")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Diagnostic Efficacy of Combined N-Terminal Pro-Brain Natriuretic Peptide (NT-proBNP) and Cardiac Troponin I (cTnI) Testing in Myocardial Injury of Children with Mycoplasma Pneumoniae Pneumonia
Received 24 March 2025
Accepted for publication 14 June 2025
Published 26 June 2025 Volume 2025:18 Pages 3709—3716
DOI https://doi.org/10.2147/JMDH.S527700
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Charles V Pollack
Mei Yang,1 Aili Xuan,1 Guoji Zhu2
1Department of Pediatrics, First Affiliated Hospital of Bengbu Medical University, Anhui, People’s Republic of China; 2Department of Infectious Diseases, Children’s Hospital, Soochow University, Jiangsu, People’s Republic of China
Correspondence: Guoji Zhu, Email [email protected]
Objective: To evaluate the diagnostic performance of combined N-terminal pro-brain natriuretic peptide (NT-proBNP) and cardiac troponin I (cTnI) testing for myocardial injury in children with Mycoplasma pneumoniae pneumonia (MPP).
Methods: This retrospective study included 103 pediatric patients with MPP complicated by myocardial injury admitted between December 2021 and December 2023. Patients were stratified by New York Heart Association (NYHA) functional class (I–IV). Demographic and clinical characteristics, biomarker levels, and diagnostic accuracy were analyzed. ROC curves were used to assess diagnostic performance of single and combined biomarkers.
Results: No significant differences were observed in age or gender across NYHA classes. However, BMI Z-scores declined significantly with worsening class (P = 0.013), while heart rate, systolic blood pressure, fever duration, respiratory rate, and hospital stay increased progressively (all P < 0.01), indicating disease severity. Serum NT-proBNP and cTnI levels rose in parallel with advancing NYHA class (P < 0.001 between all adjacent groups). A strong positive correlation was found between NT-proBNP and cTnI (r = 0.617, P < 0.001). Combined biomarker testing demonstrated superior diagnostic accuracy (AUC = 0.914), outperforming NT-proBNP (AUC = 0.877) and cTnI alone (AUC = 0.739). The combination improved sensitivity (94.15%) and specificity (95.19%), reducing false negatives and enhancing risk stratification. Notably, 80% of NYHA class III–IV cases were correctly reclassified into the high-risk group, with a net reclassification improvement (NRI) of +34.2% (P = 0.002).
Conclusion: Combined NT-proBNP and cTnI testing provides robust diagnostic efficacy for myocardial injury in pediatric MPP. This dual-biomarker strategy enables earlier identification of high-risk patients and supports more precise clinical management.
Keywords: NT-proBNP, cTnI, combined testing, children, mycoplasma pneumoniae pneumonia, myocardial injury, diagnostic efficacy, ROC
Introduction
Mycoplasma pneumoniae pneumonia is a respiratory tract infection caused by Mycoplasma, which primarily affects respiratory epithelial cells and lung tissue, being one of the common respiratory tract infections in children.1 Despite Mycoplasma infection being typically considered a mild respiratory disease, recent studies2 have indicated that it may lead to serious complications including myocardial injury. Myocardial injury refers to structural or functional abnormalities in myocardial cells, which not only increase the complexity of the patient’s condition but may also result in long-term cardiac dysfunction, even life-threatening situations.3 Therefore, timely and accurate assessment and diagnosis of myocardial injury in children with Mycoplasma pneumoniae pneumonia are particularly important.
NT-proBNP and cTnI are two clinically established biomarkers reflecting distinct pathophysiological processes: cTnI is a gold-standard marker for acute myocardial cell necrosis, while NT-proBNP predominantly indicates chronic ventricular wall stress and hemodynamic overload.4 However, emerging evidence suggests that Mycoplasma pneumoniae pneumonia may induce both acute inflammatory myocardial injury (detectable by cTnI elevation) and subclinical ventricular dysfunction (reflected by NT-proBNP rise) through systemic cytokine storms and hypoxia-mediated stress.5 This dual mechanism underscores the rationale for combined biomarker assessment to capture the spectrum of myocardial involvement.
