")
Back to Journals » Journal of Inflammation Research » Volume 17
Diagnostic Value of SAA Levels and Perianal Symptoms in the Complicated Perianal Abscesses Among Mpox-Infected Patients
Authors Wang Y , Zhang W, Liu S, Wang F, Huang Q, Li E, Zhu M , Yu J, Shi J
Received 8 April 2024
Accepted for publication 24 August 2024
Published 9 September 2024 Volume 2024:17 Pages 6239—6250
DOI https://doi.org/10.2147/JIR.S472800
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Yi Wang,1,2 Wenhui Zhang,1,3 Shourong Liu,1 Fei Wang,1 Qian Huang,1 Er Li,3 Mingli Zhu,4 Jianhua Yu,1,* Jinchuan Shi1,*
1Department of Infection, Affiliated Hangzhou Xixi Hospital, Zhejiang University of Traditional Chinese Medicine, Hangzhou, People’s Republic of China; 2Institute of Hepatology and Epidemiology, Affiliated Hangzhou Xixi Hospital, Zhejiang University of Traditional Chinese Medicine, Hangzhou, People’s Republic of China; 3Department of Nursing, Affiliated Hangzhou Xixi Hospital, Zhejiang University of Traditional Chinese Medicine, Hangzhou, People’s Republic of China; 4Medical Laboratory, Affiliated Hangzhou Xixi Hospital, Zhejiang University of Traditional Chinese Medicine, Hangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jianhua Yu; Jinchuan Shi, Department of Infection, Affiliated Hangzhou Xixi Hospital, Zhejiang University of Traditional Chinese Medicine, Hangzhou, People’s Republic of China, Email [email protected]; [email protected]
Objective: Precise prediction of the occurrence of complicated perianal abscesses (PAs) in monkeypox (mpox)-infected patients is important for therapeutic optimization. This study sought to identify risk factors of complicated PA.
Methods: A total of 48 patients with mpox infection (PA group, n = 10; non-PA (NPA) group, n = 38) were enrolled in our study, who were hospitalized in Hangzhou Xixi Hospital, China from 29 June to 3 September 2023. The data of demographic characteristics, and clinical symptoms, serum SAA, PCT, CRP, and IL-6 levels were collected by the Electronic Medical Record. The diagnostic values of these biomarkers were assessed using multivariate logistic regression and ROC curve analyses.
Results: A decrease in serum IL-6, SAA, and CRP levels (all p-value < 0.05), but not PCT, was observed in all mpox-infected patients. A significant positive correlation was also noted between IL-6, SAA, CRP, and PCT levels (all p-value < 0.05). There was a significant increase in IL-6 and SAA levels and the SAA/CRP ratio in serum samples from patients in the PA group. Multivariate logistic regression and ROC curve analyses identified that the combined use of perianal symptoms and SAA was more sensitive than perianal symptoms or SAA alone as predictors of complicated PA. This combination had the highest predictive value for disease progression, with an AUC of 0.920 (p-value < 0.001).
Conclusion: The combination of perianal symptoms and SAA levels was strongly linked to the occurrence of complicated PA in mpox-infected patients. These findings may inform the early diagnosis of this patient population.
Keywords: serum amyloid A, perianal symptoms, perianal abscess, mpox-infected patients
Introduction
Monkeypox is an infectious disease caused by the human monkeypox virus (MPXV), a zoonotic DNA virus of the Orthopoxvirus genus.1 Since May 2022, more than 80,000 MPXV infections have been reported in countries throughout the Americas, Africa, and Europe.2,3 On June 23, 2022, the World Health Organization (WHO) declared MPXV an “evolving threat of moderate public health concern”.4 There are many symptoms associated with this disease, including full-body skin lesions, fever, genital or perianal lesions, fatigue, enlarged lymph nodes, and sore throat, of which perianal lesions are most commonly reported first symptom of MPXV infection.5,6 MPXV can be transmitted directly, through tattooing or injection or the respiratory route, mostly affecting MSM.7,8 Clade IIb was the predominant strain amid the 2022 mpox outbreak.8 Despite the use of antiviral agents and intravenous vaccinia immunoglobulin, the mpox-associated perianal lesions evolved into abscesses, requiring incision and drainage.9 PA is a common perianal condition that is most often caused by metastatic gland infections.10 Ogoina et al recognized PA as one of the primary complications of MPXV infection.11 Among mpox-infected patients, persistent or progressively worsening proctalgia indicates the presence of a PA. However, to date, the clinically related factors of complicated PAs in mpox-infected patients have not been explored. Thus, it is critical to identify the predictive factors of complicated PAs associated with this infection.
