")
Back to Journals » Journal of Inflammation Research » Volume 18
Diagnostic and Predictive Values of Soluble Triggering Receptor Expressed on Myeloid Cells-1 in Sepsis: A Multi-Center Prospective Clinical Study
Authors Wang K, Zhang Y, Sang L, Hu Y, Su L, Xie S, Xiao K, Xu J, Wang J, Xie F, Zhu G, Fu S, Xie L
Received 24 January 2025
Accepted for publication 20 June 2025
Published 25 June 2025 Volume 2025:18 Pages 8419—8427
DOI https://doi.org/10.2147/JIR.S519333
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Qing Lin
Kaifei Wang,1,* Youchen Zhang,2,* Lei Sang,3,* Ye Hu,1,* Longxiang Su,4 Sheling Xie,1 Kun Xiao,1 Jianqiao Xu,1 Jiang Wang,1 Fei Xie,1 Guangfa Zhu,5 Shihui Fu,6– 8 Lixin Xie1
1College of Pulmonary and Critical Care Medicine, Chinese PLA General Hospital, Beijing, People’s Republic of China; 2Department of Pediatrics, Hainan Hospital of Chinese PLA General Hospital, Sanya, People’s Republic of China; 3Information Department, Hainan Hospital of Chinese PLA General Hospital, Sanya, People’s Republic of China; 4Department of Critical Care Medicine, Peking Union Medical College Hospital, Peking Union Medical College and Chinese Academy of Medical Sciences, Beijing, People’s Republic of China; 5Department of Pulmonary and Critical Care Medicine, Beijing Anzhen Hospital, Capital Medical University, Beijing Institute of Heart, Lung and Blood Vessel Diseases, Beijing, People’s Republic of China; 6Department of Cardiology, Hainan Hospital of Chinese PLA General Hospital, Hainan Geriatric Disease Clinical Medical Research Center, Hainan Branch of China Geriatric Disease Clinical Research Center, Sanya, People’s Republic of China; 7Department of Geriatric Cardiology, Chinese PLA General Hospital, Beijing, People’s Republic of China; 8The Second School of Clinical Medicine, Southern Medical University, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shihui Fu, Department of Cardiology, Hainan Hospital of Chinese PLA General Hospital, Hainan Geriatric Disease Clinical Medical Research Center, Hainan Branch of China Geriatric Disease Clinical Research Center, Sanya, People’s Republic of China, Email [email protected] Lixin Xie, College of Pulmonary and Critical Care Medicine, Chinese PLA General Hospital, Beijing, People’s Republic of China, Email [email protected]
Objective: To determine diagnostic values of serum and urine soluble triggering receptor expressed on myeloid cells-1 (sTREM-1) in sepsis including septic shock and their predictive values for clinical prognosis and sepsis-associated acute kidney injury (AKI).
Methods: A multi-center prospective research method was used to enroll patients with sepsis.
Results: A total of 586 cases were studied, including 238 patients with sepsis and 348 healthy individuals. In the sepsis group, 84 patients (35.3%) were diagnosed with septic shock, and 93 patients (38.1%) were diagnosed with AKI. The area under the Receiver Operating Characteristic curve (AUC) for diagnosing sepsis was 0.892 (0.862– 0.922). When the cut-off value was 295 pg/mL, the sensitivity was 76.8%, and the specificity was 89.1%. The AUC for predicting AKI was 0.803 (0.739– 0.866). When the cut-off value was 485 pg/mL, the sensitivity was 88.4%, and the specificity was 65.8%.
Conclusion: sTREM-1 is a good indicator for the diagnosis of sepsis and septic shock and significantly correlated with clinical prognosis and sepsis-associated AKI in patients with sepsis. Diagnostic and predictive values of sTREM-1 may be related to inflammatory storm mediated by TREM-1. Further mechanistic explanation or preliminary evidence in combination with clinical study with more patients will benefit for supporting diagnostic and predictive utilities of sTREM-1 in sepsis.
Keywords: acute kidney injury, clinical prognosis, sepsis, septic shock, soluble triggering receptor expressed on myeloid cells-1
Introduction
General understanding of sepsis is that it is an infection-induced systemic disease that leads to pathological and physiological abnormalities. Sepsis is commonly encountered and has rapid progression in the intensive care unit; it can cause secondary multiorgan dysfunction and threaten the patient’s life in a short time. It is one of the leading causes of death. The revised diagnostic criteria for sepsis adopted in 2001 is Sepsis 2.0, which is a detailed diagnostic criteria for sepsis and emphasizes the hierarchical diagnostic theory of sepsis. With the deepening of research, it has been found that the diagnostic criteria of Sepsis 2.0 lack specificity, and there were many limitations in clinical application. In 2016, a Sepsis Definitions Task Force composed of experts from the Society of Critical Care Medicine (SCCM)/European Society of Intensive Care Medicine (ESICM) revised and updated the diagnostic criteria for sepsis. The new major criteria for sepsis were confirmed or highly suspicious infection and a Sequential Organ Failure Assessment (SOFA) score ≥2.1 Although medical science has made great progress in the recent years, the World Health Organization has estimated that the total number of deaths caused by sepsis continues to rise, and 14 million people die of sepsis in the world each year, which is more than the number of deaths caused by acute myocardial infarction, lung cancer or breast cancer.2 Since sepsis is characterized by rapid progression and high mortality, a relevant research hotspot in clinical medicine is the search for clinical biomarkers that can accurately confirm its diagnosis, timely determine its severity, and effectively predict its prognosis.