Although prior studies in adults with Mycoplasma pneumoniae pneumonia have demonstrated independent associations of elevated cTnI and NT-proBNP with cardiac complications,6 pediatric data remain scarce. Importantly, biomarker interpretation in children requires age-specific reference values due to developmental variations: NT-proBNP levels physiologically decline with age from infancy to adolescence, and cTnI cutoff values for myocardial injury in children are 50–70% lower than adult thresholds.7 Furthermore, existing adult diagnostic criteria may not extrapolate to pediatric populations, as children exhibit distinct immune responses and myocardial vulnerability patterns.
While cost-effectiveness considerations are valid (combined testing adds ~$30-50 per patient in developing countries), early detection of myocardial injury could reduce long-term cardiac sequelae and hospitalization costs.Current research predominantly focuses on single-marker approaches, leaving a critical knowledge gap regarding the synergistic diagnostic value of these biomarkers in pediatric Mycoplasma-associated myocardial injury.8 Therefore, this study aims to explore the diagnostic efficacy of NT-proBNP and cTnI combined detection in myocardial injury in children with Mycoplasma pneumoniae pneumonia through retrospective analysis of clinical data, and to evaluate its feasibility and accuracy in clinical application.
Materials and Methods
Study Design, Setting, and Period
This retrospective cohort study analyzed pediatric patients diagnosed with Mycoplasma pneumoniae pneumonia complicated by myocardial injury at the First Affiliated Hospital of Bengbu Medical University (Anhui Province, China) between December 2021 and December 2023. The study protocol adhered to STROBE guidelines for observational research and was approved by the Institutional Review Board of the same institution (Approval No.: IRB-2023-045). Written informed consent was waived due to the retrospective nature of the analysis, with all patient data anonymized prior to inclusion in the study.
Inclusion and Exclusion Criteria
Inclusion criteria: ① Children aged 1–14 years meeting diagnostic criteria for Mycoplasma pneumoniae pneumonia;9
② Confirmed myocardial injury defined by any two of the following: Electrocardiographic abnormalities (QRS depression, ST-T changes, prolonged Q-T interval, or conduction block); Echocardiographic evidence of ventricular dysfunction (ejection fraction <55% or fractional shortening <28%); Elevated serum cTnI (>0.04 ng/mL) and NT-proBNP (>300 pg/mL for age <2 years, >125 pg/mL for age ≥2 years);10③ Complete clinical records including biomarker measurements, imaging, and treatment outcomes.
Exclusion criteria: ① Severe organ dysfunction (eg, renal failure, hepatic insufficiency); ② Immunocompromised status, hematologic disorders, or malignancy; ③ Coinfection with other pathogens (bacterial/viral/fungal); ④ Pre-existing congenital heart disease or cardiomyopathy; ⑤ Incomplete laboratory or imaging data.
Sampling Strategy and Sample Size
A convenience sampling method was employed, including all eligible cases during the study period. Sample size calculation used PASS 2021 software with the following parameters: expected AUC difference of 0.15 between single and combined biomarkers (α=0.05, β=0.20), yielding a minimum requirement of 98 patients.
Data Collection and Laboratory Methods
Fasting venous blood samples of 5 mL were collected from all patients in the morning. After standing at room temperature for 20 minutes, the samples were centrifuged at 3,500 rpm for 15 minutes. The supernatant was collected after centrifugation, and the levels of NT-proBNP and cTnI in the serum were detected using the enzyme-linked immunosorbent assay (ELISA) method. The NT-proBNP assay kit was provided by Shanghai Enzyme-linked Biotechnology Co., Ltd., and the cTnI assay kit was provided by InnoBio Science Co., Ltd. All procedures were performed according to the instructions of the assay kits under standard laboratory conditions.
