")
Back to Journals » Journal of Inflammation Research » Volume 17
Diagnostic and Prognostic Value of Soluble Triggering Receptor Expressed on Myeloid Cells-1 (sTREM-1) for Septic Cardiomyopathy
Authors Yu J, Chen Y , Pan X, Chen J, Mai Z, Zhang Y, Wang X , Zhou G, Bukhari SA, Ma D , Deng L
Received 7 June 2024
Accepted for publication 24 October 2024
Published 29 October 2024 Volume 2024:17 Pages 7869—7879
DOI https://doi.org/10.2147/JIR.S481792
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Ning Quan
Jiamin Yu,1 Yongxia Chen,1 Xiaoyan Pan,1 Ji Chen,1 Zhenhua Mai,1 Yuanli Zhang,1 Xiaoyan Wang,2– 4 Gaosheng Zhou,5 Sayed Adam Bukhari,6 Daqing Ma,6,7 Liehua Deng1
1Department of Critical Care Medicine, Affiliated Hospital of Guangdong Medical University, Zhanjiang, 524000, People’s Republic of China; 2Doctoral Scientific Research Center, Lianjiang People’s Hospital, Zhanjiang, 524400, People’s Republic of China; 3Affiliated Lianjiang People’s Hospital, Guangdong Medical University, Zhanjiang, 524400, People’s Republic of China; 4Laboratory of Southern Marine Science and Engineering, Zhanjiang, 524023, People’s Republic of China; 5Department of Critical Care Medicine, The First College of Clinical Medical Science, China Three Gorges University, Yichang Central People’s Hospital, Yichang, Hubei, 443003, People’s Republic of China; 6Division of Anaesthetics, Pain Medicine & Intensive Care, Department of Surgery and Cancer, Faculty of Medicine, Imperial College London, Chelsea and Westminster Hospital, London, SW10 9NH, UK; 7Perioperative and Systems Medicine Laboratory, The Children’s Hospital, Zhejiang University School of Medicine, National Clinical Research Center for Child Health, Hangzhou, People’s Republic of China
Correspondence: Liehua Deng, Email [email protected]
Purpose: The early diagnosis of septic cardiomyopathy remains a challenge. The present work aims to evaluate the diagnostic and prognostic value of plasma soluble triggering receptor expressed on myeloid cells-1 (sTREM-1) levels in septic cardiomyopathy when compared with traditional myocardial biomarkers.
Methods: In the 143 sepsis enrolled patients, 67 and 76 patients were classified as non-septic cardiomyopathy and septic cardiomyopathy, respectively. Their blood samples were harvested up to 14th day after hospital admission for measurements of sTREM-1 and other biomarkers, such as N-terminal pronatriuretic peptide (NT-proBNP), highly sensitive troponin (TNT-HS), myoglobin (MYO), creatine kinase isoenzyme (CK-MB), etc. All the data were collected at 8:00 a.m. The area under the receiver operating characteristic curve was obtained to assess the diagnostic accuracy of those biomarkers. The Log rank test was utilized to evaluate the prognostic value of sTREM-1 on septic cardiomyopathy.
Results: Circulating sTREM-1 showed a high specificity (88.1%) and moderate sensitivity (64.5%) to distinguish patients with septic cardiomyopathy in the 143 septic patients. The diagnostic efficiency of sTREM-1 was higher than inflammatory biomarkers and traditional myocardial markers. Logistic regression revealed that plasma sTREM-1 was an independent predictor of septic cardiomyopathy. Furthermore, in the whole septic cardiomyopathy cohorts, the sTREM-1 levels in the non-survivors were significantly higher than those of survivors during ICU stay. In addition, the left ventricular systolic dysfunction had a high odds ratio (3.968) to predict 90-day mortality in septic patients with cardiomyopathy.
Conclusion: High plasma sTREM-1 level may be a diagnostic marker in predicting ICU poor outcome of patients with septic cardiomyopathy.
Keywords: sepsis, septic cardiomyopathy, diagnosis, sTREM-1
Introduction
Sepsis is a life-threatening condition with organ dysfunction including septic cardiomyopathy (SCM) induced by an excessive host response to infection.1 Septic cardiomyopathy is common in severe sepsis and septic shock patients. SCM is characterized by reversible systolic and/or diastolic left ventricular (LV) dysfunction and/or right ventricular dysfunction.2 Approximately, 20–65% of patients with sepsis developed septic cardiomyopathy.3 Patients with septic cardiomyopathy have significantly higher mortality (70%) compared with septic patients without septic cardiomyopathy (20%).4,5 The mortality of those patients was reported to be two to three times higher when compared with those with septic shock alone in adult patients.6 Indeed, a high mortality rate (higher than 80%) was documented in patients with sepsis who had severe myocardial dysfunction.3 However, septic cardiomyopathy is reversible at an early stage, and early diagnosis and intervention of septic cardiomyopathy in sepsis patients may reduce mortality.7 In sepsis, elevated BNP and troponin is more reflective general critical illness8,9 rather than SCM. The conventional myocardial markers in identifying patients suspected to have septic cardiomyopathy is limited owing to the lack of specificity. Therefore, it remains a challenging and yet an urgent need to explore better diagnostic and/or prognostic markers.
