")
Back to Journals » Nature and Science of Sleep » Volume 17
Diagnostic Accuracy of the Alice NightOne Single-Belt Monitor for Obstructive Sleep Apnea and Reliability of Wireless Data Transfer
Authors Peng M , Zhang Y, Zhao R, Li J, Zhang X, Deng L, Zhao L, Zhou B, Wang X, Dong X, Han F
Received 18 March 2025
Accepted for publication 23 May 2025
Published 26 June 2025 Volume 2025:17 Pages 1493—1505
DOI https://doi.org/10.2147/NSS.S527805
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Ahmed BaHammam
MaoHuan Peng,1,* YuanYuan Zhang,2,* Rui Zhao,3 Jing Li,1 XueLi Zhang,1 LiHua Deng,4 Long Zhao,1 Bing Zhou,1 XinRu Wang,1 XiaoSong Dong,1 Fang Han1
1Department of Sleep Medicine, Peking University People’s Hospital, Beijing, People’s Republic of China; 2Department of General Practice, Peking University People’s Hospital, Beijing, People’s Republic of China; 3Department of Pulmonary and Critical Care Medicine, Peking University People’s Hospital, Beijing, People’s Republic of China; 4Department of Geriatrics, Peking University People’s Hospital, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: XiaoSong Dong, Department of Sleep Medicine, Peking University People’s Hospital, Beijing, 100044, People’s Republic of China, 100044, Email [email protected]
Objective: To validate the performance of a single-belt type 3 portable monitor Alice NightOne for diagnosis of obstructive sleep apnea and its reliability in remote data transmission.
Methods: Our study included two parts: in-laboratory Alice NightOne (ANO) monitoring (ANOlab) and home sleep apnea testing (HSAT) using ANO (ANOhome). For ANOlab, the participants underwent polysomnography (PSG) with ANOlab simultaneously. For ANOhome, the participants completed unattended overnight ANOhome out of sleep center and PSG was performed in another night. The ANO recordings were transmitted to cloud database wirelessly in addition to traditional wire transmission. Message digest-5 (MD5) algorithm was utilized to verify the integrity of the cloud data.
Results: Ninety-one ANOlab and 170 ANOhome recordings were analyzed. Both the respiratory event index (REI) on ANOlab and that on ANOhome were lower than the corresponding apnea-hypopnea index (AHI) on PSG (24.9 ± 20.5 events/h vs 31.6 ± 25.0 events/h, and 26.7 ± 17.0 events/h vs 35.3 ± 21.2 events/h respectively, P < 0.001). Bland-Altman analysis of REI on ANOlab versus AHI on PSG showed a mean difference (95% confidence interval) of − 6.7 (− 8.4, − 4.9) events/h. For REI on ANOhome versus AHI on PSG, the difference is − 8.0 (− 9.9, − 6.0) events/h. With threshold of REI ≥ 5 events/h for OSA diagnosis, ANOhome had 98.8% sensitivity, 90.0% specificity, 99.4% positive predictive value. The MD5 algorithm verified the identity between uploaded cloud data and original data.
Conclusion: With single thoracoabdominal belt, Alice NightOne can help diagnosis of obstructive sleep apnea with good sensitivity and specificity, though it may underestimate AHI. Furthermore, it provides reliable support based on solid data teletransmission and scoring synchronization, which may increase the ability of diagnosis and management of OSA through telemedicine.
Keywords: home sleep apnea testing, portable monitor, obstructive sleep apnea, telemedicine
Introduction
Since its development, polysomnography (PSG) has been the gold standard for diagnosis of obstructive sleep apnea (OSA). However, type 3 home sleep apnea testing (HSAT) was recommended for the diagnosis of moderate-to-severe OSA,1–4 because of its convenience for remote patients, lower cost, and its critical role in telemedicine, particularly during the COVID-19 pandemic and other unique circumstances.5–7 Current technology evaluation guidelines recommend the use of either two piezoelectric belts or respiratory inductance plethysmography (RIP) belts to assess respiratory effort due to insufficient evidence supporting the reliability of single-belt devices. Alice NightOne (ANO; Philips Respironics, Pittsburgh, Pennsylvania, USA) was identified as a type 3 portable monitor (PM), or S0C4O1xP2E2R2 device in SCOPER classification system, with only one thoracoabdominal RIP belt worn at the level of chest.8,9 One objective of the present study was to validate the ANO monitor in a larger cohort and to evaluate its performance out of sleep center. By validating the performance of this single-belt PM, it may provide more evidence for respiratory effort assessment in HSAT guideline modifications.
Telemedicine has been accepted rapidly with advances in information technology, particularly during the COVID-19 pandemic.10 Despite this progress, there were very few studies published about the technology of HSAT data teletransmission. ANO offers a platform enabling patients to upload HSAT recording data, technicians to access and score the data, and physicians to view detailed signal graphs and sleep reports, with its integrated sleep monitoring and scoring software. Accordingly, another objective of this study was to assess the reliability of ANO’s remote data transmission capabilities.
