making.
Sepsis is characterized by a dysregulated immune response to infection.2 Both innate and adaptive immune responses are involved in the development and progression of sepsis, with the interplay between immune cells and pathogenic microorganisms dominating the disease course. Neutrophils, lymphocytes, and platelets are crucial cellular components in the host’s defense against infection.23 Neutrophils are the first immune cells recruited to inflammatory sites. Activated neutrophils can trigger oxidative stress, release proteases, and form neutrophil extracellular traps, thereby inducing positive feedback that amplifies the inflammatory response in the body. Lymphocytes are key cell types in the adaptive immune system, endowing the immune system with broader and more precise recognition capabilities. Platelets play a central role in hemostasis, but current research has clearly demonstrated that these ubiquitous blood components in the vasculature are potent immunomodulators and effectors, exerting significant functions in hemostasis, coagulation, angiogenesis, innate immunity, and inflammatory responses. Sepsis affects the number and function of immune cells, including neutrophils, lymphocytes, and platelets.23 Compared to adult patients, children have immature development, poorer regulatory and compensatory capacities, and greater interindividual variability, making them more prone to imbalances in immune cells.2
In the present study, both as a continuous and categorical variable, the NLPR independently correlated with in-hospital mortality among septic children, even after adjusting for confounding factors. Limited research has been conducted on the NLPR in adult patients with infectious diseases. Gameiro et al24 performed a retrospective analysis of 399 sepsis patients with acute kidney injury to investigate the relationship between the NLPR and prognosis. Their results demonstrated that when treated as a continuous variable, the NLPR had an adjusted OR of 1.01 (95% CI 1.00–1.02, P = 0.015). When categorized, a high NLPR independently increased the risk of in-hospital mortality (unadjusted OR 1.79, 95% CI 1.13–2.83, P = 0.013; adjusted OR 2.14, 95% CI 1.23–3.71, P = 0.007). These findings align with our study’s observations. In another observational study, researchers assessed the impact of NLR and NLPR on 28-day mortality among patients with sepsis.25 The results indicated that the AUC for predicting 28-day mortality was 0.762 for NLR and 0.827 for NLPR. After stratifying patients based on optimal cutoff values for NLR and NLPR, both the high NLR and high NLPR groups exhibited higher mortality rates and shorter survival times compared to the low NLR and low NLPR groups. These findings are consistent with the results presented in our study.
This study confirms the association between the NLPR and poor prognosis among children with sepsis, despite the underlying pathophysiological mechanism remaining enigmatic. Potential explanations for this association can be postulated. In sepsis, the elevation of neutrophil counts not only activates a positive inflammatory feedback loop but also indicates the potential presence of unresolved lesions that inhibit lymphocytes. Concurrently, lymphocyte apoptosis induced by sepsis leads to lymphocytopenia and immunosuppression.26 Prior clinical studies have demonstrated that persistently low lymphocyte counts in sepsis patients are associated with an increased risk of nosocomial infection and mortality.27,28 The interplay between platelets and leukocytes plays a pivotal role in the pathogenesis of infectious diseases. Platelets respond to infection and inflammation by expressing a myriad of soluble mediators and cell surface molecules, thereby mediating various immune responses. Conversely, platelet aggregation and interaction with neutrophils can induce thrombo-inflammatory reactions, leading to platelet consumption.29 In sepsis patients, thrombocytopenia serves as a significant marker of critical illness and is recognized as a risk factor for mortality.30 Notably, thrombocytopenia was observed in approximately half of the deceased children with sepsis in this study. Therefore, the platelet count was incorporated into the NLR calculation, giving rise to a novel combined index known as the NLPR.
Our study reveals that NLPR, as an easily accessible biomarker, plays a pivotal role in early risk stratification and timely intervention for pediatric sepsis patients. The advantages of NLPR as a predictive indicator are multifold: it is a cost-effective and readily obtainable laboratory hematological parameter, even in low-income countries or regions with limited medical resources; data acquisition is swift; and interpreting the data requires minimal expertise.