Triggering receptor expressed on myeloid cells-1 (TREM-1), a member of immunoglobulin superfamily, is mainly expressed on the cell surfaces of neutrophils, macrophages and mature monocytes. Until now, the two isoforms of the receptor, membrane-bound TREM-1 (mTREM-1) and soluble TREM-1 (sTREM-1) forms have been largely studied in sepsis.10,11 mTREM-1 forms to be oligomers, which lead to downstream signaling activation and proinflammatory mediator release while sTREM-1 has only the Ig-like domain that plays a vital role in antigen recognition, making it to be a potential biomarker for disease diagnosis use.12
Recent studies identified sTREM-1 as an inflammatory marker or a prognostic marker of respiratory infections. For example, serum sTREM-1 levels were high in elderly patients with ventilator-associated pneumonia, and its levels were correlated with the severity of disease.13–15 In addition, sTREM-1 was reported to be valuable both in the diagnosis of acute bacterial infection-induced diarrhea and acute appendicitis in children.16,17 Furthermore, sTREM-1 showed diagnostic and prognostic values in both children and adults with sepsis.18,19 However, A meta-analysis demonstrated that sTREM-1 can be measurable in any kinds of sepsis patients on admission but its usefulness is not yet defined.20 In addition, sTREM-1 was also associated with development of acute and chronic cardiovascular diseases, such as atherosclerosis and acute myocardial infarction (AMI)21 and its levels were strongly related with the severity of AMI and cardiac dysfunction during sepsis.22,23 It was found to be significantly associated with sepsis induced ventricular dysfunction in our previous animal study.24 Therefore, sTREM-1 for diagnostic and/or prognostic use needs to be verified further. The aim of the present study was to access the usefulness of plasma sTREM-1 when compared with traditional myocardial markers in the diagnosis and/or prognosis of septic cardiomyopathy in patients with sepsis.
Methods
Study Design and Patient Population
This prospective cohort study protocol was reviewed and approved by the Ethics Committee of Affiliated Hospital of Guangdong Medical University (No. PJ2020-081). The study was then conducted in accordance with the Declaration of Helsinki (as revised in 2013). According to the guideline of 2016 Sepsis −3,25 67 sepsis patients without septic cardiomyopathy (non-septic cardiomyopathy group) and 76 sepsis patients with septic cardiomyopathy (septic cardiomyopathy group) were recruited to the Department of Critical Care Medicine of the Affiliated Hospital of Guangdong Medical University, Zhanjiang, China, between October 2020 to February 2022. All patients or their families agreed to participate in this study and their signed written informed consent forms were obtained before recruitment. The inclusion criteria for the study were as follows: aged 18–75 years old and their diagnosis complied with the 2016 Sepsis 3.0 standard. Exclusion criteria were set as follows: patients with valvulopathy, chronic heart and renal failure, patients with acute coronary syndromes and/or hypertensive heart disease, non-infectious shock, neutropenia, HIV infection, treatment with corticosteroids or immunosuppressive drugs within the last month, or and patients stay in ICU less than 24 hours. The patients were treated according to the sepsis and septic shock guidelines.
Data Collection
Demographic and disease data of patients included age, gender, infection sites, microorganisms, liver and kidney functions, coagulation indicators, PaO2, lactate level acute physiologic assessment and chronic health evaluation (APACHE) II scores, and sequential organ failure assessment (SOFA) scores, Procalcitonin (PCT), complete blood count, N-Terminal pronatriuretic peptide (NT-proBNP), Highly sensitive troponin (TNT-HS), Myoglobin (MYO), Creatine kinase isoenzyme (CK-MB). These data recorded on post-admission day 1, 3, 7, and 14 were collected. Plasma was harvested at post-admission day 1, 3, 7, and 14 and plasma IL-1β, IL-18, and sTREM-1 were quantified with ELISA kits following the manufacturer’s instructions (Jianglai, Shanghai, China). All the data was collected at 8:00 a.m.