Method
Participants
Patients aged 18 to 80 years who were referred to the Department of Sleep Medicine at Peking University People’s Hospital with suspected OSA, such as those with symptoms of snoring, were enrolled in the study. Individuals with any of the following conditions were excluded: prior diagnosis of sleep disorders (eg central sleep apnea, obesity hypoventilation syndrome, narcolepsy, and rapid eye movement behavior disorder), severe cardiopulmonary diseases or unstable medical conditions (eg chronic obstructive pulmonary disease, heart failure, myocardial infarction, acute infection, trauma and surgery within one month), disturbed sleep regularity (shift work, jet lag or irregular work schedules over the past 1 month) or other contradictions for HSAT (eg neuromuscular diseases, opiate use, and insomnia). For sample size estimation, see Supplementary Material.
Protocol
Our study comprised two monitoring components: in-laboratory ANO monitoring (ANOlab) and HSAT using ANO (ANOhome). For ANOlab, participants underwent PSG and ANO monitoring simultaneously in the sleep laboratory. For ANOhome, patients underwent ANOhome out of sleep center, referring to home or other inpatient wards, and PSG was performed in another night within one week.
The study complied with the Declaration of Helsinki and was approved by the Institutional Review Board of Peking University People’s Hospital (No. 2022PHB359-001). Written informed consent was obtained from each participant.
PSG Recordings
PSG were conducted in accordance with the recommendations of the American Academy of Sleep Medicine (AASM).11 The following signals were recorded: electroencephalogram (F3-M2, F4-M1, C3-M2, C4-M1, O1-M2, O2-M1), bilateral electrooculogram, chin muscle electromyogram, oronasal thermistor, nasal pressure, rib cage and abdominal movement, electrocardiogram (lead 1), snoring, body position, bilateral anterior tibialis electromyograms, and pulse rate and oxygen saturation by pulse oximetry.
Portable Monitor Recordings
Philips Respironics Inc. provided the ANO devices, pads used for uploading data, analytic software, and cloud database service, with no other involvement besides. The ANO devices collected oxygen saturation and pulse rate via finger pulse oximetry, airflow via nasal cannula (nasal pressure), respiratory effort via one thoracoabdominal RIP belt, snoring and body position by central box. For ANOlab monitoring, patients wore both sets of recording (PSG and ANO devices) simultaneously. As for ANOhome, ANO devices were worn by patients at home or in other inpatient wards, with instructions provided through an instructional card and video.
Recordings Scoring
The PSG and portable monitor recordings were scored by qualified technicians, in accordance with the AASM scoring manual. The scoring process was conducted in a blinded manner. Apneas were scored when there was a ≥90% reduction in airflow from baseline for ≥10 seconds on the oronasal thermistor signal. The same criteria used to identify obstructive, central, and mixed apneas on the portable monitor recordings were used to score those events using PSG. Hypopneas were defined by a ≥ 30% reduction in a respiratory signal for at least 10 seconds associated with a ≥ 3% reduction in oxygen saturation or an arousal. AHI measured using PSG was calculated as the average number of apnea and hypopnea events per hour of sleep. Oxygen desaturation was defined in our laboratory as a decrease of ≥3% for both PSG and portable monitor recordings.11 To test the discrepancy in the indices caused by the difference between total sleep time (TST) on PSG and monitoring time (MT) on ANO, we introduced a correction based on sleep efficiency. The ratio of TST to total recording time (TRT) on PSG was defined as sleep efficiency.

Remote Data Transmission and Verification of Integrity
In addition to traditional data transmission, ANO recordings could be transmitted to a portable pad via wire, then automatically uploaded to the cloud database via a wireless network (5G cellular network in our study). The recording data could be accessed, downloaded automatically, and scored using the Sleepware G3 software, when the computers in the sleep center were connected to the Internet. Furthermore, any scoring or editing was synchronized with the cloud database. The data were downloaded and collected, then compared with the original data to verify the integrity and identity.
The Message-digest 5 (MD5) algorithm is a one-way hash function developed by Ron Rivest, which is widely used to verify file identity and integrity. It is designed to determine whether data transmitted over the internet has been altered.12 This algorithm encrypts digital data into a 32-digit code, such as 04e12fb6213e7be8f5afd85573e24aa2. Even a minor change, such as altering one character in a file, would result in a completely different MD5 code. The ANO original data recordings were stored in .edf format. A single night’s recording might generate multiple .edf files, depending on the monitoring duration. Each .edf file was assigned a unique MD5 code. Then there would be two sets of MD5 codes: one for the cloud data and one for the original data. By comparing the MD5 codes of the cloud data with those of the original data, we could verify the integrity of the cloud data and confirm its identity.
Statistical Analysis
Continuous variables were expressed as mean ± standard deviation (SD), with normality of distribution verified using the Kolmogorov–Smirnov tests. Paired t-tests were performed to assess the level of agreement between variables, while Pearson’s correlation coefficient (R) was used to evaluate their correlation. As the primary outcome variables were the REI and AHI derived from ANO and PSG, in order to test their agreement, a statistic method described by Bland and Altman was introduced.13,14
For diagnostic tests, using AHI on PSG we determined the presence and severity of every patient, and test the sensitivity, specificity, likelihood ratios and positive/negative predictive values when using REI on ANO for diagnosis. We graphed identity scatter plots and sheets that patients falling into different groups diagnosed by REI on ANO compared with gold standard PSG. For remote data transmission verification, the 32-digit MD5 codes generated for remotely transmitted data were directly compared with those of the original data to verify identity and integrity. The results were presented as numbers and percentages. Data were analyzed using IBM SPSS Statistics (version 26), MedCalc (version 19) and R (version 4.4.3).