Statistical Analysis
Statistical analyses were performed in three phases. First, descriptive analysis compared continuous variables (mean ± SD) using ANOVA or the Kruskal–Wallis test, and categorical variables (n, %) using the χ²-test or Fisher’s exact test. Second, Pearson’s correlation coefficient (r) was used to evaluate collinearity between NT-proBNP and cTnI. Third, diagnostic performance was assessed with the primary outcome defined as binary classification of myocardial injury based on NYHA class ≥ II. Logistic regression models including both biomarkers were used to generate predicted probabilities for ROC curve construction, and optimal cutoffs were determined by maximizing Youden’s index. Differences between single and combined biomarkers’ AUCs were compared using DeLong’s test. All analyses were conducted using SPSS 22.0 and MedCalc 20.1, with statistical significance set at P < 0.05.
Results
Baseline Characteristics of Patients Stratified by NYHA Functional Class
Table 1 summarizes the baseline demographic and clinical characteristics of the patients classified according to the New York Heart Association (NYHA) functional classes I to IV. No significant differences were observed in gender distribution (P = 0.991) or age (P = 0.874) across the groups. However, BMI Z-scores differed significantly among groups (P = 0.013). Heart rate, systolic blood pressure, fever duration, respiratory rate, and hospital stay all showed a progressive increase with advancing NYHA class (all P < 0.01).
 |
Table 1 Baseline Characteristics of Patients Stratified by NYHA Functional Class |
Biomarker Stratification by NYHA Class
Serum NT-proBNP and cTnI levels progressively increased with worsening NYHA class (Table 2). NT-proBNP levels rose from 238.47 ± 65.82 ng/L in Class I to 551.91 ± 110.49 ng/L in Class IV, with statistically significant differences between all adjacent classes (P < 0.001). Similarly, cTnI levels increased from 0.38 ± 0.11 ng/mL in Class I to 0.89 ± 0.26 ng/mL in Class IV (P < 0.001).
 |
Table 2 Biomarker Levels Stratified by NYHA Class |
Biomarker Correlation and Diagnostic Performance
A strong positive correlation was observed between NT-proBNP and cTnI (r = 0.617, P < 0.001; Figure 1). ROC analysis revealed that combined detection of these biomarkers provided superior diagnostic accuracy with an AUC of 0.914, compared to individual markers (Table 3 and Figure 2). Importantly, combined testing reduced false negatives by correctly identifying 12 cases missed by cTnI alone and improved risk stratification, upgrading 28 out of 35 (80%) NYHA class III–IV cases to a high-risk category using dual thresholds. The net reclassification improvement (NRI) was +34.2% (P = 0.002), indicating significant enhancement in patient classification.
 |
Table 3 Diagnostic Performance and Clinical Reclassification |
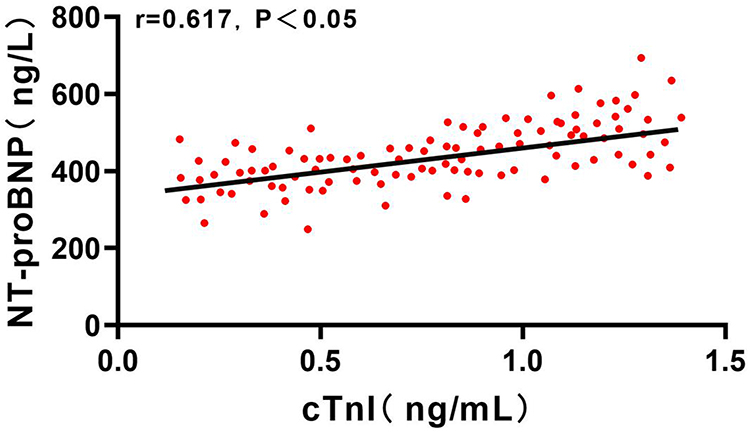 |
Figure 1 Correlation Analysis between Serum NT-proBNP and cTnI. |
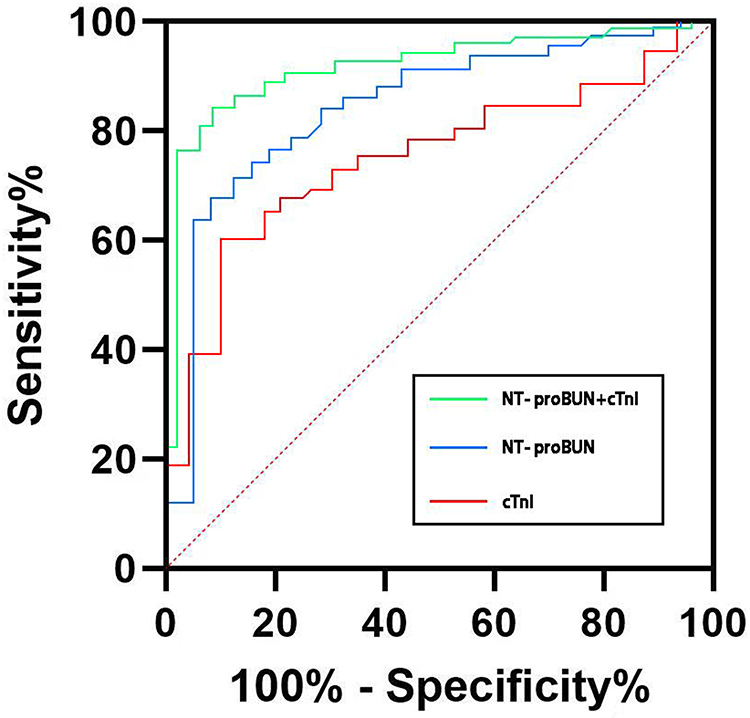 |
Figure 2 ROC Curves for NT-proBNP, cTnI, and Combined Detection in Diagnosing Myocardial Injury in MPP. |
Discussion