Echocardiography
Transthoracic echocardiography was done at post-admission day 1, 3, 7, and 14 with an ultrasound system (SONIMAGE HS1, KONICA MINOLTA China, Shanghai, China). To reduce the heterogeneity, echocardiograms were recorded by the same senior intensivist. Left ventricular ejection fraction (LVEF) was calculated using the Teichholz correction formula from parasternal long-axis views. Left ventricular systolic dysfunction was grouped into two categories: mild systolic dysfunction with LVEF less than 55% and severe dysfunction with LV systolic less than 45%.26–28 Mitral inflow was obtained via pulse-wave Doppler echocardiography using the sample volume between mitral leaflet tips during diastole (E). Mitral annular tissue velocity (e′) was obtained using tissue Doppler imaging with the sample volume on the septal area of the mitral annulus during diastole. E/e′ >14 or/and e′ <10mm was used to judge to have left ventricular diastolic dysfunction.29 The right ventricular function was assessed at end expiration in a multimodal fashion as per American Society of Echocardiography guidelines (tricuspid annular plane systolic excursion TAPSE, lateral tricuspid annular velocity s′. Right ventricular area changes FAC),30 and RVFAC% <35% or/and TAPSE <17mm or/and s′ <10mm were classified as right ventricular systolic dysfunction.29 Tei index is a numeric value derived from the sum of isovolumetric contraction and isovolumetric relaxation divided by total ejection time (Tei=ICT+IRT/ET), which is independent of heart rate, preload and afterload making Tei index a facile parameter to assess overall myocardial performance.31 Tei index >0.48 was defined as myocardial performance deterioration.32
Diagnostic Criteria
Septic cardiomyopathy was diagnosed when patient met criteria 1 or/and criteria 2 of the definition:26–29 1. Severe heart dysfunction with LVEF <45%; 2. At least two of the following: (1) LVEF <55%; (2) Left ventricular diastolic dysfunction (E/e′>14 or/and e′<10 mm); (3) Right ventricular systolic dysfunction (RVFAC% <35% or/and TAPSE <17mm or/and s′ <10mm); (4)Tei index >0.48.
Statistical Analysis
The sample size was calculated based on our preliminary data, which showed that sTREM-1 was 52.3pg/mL and 118.7pg/mL in SCM patients (n =10) and non-SCM patients at admission (n =10), respectively. To detect the significance between the two groups with a desired power of 80% and type I error set at 0.05, then minimal n=49/group was required. All data were analyzed with SPSS 25.0 software (IBM Corp, Armonk, NY, USA) and MedCalc 20.0 software (MedCalc Software Ltd, Ostend, Belgium). Quantitative data with normal distributions are expressed as means ± standard deviations (SD); otherwise, expressed as the median (interquartile ranges). Data were then analysed with Student’s t-test for group comparison, the Mann–Whitney (MW) test of the independent samples for inter-group comparison, or the related sample Wilcoxon test was used for intra-group comparison as appropriate. Proportions and the differences in proportions between groups were compared using a chi-square test. Receiver operating characteristics (ROC) curves was used to evaluate diagnostic value of the biomarkers and the diagnostic efficacy of biomarkers were compared by z-test. Besides, compared the multiple mortality of patients using the Log rank test. Multivariate logistic regression analysis was used to further identify the independent predictor of septic cardiomyopathy and the 90 day mortality of septic cardiomyopathy patients. A statistical significance was set when a p value less than 0.05.
Results
Baseline Characteristics
The routine laboratory measurements and clinical parameters of patients with septic cardiomyopathy (n = 76) and non-septic cardiomyopathy (n = 67) are presented in Table 1. No significant difference was found in gender, age, infection site, comorbidities, pathogenic microorganism, acute physiology and chronic health evaluation II (APACHE II) score, sequential organ failure assessment (SOFA) score, blood creatinine, AST, ALT, lactate level, oxygenation index, SAP, DAP, and MAP between the two groups (P > 0.05). The septic cardiomyopathy group had higher vasopressors usage than that of the non-septic cardiomyopathy group (P =0.021). The respiratory system infection was the most common in whole study population (n = 67, 46.9%) (Table 1).
 |
Table 1 Clinical Characteristics of Patients on the Day of Admission to ICU |
Laboratory Biomarkers
Plasma IL-18 and IL-1β in the septic cardiomyopathy group were considerably increased than those in the non-septic cardiomyopathy group on the 1st and 3rd days of admission (P < 0.005) (Figure 1A and B). At the early stage of admission, PCT in the septic cardiomyopathy group was higher than those in the non-septic cardiomyopathy group (P < 0.05) (Figure 1C).The plasma sTREM-1 level in the septic cardiomyopathy group was significantly increased when compared with those in the non-septic cardiomyopathy group at admission day 1 (median 263.5 vs 82.3 pg/mL, P < 0.001), 3 (median 230.2 vs 75.8 pg/mL, P < 0.001), 7 (median 167.3 vs 84.7 pg/mL, P < 0.001), and 14 (median 118.2 vs 66.6 pg/mL, P < 0.005) (Figure 1D). However, there were no significant differences among the MYO, CK-MB, TNT-HS, and NT-proBNP concentration between the non-septic cardiomyopathy and septic cardiomyopathy patients (Supplementary Figure S1A–D).