Inflammation is a protective response to invading pathogens and plays an important role during infection. This process is triggered by activation of the inflammasome through endogenous stress signals or the binding of evolutionarily conserved microbial structures to Toll-like receptors.12 Inflammatory processes are mediated by various inflammatory molecules, including cytokines such as interleukin (IL)-6 and acute phase proteins (APP) such as C-reactive protein (CRP), serum amyloid A (SAA), and procalcitonin (PCT).13 Both cytokines and APPs are widely used to aid the clinical diagnosis of infections.14–16 For example, IL-6, CRP and PCT correlate significantly with the progression of infectious diseases such as coronavirus disease 2019 (COVID-19) and respiratory tract infections.17–19 Perez et al reported that prematurely elevated SAA helps to differentiate viral from bacterial etiologies.20 However, the role of cytokines or APPs during MPXV infection are less well studied. Existing research has confirmed that proinflammatory cytokines (such as IL-6)21 and other cytokines (including IFN-γ, IL-2, and TNF)22 are higher in mpox-infected patients than in healthy donors. In reported cases of human MPXV infection, several cytokines are elevated regardless of disease severity.23 Further evidence indicates that marked inflammatory cytokine responses induced by MPXV infection play a critical role in disease progression.24 However, additional research is needed to determine how well inflammatory cytokine levels correlate with the progression of MPXV disease.
The current study evaluated the association between SAA, PCT, CRP, and IL-6 levels and disease progression in mpox-infected patients. To our knowledge, this is the first time a potential link between diagnostic SAA levels and symptoms associated with complicated PAs in mpox-infected patients has been explored. The findings may inform the development of a method to improve the diagnosis of MPXV disease.
Materials and Methods
Study Population and Design
This retrospective study recruited 54 patients with MPXV infection who were hospitalized in Hangzhou Xixi Hospital, China from 29 June to 3 September 2023. The inclusion criteria were: (1) positive MPXV DNA test from a throat swab or blister fluid; (2) clinical signs consistent with MPXV, including skin rash or mucosal lesions which can last 2–4 weeks accompanied by fever, headache, muscle aches, back pain, low energy, and swollen lymph nodes (https://www.who.int/news-room/fact-sheets/detail/monkeypox). The exclusion criteria were: (1) suffered from acute tonsillitis or sepsis; (2) had a history of a PA or anal fistula; (3) died from other diseases.
According to the exclusion criteria, 5 mpox-infected patients were excluded due to tonsillitis or sepsis, and one was excluded due to death. In total, 48 mpox-infected patients were included in the further analysis. On magnetic resonance imaging (MRI) and rectal examinations, a total of 10 patients developed PA with fluid exudation and intermittent pain (PA group). The MPXV nucleic acid test was positive in perianal blister fluid among 10 PA-patients, only 2 patients with perianal blister fluid culture were weakly positive for Escherichia coli, indicating complicated PA is attributed to MPXV infection rather than bacterial superinfection. There was no severe perianal symptoms in the remaining 38 patients (non-PA group). Baseline data including demographic characteristics (age, sex, marital status, education level, homosexual behavior, HIV status, body mass index (BMI), smoking status, drinking status, syphilis status, and antibiotic use) and clinical symptoms were collected from the Electronics Medical Records (EMR) management system. A study flowchart is shown in Figure 1.
 |
Figure 1 Study profile for follow-up. A total of 48 mpox-infected patients were included in the study. MPXV: monkeypox virus. |
Measurement for Serum Parameters
SAA and CRP levels were quantitatively determined using an Immunoturbidimetric Assay (Goldsite Diagnostics Inc)., according to the manufacturer’s instructions. An immunochemiluminescence instrument (Roche COBAS 601) was used to detect IL-6 and PCT levels using the manufacturer’s matching reagent. All equipment was maintained and calibrated according to the specified requirements. Internal and external quality assessments were performed.