The application of clinical prediction models in pediatric sepsis prognosis remains scarce, and there is a dire need for nomogram prediction models that provide clinicians in primary hospitals with powerful auxiliary tools. Notably, the well-recognized risk prediction models for pediatric sepsis are PERSEVERE and PERSEVERE-II. PERSEVERE, introduced by Wong et al in 2012,31 was constructed using the CART method. This prediction model utilized serum samples from children with septic shock to detect specific biomarkers. The classification tree encompassed six decision rules based on biomarkers (CCL3, HSPA1B, IL-8, GZMB, and MMP8), one rule based on age, and 14 subnodes. PERSEVERE exhibited an AUC of 0.883, a sensitivity of 93%, and a specificity of 74% in predicting mortality. PERSEVERE-II, an enhanced version of PERSEVERE introduced in 2016,9 categorizes patients into three subtypes based on the presence or absence of multiple organ failure (MOF) and new thrombocytopenia. These subtypes included new thrombocytopenia with MOF, no new thrombocytopenia with MOF, and no MOF. PERSEVERE performed impressively in the new thrombocytopenia with MOF cohort (AUC 0.84, 95% CI 0.77–0.90) but less so in the no new thrombocytopenia with MOF cohort (AUC 0.71, 95% CI 0.61–0.80). The authors revised PERSEVERE, replacing age with platelet count upon admission while maintaining the other five biomarkers. PERSEVERE-II demonstrated an AUC of 0.89 (95% CI 0.85–0.93) across all patients and performed similarly well in both cohorts.
The primary strengths of PERSEVERE and PERSEVERE-II are their exceptional predictive accuracy. These prediction models rely on data obtained within the initial 24 hours of septic shock onset in the PICU, a crucial period for risk stratification. Nonetheless, significant challenges hinder their widespread application in primary hospitals. These challenges stem from the intricate experimental procedures and costly detection reagent costs associated with measuring the five biomarkers. Furthermore, the requirement for additional blood samples places a considerable burden on infants and patients with anemia. Last, the relatively limited detection time can delay data availability, potentially compromising critical clinical decisions.
This study aimed to assess the ability of a nomogram prediction model that integrates the NLPR, arterial blood lactate level, and PCIS to predict the outcomes of pediatric sepsis patients admitted to the PICU. In this study, the predictive model constructed using NLPR, arterial blood lactate, and PCIS demonstrated a significantly higher AUC value compared to the PCIS alone (0.831 vs 0.738, P = 0.008), as well as when compared to any combination of two out of the three variables (all P-values < 0.05). To further assess the discriminatory power of the nomogram prediction model, we employed NRI and IDI. When comparing the nomogram prediction model (Model 5) to Models 1 through 4, the results for both categorical NRI, continuous NRI, and IDI were greater than 0, indicating the nomogram’s ability to accurately predict the risk of mortality in sepsis patients. Furthermore, the calibration curve showed a good alignment between the predicted and observed curves, and the model maintained good discrimination and consistency after internal validation. In the DCA analysis, our findings indicated that, across nearly all threshold probability ranges, the curves represented by the nomogram prediction model and the PCIS model had higher net benefits than the extreme curve. Moreover, when comparing the nomogram prediction model curve to the PCIS curve, the nomogram curve was significantly higher than the PCIS curve over a wide range of threshold probabilities, highlighting the greater net benefit and higher practical utility of the nomogram prediction model in clinical practice.
Blood routine tests and lactate measurements are routinely conducted upon admission to the PICU, while the PCIS, which incorporates ten physiological indicators, is widely utilized and completed within the first day of hospitalization. Notably, tissue perfusion and blood routine parameters were excluded from the PCIS calculation. Arterial blood lactate levels exceeding 2 mmol/L (>18 mg/dL) are a crucial component of the Sepsis-3 criteria for adult septic shock.32 Multiple studies have demonstrated that elevated lactate levels among infected children, particularly those exceeding 4 mmol/L (>36 mg/dL), are associated with a heightened risk of organ dysfunction and mortality.33 Lactate accumulation in sepsis results from diverse mechanisms, such as tissue hypoperfusion-induced anaerobic metabolism, decreased lactate clearance, and the body’s bioenergetic response to sepsis.34 Incorporating NLPR and lactate measurements into the PCIS may enhance its predictive accuracy for pediatric sepsis outcomes.