The triggering receptor expressed on myeloid cells-1 (TREM-1) was first reported in 2000. It is a transmembrane protein on the surface of neutrophils and monocytes and is involved in inflammatory response. TREM-1 can amplify the infection-related inflammatory response, and after its activation, extracellular structures can be shed to form soluble triggering receptor expressed on myeloid cells-1 (sTREM-1). It is selectively expressed on the surface of neutrophils and monocytes, is a receptor of immunoglobulin superfamily associated with inflammatory response, and has been estimated to have a relative molecular weight of 26kD.3 TREM-1 can amplify inflammatory response activated by microorganisms and their products. Pathogens, lipoteichoic acid, and lipopolysaccharide (LPS) can all increase TREM-1 expression in phagocytes. sTREM-1 is a soluble form of TREM-1; it is a cleavage product of extracellular structure of TREM-1 after the cleavage of matrix metalloproteinases.4 When cellular expression of TREM-1 increases, sTREM-1 in body fluids also increases. Studies have confirmed that sTREM-1 may be used as a biomarker for early diagnosis of inflammatory diseases.5 The purpose of this multi-center prospective clinical study was to determine diagnostic values of serum and urine sTREM-1 in sepsis including septic shock and their predictive values for clinical prognosis and sepsis-associated acute kidney injury (AKI).
Methods
Study Subjects
This study included patients with sepsis who were admitted to the intensive care unit of the First Medical Center of Chinese PLA General Hospital, the Fourth Medical Center of Chinese PLA General Hospital, the Eighth Medical Center of Chinese PLA General Hospital, the Hainan Hospital of Chinese PLA General Hospital, the Beijing Shijitan Hospital, and the Beijing Anzhen Hospital from January 1, 2016, to January 1, 2021, and healthy volunteers from these centers. The inclusion criteria were as follows: 1) hospitalized patients ≥18 years of age; 2) meeting the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis 3.0); and 3) agreeing to participate in this study and having signed the informed consent forms. The exclusion criteria were as follows: chronic renal insufficiency and renal replacement therapy. According to the Sepsis 3.0 criteria, the enrolled patients were divided into a non-septic shock group and a septic shock group. Patients in the non-septic shock group had 1) confirmed or highly suspicious infection and 2) a SOFA score ≥2. Patients in the septic shock group 1) met the diagnostic criteria for sepsis and 2) needed vasopressor drugs to maintain a mean arterial pressure ≥65 mmHg and had a serum lactate acid >2 mmol/L after fluid resuscitation. This study was approved by the Clinical Ethics Committee of Chinese PLA General Hospital with the approval number S2014-114-02 and was registered on the Clinical Trials Website with the registration number NCT02920736. Prior to this study, written informed consent forms were required from all participants. This study complies with the Declaration of Helsinki.
Sample Collection
If the inclusion criteria were met and the exclusion criteria were not met, fasting blood and urine samples of patients were collected at each research center. Blood samples were collected on day 1, day 7, and day 14 of enrollment (or until death or discharge). Urine samples were collected on day 1, day 3, day 5, day 7, and day 14 of enrollment (or until death or discharge). Venous blood samples and midstream urine samples were collected on the morning of day 1 (within 24 hours) in healthy individuals and treated in the same way that the samples from the patients were treated. A 4-mL venous blood sample was centrifuged at 3000 rpm for 15 minutes, and 2 mL of the supernatant was transferred into an Eppendorf tube. A 5-mL urine sample was kept at room temperature for 2 hours and then centrifuged at 3000 rpm for 15 minutes, and then the supernatant was transferred into an Eppendorf tube. Blood and urine samples were numbered, centrifuged, aliquoted, and then stored in a −80°C refrigerator for subsequent testing. sTREM in human blood and urine samples was detected in clinical laboratory of College of Pulmonary and Critical Care Medicine in Chinese PLA General Hospital using the Human TREM-1 Quantikine Enzyme-linked Immunosorbent Assay Kit (R&D Systems, Minnesota, USA) according to the manufacturer instructions.