Results
Sample Overview and Success Rate
As illustrated in Figure 1, 99 and 180 patients were enrolled in the study of ANOlab and ANOhome respectively. Of the 99 paired PSG and ANOlab recordings conducted, 8 ANOlab recordings failed and were excluded (6 records had short total recording time [<240 minutes], and 2 recordings had airflow signal loss [losing >50% of total recording time]). Consequently, the success rate for ANOlab monitoring was 91.9% (91/99). Similarly, among the 180 ANOhome monitoring conducted, 10 failed and were excluded from analysis (8 records had short total recording time, and 2 records had airflow signal loss). Thus, the success rate for ANOhome monitoring was 94.4% (170/180).
 |
Figure 1 Diagram of the overall study flow. |
The participants in the ANOlab group were 78.0% male, with age of 50.1 ± 14.6 years, a body mass index (BMI) of 27.1 ± 4.1 kg/m², and an AHI of 31.6 ± 25.0 events/hour. In the ANOhome group, 67.3% of the participants were male, with an age of 57.0 ± 14.4 years, a BMI of 27.1 ± 3.8 kg/m², and an AHI of 35.3 ± 21.3 events/hour.
Comparison of Parameters in Sleep Reports
The results of PSG and ANOlab recording were compared firstly (see Table 1). Total recording time did not show a significant difference (P = 0.054), but MT of ANOlab was on average 100.6 minutes longer than TST of PSG. There was no difference between the ANOlab and PSG in the number of total respiratory events and hypopnea events per night. But there were differences in the numbers of obstructive/mixed apnea events and central apnea events. Thus, the REI on ANOlab was significantly lower than AHI on PSG (P < 0.001). There was no difference in ODI3 and mean SpO2 between ANOlab and PSG. Most parameters showed strong correlation (R ≥ 0.6) except for TRT, TST/MT and the number of central apneas.
 |
Table 1 Description and Comparison on Sleep Parameters Acquired by PSG and ANOlab Recordings |
The results of PSG and ANOhome recording were also compared (shown in Table 2), with similar trends to the comparison between PSG and ANOlab: longer MT and lower REI on ANOhome. There was no significant difference between the total respiratory events on PSG and ANOhome (P = 0.172). Most parameters showed strong correlation (R ≥ 0.6) except for TRT, TST/MT, the numbers of central apneas and hypopneas.
 |
Table 2 Description and Comparison on Sleep Parameters Acquired by PSG and ANOhome Recordings |
Correlation and Agreement Between Monitoring Methods
The correlation coefficient between REI on ANOlab and AHI on PSG was 0.953 (see Figure 2). Bland-Altman analysis indicated a mean difference of −6.7 events/h (95% CI: −8.4 to −4.9, P<0.001), with limits of agreement ranging from −23.0 to 9.6 events/h. When corrected REI on ANOlab was compared with AHI on PSG, Bland-Altman analysis showed a mean difference of −1.1 events/h (95% CI: −2.5 to 0.3, P = 0.113).
 |
Figure 2 Scatter plot and Bland-Altman plot of REI on ANOlab and AHI on PSG, and Bland-Altman plot of corrected REI on ANOlab and AHI on PSG. (n = 91). (A) Scatter plot of REI on ANOlab and AHI on PSG. (B) Bland-Altman plot of REI on ANOlab and AHI on PSG. (C) Bland-Altman plot of corrected REI on ANOlab and AHI on PSG. * For detailed statistical results of Bland-Altman analyses, such as regression equation, see Supplementary Table S1. |
The correlation coefficient of REI on ANOhome and AHI on PSG was 0.795 (see Figure 3). The Bland-Altman plot revealed a mean difference of −8.0 events/h (95% CI: −9.9 to −6.0, P < 0.001), with limits of agreement ranging from –30.7 to 17.3 events/h. When corrected REI on ANOhome was compared with AHI on PSG, Bland-Altman analysis showed a mean difference of −1.9 events/h (95% CI: −4.1 to 0.3, P = 0.093).
 |
Figure 3 Scatter plot and Bland-Altman plot of REI on ANOhome and AHI on PSG, and Bland-Altman plot of corrected REI on ANOhome and AHI on PSG. (n = 170). (A) Scatter plot of REI on ANOhome and AHI on PSG. (B) Bland-Altman plot of REI on ANOhome and AHI on PSG. (C) Bland-Altman plot of corrected REI on ANOhome and AHI on PSG. * For detailed statistical results of Bland-Altman analyses, such as regression equation, see Supplementary Table S1. |
Diagnostic Accuracy
Table 3 compares the diagnostic performance of ANOlab and ANOhome across different REI thresholds. With a threshold of REI ≥ 5 events/h, ANOlab had 97.4% sensitivity, 92.9% specificity, 98.7% positive predictive value, 86.7% negative predictive value and 96.7% accuracy. For patients with moderate-to-severe OSA whose AHI was ≥15 events/h, ANOlab exhibited reduced sensitivity (86.4%) but improved specificity (96.9%). For ANOhome, a threshold of REI ≥ 5 events/h resulted in 98.8% sensitivity, 90.0% specificity, 99.4% positive predictive value, 81.8% negative predictive value and 98.2% accuracy. For patients with moderate-to-severe OSA whose AHI was ≥15 events/h, ANOhome had decreased sensitivity (88.9%) but maintained relatively high specificity (74.3%).