Mycoplasma pneumoniae (MP) is a prokaryotic microorganism that lies between bacteria and viruses and can spread through various routes such as oral and nasal secretions and airborne transmission, causing infections.11 When the human body is infected with MP pneumonia, it can adhere to the respiratory epithelial cells through specific cell membrane receptors, not just existing on the surface of the respiratory tract. This adhesion not only inhibits the normal movement of respiratory cilia but also damages the epithelial cells, leading to the production of harmful substances and causing damage to local tissues.12 Studies13 have shown that if MP pneumonia does not receive timely and effective intervention, it may lead to damage to other organ functions, such as the liver, kidneys, and myocardium, thereby threatening the health and life of patients. Additionally, research14 indicates that myocardial damage is the most common complication of MP pneumonia. Studies by Ludwikowska15 et al found that children aged 13 to 36 months and 6 to 14 years with MP pneumonia are more prone to myocardial damage, which may be related to the immune systems of children at different ages. Studies by Mei16 et al found that factors such as the degree and duration of fever, C-reactive protein (CRP), among others, may independently become risk factors for concomitant myocardial damage in pneumonia patients. Therefore, early screening and diagnosis of myocardial damage in MP pneumonia children are crucial for detecting and adopting appropriate treatment measures promptly, which is essential for improving the condition of the children and enhancing clinical treatment outcomes.
Currently, electrocardiography, echocardiography, and serum biochemical markers are commonly used in clinical practice to screen for myocardial injury. However, multiple studies17,18 have shown that due to the lack of specific manifestations of early myocardial injury, electrocardiography, echocardiography, and other methods have not been able to detect significant changes, posing a challenge to the early diagnosis of myocardial injury. Serum biochemical markers can timely and accurately reflect physiological changes in the body, playing an important role in clinical diagnosis. Cardiac enzyme spectrum is a common indicator used in the past clinical diagnosis of diseases such as myocardial ischemia and myocardial infarction, but recent studies19 have shown issues with its sensitivity and specificity in diagnosing myocardial injury. Therefore, finding serum biochemical markers more suitable for detecting myocardial injury in Mycoplasma pneumoniae (MP) pneumonia is particularly important. cTnI is a protein present in myocardial cells that binds to calcium ions during the process of myocardial contraction and relaxation, playing an important regulatory role.20 When myocardial cells are damaged or die, cTnI is released into the bloodstream, and its elevated serum levels can reflect the extent of myocardial injury. This study found that with the increase in the functional classification of patients, the level of cTnI also increased correspondingly, suggesting that patients with MP pneumonia complicated by myocardial injury exhibit abnormally elevated levels of cTnI. Analysis suggests that in patients with MP pneumonia, inflammatory and immune responses caused by infection may lead to damage or death of myocardial cells, resulting in increased release of cTnI and elevated concentrations in the blood.