Clinical Information
The following information of the enrolled patients were recorded using the developed standard case enrollment registration form: 1) sex, age, underlying diseases, admission diagnoses, and hospitalization number; 2) serum creatinine, blood urea nitrogen, complete blood count, C-reactive protein, procalcitonin, and interleukin-6; and 3) 28-day prognosis including survival or death and AKI. Based on the definition in the 2012 Kidney Disease: Improving Global Outcomes (KDIGO) clinical guideline, AKI was diagnosed based on the following criteria: 1) serum creatinine increased >3 times baseline; 2) serum creatinine increased to >353 μmol/L; 3) initiation of renal replacement therapy; and 4) urinary output <0.3 mL/kg/h during more than 24 hours.
Statistical Methods
Statistical Package for Social Science and GraphPad Prism were used for statistical analysis. The Receiver Operating Characteristic (ROC) curve was used to analyze the area under the curve (AUC) of diagnostic indices. The Youden’s J index (sensitivity+specificity-1) was used to calculate the best diagnostic cut-off values of diagnostic indices. Logistic regression models were used to adjust for confounding variables. P<0.05 was considered to be statistically significant.
Results
Basic Information of Each Group
A total of 586 cases were studied, including 238 patients with sepsis (the sepsis group, 165 males and 73 females with a median age of 64 years) and 348 healthy individuals (the control group, 240 males and 108 females with a median age of 51 years). Clinical characteristics of the enrolled patients and healthy individuals are shown in Table 1. In the sepsis group, 84 patients were diagnosed with septic shock, and 79 patients with sepsis died within 28 days, for a mortality of 33.2% (79/238).
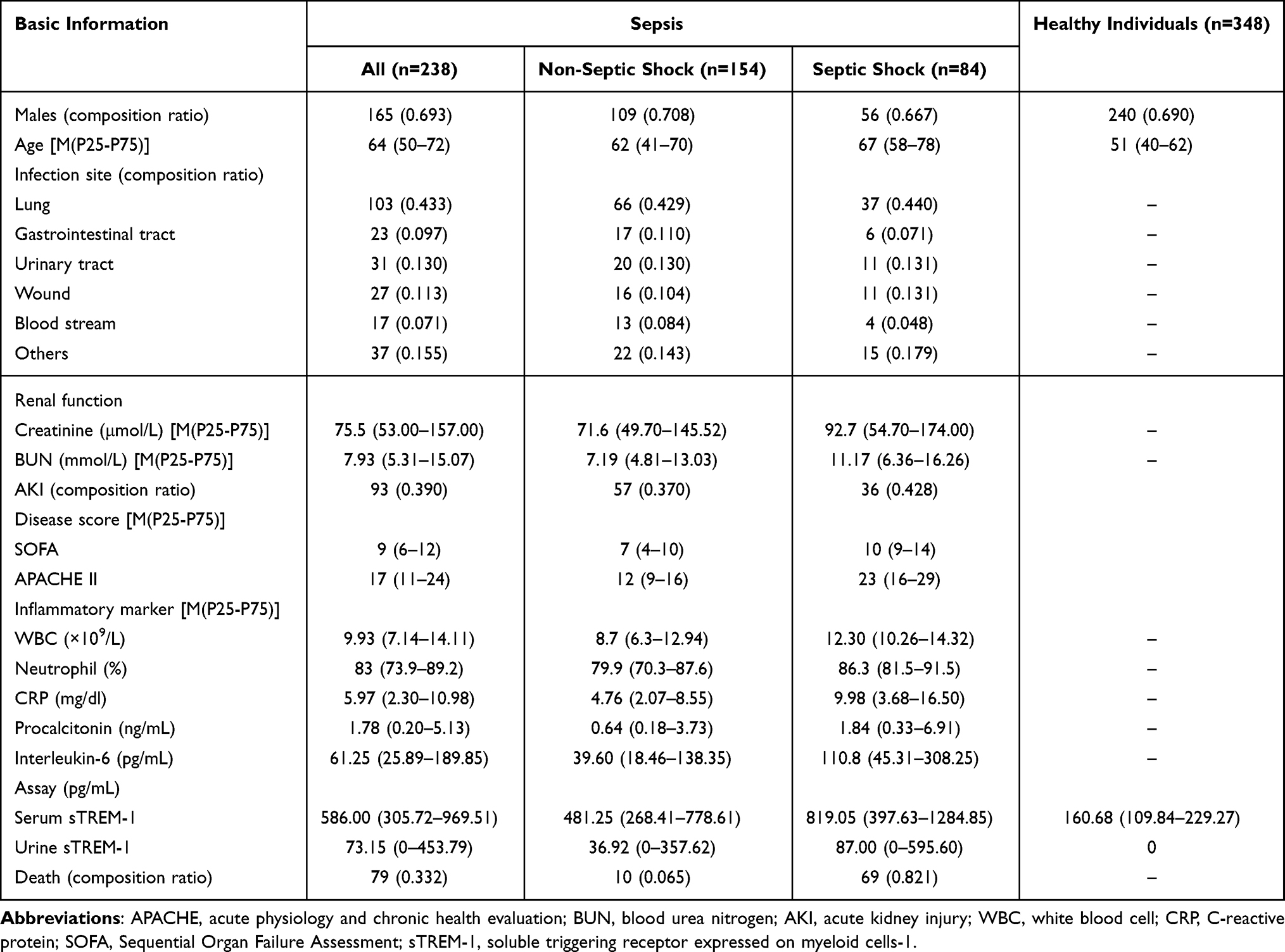 |
Table 1 Clinical Characteristics of All Participants |
Serum and Urine sTREM-1
All of the enrolled patients and healthy individuals completed venous blood and urine sample collection at least once and had data regarding sTREM-1 detection in blood and urine samples. A total of 348 healthy individuals in the control group underwent the detection of serum sTREM-1. Ages of healthy individuals were 19–91 years, and the Spearman Correlation coefficient between age and serum sTREM-1 was 0.439 (P<0.001; Figure 1A). The Mann–Whitney U-test indicated a significant difference in serum sTREM-1 between males and females (U=9908.500, P<0.001; Figure 1B). The medians of serum sTREM-1 were 175.04 (121.56–238.94) pg/mL in males, 137.55 (82.22–204.38) pg/mL in females, and 160.68 (109.84–229.27) pg/mL in the control group. The detection of sTREM-1 was performed in urine samples of 172 healthy individuals, with sTREM-1 undetectable in others, and the remaining 176 patients in the control group did not undergo further detection and analysis of urine sTREM-1.