 |
Table 3 Diagnostic Test of ANOlab and ANOhome Compared with Different Cutoffs of REI Compared with Gold Standard PSG |
Figure 4 presents the receiver operating characteristic (ROC) curves comparing the diagnostic performance of REI and corrected REI from ANOlab and ANOhome for detecting OSA and moderate-severe OSA. ANOlab demonstrated excellent diagnostic accuracy, with REI showing AUC values of 0.991 (OSA) and 0.959 (moderate-severe OSA), corresponding to optimal cutoff values of 5.7 (sensitivity 95%, specificity 100%) and 15.15 (sensitivity 84%, specificity of 97%), respectively. Similarly, ANOhome showed strong performance with AUCs of 0.955 (OSA) and 0.868 (moderate-severe OSA), with best cutoff thresholds at 4.05 (sensitivity 98%, specificity 90%) and 19.45 (sensitivity 71%, specificity 91%), respectively. While the Youden index-optimized cutoffs favored specificities, clinical consideration of ANOhome’s REI underestimation suggested adopting REI ≥15.9 (sensitivity 81%, specificity 80%) as a balanced threshold for moderate-severe OSA detection. Corrected REI values exhibited largely comparable diagnostic accuracy across both systems.
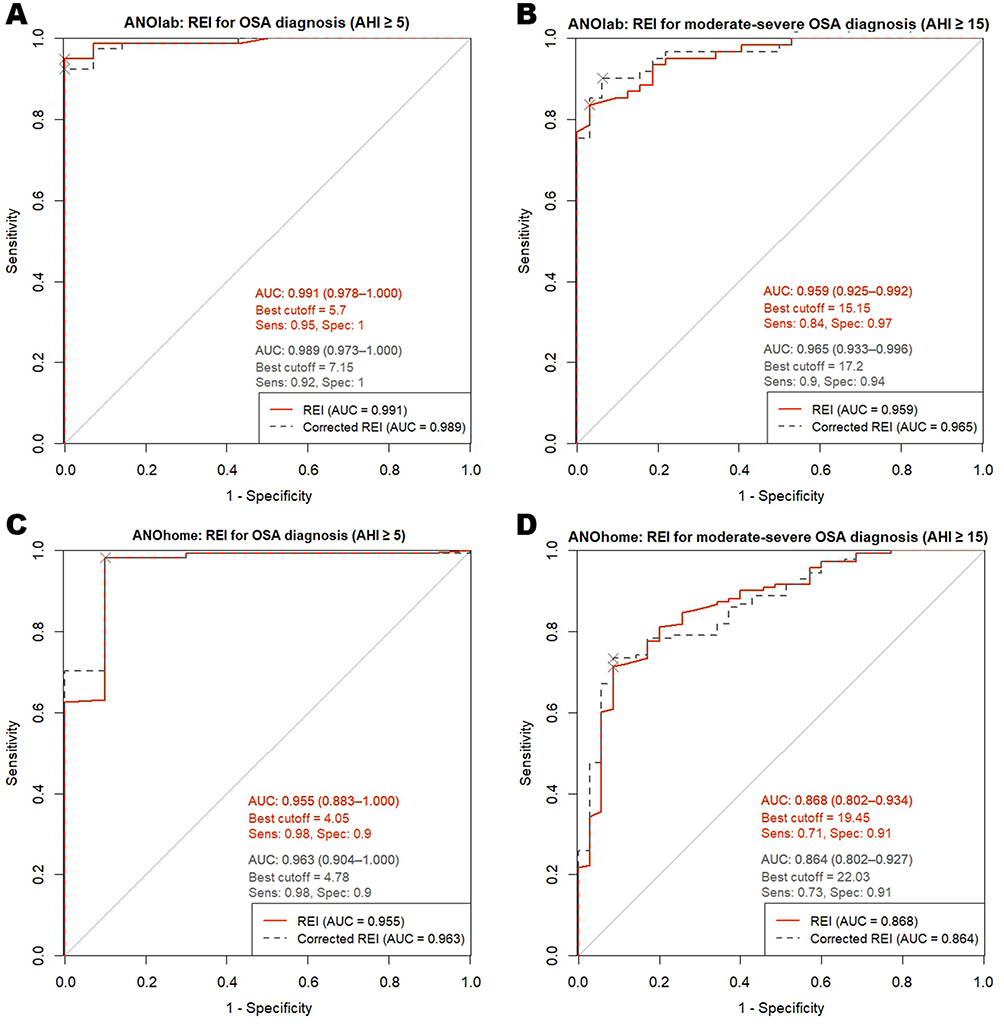 |
Figure 4 Receiver operating characteristic (ROC) curve evaluating REI diagnostic accuracy for OSA. (A) ANOlab: REI performance in diagnosing OSA (AHI ≥ 5). (B) ANOlab: REI performance in diagnosing moderate-severe OSA (AHI ≥ 15). (C) ANOhome: REI performance in diagnosing OSA (AHI ≥ 5). (D) ANOhome: REI performance in diagnosing moderate-severe OSA (AHI ≥ 15). |
ANO vs PSG Based on OSA Severity
Figure 5 illustrates the numbers and percentage of subjects categorized as having no OSA, mild, moderate, or severe OSA based on AHI on PSG or REI on ANOlab/ANOhome. Consistent with the agreement between PSG and ANOlab, the proportions in each clinical grouping were similar for these two methods. Compared to PSG, ANOhome identified a higher proportion of participants in the moderate OSA group and a lower proportion in the severe OSA group. Although ANOlab and ANOhome demonstrated occasional misclassification across OSA severity categories, no instances of gross misclassification (eg, labeling moderate-severe OSA as non-OSA) were observed.