NT-proBNP is a peptide hormone produced by myocardial cells and is a novel serum marker that has received considerable attention in recent years. Studies21 have shown that when myocardial cells suffer from ischemia, injury, or decreased cardiac function, serum NT-proBNP tends to increase abnormally, and is less susceptible to the influence of drugs. Research by Yuan22 and others has demonstrated that NT-proBNP is superior to traditional methods such as electrocardiography and echocardiography in early screening for heart failure and myocardial injury. This study analyzed the clinical application of NT-proBNP in the diagnosis of myocardial injury combined with Mycoplasma pneumoniae (MP) pneumonia. The results showed that as the functional classification of patients increased, the serum NT-proBNP levels also increased correspondingly, which is consistent with previous research.23 It is believed that when myocardial cells are damaged, proBNP is produced, which is then broken down by endopeptidases into NT-proBNP and BNP. Due to the longer half-life and stability of NT-proBNP both in vivo and in vitro, the NT-proBNP level continues to increase abnormally with the increasing degree of myocardial cell damage. Therefore, measuring serum NT-proBNP levels can reflect the extent of myocardial injury in patients.
This study analyzed the correlation between NT-proBNP and cTnI, and the results showed a significant positive correlation between serum NT-proBNP and cTnI levels (r=0.617, P<0.05). Furthermore, the diagnostic efficacy of NT-proBNP and cTnI for children with Mycoplasma pneumoniae (MP) pneumonia combined with myocardial injury was analyzed using ROC curve analysis. It was found that the AUC for NT-proBNP and cTnI in diagnosing myocardial injury associated with Mycoplasma pneumoniae pneumonia was 0.877 and 0.739, respectively, indicating a certain diagnostic value. However, the AUC for NT-proBNP+cTnI combined detection was 0.914, with a sensitivity of 94.15% and a specificity of 95.19%, which was significantly higher than that of single NT-proBNP and cTnI detection (P<0.05). Therefore, the combined detection of NT-proBNP and cTnI has a more ideal diagnostic value in diagnosing children with Mycoplasma pneumoniae pneumonia combined with myocardial injury.
Despite these promising results, it is important to clarify the justification and clinical relevance of this study in the context of existing literature. Previous research has established the utility of NT-proBNP and cTnI as biomarkers of myocardial injury in adults and in other cardiac conditions, but studies focusing specifically on pediatric patients with Mycoplasma pneumoniae pneumonia remain scarce and fragmented.24 This study fills this gap by providing focused data on the pediatric population, highlighting how combining these biomarkers can improve diagnostic accuracy compared to single-marker or ECG-based approaches.
Electrocardiography (ECG) and echocardiography are commonly used in clinical practice to detect myocardial injury; however, their sensitivity in early or mild cases—especially in children—is limited due to nonspecific or delayed changes. Biochemical markers like NT-proBNP and cTnI offer a more sensitive and timely indication of myocardial injury, which is critical for early diagnosis and intervention.9 This clinical implication underscores the value of biochemical testing as a complementary tool to traditional cardiac assessments, particularly when ECG findings are inconclusive or when access to echocardiography is limited.
Regarding the diagnostic metrics, while area under the curve (AUC) values provide a statistical measure of test accuracy, they may not fully convey clinical utility. To address this, our study further analyzed net reclassification improvement (NRI), demonstrating a 34.2% enhancement in patient risk stratification when combining NT-proBNP and cTnI. This improvement translated into identifying 12 previously missed cases and upgrading 80% of patients with severe functional impairment (NYHA class III–IV) to a high-risk category. These findings highlight the tangible patient-level benefits of combined biomarker testing beyond statistical indices.5
Nevertheless, several limitations should be acknowledged: the single-center, retrospective design may introduce selection bias despite consecutive enrollment; age-related differences in myocardial vulnerability require further exploration; and long-term outcomes of biomarker-guided therapy remain to be prospectively validated. Future multicenter studies incorporating serial biomarker measurements alongside cardiac MRI are warranted to elucidate the causal relationship between Mycoplasma-induced inflammation and myocardial injury. Despite these limitations, our findings offer actionable evidence supporting the integration of dual-biomarker screening into pediatric pneumonia guidelines, particularly in cases with inconclusive ECG findings.