 |
Figure 1 (A) Distribution of age and serum sTREM-1 in healthy individuals. (B) Difference of serum sTREM-1 among different sex in healthy individuals. (C) The Receiver Operating Characteristic (ROC) curve of serum sTREM-1 in diagnosing sepsis. (D) The ROC curve of serum sTREM-1 in diagnosing septic shock. (E) The ROC curve of serum sTREM-1 in predicting death. (F) The ROC curve of urine sTREM-1 in predicting death. (G) The ROC curve of serum sTREM-1 in predicting AKI. (H) The ROC curve of urine sTREM-1 in predicting AKI. (I) Trend of serum sTREM-1 over time in 19 death patients. Notes: The Spearman Correlation analysis was done for age and serum sTREM-1 (r=0.439, P<0.001). The Mann–Whitney U-test was done in serum sTREM-1 between males (M) and females (F, U=9908.500, P<0.001). The area under the ROC curve (AUC) of serum sTREM-1 for diagnosing sepsis was 0.892 (0.862–0.922, P<0.001). The AUC of serum sTREM-1 for diagnosing septic shock was 0.665 (0.586–0.744, P<0.001). The AUC of serum sTREM-1 for predicting death was 0.685 (0.608–0.763, P<0.001). The AUC of urine sTREM-1 for predicting death was 0.628 (0.545–0.711, P=0.004). The AUC of serum sTREM-1 for predicting AKI was 0.803 (0.739–0.866, P<0.001). The AUC of urine sTREM-1 for predicting AKI was 0.721 (0.645–0.798, P<0.001). Serum sTREM-1 of 19 death patients showed an increased trend. |
Values of Serum and Urine sTREM-1 for Diagnosing Sepsis
The Spearman Correlation analysis showed a significant correlation between serum and urine sTREM-1 in 238 patients who had sepsis at the time of enrollment (r=0.778, P<0.001). The Pearson’s Chi-square test showed no significant difference in sex between 238 patients in the sepsis group and 348 healthy individuals in the control group (χ2=0.009, P=0.926). The Mann–Whitney U-test showed a significant difference in age between the sepsis group and the control group (U=26394.00, P<0.001). Serum sTREM-1 of 238 patients with sepsis and 348 healthy individuals were subjected to the ROC curve. The AUC for diagnosing sepsis was 0.892 (0.862–0.922; Figure 1C). When the cut-off value was 295 pg/mL, the sensitivity was 76.8%, and the specificity was 89.1%. The detailed results are shown in Table 2. Serum sTREM-1 had a significant association with sepsis among all participants in Logistic regression model (P<0.001; Table 3). Urine sTREM-1 can be detected in the most patients with sepsis but not in the most healthy individuals, indicating that urine sTREM-1 is a specific indicator for patients with sepsis compared with healthy individuals.