 |
Figure 5 The percentages and numbers of patients falling into clinical OSA groupings based on PSG and ANOlab (left) or ANOhome (right) results. (A) Proportional distribution of patients across clinical OSA severity groups, comparing AHI on PSG and REI on ANOlab. (B) Proportional distribution of patients across clinical OSA severity groups, comparing AHI on PSG and REI on ANOhome. (C) The numbers of patients falling into clinical OSA groupings based on AHI on PSG and REI on ANOlab. (D) The numbers of patients falling into clinical OSA groupings based on AHI on PSG and REI on ANOhome. None: AHI or REI < 5; Mild: AHI or REI ≥5 and <15; Moderate: AHI or REI ≥15 and <30; Severe: AHI or REI ≥30. |
Reliability in Remote Data Transmission
A total of 129 recordings (63 ANOlab, 66 ANOhome) were uploaded, with 126 (62 ANOlab, 64 ANOhome) successful uploads, resulting in a success rate of 97.7%. Utilizing MD5 algorithm, the tool for verifying file integrity and identity, we generated 126 pairs of MD5 code sets for 126 original recordings that were transmitted via wire, and for 126 corresponding cloud data recordings. A total of 1205 pairs of MD5 codes were generated, for 1205 .edf files. The analysis revealed that 1199 pairs (99.50%) of MD5 codes from the two transmission methods were identical, confirming that the uploading and downloading processes did not compromise recording integrity or alter the data.
Furthermore, our practice demonstrated that scoring could be reliably performed using cloud data, with any modifications – such as scoring adjustments or report generation – seamlessly synchronized, provided the scoring device was connected to the Internet.
Discussion
The results demonstrated a relatively good performance in screening and diagnosing OSA by ANO monitoring, as evidenced by the strong correlation between PSG and ANO recordings, both in-lab and out of sleep center. A comparison of total respiratory events recorded by PSG and simultaneous ANOlab monitoring revealed no significant differences, indicating the reliability of ANO signals. Both ANOhome and ANOlab demonstrated high sensitivity and specificity in OSA diagnosis, as well as in identifying moderate-to-severe OSA. Additionally, this study showed that the data collected by ANO could be successfully transmitted wirelessly, with the MD5 algorithm ensuring the integrity and identity of the transmitted data.
Currently, thoracoabdominal movements monitoring remains most frequently used for detecting respiratory effort during sleep, using RIP, piezoelectric or polyvinylidene difluoride (PVDF) belts.4 AASM does not recommend the use of 1 RIP belt, 2 or 1 piezo belt and other effort measures due to the scanty publication of regarding researches,9 and AASM scoring manual (version 3) listed “single thoracoabdominal RIP belt” as acceptable.11 European Respiratory Society (ERS) does not require a specific number of RIP belts in its technical standards for type 3 PM, and describes RIP as often is a “back-up” signal for detecting respiratory events.4 Prior to our study, several studies tested the performance of different PMs using single-belt respiratory effort recording, as listed in Table 4. Our study extended this research by validating the reliability of ANO, a type 3 PM with single RIP belt, in detecting respiratory events and identifying OSA patients. Notably, ANO demonstrated superior performance with higher sensitivities and specificities compared to other PMs, while maintaining its distinctive advantage in data teletransmission capabilities. All of these studies showed that a single belt could reliably monitor respiratory effort signals in patients with OSA. Thinking about all the above, the single-belt technology could be recommended for the diagnosing of OSA in patients with a high pretest probability of moderate-to-severe OSA besides the current guideline recommendation.
 |
Table 4 Characteristics of Studies Comparing Single-Belt Type 3 PMs and PSG |
Noticed by our study, single-belt technology may occasionally face challenges in distinguishing central from obstructive or mixed respiratory events. As during the obstructive events, the respiratory movement of chest and abdomen could be contradictory, and the single-belt might mistake these events as central ones. However, since central apneas typically constitute only a minor proportion of total respiratory events in OSA patients, this limitation does not significantly impact the overall diagnostic accuracy for OSA. We also suggested that particular attention must be paid to ensuring proper RIP belt tightness during testing, as this critically affects respiratory effort signal quality. Notably, ANO may demonstrate a slight tendency to overestimate central apneas. Therefore, following strategies should be recommended. Comprehensive sleep evaluation must be supervised by a sleep medicine practitioner before using PM. When HSAT results show a substantial number of central apneas or pattern of Cheyne-Stokes breathing, PSG should be performed. Patients with known predisposing factors for central sleep apnea (such as heart failure) should be considered for PSG or other validated portable devices, but not this kind of single-belt technology.