Outcomes of Interest
The primary outcome was the complicated PA of mpox-infected patients. The diagnosis of PA is usually based on a detailed medical history and physical examination (including magnetic resonance imaging (MRI) and digital rectal examination or anoscopy). Superficial abscesses are often present with perianal pain and swelling but rarely fever. Deep abscesses such as ischial rectal fossa or pelvic rectal space abscesses can be accompanied by perineum and lumbosacral pain and swelling. PA diagnosis requires confirmation by MRI and digital rectal examination or anoscopy.25,26 The main clinical manifestations of PA included perianal ulcerative lesions, rectal wall thickening and edema with fluid exudation, enlarged pelvic and groin lymph nodes, and persistent or progressively worse proctalgia.27 PA as a complication of refractory MPXV lesions treated with incision and drainage.7
Statistical Analysis
All statistical analyses were performed using R statistical software (R version 4.1.3) and SPSS (Version 25.0). Normally distributed continuous variables were described as means with standard deviations (SD). The median (M) and its interquartile range (IQR, 1st quartile, 3rd quartile) and nonparametric Wilcoxon signed-rank tests were used to describe and compare variables with non-normal distributions, respectively. Numbers and percentages were reported for categorical variables. Proportions were compared using Pearson’s Chi-square test. Correlation analysis was performed using Spearman non-parametric correlation tests.28 Multivariate logistic regression analysis was used to determine covariate association with the occurrence of PA. All graphs were created using GraphPad Prism 8 software (GraphPad Software Inc., San Diego, CA, USA).29 The area under the curve (AUC) was plotted using MedCalc software (MedCalc, version 18.2.1) with sensitivity and specificity values.30 All reported levels of statistical significance were two-sided, and p-value < 0.05 were considered statistically significant.
Results
Baseline Characteristics of the Patients
A total of 48 mpox-infected patients were enrolled in this study, of whom 10 had PA (20.83%). The mean age of 48 mpox-infected patients was 29.6 years (SD: 5.9), 100% were male, and the mean BMI was 22.4 (SD: 2.8). In addition, 70.83% of males as having engaged in same-sex sexual experiences. Among 48 patients, 24 patients (50%) were HIV-positive, 24 patients (50%) were HIV-negative. Some clinical symptoms related to MPXV infection, including pruritus (27.08%), fever (64.58%), chills (6.25%), perianal manifestations (31.25%; including redness, pain, and oozing), PA (20.83%), dizziness (10.42%), headache (8.33%), sore throat (4.17%), muscle aches (6.25%), fatigue (2.08%), swollen lymph nodes (14.58%) and herpes (60.42%). All mpox-infected patients had rashes on different body regions, including the head/face, trunk, limbs, and genitals or perianal regions. While in the hospital, more than half of the patients received antibiotics for preventing secondary bacterial infections (54.17%), including doxycycline, ampicillin, moxifloxacin, cephalosporins, levofloxacin, and azithromycin. Additional clinical characteristics of the patients are shown in Table 1.
 |
Table 1 Baseline Characteristics of All Participants (n = 48) |
Dynamic Changes in the Levels of Inflammatory Markers in Serum Samples from Mpox-Infected Patients
IL-6, SAA, CRP, and PCT levels were compared among the mpox-infected patients at three time points (T1–T3) after hospitalization. The levels of IL-6 (Figure 2A and Table S1; both p-value < 0.01), SAA (Figure 2B and Table S1; p-value < 0.001), CRP (Figure 2C and Table S1; p-value < 0.05), and PCT (Figure 2D and Table S1; p-value < 0.01) declined significantly from T1 (< 3 days) to T2 (4–7 days) and T3 (> 8 days). The levels of IL-6 (Figure 2A and Table S1; p-value = 0.003), SAA (Figure 2B and Table S1; p-value < 0.001), and CRP (Figure 2C and Table S1; p-value = 0.023) further decreased from T2 to T3. PCT levels remained similar between these time points (Figure 2D and Table S1; p-value = 0.557).
 |
Figure 2 Comparison of the serum levels of IL-6 (A), SAA (B), CRP (C), and PCT (D) at T1 and T2, or T3 after hospitalization in mpox-infected patients. ns p-value > 0.05, * p-value < 0.05, ** p-value < 0.01, *** p-value < 0.001. Abbreviations: IL-6, interleukin 6; SAA, serum amyloid A; CRP, C-reactive protein; PCT, procalcitonin; T1, < 3 days; T2, 4–7 days; T3, > 8 days. |
3.3 Significant positive interplay among IL-6, SAA, CRP, and PCT levels in the serum of mpox-infected patients.
A significant positive association was observed among the levels of IL-6 and SAA (Figure 3A, r = 0.702, p-value < 0.001), IL-6 and CRP (Figure 3B, r = 0.835, p-value < 0.001), IL-6 and PCT (Figure 3C, r = 0.558, p-value < 0.001), SAA and CRP (Figure 3D, r = 0.867, p-value < 0.001), SAA and PCT (Figure 3E, r = 0.558, p-value < 0.001), and CRP and PCT (Figure 3F, r = 0.647, p-value < 0.001).