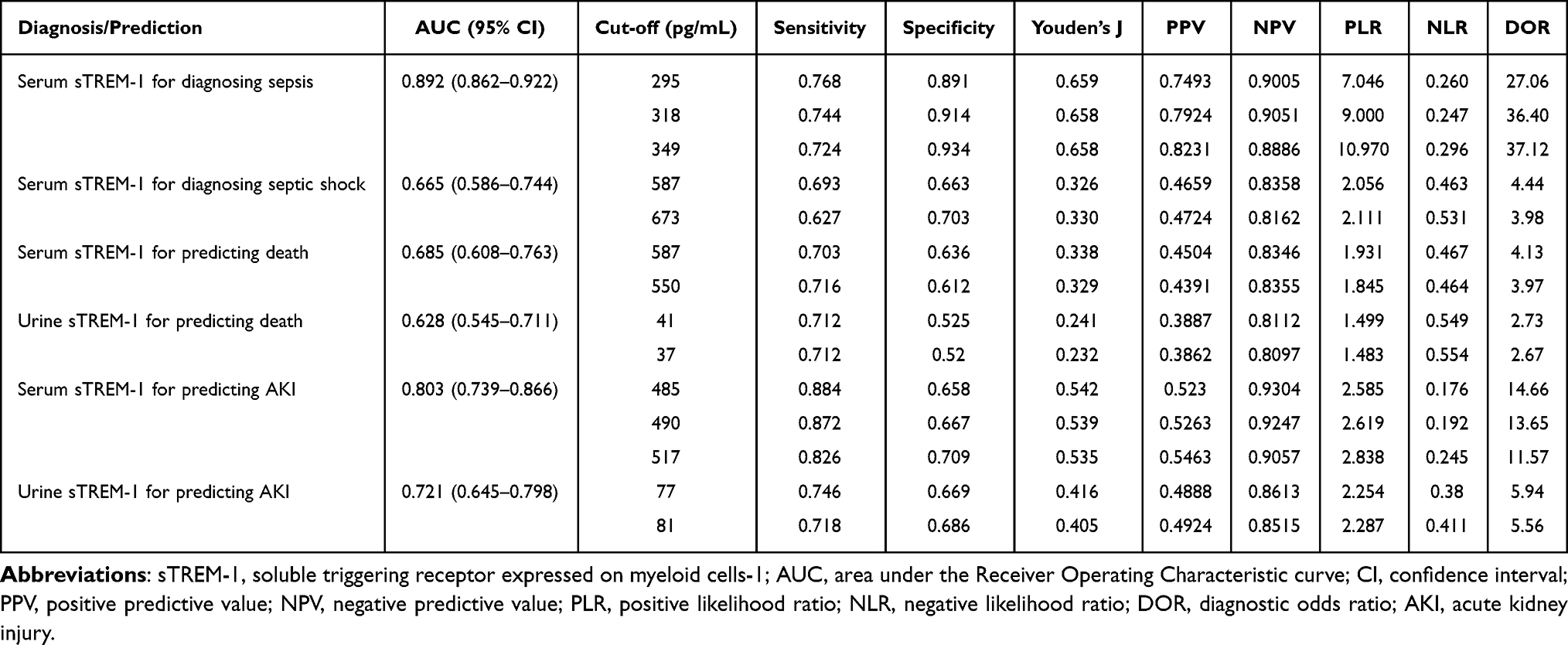 |
Table 2 Diagnostic and Predictive Values of sTREM-1 |
 |
Table 3 Associations with Serum sTREM-1 in Logistic Regression Models |
Values of Serum and Urine sTREM-1 for Distinguishing Septic Shock
Among 238 patients with sepsis who were enrolled in this study, 84 patients were diagnosed with septic shock, and there were 154 patients without septic shock. The Mann–Whitney U-test showed a significant difference in serum sTREM-1 between the non-septic shock group and the septic shock group (U=3217.00, P<0.001). The ROC curve was obtained in Figure 1D. Serum sTREM-1 had a significant association with septic shock among patients with sepsis in Logistic regression model (P=0.001). The Mann–Whitney U-test showed no significant difference in urine sTREM-1 between the non-septic shock group and the septic shock group (U=3464.5, P=0.062).
Values of Serum and Urine sTREM-1 for Predicting Death
Among 238 patients in the sepsis group, 79 patients (the death group) died, and 159 patients (the survival group) did not die within 28 days. The Mann–Whitney U-test indicated a significant difference in serum sTREM-1 at the time of enrollment between the death group and the survival group (U=3003.00, P<0.001). The AUC of serum sTREM-1 for predicting death was 0.685 (0.608–0.763; Figure 1E). The ROC curve was obtained in Figure 1F. Serum sTREM-1 had a significant association with death among patients with sepsis in Logistic regression model (P<0.001). The Mann–Whitney U-test showed a significant difference in urine sTREM-1 between the death group and the survival group (U=3020.00, P=0.004).
Values of Serum and Urine sTREM-1 for Predicting AKI
The Spearman Correlation analysis indicated a significant correlation between serum sTREM-1 and serum creatinine during the same period in 238 patients with sepsis (r=0.542, P<0.001). Among 238 patients with sepsis, 93 patients were diagnosed with AKI, and 145 patients were not diagnosed with AKI. The Mann–Whitney U-test showed a significant difference in serum sTREM-1 between patients with AKI and patients without AKI (U=1985.50, P<0.001). The AUC for predicting AKI was 0.803 (0.739–0.866; Figure 1G). The ROC curve was obtained in Figure 1H. When the cut-off value was 485 pg/mL, the sensitivity was 88.4%, and the specificity was 65.8%. Serum sTREM-1 had a significant association with AKI among patients with sepsis in Logistic regression model (P<0.001).