Conclusion
This study systematically validates the synergistic diagnostic value of NT-proBNP and cTnI in detecting myocardial injury among 103 pediatric patients with Mycoplasma pneumoniae pneumonia (MPP), addressing a critical gap in existing literature that has largely focused on adult populations or single-biomarker approaches. Key findings demonstrate that serum NT-proBNP and cTnI levels increased progressively with worsening NYHA functional class. A strong positive correlation between the two markers highlights their complementary role in disease severity assessment. Combined biomarker detection significantly improved diagnostic performance (AUC = 0.914), reduced false negatives, and upgraded 80% of NYHA class III–IV cases to a high-risk tier. The observed net reclassification improvement of 34.2% further reinforces the clinical utility of dual-marker screening in enhancing diagnostic accuracy and risk stratification.
Funding
Natural science research projects in Bengbu Medical College (2021byzd183).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Borensztajn DM, Tan CD, de Rijke Y, et al. Elevated high-sensitivity troponin and NT-proBNP values in febrile children. Pediatric Emergency Care. 2023;
2. Cai Q, Liu M, Xie Z, et al. Specific reference interval for high-sensitivity cardiac troponin I among healthy children in Wuhan. Trans Pediatrics. 2024;13(6):908. doi:10.21037/tp-24-98
3. Chung W-S, Hsu W-H, Lin C-L, C-HJQAIJo K. Mycoplasma pneumonia increases the risk of acute coronary syndrome: a nationwide population-based cohort study. QJM. 2015;108(9):697–703. doi:10.1093/qjmed/hcv015
4. Clerico A, Aimo A, Mjcc C, Medicine L. High-sensitivity cardiac troponins in pediatric population. Clin Chem Laboratory med. 2022;60(1):18–32. doi:10.1515/cclm-2021-0976
5. Desai A, Aliberti S, Amati F, Stainer A, Voza AJM. Cardiovascular complications in community-acquired pneumonia. Microorganisms. 2022;10(11):2177.
6. Dong K, Xing J, Dai Y, et al. Age-and sex-specific upper reference limits for cardiac biomarkers in Chinese children and adolescents: a prospective study. Sci Reports. 2024;14(1):28295. doi:10.1038/s41598-024-77153-8
7. Fasano T, Fortunato A, Giacomini G, et al. Analytical characteristics and performance of a new hs-cTnI method: a multicenter-study: on behalf of the study group on cardiac biomarkers of the Italian societies of laboratory medicine SIBioC and ELAS. Clin Chem Laboratory Med. 2025;63:821–830. doi:10.1515/cclm-2024-0905
8. Gessner R, Gärtner C, Schmidt M, et al. Higher troponin T serum concentrations in hospital patients without diagnosed cardiac diseases compared to a population-based cohort. Clin Chem Laboratory Med. 2023;61(11):2046–2052. doi:10.1515/cclm-2023-0040
9. Gore MO, Seliger SL, Defilippi CR, et al. Age-and sex-dependent upper reference limits for the high-sensitivity cardiac troponin T assay. J Am College Cardiol. 2014;63(14):1441–1448. doi:10.1016/j.jacc.2013.12.032
10. Guo Q, Yang D, Zhou Y, et al. Establishment of the reference interval for high-sensitivity cardiac troponin T in healthy children of Chongqing Nan’an district. Scandinavian J Clin Laboratory Investig. 2021;81(7):579–584. doi:10.1080/00365513.2021.1979245
11. Huang C, Xiao S, Xia Z, et al. The diagnostic value of plasma miRNA-497, cTnI, FABP3 and GPBB in pediatric sepsis complicated with myocardial injury. Ther. Clin. Risk Manag. 2021;563–570.