 |
Figure 1 Changes in Laboratory biomarkers in patients with Non-SCM and SCM after admission to ICU. (A) IL-18. (B) IL-1β. (C) PCT. (D) sTREM-1. ** P<0.01, *** P<0.005, **** P<0.001. ns indicates no statistical significance. Abbreviations: IL-18, Interleukin18; IL-1β, Interleukin-1β; PCT, Procalcitonin; sTREM-1, soluble myeloid cells trigger receptor-1. |
Cardiac Function
Compared both groups, the septic cardiomyopathy group demonstrated a rather low LVEF on admission day 1 (median 63.1% vs 55.8%, P < 0.001) and day 3 (median 62.3% vs 56.3%, P < 0.001) (Figure 2A). We had three indicators (RVFAC%, TAPSE, s’) that reflect right ventricular systolic dysfunction and they were significant differences between the non-septic cardiomyopathy and septic cardiomyopathy groups. RVFAC% was lower in patients with septic cardiomyopathy than those with non-septic cardiomyopathy (RVFAC%: day 1: 47.7% vs 38.3%, P < 0.001; day 3: 47.5% vs 40.3%, P < 0.001). The levels of TAPSE in the non-septic cardiomyopathy group were higher than those in the septic cardiomyopathy group (TAPSE: day 1: 19.7mm vs 16.2mm, P < 0.001; day 3: 19.6mm vs 16.6mm, P < 0.001; day 7: 18.8mm vs 17.8mm, P = 0.009; day 14: 19.8mm vs 17.9mm, P = 0.001). At the same time, s’ was lower in patients with septic cardiomyopathy (s’: day 1: 14.2cm/s vs 13.0cm/s, P = 0.009; day 3: 14.1cm/s vs 13.2cm/s, P = 0.001) (Figure 2B–D). Furthermore, the Tei index of patients with septic cardiomyopathy was significantly higher than that of the non-septic cardiomyopathy group on admission day 1 (median 0.41 vs 0.48, P < 0.001), 3 (median 0.41 vs 0.47, P < 0.001), and 7 (median 0.42 vs 0.43, P < 0.001) (Figure 2E). Besides, on the day of admission, e′ in the septic cardiomyopathy group were lower than those in the non-septic cardiomyopathy group (median 9.1cm/s vs 8.4cm/s,P < 0.05) (Figure 2F). Only E/ e′ showed no significant differences between the two groups (Figure 2G).
 |
Figure 2 Changes in echocardiography in patients with Non-SCM and SCM after admission to ICU. (A) EF. (B) RVFAC. (C) TAPSE. (D) s′. (E) Tei Index. (F) e′. (G) E/e′. Tei Index=(ICT+IRT)/ET. * P<0.05, ** P<0.01, *** P<0.005, **** P<0.001. ns indicates no statistical significance. Abbreviations: e′, mitral annulus early diastolic velocity; E, mitral annulus diastolic blood flow velocity; EF, ejection fraction; ET, ejection time; ICT, isovolumetric contraction time; IRT, isovolumic relaxation time; RVFAC, right ventricular fractional area changes; s′, tricuspid annular peak systolic velocity; TAPSE, tricuspid annular plane systolic excursion. |
Diagnosis of Septic Cardiomyopathy
We analyzed all patients’ biomarker concentration on the day they were admitted. The receiver operating characteristic (ROC) curve were established to assess septic cardiomyopathy with serum sTREM-1 levels, inflammatory biomarkers and traditional myocardial markers. The AUCs of sTREM-1, TNT-HS, CK-MB, MYO and NT-proBNP were 0.824, 0.547, 0.556, 0.545 and 0.514, respectively (Figure 3A). The AUCs of PCT, IL-1β and IL-18 were 0.630, 0.674, and 0.573, respectively (Figure 3B). The optimal sTREM-1 cut-off value to predict septic cardiomyopathy was 172.6 pg/mL, which had 64.5% sensitivity and 88.1% specificity (P < 0.0001). Moreover, The AUCs of sTREM-1 and other biomarkers were compared by Z-test, the diagnostic efficacy of sTREM-1 of septic cardiomyopathy were superior to traditional myocardial markers and inflammatory biomarkers (Table S1). When analyzed separately for each category of heart dysfunction, sTREM-1 levels also has certain diagnostic value for left ventricular systolic dysfunction (P < 0.001), right ventricular systolic dysfunction (P < 0.001) and left ventricular diastolic dysfunction (P = 0.0419) (Figure 3C). Multivariate logistic regression analysis demonstrated that serum sTREM-1 level was an independent predictor of septic cardiomyopathy with an odds ratio (OR) of 1.009 (95% CI 1.005–1.012). Similar to the sTREM-1, higher IL-1β level had a significant detrimental effect on sepsis patient (OR 1.016, 95% CI 1.003–1.030). Meanwhile, septic shock (OR 2.634, 95% CI 1.015–6.833) was significantly associated with an increased risk of septic cardiomyopathy (Table 2).