In the simultaneous monitoring of ANOlab and PSG, MT on ANOlab was on average 100.6 minutes longer than TST on PSG, as the lack of sleep staging in ANO tended to result in lower indices on ANO. The significant differences between REI and AHI were observed mainly because of the variation between MT and TST.19–22 In both Bland-Altman analyses of REI on ANO and AHI on PSG, regression analysis indicated a negative correlation between the difference and mean (Figures 2B, 3B and supplementary Table S1), suggesting that in patients with higher AHI values, ANOlab and ANOhome were more likely to underestimate of the REI, resulting in a larger difference between REI on ANOlab/ANOhome from the actual AHI. After the correction of REI on ANOlab and ANOhome using sleep efficiency, both Bland-Altman analyses showed no significant difference between those two REI and AHI. The discrepancy between recording time and sleep time has been an important factor influencing the indices in portable monitoring devices, and similar results were reported in other studies of type 3 PMs in OSA. Cho et al found that sleep efficiency negatively correlated with the AHI difference, while the arousal index positively correlated in their validation study of the ApneaLink Plus.15 Xu et al addressed this issue by collecting self-reported sleep duration and modifying the monitoring time by the responses and recorded activity signals to generate more precise indices.23 In further practice, greater efforts should be made to estimate total sleep time more accurately to enhance the reliability of portable monitoring devices.
Both ANOhome and ANOlab demonstrated reliable value in OSA diagnosis. However, Bland-Altman analysis between REI on ANOhome with AHI on PSG showed a mean difference of −8.0 events/h, which was thought to be contributed by the known night-to-night variability of sleep and the discrepancy between MT and TST.24–26 The maximum one-week interval between PSG and ANOhome testing was designed to minimize night-to-night variability, while acknowledging that complete elimination of this inherent physiological fluctuation was unachievable. Moreover, as ANO lacked a method such as electroencephalogram to detect arousal events, it identified fewer hypopneas, resulting in a reduced REI. As illustrated in Figure 5, while ANOhome results were effective in diagnosing OSA, they tended to underestimate the severity of OSA, primarily due to the same factors as in prior papers.27,28
While the underestimation of REI on ANOlab/ANOhome may largely contribute to the discrepancy in TST and MT, and corrected by sleep efficiency, the persistent gap could have implications in clinical practice, such as missed or delayed diagnosis in mild-to-moderate OSA patients. However, our study demonstrated that ANOhome maintained high sensitivity (98.8% for OSA and 88.9% for moderate-to-severe OSA), supporting its utility as a screening or diagnostic tool. To mitigate underestimation, potential clinical strategies should be considered: For high-risk phenotypes (eg, high BMI, or comorbid with hypertension), a more proactive treatment approach may be warranted, even with borderline REI values; For symptomatic patients, such as showing high ESS scores, with REI values between 5 and 15, confirmatory PSG should be performed if available or choose a lower cutoff of REI for treatment; For patients with insomnia complaints, ANOhome may not be the optimal diagnostic tool, and alternative PSG should be prioritized.
Telemedicine, consisting of all stages of diagnosis, treatment and follow-up, has gained wide acceptance across various medical specialties.10 For sleep-related breathing disorders, the data teletransmission of PSG or home monitoring plays a crucial role. Though the reliability of PSG data teletransmission has been validated in previous studies,29–31 researches on the teletransmission and telediagnosis of HSAT devices remained limited. In our study, the HSAT data collected by ANO was successfully transmitted wirelessly, as supported when the integrity and identity of the transmitted data ensured by the MD5 algorithm. These results demonstrated the reliability of ANO in remote data transmission, providing a robust foundation for the telediagnosis and follow-up of OSA.32 However, from our experience, the uploading process was somewhat complex for the general population. The ANO system utilized Philips Sleepware G3 software - the same platform employed for PSG scoring and other professional sleep monitoring devices. While this software provided comprehensive functionality for healthcare professionals, its interface complexity created barriers for other users, including the multiplicity of buttons and functions designed for specialist use, the non-intuitive sequence of operations required for data upload, and interface elements with small font sizes on tablet devices. Developing a simplified one-click, intuition-driven interface and optimizing the uploading process would likely improve feasibility in practical telemedicine applications. Furthermore, several practical implementation challenges must be considered for real-world telemedicine applications, such as the need for standardized protocols to accommodate varying levels of technical infrastructure across clinical settings, to account for potential internet connectivity issues and to establish clear contingency protocols for failed transmissions.
However, our study had several limitations. Firstly, the sequence of in-laboratory monitoring of PSG and HSAT was not fixed. As the “first-night effect” in the sleep laboratory may lead to some changes in sleep architecture, the different sequence might lead to different impact on sleep-related parameters.33 Secondly, the data in our study were uploaded by technicians rather than patients themselves, which did not fully reflect real-world telemedicine scenarios. Thirdly, when the subjects conducted the HSAT, they should be told to record the estimated sleep time and other influence factors to reduce the bias between in center PSG and HSAT. Lastly, the further validation study should explore these findings in diverse clinical populations, particularly those with comorbid conditions, to enhance generalizability.