12. Jat NK, Bhagwani D, Bhutani N, et al. Assessment of the prevalence of congenital heart disease in children with pneumonia in tertiary care hospital: a cross-sectional study. Ann Med Surg. 2022;73:103111. doi:10.1016/j.amsu.2021.103111
13. Kopec M, Duma A, Helwani MA, et al. Improving prediction of postoperative myocardial infarction with high-sensitivity cardiac troponin T and NT-proBNP. Anesthesia Analgesia. 2017;124(2):398–405. doi:10.1213/ANE.0000000000001736
14. C-w L, Tang W, Wen F, J-j C, X-l Z, Z-gJPO C. Diagnostic accuracy of NT-ProBNP for heart failure with sepsis in patients younger than 18 years. PLoS One. 2016;11(1):e0147930. doi:10.1371/journal.pone.0147930
15. Ludwikowska KM, Tokarczyk M, Paleczny B, Tracewski P, Szenborn L, Kusa JJIJo MS. Clinical significance of B-type natriuretic peptide and N-terminal pro-B-type natriuretic peptide in pediatric patients: insights into their utility in the presence or absence of pre-existing heart conditions. Int J Mol Sci. 2024;25(16):8781. doi:10.3390/ijms25168781
16. Mei Y, Tang D, Zhao L, Peng M, Bjhjp Z. Risk factors for myocardial damage and its effects on the prognosis of children with severe pneumonia: a cross-sectional study. HK J Paediatr. 2024;29(4):212–224.
17. Nantanda R, Bwanga F, Najjingo I, Ndeezi G, Jkjp T, Health IC. Prevalence, risk factors and outcome of Mycoplasma pneumoniae infection among children in Uganda: a prospective study. Paediatrics Int Child health. 2021;41(3):188–198. doi:10.1080/20469047.2021.1980698
18. Palm J, Hoffmann G, Klawonn F, et al. Continuous, complete and comparable NT-proBNP reference ranges in healthy children. Clin Chem Laboratory Med. 2020;58(9):1509–1516. doi:10.1515/cclm-2019-1185
19. Rodríguez-González M, Estepa-Pedregosa L, Estalella-Mendoza A, Castellano-Martínez A, Rodríguez-Campoy P, Jcjcca F-G. Early elevated NT-proBNP but not troponin I is associated with severe bronchiolitis in infants. Clin Chimica Acta. 2021;518:173–179. doi:10.1016/j.cca.2021.03.023
20. Shen H, He Q, Shao X, et al. Predictive value of NT-proBNP and hs-TnT for outcomes after pediatric congenital cardiac surgery. Int J Surg. 2024;110(6):3365–3372. doi:10.1097/JS9.0000000000001311
21. Yu Y, Jin X, Zhang X, Yjtpidj S. Pulmonary thrombotic complication of mycoplasma pneumoniae pneumonia in Chinese children: clinical feature and risk factor analysis. Pediat Inf Dis J. 2024;43(6):505–510. doi:10.1097/INF.0000000000004287
22. Yuan Y, Pan B, Wang F, et al. Age‐based classification and outcomes in pediatric heart failure: findings from a retrospective multicenter cohort study. J Ame Heart Association. 2025;14(4):e038129. doi:10.1161/JAHA.124.038129
23. Zhang Y, Luo Y, Nijiatijiang G, et al. Correlations of changes in brain natriuretic peptide (BNP) and cardiac troponin I (cTnI) with levels of C-reactive protein (CRP) and TNF-α in pediatric patients with sepsis. Med Sci Monitor. 2019;25:2561. doi:10.12659/MSM.912318
24. Zhou Y, Shan Y, Cui Y, et al. Characteristics and outcome of severe Mycoplasma pneumoniae pneumonia admitted to PICU in Shanghai: a retrospective cohort study. Critical Care Explorations. 2021;3(3):e0366. doi:10.1097/CCE.0000000000000366
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Clinical Significance of Pathogen Loads and Macrolide Resistance Levels for Macrolide-Resistant Mycoplasma pneumoniae Pneumonia in Children
Leng M, Xu L, Dong Z, Yang J
Journal of Inflammation Research 2024, 17:7339-7346
Published Date: 15 October 2024