 |
Table 2 Logistics Analysis of Septic Cardiomyopathy Events |
 |
Figure 3 (A) ROC curves of soluble biomarkers for diagnosing septic cardiomyopathy. CK-MB, creatine kinase isoenzyme; (B) ROC curves of infection indicators and inflammatory biomarkers for diagnosing septic cardiomyopathy. (C) ROC curves of sTREM-1 for diagnosing left ventricular systolic dysfunction (LVSD), right ventricular systolic dysfunction (RVSD) and left ventricular diastolic dysfunction (LVDD). P<0.05 means statistically significant. Abbreviations: MYO, myoglobin; NT-proBNP, N-Terminal pronatriuretic peptide; sTREM-1, soluble myeloid cells trigger receptor-1; TNT-HS, highly sensitive troponin. |
Mortality of Patients with or Without Cardiomyopathy
To study the differences in mortality between patients with non-septic cardiomyopathy and those with septic cardiomyopathy, ICU mortality, 28-day mortality and 90-day mortality of the patients were analyzed by log-rank, and the Kaplan-Meier survival curve was established. Log rank tests showed no difference between 28-day and 90-day mortality between the two group, but the ICU mortality rate in the septic cardiomyopathy group was significantly higher than that in the non-septic cardiomyopathy group (P < 0.05) (Figure 4A–C). To evaluate the association between sTREM-1 levels and ICU mortality in the septic cardiomyopathy patients, the plasma sTREM-1 concentrations of patients with septic cardiomyopathy were divided into four segments according to interquartile range. These are Quartile 1: < 116.1 pg/mL, Quartile 2: 116.1–263.5 pg/mL, Quartile 3: 263.5–515.7 pg/mL and Quartile 4: > 515.7 pg/mL. The total cohort ICU mortality was increased with the highest-level sTREM-1 concentration (P < 0.05) (Figure 5). However, multivariate analysis showed that the left ventricular systolic dysfunction remained an independent predictor of mortality at 90 days (Left ventricular systolic dysfunction: OR = 3.968, 95% CI 1.068–14.751, P < 0.05) (Table 3).
 |
Table 3 Logistics Analysis of 90-Day Mortality in Patient with SCM |
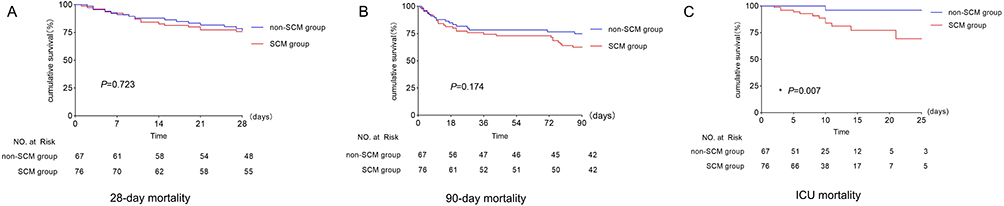 |
Figure 4 Mortality of non-septic cardiomyopathy and septic cardiomyopathy patient. (A) Cumulative survival of 28-day mortality. (B) Cumulative survival of 90-day mortality. (C) Cumulative survival of ICU mortality. |
 |
Figure 5 Cumulative survival of ICU mortality by sTREM-1 concentration. (Quartile 1: < 116.1 pg/mL, Quartile 2: 116.1–263.5 pg/mL, Quartile 3: 263.5–515.7 pg/mL, Quartile 4: > 515.7 pg/mL). ns means no statistical significance compare with the first quartile. *P<0.05 means statistical significance compare with the first quartile. |
Discussion
Our study indicated that the high level of sTREM-1 is a sensitive biomarker to distinguish between patients with or with cardiomyopathy and it is associated with high mortality in septic patients with cardiomyopathy. Our work suggests that sTREM-1 may be diagnostic and/or prognostic marker of septic cardiomyopathy. The utility of sTREM-1 integrated with echocardiography may be a useful and better approach for the diagnosis and prognosis of septic cardiomyopathy clinically.
Septic cardiomyopathy is a common complication following sepsis that exacerbates poor prognosis.33 Sepsis-induced myocardial dysfunction can be manifested as left ventricular systolic dysfunction, left ventricular diastolic dysfunction and right ventricular dysfunction, alone or in combination. The diagnostic criteria for septic cardiomyopathy currently are mainly based on LVEF. However, there is no consensus regarding the cut-off value for LVEF for patients with or without septic cardiomyopathy. For example, LVEF <45% was used in some studies as the diagnostic criterion while others used LVEF <50%.2,34,35 Our diagnostic criteria, based on previous studies and American Society of Echocardiography guidelines, included systolic and/or diastolic left ventricular dysfunction and/or right ventricular dysfunction.