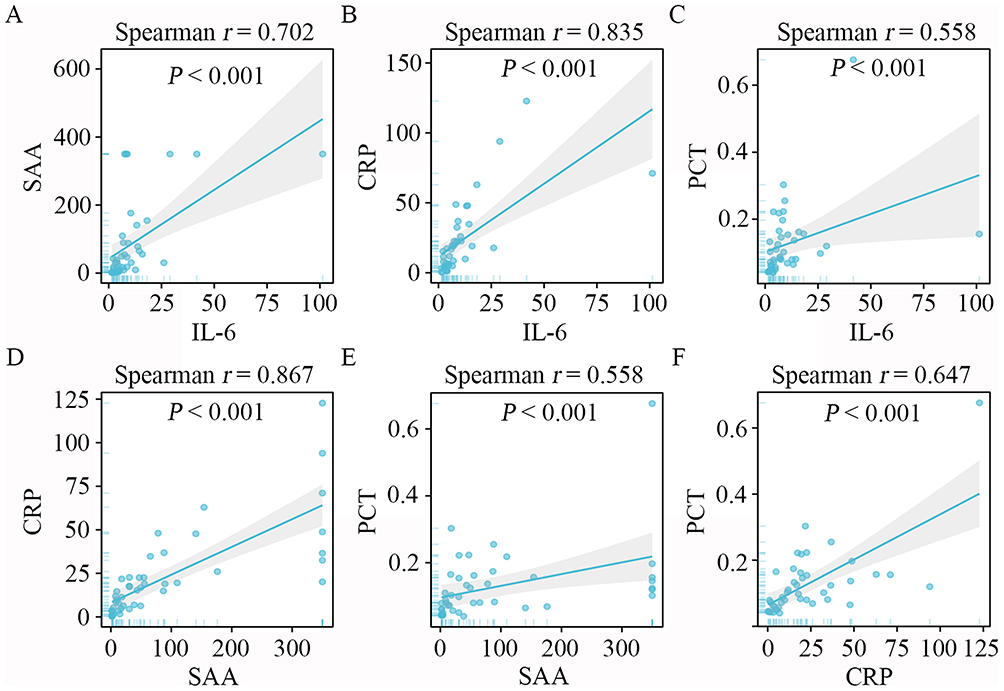 |
Figure 3 Mutual correlation of the serum levels of IL-6, SAA, CRP, and PCT after patient hospitalization. (A–C) Association between IL-6 and SAA, CRP, and PCT levels. (D and E) Correlation between SAA and CRP and PCT levels. (F) Correlation between CRP and PCT levels. Abbreviations: IL-6, interleukin 6; SAA, serum amyloid A; CRP, C-reactive protein; PCT, procalcitonin. |
To better understand the relationship between serum IL-6, SAA, CRP, and PCT levels within the PA and NPA groups, Spearman rank correlation analysis was performed. There was a significant correlation between IL-6 and CRP (NPA: r = 0.770, p-value < 0.001; PA: r = 0.762, p-value < 0.05), SAA and CRP (NPA: r = 0.837, p-value < 0.001; PA: r = 0.873, p-value < 0.01), SAA and PCT (NPA: r = 0.642, p-value < 0.001; PA: r = 0.791, p-value < 0.05), and CRP and PCT (NPA: r = 0.734, p-value < 0.001; PA: r = 0.738, p-value < 0.05) in the NPA (Table S2) and PA groups (Table S3). In the NPA group, there was also a significant correlation between IL-6 and SAA (Table S2, r = 0.626, p-value < 0.001), and IL-6 and PCT (Table S2, r = 0.616, p-value < 0.001). In contrast, IL-6 was not significantly positively correlated with SAA (Table S3, r = 0.464, p-value > 0.05) and PCT (Table S3, r = 0.333, p-value > 0.05) in the PA group.
Comparison of the Clinical Characteristics Between the NPA and PA Groups in Mpox-Infected Patients
Except for antibiotic use, the demographic characteristics of the two groups were similar (Table S4). Further analyses revealed that patients in the PA group had more perianal symptoms (including redness, pain, and oozing) than those in the NPA group (Table 2, p-value = 0.001). Serum levels of IL-6 (p-value = 0.01) and SAA (p-value = 0.001) and the ratio of SAA/CRP (p-value = 0.004) were also significantly higher in the PA group than in the NPA group (Table 2). However, there was no significant difference in CRP and PCT levels between both groups (Table 2).
 |
Table 2 Comparison of the Clinical Characteristics Between Non-Perianal Abscess and Perianal Abscess Groups |
Risk Factors for Predicting the Occurrence of PA in Mpox-Infected Patients
Potential factors associated with the occurrence of PA in mpox-infected patients were explored. First, the optimal cut-off values of age, IL-6 levels, SAA levels, and the SAA-CRP ratio to effectively predict the outcome of patients with PA were explored. The values were > 29 years, > 6.59 mg/L, > 87.99 mg/L, and > 2.82 for age, IL-6, SAA, and the SAA-CRP ratio, respectively (Table S5). Moreover, univariate analysis revealed that age, perianal symptoms, and SAA were associated with PA. After controlling for age, multivariate analysis verified that the risk factors associated with PA were perianal symptoms (p-value = 0.02) and an SAA of 87.99 mg/L (p-value = 0.015) (Table 3).