Trend in Serum and Urine sTREM-1 with Disease Progression
Dynamic monitoring of serum and urine sTREM-1 in patients with sepsis showed no significant trend in patients in the survival group. Among 79 patients in the death group, 19 patients took blood and urine samples and completed the detection of sTREM-1 at all time points within 2 weeks after enrollment. Serum sTREM-1 of these 19 patients showed an increased trend (Figure 1I), while urine sTREM-1 showed no significant trend.
Discussion
TREM-1 upregulates the LPS-induced inflammatory response and plays an important role in inflammatory response. In addition to LPS, extracellular bacteria, fungi, viruses, and parasites can all increase TREM-1 expression in phagocytes.6–8 However, TREM-1 expression does not depend on the neutrophils. In non-infectious inflammation such as vasculitis, psoriasis, and ulcerative colitis, although neutrophils are increased, TREM-1 expression is almost undetectable, indicating that TREM-1 is more closely correlated with infectious diseases.9,10
Sepsis is a systemic inflammatory response secondary to infection. To determine diagnostic and predictive values of TREM-1 in sepsis was the main objective of this multi-center prospective clinical study. However, TREM-1 expression is difficult to detect. Fortunately, its soluble product sTREM-1, which is generated and activated after TREM-1 binds to its receptor, can be detected in body fluids. This study included diagnostic and prognostic values of serum and urine sTREM-1 in sepsis and septic shock and their predictive values for clinical prognosis and sepsis-associated AKI.
Serum sTREM-1 detection results were compared between healthy individuals and patients with sepsis. The ROC curve showed an AUC of 0.892 and a specificity of >90%, indicating that serum sTREM-1 distinguishes patients with sepsis from healthy individuals and is a good indicator for sepsis screening. Urine sTREM-1 is almost undetectable in healthy individuals and can only be detected in patients with sepsis, indicating that urine sTREM-1 can also be used as an indicator for sepsis screening. A meta-analysis by Bellos et al, which included 667 neonates in 8 clinical trials, revealed that sTREM-1 can predict neonatal sepsis with a sensitivity of 0.95 and a specificity of 0.87, similar to the results of this study.11
Jedynak et al found in a prospective observational study12 that the AUC of serum sTREM-1 for the diagnosis of septic shock was 0.705. This study showed a significant difference in serum sTREM-1 between the non-septic shock group and the septic shock group, indicating that serum sTREM-1 can reflect the severity of sepsis. In addition, sTREM-1 may be a driving factor in the aggravation of sepsis, and inflammatory storm may be one factor leading to septic shock. At present, the most clinical studies on the diagnostic value of sTREM-1 were based on the Sepsis 2.0 criteria. This study was based on the Sepsis 3.0 criteria. The diagnostic criteria may cause different results, a possibility that requires clinical attention.
Although serum and urine sTREM-1 differed significantly between the death group and the survival group, their predictive values were low, with the AUC of 0.685 and 0.628, respectively. Arízaga et al found in the study on neonatal sepsis that serum sTREM-1 had predictive value for neonatal death from sepsis.13 This study showed that sTREM-1 had a low predictive value for death within 28 days, mainly because the most patients were older and there were factors affecting death. Predicting clinical prognosis solely based on a single indicator proves to be considerably challenging. Consequently, while plasma or urine sTREM-1 may serve as prognostic predictors, their effectiveness is limited and should be interpreted with caution. It is difficult for a single indicator to have a high predictive value for death.
A number of clinical studies have shown that urine sTREM-1 has a high value for the diagnosis of sepsis-associated AKI.14–16 A study conducted by Dai et al suggested that both serum and urine sTREM-1 have diagnostic values for sepsis-associated AKI.14 In this study, the correlation between serum sTREM-1 and sepsis-associated AKI was greater than that between urine sTREM-1 and sepsis-associated AKI; the AUC of serum sTREM-1 was 0.803, which was higher than that of urine sTREM-1 (0.721). This finding is different from that of the existing studies. Serum sTREM-1 and sepsis-associated AKI are correlated for the following reasons: 1) serum sTREM-1 reflects the severity of sepsis-associated inflammatory storm, indicating that inflammatory storm may be a leading cause of AKI; 2) sTREM-1 may be catabolized by kidney, and AKI causes reduced elimination of serum sTREM-1, resulting in the increased serum sTREM-1. Urine sTREM-1 and sepsis-associated AKI are correlated for the following reasons: 1) in addition to the systemic inflammatory response, the local inflammatory and immune responses in kidney may also participate in the AKI process. During the AKI-induced acute tubular necrosis, TREM-1 can be locally produced by inflammatory cells, immune molecules, and oxidative stress recruited by glomerular endothelial cells and tubular epithelial cells, which damages charge barrier of glomerular filtration membrane. This effect leads to the changes in other related downstream pathways and molecular mechanisms, causing further damage to renal tubules;17 2) an increase in serum sTREM-1 results in urine excretion of sTREM-1, and there is a moderate correlation between serum sTREM-1 and urine sTREM-1. In this study, serum sTREM-1 showed an increased trend in 19 death patients, again indicating that it had some correlation with disease prognosis.