Although transthoracic echocardiography has advantages in assessing myocardial dysfunction, complicated data and procedures limit its wide use in practice. Laboratory biomarkers for the diagnosis of septic cardiomyopathy are, therefore, urgently needed. Elevated plasma troponin in patients with sepsis was associated with left ventricular systolic dysfunction and worse prognosis in patients with sepsis.36 The peak troponin also correlates with SCM diagnosis.37 Besides, Kada et al38 reported that BNP may predict clinical outcomes and myocardial dysfunction. However, the causes of increased troponin and BNP levels in severe sepsis and septic shock are multifactorial. Therefore, troponin and BNP lack specificity in predicting septic cardiomyopathy.39 sTREM-1 emerges as a useful diagnostic and prognostic marker of septic cardiomyopathy. When LVEF <50% and cardiac function index <4.1 L/min as diagnostic criteria were used, the study of 84 patients with sepsis showed that sTREM-1 was negatively correlated with LVEF, CFI, CI, GEF and dP/dt Max.40 In our prospective observational study, 53.1% of patients had cardiac function dysfunction in sepsis. Additionally, we measured plasma sTREM-1 concentrations and similar to previous animal experiments,40 sTREM-1 levels were significantly higher in the septic cardiomyopathy patients than the non-septic cardiomyopathy patients. The multivariable analysis demonstrated that sTREM-1 was an independent predictor of septic cardiomyopathy in patients with sepsis, indicating that sTREM-1 is closely related to the myocardial dysfunction development in sepsis patients. The optimal cut-off points of sTREM-1 for detecting patients with septic cardiomyopathy was 172.6 pg/mL with sensitivity of 64.5% and specificity of 88.1% as reported here. Our study suggests that sTREM-1 level may be promising in identifying sepsis-induced myocardial dysfunction with a moderate risk of missed diagnosis. Interestingly, our data showed that diagnostic value of sTREM-1 for systolic dysfunction was greater than that of diastolic function. When the relationship between sTREM-1 level and ICU mortality was analyzed, sTREM-1 was an independent predictor. Liang et al41 also reported that hospital mortality was higher in the septic cardiomyopathy patients compared with the non- septic cardiomyopathy patients which may be related to the uncontrollable inflammatory storms in the late stages of septic cardiomyopathy.42
The novelty of the current work was that sTREM-1 in diagnosing septic cardiomyopathy integrated with systolic and/or diastolic left ventricular dysfunction and/or right ventricular dysfunction while previous studies were mainly focused on the left ventricular systolic dysfunction. The data reported in the present study are more sensitive and reliable due to the more rigorous transthoracic echocardiography monitoring. The limitation of this study is that the sample size is relatively small and more studies are needed to further clarify the usefulness of sTREM-1 in predicting septic cardiomyopathy development and its associated outcome. Second, we did not measure TNF-a, another key inflammatory cytokine. Third, we did not track long-term survival in the SCM and SCM groups. Despite these limitations, we still believe that our findings advance potential laboratory markers for diagnosing SCM.
Conclusion
In summary, the elevated sTREM-1 level on admission was an independent predictor of septic cardiomyopathy and ICU mortality. However, caution should be taken until further studied data are available.
Abbreviations
CK-MB, Creatine kinase isoenzyme; ET, Ejection Time; FAC, Right Ventricular Area Changes; ICU, Intensive Care Unit; IL-1β, Interleukin-1β; IL-18, Interleukin18; ICT, Isovolumetric Contraction Time; IRT, Isovolumetric Relaxation Time; LVEF, Left Ventricular Ejection Fraction; MYO, Myoglobin; NT-proBNP, N-Terminal pronatriuretic peptide; PCT, Procalcitonin; SCM, Septic Cardiomyopathy; sTREM-1, Soluble Triggering Receptor Expressed on Myeloid Cells-1; TNT-HS, Highly sensitive troponin; TAPSE, Tricuspid Annular Plane Systolic Excursion; WBC, White blood cells.
Data Sharing Statement
All data are available in the manuscript. Data will be made available immediately following publication, with no anticipated end date, to achieve the aims specified in the approved proposal. Proposals should be directed to Liehua Deng [email protected].
Ethical Approval and Consent to Participate
Before including the first patient, the trial protocol was reviewed and approved by the Ethics Committee of Affiliated Hospital of Guangdong Medical University (No. PJ2020-081). The study was then conducted in accordance with the Declaration of Helsinki (as revised in 2013).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China under grant No. 82172148 and 81974298.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Coopersmith CM, De Backer D, Deutschman CS, et al. Surviving sepsis campaign: research priorities for sepsis and septic shock. Intens Care Med. 2018;44:1400–1426.
2. Boissier F, Aissaoui N. Septic cardiomyopathy: diagnosis and management. J Intensive Med. 2022;2:8–16. doi:10.1016/j.jointm.2021.11.004
3. Bréchot N, Hajage D, Kimmoun A, et al. Venoarterial extracorporeal membrane oxygenation to rescue sepsis-induced cardiogenic shock: a retrospective, multicentre, international cohort study. Lancet. 2020;396:545–552. doi:10.1016/S0140-6736(20)30733-9
4. Jesús B, Arturo M, Víctor S, et al. Incidence, organ dysfunction and mortality in severe sepsis: a Spanish multicentre study. Crit Care. 2008;12:1–4.
5. Joseph EP, Margaret MP, Charles N, et al. Septic shock in humans: advances in the understanding of pathogenesis, cardiovascular dysfunction, and therapy. Ann Intern Med. 1990;113:227–242.
6. Ling RR, Ramanathan K, Poon WH, et al. Venoarterial extracorporeal membrane oxygenation as mechanical circulatory support in adult septic shock: a systematic review and meta-analysis with individual participant data meta-regression analysis. Crit Care. 2021;25. doi:10.1186/s13054-021-03668-5
7. Lin H, Wang W, Lee M, Meng Q, Ren H. Current status of septic cardiomyopathy: basic science and clinical progress. Front Pharmacol. 2020;11. doi:10.3389/fphar.2020.00210
8. John P, Demosthenes M, Maria M, Eleni P, Paris Z, Epaminondas Z. New insights into the mechanisms involved in B-type natriuretic peptide elevation and its prognostic value in septic patients. Crit Care. 2014;18:1–3.