 |
Table 3 Logistic Regression for Factors Associated with Perianal Abscess |
ROC analysis was then used to assess the ability of perianal symptoms and SAA to predict the occurrence of complicated PA in mpox-infected patients. The AUC values for perianal symptoms and SAA levels were 0.808 (95% CI: 0.665–0.909, p-value < 0.001) (Figure 4A and Table S6) and 0.850 (95% CI: 0.714–0.938, p-value < 0.001), respectively (Figure 4B and Table S6). A prediction model with an AUC of 0.920 (95% CI: 0.802–0.980, p-value < 0.001) was constructed using these variables (Figure 4C and Table S6). The sensitivity and specificity of the model were 100% and 70.27%, respectively.
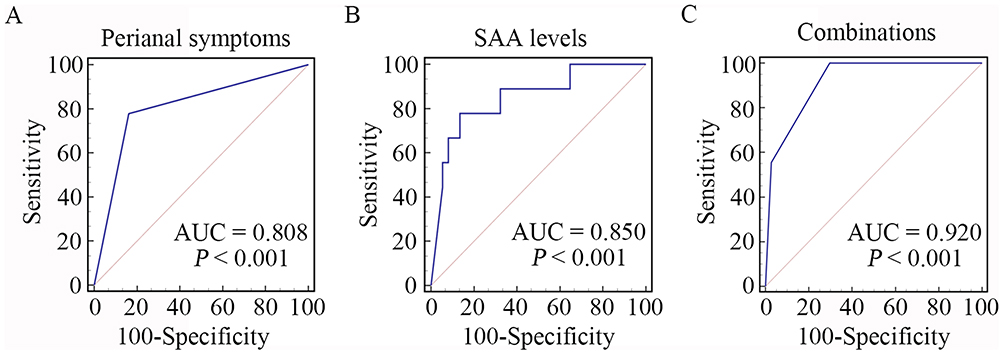 |
Figure 4 Diagnostic value of perianal symptoms and serum SAA levels in mpox-infected patients with PA. (A) ROC curve of perianal symptoms in the PA and NPA groups. (B) ROC curve of SAA levels in the PA and NPA groups. (C) ROC curve of perianal symptoms and SAA levels in the PA and NPA groups. Abbreviations: SAA, serum amyloid A; AUC: NPA, non-perianal abscess; PA, perianal abscess. |
Discussion
Mpox is usually a self-limited disease, patients can suffer from extremely painful skin lesions, and complications are limited as recent publications mainly focus on patients with inflammatory bowel disease (including PAs).31–33 PAs have been reported as one of the primary complications of MPXV infection,11 while PA is regarded as be associated with inflammatory conditions.33 Further evidence indicates that marked inflammatory cytokine responses induced by MPXV infection play a critical role in MPXV disease progression.24 However, additional research is needed to determine how well inflammatory cytokine levels correlate with the occurrence of complicated PAs of MPXV disease. Assessing inflammatory cytokine serum levels can play a vital role in the management of infectious diseases, aiding in risk assessment, monitoring disease progression, determining diagnosis or prognosis, selecting therapy, and predicting the response to treatment.16,34–36 The current study demonstrated a significant increase in IL-6 and SAA levels, and the SAA/CRP ratio in the serum samples of mpox-infected patients with PA. Importantly, both perianal symptoms and SAA levels were strongly linked with the risk of complicated PA in this patient population.
Few clinical studies have assessed how well IL-6, SAA, PCT, and CRP levels correlate with disease progression in mpox-infected patients. The current study revealed an increasing trend in serum IL-6, SAA, and CRP levels for the complicated PAs of mpox-infected patients comparing to non-PA mpox-infected patients. This result consistent with a prior study that linked the inflammatory cytokines with infectious disease severity.37 We also observed a significant positive correlation between the increased serum levels of IL-6, SAA, CRP, and PCT among mpox-infected patients. This finding suggests that these cytokines may be produced from a single cell source, such as monocytes, that release all of these cytokines upon activation.38 Together, these results favor a strong correlation among these acute phase proteins and cytokines.