Conclusion
In summary, the study proves that Alice NightOne is a reliable type 3 portable monitor with single thoracoabdominal belt for diagnosis of OSA. Its good sensitivity and specificity in both in-laboratory and home monitoring, coupled with its robust remote data transmission function, positions it as a valuable tool for facilitating telediagnosis and management of OSA patients, potentially improving access to care. The system, including the monitor device and the remote data transmission kit, will provide a new access for the patients with suspected OSA.
Abbreviations
AASM, American Academy of Sleep Medicine; AHI, apnea-hypopnea index; ANO, Alice NightOne; ANOhome, home sleep apnea testing using Alice NightOne; ANOlab, in-laboratory Alice NightOne monitoring; BMI, body mass index; CI, confidence interval; ERS, European Respiratory Society; HSAT, home sleep apnea testing; LR+, positive likelihood ratio; LR-, negative likelihood ratio; MD5, Message digest-5; MT, monitoring time; NPV, negative predictive value; ODI3, oxygen desaturation index (decreased by ≥3%); OSA, obstructive sleep apnea; PM, portable monitor; PPV, positive predictive value; PSG, polysomnography; R, Pearson correlation coefficient; REI, respiratory event index; RIP, respiratory inductance plethysmography; ROC, receiver operating characteristic; SD, standard deviation; SIT90, saturation-impaired time of oxygen saturation < 90%; SpO2, percutaneous arterial oxygen saturation; TRT, total recording time; TST, total sleep time.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, XiaoSong Dong, upon reasonable request.
Author Contributions
MaoHuan Peng: Data curation, software, formal analysis, visualization, and writing – original draft.
YuanYuan Zhang: Methodology, resources, validation, visualization, and writing – original draft.
Rui Zhao, LiHua Deng, XinRu Wang, XueLi Zhang, Jing Li, Long Zhao, Bing Zhou: Data curation, investigation, writing – review and editing.
XiaoSong Dong: Conceptualization, supervision, funding acquisition, writing – review and editing.
Fang Han: Conceptualization, resources, project administration, writing – review and editing.
All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
Dr. XiaoSong Dong was supported by the National Key Research and Development Program of China (Project No. 2023YFC3603503), and Natural Science Foundation of China (82470092).
Disclosure
Philips Respironics provided the Alice NightOne devices and analytic software. All authors have indicated no financial conflicts of interest. Work for this study was performed at Peking University People’s Hospital.
The abstract of this paper was presented at the 17th World Sleep Congress as a poster presentation with interim findings. The poster’s abstract was published in ‘Abstracts from the 17th World Sleep Congress’ in Sleep Medicine (Volume 115, Supplement 1, February 2024, Page S420): https://doi.org/10.1016/j.sleep.2023.11.1126.
References
1. Kapur VK, Auckley DH, Chowdhuri S, et al. Clinical practice guideline for diagnostic testing for adult obstructive sleep apnea: an American Academy of sleep medicine clinical practice guideline. J Clin Sleep Med. 2017;13(3):479–504. doi:10.5664/jcsm.6506
2. Kirsch DB. PRO: sliding into home: portable sleep testing is effective for diagnosis of obstructive sleep apnea. J Clin Sleep Med. 2013;9(1):5–7. doi:10.5664/jcsm.2324
3. Collop NA, Anderson WM, Boehlecke B, et al. Clinical guidelines for the use of unattended portable monitors in the diagnosis of obstructive sleep apnea in adult patients. J Clin Sleep Med. 2007;3(7):737–747.
4. Riha RL, Celmina M, Cooper B, et al. ERS technical standards for using type III devices (limited channel studies) in the diagnosis of sleep disordered breathing in adults and children. Eur Respir J. 2023;61(1):2200422. doi:10.1183/13993003.00422-2022
5. Voulgaris A, Ferini-Strambi L, Steiropoulos P. Sleep medicine and COVID-19. Has a new era begun? Sleep Med. 2020;73:170–176. doi:10.1016/j.sleep.2020.07.010
6. Kole A. Home sleep apnea testing in the era of COVID-19: a community perspective. J Clin Sleep Med. 2020;16(9):1633. doi:10.5664/jcsm.8614
7. Powell AC, Horrall LM, Long JW, Gupta AK, Gitnacht D. Sleep testing during the pandemic. Sleep Med. 2023;101:375–383. doi:10.1016/j.sleep.2022.11.008
8. Association SoPCotASD. Practice parameters for the use of portable recording in the assessment of obstructive sleep apnea. Sleep. 1994;17(4):372–377.
9. Collop NA, Tracy SL, Kapur V, et al. Obstructive sleep apnea devices for out-of-center (OOC) testing: technology evaluation. J Clin Sleep Med. 2011;7(5):531–548. doi:10.5664/JCSM.1328
10. Verbraecken J. Telemedicine in sleep-disordered breathing: expanding the horizons. Sleep Med Clin. 2021;16(3):417–445. doi:10.1016/j.jsmc.2021.05.009
11. Troester MM, Quan SF, Berry RB, et al. The AASM Manual for the Scoring of Sleep and Associated Events - Rules, Terminology and Technical Specifications. Version 3. Darien, IL: American Academy of Sleep Medicine; 2023.