9. Marlies O, Salma A, Emma T, et al. Cardiac troponin release is associated with biomarkers of inflammation and ventricular dilatation during critical illness. Shock. 2016;47:702–708.
10. de Oliveira Matos A, Dos Santos Dantas PH, Figueira Marques Silva-Sales M, Sales-Campos H. The role of the triggering receptor expressed on myeloid cells-1 (TREM-1) in non-bacterial infections. Crit Rev Microbiol. 2020;46:237–252. doi:10.1080/1040841X.2020.1751060
11. Dantas PHDS, Matos ADO, Da Silva Filho E, Silva-Sales M, Sales-Campos H. Triggering receptor expressed on myeloid cells-1 (TREM-1) as a therapeutic target in infectious and noninfectious disease: a critical review. Int Rev Immunol. 2020;39:188–202. doi:10.1080/08830185.2020.1762597
12. Matos AO, Dantas P, Silva-Sales M, Sales-Campos H. TREM-1 isoforms in bacterial infections: to immune modulation and beyond. Crit Rev Microbiol. 2021;47:290–306. doi:10.1080/1040841X.2021.1878106
13. Fang C, Mao Y, Jiang M, Yin W. Serum sTREM-1 and CXCL-16 levels in children with Mycoplasma pneumoniae Pneumonia and their diagnostic value. Evid Based Complementary Altern Med. 2021;2021:1–7.
14. Liu Y, Tian L, You J, Li Y. The predictive value of postoperative C-reactive protein (CRP), procalcitonin (PCT) and triggering receptor expressed on myeloid cells 1 (TREM-1) for the early detection of pulmonary infection following laparoscopic general anesthesia for cervical cancer treatment. Ann Palliat Med. 2021;10:4502–4508. doi:10.21037/apm-21-554
15. Wang J, Zhao Y, Pan L, He X, Zhang X. The relationship between the expression of serum IL-18 mRNA, CC16, and sTREM-1 and the severity and prognosis of ventilator-associated pneumonia in elderly patients. Ann Palliat Med. 2021;10:12767–12774. doi:10.21037/apm-21-3511
16. Al-Asy HM, Gamal RM, Albaset AMA, Elsanosy MG, Mabrouk MM. New diagnostic biomarker in acute diarrhea due to bacterial infection in children. Int J Pediatrics Adolesce Med. 2017;4:75–80. doi:10.1016/j.ijpam.2016.12.004
17. Klein TT, Kohn E, Klin B, et al. sTREM-1 as a diagnostic biomarker for acute appendicitis in children. Asian J Surg. 2021;44:1172–1178. doi:10.1016/j.asjsur.2021.02.025
18. Şen S, Kamit F, Işgüder R, et al. Surface TREM-1 as a prognostic biomarker in pediatric sepsis. Indian J Pediatr. 2021;88:134–140. doi:10.1007/s12098-020-03355-3
19. Kung C, Su C, Hsiao S, et al. The prognostic value of serum soluble TREM-1 on outcome in adult patients with sepsis. Diagnostics. 2021;11:1979. doi:10.3390/diagnostics11111979
20. Qin Q, Liang L, Xia Y. Diagnostic and prognostic predictive values of circulating sTREM-1 in sepsis: a meta-analysis. Infect Genet Evol. 2021;96:105074. doi:10.1016/j.meegid.2021.105074
21. Kouassi K, Gunasekar P, Agrawal D, Jadhav G. TREM-1; is it a pivotal target for cardiovascular diseases? J Cardiovasc Dev Dis. 2018;5:45. doi:10.3390/jcdd5030045
22. Boufenzer A, Lemarié J, Simon T, et al. TREM-1 mediates inflammatory injury and cardiac remodeling following myocardial infarction. Circ Res. 2015;116:1772–1782. doi:10.1161/CIRCRESAHA.116.305628
23. Ait-Oufella H, Yu M, Kotti S, et al. Plasma and genetic determinants of soluble TREM-1 and major adverse cardiovascular events in a prospective cohort of acute myocardial infarction patients. Results from the FAST-MI 2010 study. Int J Cardiol. 2021;344:213–219. doi:10.1016/j.ijcard.2021.09.018
24. Zhou G, Ye L, Zhang L, et al. Association of myeloid cells of triggering receptor-1 with left ventricular systolic dysfunction in BALB/c mice with sepsis. Mediators Inflammation. 2014;2014:1–8.
25. Mervyn S, Clifford SD, Christopher Warren S, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). J Am Med Assoc. 2016;315:801–810.