High-dose nangibotide (a TREM-1 inhibitor) led to a clinically relevant improvement in SOFA scores over placebo in those with higher sTREM-1 at baseline (≥532 pg/mL).18 The study by Weber et al on TREM-1 knockout mice found that body’s ability to clear virus did not change, but inflammatory cytokines and mortality decreased in knockout mice.19 However, Zhong et al found that injecting mTREM-1/IgG fusion protein to antagonize TREM-1 expression can reduce the severity of fungal keratitis.20
Limitation should be mentioned in this study. The AUC of serum sTREM-1 for diagnosing sepsis was 0.892, for predicting death was 0.685, and for predicting AKI was 0.803. Predictive value for death was relatively low, and more patients will be re-enrolled in the future studies. Increased number of patients will be studied longitudinally to improve the validity of conclusions about sTREM-1 trends over time.
Conclusions
This multi-center prospective clinical study demonstrated that sTREM-1 is a good indicator for the diagnosis of sepsis and septic shock and significantly correlated with clinical prognosis and sepsis-associated AKI in patients with sepsis. Diagnostic and predictive values of sTREM-1 may be related to inflammatory storm mediated by TREM-1. Further mechanism explanation in combination with more clinical studies will benefit for supporting diagnostic and predictive utilities of sTREM-1 in sepsis.
Data Sharing Statement
All data and material are available under the requirement to the corresponding authors.
Ethics Approval and Consent to Participate
This study was approved by the Clinical Ethics Committee of Chinese PLA General Hospital with the approval number S2014-114-02 and was registered on the Clinical Trials Website with the registration number NCT02920736. Prior to this study, written consent forms were required from all participants. This study complies with the Declaration of Helsinki.
Acknowledgments
We appreciate all staff for their continued cooperation and contribution in this study.
Funding
This work was supported by grants from the Beijing Municipal Natural Science Foundation (7222181), the Hainan Clinical Medical Research Center Project (LCYX202201, LCYX202303, LCYX202106), and the Natural Science Foundation of Hainan Province (821QN389). The sponsors had no role in the design, conduct, interpretation, review, approval or control of this article.
Disclosure
All authors declare that they have no conflicts of interest.
References
1. Rhodes A, Evans LE, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 2017;43(3):304–377. doi:10.1007/s00134-017-4683-6
2. Cecconi M, Evans L, Levy M, Rhodes A. Sepsis and septic shock. Lancet. 2018;392(10141):75–87. doi:10.1016/S0140-6736(18)30696-2
3. Bouchon A, Facchetti F, Weigand MA, Colonna M. TREM-1 amplifies inflammation and is a crucial mediator of septic shock. Nature. 2001;410(6832):1103–1107. doi:10.1038/35074114
4. Gómez-Piña V, Martínez E, Fernández-Ruíz I, et al. Role of MMPs in orchestrating inflammatory response in human monocytes via a TREM-1-PI3K-NF-κB pathway. J Leukoc Biol. 2012;91(6):933–945. doi:10.1189/jlb.0711340
5. Su L, Liu D, Chai W, Liu D, Long Y. Role of sTREM-1 in predicting mortality of infection: a systematic review and meta-analysis. BMJ Open. 2016;6(5):e010314. doi:10.1136/bmjopen-2015-010314
6. Chin VK, Asyran A, Zakaria ZA, et al. TREM-1 modulation produces positive outcome on the histopathology and cytokines release profile of Plasmodium berghei-infected mice. J Parasit Dis. 2019;43(1):139–153. doi:10.1007/s12639-018-1070-3
7. Carrasco K, Boufenzer A, Jolly L, et al. TREM-1 multimerization is essential for its activation on monocytes and neutrophils. Cell Mol Immunol. 2019;16(5):460–472. doi:10.1038/s41423-018-0003-5
8. de Oliveira Matos A, Dos Santos Dantas PH, Figueira Marques Silva-Sales M, Sales-Campos H. The role of the triggering receptor expressed on myeloid cells-1 (TREM-1) in non-bacterial infections. Crit Rev Microbiol. 2020;46(3):237–252. doi:10.1080/1040841X.2020.1751060