The nomogram prediction model developed in this study offers several noteworthy advantages in addition to its commendable accuracy, consistency, and clinical utility. First, the model utilizes routinely tested indicators in clinical practice, thus eliminating the need for additional blood sampling among patients. Second, it avoids any incremental testing costs, which is particularly beneficial in economically disadvantaged regions, particularly for impoverished patients who have already borne significant medical expenses in the PICU. Finally, clinicians can promptly acquire data for each indicator within the prediction model upon patient admission to the PICU, facilitating swift risk stratification and timely intervention.
This study explored the association between the NLPR and short-term prognosis in pediatric sepsis patients by introducing a novel nomogram prediction model rooted in the NLPR. Its strengths lie in several aspects. First, because of the potential influence of diverse factors, such as age, anemia, liver, and kidney dysfunction, on the NLPR, this study ensured the inclusion of a comprehensive set of confounding variables to increase the accuracy of the results. Second, the use of multiple statistical techniques to evaluate the predictive capacity of the studied variables further bolsters the credibility and scientific validity of the findings.
However, our study utilized a single-center, retrospective dataset for model development, which entails several limitations. Firstly, single-center studies inherently suffer from limitations in sample representativeness and external validity, introducing potential selection bias that restricts the generalizability of our results. External validation in independent cohorts is imperative. Secondly, the predictive power of the model may be constrained by the sample size and event rate within the retrospective dataset. Smaller sample sizes and lower event rates can lead to wider confidence intervals and reduced precision in estimates. Thirdly, although we employed various sensitivity analysis methods to validate our findings, such as using a stepwise backward approach for covariate selection, applying propensity score matching to minimize confounding factors, and performing internal validation through bootstrap resampling with 1000 iterations, the single-center sample size still poses a risk of potential overfitting in the constructed model. Additionally, sensitivity analyses often rely on the experience and subjective judgments of analysts, such as selecting which variables to analyze and setting the ranges for variations. This subjectivity can lead to inconsistencies in results and difficulties in interpretation, and may fail to account for all potential unmeasured confounding factors. Fourthly, due to the constraints of retrospective research, certain potentially important predictors or outcomes not recorded in the existing data could not be evaluated. Future prospective, multicenter studies could incorporate a broader range of variables to enhance the robustness and applicability of the model.
Conclusion
This study delves into multiple factors associated with the prognosis of pediatric sepsis and constructs a clinical prediction model based on NLPR, arterial blood lactate levels, and the PCIS. While NLPR has demonstrated a significant association with adverse outcomes in septic children, the core value of this research lies in showcasing how these biomarkers and clinical scoring systems can be effectively integrated to develop a predictive model with high discriminatory power, consistency, and clinical utility. This model not only enhances the accuracy of clinicians’ prognostic assessments for septic children but also facilitates prompt risk stratification upon PICU admission, guiding early and effective intervention strategies. With the rapid advancement of artificial intelligence technology, there is reason to believe that combining artificial intelligence algorithms with multi-source clinical data can further improve the precision and generalization capability of prediction models. Leveraging big data analytics and machine learning techniques, additional potential prognostic factors can be uncovered, continually optimizing and iterating the model to make it more intelligent and personalized, ultimately providing stronger support for precision medicine in pediatric sepsis.