26. Ehrman RR, Sullivan AN, Favot MJ, et al. Pathophysiology, echocardiographic evaluation, biomarker findings, and prognostic implications of septic cardiomyopathy: a review of the literature. Crit Care. 2018;22. doi:10.1186/s13054-018-2043-8
27. Sam RO, Juan NP, Mitsuru M, et al. Outcome prediction in sepsis: speckle tracking echocardiography based assessment of myocardial function. Critical Care. 2014;18:R149. doi:10.1186/cc13987
28. Lang RM, Bierig M, Devereux RB, et al. Recommendations for chamber quantification: a report from the American Society of Echocardiography’s Guidelines and Standards Committee and the chamber quantification writing group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiography. 2005;18:1440–1463. doi:10.1016/j.echo.2005.10.005
29. Hollenberg SM, Singer M. Pathophysiology of sepsis-induced cardiomyopathy. Nat Rev Cardiol. 2021;18:424–434. doi:10.1038/s41569-020-00492-2
30. Rudski LG, Lai WW, Afilalo J, et al. Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography. J Am Soc Echocardiog. 2010;23:685–713. doi:10.1016/j.echo.2010.05.010
31. Goroshi M, Chand D. Myocardial performance index (Tei Index): a simple tool to identify cardiac dysfunction in patients with diabetes mellitus. Indian Heart J. 2016;68:83–87. doi:10.1016/j.ihj.2015.06.022
32. Bennett S, Cubukcu A, Wong CW, et al. The role of the Tei index in assessing for cardiotoxicity from anthracycline chemotherapy: a systematic review. Echo Res Pract. 2021;8:R1–R11. doi:10.1530/ERP-20-0013
33. Wang R, Xu Y, Fang Y, et al. Pathogenetic mechanisms of septic cardiomyopathy. J Cell Physiol. 2022;237:49–58. doi:10.1002/jcp.30527
34. Sato R, Kuriyama A, Takada T, Nasu M, Luthe S. Prevalence and risk factors of sepsis-induced cardiomyopathy: a retrospective cohort study. Medicine. 2016;95:e5031. doi:10.1097/MD.0000000000005031
35. Narváez I, Canabal A, Martín C, et al. Incidence and evolution of sepsis-induced cardiomyopathy in a cohort of patients with sepsis and septic shock. Med Intensiva. 2018;42:283–291. doi:10.1016/j.medin.2017.08.008
36. Maeder M, Fehr T, Rickli H, Ammann P. Sepsis-associated myocardial dysfunction: diagnostic and prognostic impact of cardiac troponins and natriuretic peptides. Chest. 2006;129:1349–1366. doi:10.1378/chest.129.5.1349
37. June-Sung K, Muyeol K, Youn-Jung K, et al. Troponin testing for assessing sepsis-induced myocardial dysfunction in patients with septic shock. J Clin Med. 2019;8:239.
38. Klouche K, Pommet S, Amigues L, et al. Plasma brain natriuretic peptide and troponin levels in severe sepsis and septic shock: relationships with systolic myocardial dysfunction and intensive care unit mortality. J Intensive Care Med. 2014;29:229–237. doi:10.1177/0885066612471621
39. Nabzdyk CS, Couture EJ, Shelton K, Cudemus G, Bittner EA. Sepsis induced cardiomyopathy: pathophysiology and use of mechanical circulatory support for refractory shock. J Crit Care. 2019;54:228–234. doi:10.1016/j.jcrc.2019.09.001
40. Li Z, Zhang E, Hu Y, Liu Y, Chen B. High serum sTREM-1 correlates with myocardial dysfunction and predicts prognosis in septic patients. Am J Med Sci. 2016;351:555–562. doi:10.1016/j.amjms.2016.01.023
41. Liang Y, Zhu Y, Zhang R, Zhang M, Ye X, Wei J. Incidence, prognosis, and risk factors of sepsis-induced cardiomyopathy. World J Clin Cases. 2021;9:9452–9468. doi:10.12998/wjcc.v9.i31.9452
42. Beesley SJ, Weber G, Sarge T, et al. Septic Cardiomyopathy. Crit Care Med. 2018;46:625–634. doi:10.1097/CCM.0000000000002851
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Diagnostic and Prognostic Value of Monocyte Distribution Width in Sepsis
Wu J, Li L, Luo J
Journal of Inflammation Research 2022, 15:4107-4117
Published Date: 20 July 2022
Identification of an Immune-Related Gene Diagnostic Model and Potential Drugs in Sepsis Using Bioinformatics and Pharmacogenomics Approaches
Chen P, Chen J, Ye J, Yang L
Infection and Drug Resistance 2023, 16:5665-5680
Published Date: 28 August 2023
Types of Septic Cardiomyopathy: Prognosis and Influencing Factors - A Clinical Study
Lu NF, Niu HX, Liu AQ, Chen YL, Liu HN, Zhao PH, Shao J, Xi XM
Risk Management and Healthcare Policy 2024, 17:1015-1025
Published Date: 23 April 2024
Novel Identification of CD74 as a Biomarker for Diagnosing and Prognosing Sepsis Patients

Hu K, Shi A, Shu Y, Sudesh S, Ling J, Chen Y, Hua F, Yu S, Zhang J, Yu P
Journal of Inflammation Research 2025, 18:3829-3842
Published Date: 15 March 2025