9. Dantas P, Matos AO, da Silva Filho E, Silva-Sales M, Sales-Campos H. Triggering receptor expressed on myeloid cells-1 (TREM-1) as a therapeutic target in infectious and noninfectious disease: a critical review. Int Rev Immunol. 2020;39(4):188–202. doi:10.1080/08830185.2020.1762597
10. Ajmani S, Singh H, Chaturvedi S, et al. Utility of neutrophil CD64 and serum TREM-1 in distinguishing bacterial infection from disease flare in SLE and ANCA-associated vasculitis. Clin Rheumatol. 2019;38(4):997–1005. doi:10.1007/s10067-018-4334-5
11. Bellos I, Fitrou G, Daskalakis G, Thomakos N, Papantoniou N, Pergialiotis V. Soluble TREM-1 as a predictive factor of neonatal sepsis: a meta-analysis. Inflamm Res. 2018;67(7):571–578. doi:10.1007/s00011-018-1149-4
12. Jedynak M, Siemiatkowski A, Milewski R, Mroczko B, Szmitkowski M. Diagnostic effectiveness of soluble triggering receptor expressed on myeloid cells-1 in sepsis, severe sepsis and septic shock. Arch Med Sci. 2019;15(3):713–721. doi:10.5114/aoms.2018.73090
13. Arízaga-Ballesteros V, Alcorta-García MR, Lázaro-Martínez LC, et al. Can sTREM-1 predict septic shock & death in late-onset neonatal sepsis? A pilot study. Int J Infect Dis. 2015;30:27–32. doi:10.1016/j.ijid.2014.10.013
14. Dai X, Zeng Z, Fu C, Zhang S, Cai Y, Chen Z. Diagnostic value of neutrophil gelatinase-associated lipocalin, cystatin C, and soluble triggering receptor expressed on myeloid cells-1 in critically ill patients with sepsis-associated acute kidney injury. Crit Care. 2015;19(1):223. doi:10.1186/s13054-015-0941-6
15. Su LX, Feng L, Zhang J, et al. Diagnostic value of urine sTREM-1 for sepsis and relevant acute kidney injuries: a prospective study. Crit Care. 2011;15(5):R250. doi:10.1186/cc10508
16. Campanholle G, Mittelsteadt K, Nakagawa S, et al. TLR-2/TLR-4 TREM-1 signaling pathway is dispensable in inflammatory myeloid cells during sterile kidney injury. PLoS One. 2013;8(7):e68640. doi:10.1371/journal.pone.0068640
17. Su L, Xie L, Liu D. Urine sTREM-1 may be a valuable biomarker in diagnosis and prognosis of sepsis-associated acute kidney injury. Crit Care. 2015;19(1):281. doi:10.1186/s13054-015-0998-2
18. François B, Lambden S, Fivez T, et al. Prospective evaluation of the efficacy, safety, and optimal biomarker enrichment strategy for nangibotide, a TREM-1 inhibitor, in patients with septic shock (ASTONISH): a double-blind, randomised, controlled, phase 2b trial. Lancet Respir Med. 2023;11(10):894–904. doi:10.1016/S2213-2600(23)00158-3
19. Weber B, Schuster S, Zysset D, et al. TREM-1 deficiency can attenuate disease severity without affecting pathogen clearance. PLoS Pathog. 2014;10(1):e1003900. doi:10.1371/journal.ppat.1003900
20. Zhong J, Huang W, Deng Q, et al. Inhibition of TREM-1 and Dectin-1 alleviates the severity of fungal keratitis by modulating innate immune responses. PLoS One. 2016;11(3):e0150114. doi:10.1371/journal.pone.0150114
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Correlation and Prognostic Assessment of Low T3 Syndrome and Norepinephrine Dosage for Patients with Sepsis: A Retrospective Single-Center (Cohort) Study
Zhang J, Fu S, Liu F, Wan J, Wu S, Jiang G, Tao W, Zhou W, Qian K
International Journal of General Medicine 2022, 15:4837-4847
Published Date: 10 May 2022
A Predictive Model Based on Inflammatory and Coagulation Indicators for Sepsis-Induced Acute Kidney Injury
Xin Q, Xie T, Chen R, Zhang X, Tong Y, Wang H, Wang S, Liu C, Zhang J
Journal of Inflammation Research 2022, 15:4561-4571
Published Date: 11 August 2022
Impaired Circulating Antibody-Secreting Cells Generation Predicts the Dismal Outcome in the Elderly Septic Shock Patients
Xu H, Li T, Zhang X, Li H, Lv D, Wang Y, Huo F, Bai J, Wang C
Journal of Inflammation Research 2022, 15:5293-5308
Published Date: 13 September 2022
The Sphingosine Kinase 2 Inhibitor Opaganib Protects Against Acute Kidney Injury in Mice
Maines LW, Green CL, Keller SN, Fitzpatrick LR, Smith CD
International Journal of Nephrology and Renovascular Disease 2022, 15:323-334
Published Date: 17 November 2022
Integrated Analysis Identified TGFBI as a Biomarker of Disease Severity and Prognosis Correlated with Immune Infiltrates in Patients with Sepsis
Shi M, Wei Y, Guo R, Luo F
Journal of Inflammation Research 2024, 17:2285-2298
Published Date: 15 April 2024