Acknowledgments
This research was supported by Post-doctoral Innovative Talent Support Program of Shandong Province (grant number SDBX2022020), Shandong Provincial Natural Science Foundation (grant number ZR2023QH382), and Postdoctoral Program of Affiliated Hospital of Jining Medical University (grant number JYFY321211).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fleischmann-Struzek C, Goldfarb DM, Schlattmann P. et al. The global burden of paediatric and neonatal sepsis: a systematic review. Lancet Resp Med. 2018;6(3):223–230. doi:10.1016/S2213-2600(18)30063-8
2. Balamuth F, Weiss SL, Neuman MI, et al. Pediatric severe sepsis in U.S. Children’s Hospitals. Pediatr Crit Care Med. 2014;15(9):798–805. doi:10.1097/PCC.0000000000000225
3. Weiss SL, Fitzgerald JC, Pappachan J, et al. Global epidemiology of pediatric severe sepsis: the sepsis prevalence, outcomes, and therapies study. Am J Respir Crit Care Med. 2015;191(10):1147–1157. doi:10.1164/rccm.201412-2323OC
4. Staffa SJ, Zurakowski D. Statistical development and validation of clinical prediction models. Anesthesiology. 2021;135(3):396–405. doi:10.1097/ALN.0000000000003871
5. Altman DG, Vergouwe Y, Royston P, Moons KGM. Prognosis and prognostic research: validating a prognostic model. BMJ. 2009;338:605. doi:10.1136/bmj.b605
6. Park SY. Nomogram: an analogue tool to deliver digital knowledge. J Thorac Cardiovasc Surg. 2018;155(4):1793. doi:10.1016/j.jtcvs.2017.12.107
7. Bonnett LJ, Snell KIE, Collins GS, Riley RD. Guide to presenting clinical prediction models for use in clinical settings. BMJ. 2019;365:l737. doi:10.1136/bmj.l737
8. Kattan MW, Heller G, Brennan MF. A competing-risks nomogram for sarcoma-specific death following local recurrence. Stat Med. 2003;22(22):3515–3525. doi:10.1002/sim.1574
9. Wong HR, Cvijanovich NZ, Anas N, et al. Pediatric sepsis biomarker risk model-II: redefining the pediatric sepsis biomarker risk model with septic shock phenotype. Crit Care Med. 2016;44(11):2010–2017. doi:10.1097/CCM.0000000000001852
10. Moldawer LL, Wong HR, Weiss SL, et al. Testing the prognostic accuracy of the updated pediatric sepsis biomarker risk model. PLoS One. 2014;9(1):e86242. doi:10.1371/journal.pone.0086242
11. Wang H, Huang J, Yi W, et al. Identification of immune-related key genes as potential diagnostic biomarkers of sepsis in children. J Inflamm Res. 2022;15:2441–2459. doi:10.2147/JIR.S359908
12. Bilen MA, Martini DJ, Liu Y, et al. The prognostic and predictive impact of inflammatory biomarkers in patients who have advanced-stage cancer treated with immunotherapy. Cancer. 2018;125(1):127–134. doi:10.1002/cncr.31778
13. Takenaka Y, Oya R, Takemoto N, Inohara H. Neutrophil-to-lymphocyte ratio as a prognostic marker for head and neck squamous cell carcinoma treated with immune checkpoint inhibitors: meta-analysis. Head Neck. 2022;44(5):1237–1245. doi:10.1002/hed.26997
14. Chennamadhavuni A, Abushahin L, Jin N, Presley CJ, Manne A. Risk factors and biomarkers for immune-related adverse events: a practical guide to identifying high-risk patients and rechallenging immune checkpoint inhibitors. Front Immunol. 2022;13:779691. doi:10.3389/fimmu.2022.779691
15. Velissaris D, Zareifopoulos N, Karamouzos V, et al. Presepsin as a diagnostic and prognostic biomarker in sepsis. Cureus. 2021;13(5):e15019. doi:10.7759/cureus.15019
16. Sun Z, Song Y, Li J, et al. Potential biomarker for diagnosis and therapy of sepsis: lactylation. Immun Inflamm Dis. 2023;11(10):e1042. doi:10.1002/iid3.1042
17. Gopal N, Chauhan N, Jain U, et al. Advancement in biomarker based effective diagnosis of neonatal sepsis. Artif Cell Nanomed B. 2023;51(1):476–490. doi:10.1080/21691401.2023.2252016