To identify factors that predict complicated PA in mpox-infected patients, clinical characteristics were compared between patients in the PA and NPA groups. Serum IL-6 and SAA levels and the SAA/CRP ratio were higher in PA patients than in NPA patients following hospitalization. Thus, the mpox-infected patients with higher Serum IL-6 and SAA levels and the SAA/CRP ratio should pay more attention. Buck et al found that hepatic cell-induced SAA and CRP production is affected by IL-6 in vitro, suggesting that the transcription, translation, and/or secretion of these factors may be coordinated.39 SAA is a better predictor of disease in patients with a high SAA/CRP ratio.40 Indeed, SAA levels are not only closely associated with the progression of MPXV disease, but also serve as a predictor of complicated PA among mpox-infected patients. The current study found that hospitalized mpox-infected patients with a higher serum concentration of SAA had a noticeably higher risk of complicated PA. Previous studies have also shown that SAA can be used as an indicator of the immune response to infection,14,41 reflecting the extent and severity of underlying inflammation.41 Thus, increased serum SAA concentrations may correlate highly with inflammation and disease progression,42,43 suggesting that this factor plays an important role in the response to infectious disease. The current study provides strong evidence that serum SAA levels may serve as an early indicator of MPXV disease progression including secondary bacterial infections or other severe outcomes,44 and inform the use of treatment to prevent perianal disease.
The univariate analysis in this study confirmed that the presence of perianal symptoms was a predictor of complicated PA in mpox-infected patients. A similar study also showed that perianal manifestations may be an initial sign of inflammatory disease.45 The inflammatory processes in the current study were mediated by cytokines and acute-phase proteins, suggesting that there is a potential correlation between perianal manifestations and both cytokine and acute-phase protein production. Further research is needed to confirm these findings.
A single factor is insufficient for disease prediction due to the potential influence of other variables. Interestingly, this study found that the combined use of perianal symptoms and SAA was more sensitive than perianal symptoms or SAA alone in predicting complicated PA since this combination had the highest predictive value for disease progression. Thus, assessing both perianal symptoms and SAA may inform the risk of MPXV disease progression.
This study had some limitations. First, this study is a retrospective and rather small sample size may limit our selection of potential risk factors in the multivariate regression analysis to some degree. Second, the smallpox vaccination status of individual blood donors is unknown, which may lead to differences in the status of immune response to MPXV in each mpox-infected patient. Third, additional sampling time points may be needed to determine the peak levels of each inflammatory cytokine, which will help to understand the dynamic changes in inflammatory response status in mpox-infected patients with different disease severity. Future studies with enhanced coverage (including multiple centers and female participants) and long-term follow-up could ensure more accurate and generalizable findings.
In summary, the combination of perianal symptoms and SAA levels were strongly linked with the complicated PA of mpox-infected patients. Thus, monitoring perianal symptoms and changes in SAA serum levels may aid the early identification and prediction of complicated PA risk in this patient population.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethical Approval
This research was reviewed and approved by the Clinical Research Ethics Committee of the Hangzhou Xixi Hospital (No. 2023-Research ethics-057). This study was completed in accordance with the Helsinki Declaration. All data were anonymized before use in this retrospective study.
Author Contributions
All authors made a significant contribution to the work reported, including its conception, study design, execution, acquisition of data, analysis, and/or interpretation. The authors took part in drafting, revising, or critically reviewing the article, gave final approval of the version to be published, agreed on the journal to which the article has been submitted, and agreed to be accountable for all aspects of the work.