12. Rivest R. RFC1321: The MD5 Message-Digest Algorithm. United States: RFC Editor; 1992.
13. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;327(8476):307–310. doi:10.1016/S0140-6736(86)90837-8
14. Bland JM, Altman DG. Comparing methods of measurement: why plotting difference against standard method is misleading. Lancet. 1995;346(8982):1085–1087. doi:10.1016/S0140-6736(95)91748-9
15. Cho JH, Kim HJ. Validation of ApneaLink Plus for the diagnosis of sleep apnea. Sleep Breath. 2017;21(3):799–807. doi:10.1007/s11325-017-1532-3
16. Cheliout-Heraut F, Djouadi F, Senny F, Ouayoun M, Bour F. Obstructive sleep apnoea syndrome: comparison between polysomnography and portable sleep monitoring based on jaw recordings. Neurophysiol Clin. 2011;41(4):191–198. doi:10.1016/j.neucli.2011.09.001
17. Santos-Silva R, Sartori DE, Truksinas V, Truksinas E. Validation of a portable monitoring system for the diagnosis of obstructive sleep apnea syndrome. Sleep. 2009;32(5):629–636. doi:10.1093/sleep/32.5.629
18. Polese JF, Santos-Silva R, de Oliveira Ferrari PM, Sartori DE, Tufik S, Bittencourt L. Is portable monitoring for diagnosing obstructive sleep apnea syndrome suitable in elderly population? Sleep Breath. 2013;17(2):679–686. doi:10.1007/s11325-012-0742-y
19. Setty AR. Underestimation of sleep apnea with home sleep apnea testing compared to in-laboratory sleep testing. J Clin Sleep Med. 2017;13(4):531–532. doi:10.5664/jcsm.6534
20. Bianchi MT, Goparaju B. Potential underestimation of sleep apnea severity by at-home kits: rescoring in-laboratory polysomnography without sleep staging. J Clin Sleep Med. 2017;13(4):551–555. doi:10.5664/jcsm.6540
21. Zhao YY, Weng J, Mobley DR, et al. Effect of manual editing of total recording time: implications for home sleep apnea testing. J Clin Sleep Med. 2017;13(1):121–126. doi:10.5664/jcsm.6404
22. Claman D, Sunwoo B. Improving accuracy of home sleep apnea testing. J Clin Sleep Med. 2017;13(1):9–10. doi:10.5664/jcsm.6374
23. Xu L, Han F, Keenan BT, et al. Validation of the Nox-T3 portable monitor for diagnosis of obstructive sleep apnea in Chinese adults. J Clin Sleep Med. 2017;13(5):675–683. doi:10.5664/jcsm.6582
24. Bon OL, Hoffmann G, Tecco J. Mild to moderate sleep respiratory events - one negative night may not be enough. Chest. 2000;118(2):353–359. doi:10.1378/chest.118.2.353
25. Punjabi NM, Patil S, Crainiceanu C, Aurora RN. Variability and misclassification of sleep apnea severity based on multi-night testing. Chest. 2020;158(1):365–373. doi:10.1016/j.chest.2020.01.039
26. Dzierzewski JM, Dautovich ND, Rybarczyk B, Taylor SA. Night-to-night fluctuations in sleep apnea severity: diagnostic and treatment implications. J Clin Sleep Med. 2020;16(4):539–544. doi:10.5664/jcsm.8272
27. Ahmadi N, Shapiro GK, Chung SA, Shapiro CM. Clinical diagnosis of sleep apnea based on single night of polysomnography vs. two nights of polysomnography. Sleep Breath. 2009;13(3):221–226. doi:10.1007/s11325-008-0234-2
28. Jonas DE, Amick HR, Feltner C, et al. Screening for Obstructive Sleep Apnea in Adults: An Evidence Review for the U.S. Preventive Services Task Force. Rockville (MD): Agency for Healthcare Research and Quality (US); 2017.
29. Bruyneel M, Van den Broecke S, Libert W, Ninane V. Real-time attended home-polysomnography with telematic data transmission. Int J Med Inform. 2013;82(8):696–701. doi:10.1016/j.ijmedinf.2013.02.008
30. Borsini E, Blanco M, Bosio M, Fernando DT, Ernst G, Salvado A. “Diagnosis of sleep apnea in network” respiratory polygraphy as a decentralization strategy. Sleep Sci. 2016;9(3):244–248. doi:10.1016/j.slsci.2016.10.009
31. Bruyneel M. Telemedicine in the diagnosis and treatment of sleep apnoea. Eur Respir Rev. 2019;28(151):180093. doi:10.1183/16000617.0093-2018
32. Tran NT, Tran HN, Mai AT. A wearable device for at-home obstructive sleep apnea assessment: state-of-the-art and research challenges. Front Neurol. 2023;14:1123227. doi:10.3389/fneur.2023.1123227
33. Ding L, Chen B, Dai Y, Li Y. A meta-analysis of the first-night effect in healthy individuals for the full age spectrum. Sleep Med. 2022;89:159–165. doi:10.1016/j.sleep.2021.12.007
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.