18. El-Khazragy N, Mohamed NM, Mostafa MF, et al. miRNAs: novel noninvasive biomarkers as diagnostic and prognostic tools in neonatal sepsis. Diagn Microbiol Infect Dis. 2023;107(3):116053. doi:10.1016/j.diagmicrobio.2023.116053
19. Goldstein B, Giroir B, Randolph A. International pediatric sepsis consensus conference: definitions for sepsis and organ dysfunction in pediatrics. Pediatr Crit Care Med. 2005;6(1):2–8. doi:10.1097/01.PCC.0000149131.72248.E6
20. Shen H, Qu D, Na W, et al. Comparison of the OI and PaO2/FiO2 score in evaluating PARDS requiring mechanical ventilation. Pediatr Pulmonol. 2020;56(5):1182–1188. doi:10.1002/ppul.25194
21. Ren C, Yao R-Q, Zhang H, Feng Y-W, Yao Y-M. Sepsis-associated encephalopathy: a vicious cycle of immunosuppression. J Neuroinflammation. 2020;17(1):14. doi:10.1186/s12974-020-1701-3
22. Cox D. Sepsis–it is all about the platelets. Front Immunol. 2023;14:1210219. doi:10.3389/fimmu.2023.1210219
23. Wang H, Guo C, Wang Y, Li C, Wu Y, Ren X. Immune cell composition and its impact on prognosis in children with sepsis. BMC Pediatr. 2024;24(1):611. doi:10.1186/s12887-024-05087-1
24. Gameiro J, Fonseca JA, Jorge S, Gouveia J, Lopes JA. Neutrophil, lymphocyte and platelet ratio as a predictor of mortality in septic-acute kidney injury patients. Nefrología. 2020;40(4):461–468. doi:10.1016/j.nefro.2019.11.006
25. Liu D, Yu Z, Zhang D, Zhang J, Zhang Y, Wang X. Value of neutrophil to lymphocytes and platelets ratio for predicting 28-day mortality in sepsis patients. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2021;33(1):33–37. doi:10.3760/cma.j.cn121430-20200727-00545
26. Heffernan DS, Monaghan SF, Thakkar RK, et al. Failure to normalize lymphopenia following trauma is associated with increased mortality, independent of the leukocytosis pattern. Critical Care. 2012;16(1):R12. doi:10.1186/cc11157
27. Drewry AM, Samra N, Skrupky LP, et al. Persistent lymphopenia after diagnosis of sepsis predicts mortality. Shock. 2014;42(5):383–391. doi:10.1097/SHK.0000000000000234
28. Felmet KA, Hall MW, Clark RSB, Jaffe R, Carcillo JA. Prolonged lymphopenia, lymphoid depletion, and hypoprolactinemia in children with nosocomial sepsis and multiple organ failure. J Immunol. 2005;174(6):3765–3772. doi:10.4049/jimmunol.174.6.3765
29. Blair P, Rex S, Vitseva O, et al. Stimulation of Toll-like receptor 2 in human platelets induces a thromboinflammatory response through activation of phosphoinositide 3-kinase. Circul Res. 2009;104(3):346–354. doi:10.1161/CIRCRESAHA.108.185785
30. Menard CE, Kumar A, Houston DS, et al. Evolution and impact of thrombocytopenia in septic shock: a retrospective cohort study. Crit Care Med. 2019;47(4):558–565. doi:10.1097/CCM.0000000000003644
31. Wong HR, Salisbury S, Xiao Q, et al. The pediatric sepsis biomarker risk model. Critical Care. 2012;16(5):R174. doi:10.1186/cc11652
32. Shankar-Hari M, Phillips GS, Levy ML, et al. Developing a new definition and assessing new clinical criteria for septic shock. JAMA. 2016;315(8):775–787. doi:10.1001/jama.2016.0289
33. Scott HF, Brou L, Deakyne SJ, et al. Association between early lactate levels and 30-day mortality in clinically suspected sepsis in children. JAMA Pediatr. 2017;171(3):249–255. doi:10.1001/jamapediatrics.2016.3681
34. Puskarich MA, Shapiro NI, Massey MJ, et al. Lactate clearance in septic shock is not a surrogate for improved microcirculatory flow. Acad Emerg Med. 2016;23(6):690–693. doi:10.1111/acem.12928
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.