Funding
This research was supported by grants from the Key Programs of Hangzhou Bureau of Science and Technology (202204A02), Medical Science and Technology Project of Zhejiang Province (2023KY978), Zhejiang Province Traditional Chinese Medicine Science and Technology Project (2023ZL588), Zhejiang Province Traditional Chinese Medicine Science and Technology Project (2024ZL758).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Titanji BK, Tegomoh B, Nematollahi S, Konomos M, Kulkarni PA. Monkeypox: a contemporary review for healthcare professionals. Open Forum Infect Dis. 2022;9(7):ofac310. doi:10.1093/ofid/ofac310
2. Spirito F, Guida A, Caponio VCA, Lo Muzio L. Monkeypox: a new challenge for global health system? Life. 2023;13(6):1250. doi:10.3390/life13061250
3. Otter AD, Jones S, Hicks B, et al. Monkeypox virus-infected individuals mount comparable humoral immune responses as Smallpox-vaccinated individuals. Nat Commun. 2023;14(1):5948. doi:10.1038/s41467-023-41587-x
4. Sammartino JC, Cassaniti I, Ferrari A, et al. Characterization of immune response against monkeypox virus in cohorts of infected patients, historic and newly vaccinated subjects. J Med Virol. 2023;95(5):e28778. doi:10.1002/jmv.28778
5. Angelo KM, Smith T, Camprubí-Ferrer D, et al. GeoSentinel network collaborators. epidemiological and clinical characteristics of patients with monkeypox in the geosentinel network: a cross-sectional study. Lancet Infect Dis. 2023;23(2):196–206. doi:10.1016/S1473-3099(22)00651-X
6. Gan J, Patel J, Ainsworth E, Patel A, O’Hara G, Elowaidy A. Case series of perianal and pelvic MRI imaging findings in monkeypox. BJR Case Rep. 2022;9(4):20220109. doi:10.1259/bjrcr.20220109
7. Saied AA, Chandran D, Chakraborty S, Emran TB, Dhama K. Mpox and healthcare workers — a minireview of our present knowledge. Egypt J Intern Med. 2023;35(46). doi:10.1186/s43162-023-00233-0
8. Saied AA. Mpox virus Clade IIb detection in the air. J Med Virol. 2023;95(5):e28775. doi:10.1002/jmv.28775
9. Cherfan P, Massaad E, Hui VW. Anorectal manifestations of treatment-refractory monkeypox requiring surgical intervention. Am Surg. 2023;89(12):6370–6373. doi:10.1177/00031348231177931
10. Yang J, Han S, Xu J. Deep Learning-Based Magnetic Resonance Imaging Features in Diagnosis of Perianal Abscess and Fistula Formation. Contrast Media Mol Imaging. 2021;2021:9066128. doi:10.1155/2021/9066128
11. Ogoina D, Damon I, Nakoune E. Clinical review of human mpox. Clin Microbiol Infect. 2023;29(12):1493–1501. doi:10.1016/j.cmi.2023.09.004
12. Takahama M, Akira S, Saitoh T. Autophagy limits activation of the inflammasomes. Immunol Rev. 2018;281(1):62–73. doi:10.1111/imr.12613
13. Gabay C, Kushner I. Acute-phase proteins and other systemic responses to inflammation. N Engl J Med. 1999;340(6):448–454. doi:10.1056/NEJM199902113400607
14. Li H, Xiang X, Ren H, et al. Serum amyloid A is a biomarker of severe coronavirus disease and poor prognosis. J Infect. 2020;80(6):646–655. doi:10.1016/j.jinf.2020.03.035
15. Copaescu A, Smibert O, Gibson A, Phillips EJ, Trubiano JA. The role of IL-6 and other mediators in the cytokine storm associated with SARS-CoV-2 infection. J Allergy Clin Immunol. 2020;146(3):518–534.e1. doi:10.1016/j.jaci.2020.07.001
16. Zhu G, Zhu J, Song L, Cai W, Wang J. Combined use of biomarkers for distinguishing between bacterial and viral etiologies in pediatric lower respiratory tract infections. Infect Dis. 2015;47(5):289–293. doi:10.3109/00365548.2014.987163
17. Fan R, Cheng Z, Huang Z, et al. TREM-1, TREM-2 and their association with disease severity in patients with COVID-19. Ann Med. 2023;55(2):2269558. doi:10.1080/07853890.2023.2269558
18. Ponti G, Maccaferri M, Ruini C, Tomasi A, Ozben T. Biomarkers associated with COVID-19 disease progression. Crit Rev Clin Lab Sci. 2020;57(6):389–399. doi:10.1080/10408363.2020.1770685
19. Zhu S, Zeng C, Zou Y, Hu Y, Tang C, Liu C. The clinical diagnostic values of SAA, PCT, CRP, and IL-6 in children with bacterial, viral, or co-infections. Int J Gen Med. 2021;14:7107–7113. doi:10.2147/IJGM.S327958
20. Perez L. Acute phase protein response to viral infection and vaccination. Arch Biochem Biophys. 2019;671:196–202. doi:10.1016/j.abb.2019.07.013
21. Agrati C, Cossarizza A, Mazzotta V, et al. Immunological signature in human cases of monkeypox infection in 2022 outbreak: an observational study. Lancet Infect Dis. 2023;23(3):320–330. doi:10.1016/S1473-3099(22)00662-4
22. Adamo S, Gao Y, Sekine T, et al. Memory profiles distinguish cross-reactive and virus-specific T cell immunity to mpox. Cell Host Microbe. 2023;31(6):928–936.e4. doi:10.1016/j.chom.2023.04.015
23. Lum FM, Torres-Ruesta A, Tay MZ, et al. Monkeypox: disease epidemiology, host immunity and clinical interventions. Nat Rev Immunol. 2022;22(10):597–613. doi:10.1038/s41577-022-00775-4
24. Johnston SC, Johnson JC, Stonier SW, et al. Cytokine modulation correlates with severity of monkeypox disease in humans. J Clin Virol. 2015;63:42–45. doi:10.1016/j.jcv.2014.12.001
25. Vogel JD, Johnson EK, Morris AM, et al. Clinical practice guideline for the management of anorectal abscess, fistula-in-ano, and rectovaginal fistula. Dis Colon Rectum. 2016;59(12):1117–1133. doi:10.1097/DCR.0000000000000733
26. Clinical Consensus Guide Specialized Committee of Chinese Medical Doctor Association Anorectal Doctor Branch. Chinese expert consensus on clinical diagnosis and treatment of perianal abscess. Chin J Gastro Surg. 2018;21(4):456–457. doi:10.3760/cma.j.issn.1671-0274.2018.04.018
27. Guevara-Martínez J, La-Noire FP, Arteaga-Asensio P, et al. Monkeypox multidisciplinary collaboration group. Proctitis in patients with monkeypox infection: a single-center analysis of 42 consecutive cases from a multidisciplinary observational study on monkeypox proctitis. Tech Coloproctol. 2023;27(12):1211–1218. doi:10.1007/s10151-023-02782-6
28. Zhang W, Liu S, Miao L, et al. Dynamics of CD4+ T-cells and neutralizing antibody responses to three consecutive doses of inactivated COVID-19 vaccines in PLWH. Infect Drug Resist. 2023;16:2695–2707. doi:10.2147/IDR.S409147
29. Wang Y, Li J, Zhang W, et al. Extending the dosing interval of COVID-19 vaccination leads to higher rates of seroconversion in people living with HIV. Front Immunol. 2023;14:1152695. doi:10.3389/fimmu.2023.1152695
30. Kats L, Goldman Y, Kahn A. Automatic detection of image sharpening in maxillofacial radiology. BMC Oral Health. 2021;21(1):411. doi:10.1186/s12903-021-01777-9
31. Ophinni Y, Frediansyah A, Sirinam S, et al. Monkeypox: immune response, vaccination and preventive efforts. Narra J. 2022;2(3):e90. doi:10.52225/narra.v2i3.90
32. Sofyantoro F, Kusuma HI, Vento S, Rademaker M, Frediansyah A. Global research profile on monkeypox-related literature (1962-2022): a bibliometric analysis. Narra J. 2022;2(3):e96. doi:10.52225/narra.v2i3.96
33. Barkai O, Abramov R, Harbi A, Gilshtein H. Characterization of risk factors affecting the recurrence of perianal abscesses and complications. Isr Med Assoc J. 2024;26(7):428–433. PMID: 39082452.
34. Liu BM, Martins TB, Peterson LK, Hill HR. Clinical significance of measuring serum cytokine levels as inflammatory biomarkers in adult and pediatric COVID-19 cases: a review. Cytokine. 2021;142:155478. doi:10.1016/j.cyto.2021.155478
35. Gao L, Liu X, Zhang D, et al. Early diagnosis of bacterial infection in patients with septicopyemia by laboratory analysis of PCT, CRP and IL-6. Exp Ther Med. 2017;13(6):3479–3483. doi:10.3892/etm.2017.4417
36. Zhou YZ, Teng XB, Han MF, et al. The value of PCT, IL-6, and CRP in the early diagnosis and evaluation of COVID-19. Eur Rev Med Pharmacol Sci. 2021;25(2):1097–1100. doi:10.26355/eurrev_202101_24680
37. Ragab D, Salah Eldin H, Taeimah M, Khattab R, Salem R. The COVID-19 cytokine storm; what we know so far. Front Immunol. 2020;11:1446. doi:10.3389/fimmu.2020.01446
38. Smail SW, Babaei E, Amin K, Serum IL-23 AWH. IL-10, and TNF-α predict in-hospital mortality in COVID-19 patients. Front Immunol. 2023;14:1145840. doi:10.3389/fimmu.2023.1145840
39. De Buck M, Gouwy M, Wang JM, et al. The cytokine-serum amyloid A-chemokine network. Cytokine Growth Factor Rev. 2016;30:55–69. doi:10.1016/j.cytogfr.2015.12.010
40. Saiki O, Uda H. Ratio of serum amyloid A to C-reactive protein is constant in the same patients but differs greatly between patients with inflammatory diseases. Scand J Immunol. 2022;95(2):e13121. doi:10.1111/sji.13121
41. Fu J, Huang PP, Zhang S, et al. The value of serum amyloid A for predicting the severity and recovery of COVID-19. Exp Ther Med. 2020;20(4):3571–3577. doi:10.3892/etm.2020.9114
42. Sun Z, Li Y, Chang F, Jiang K. Utility of serum amyloid A as a potential prognostic biomarker of aneurysmal subarachnoid hemorrhage. Front Neurol. 2023;13:1099391. doi:10.3389/fneur.2022.1099391
43. Abdelhakam DA, Badr FM, Abd El Monem Teama M, Bahig Elmihi NM, El-Mohamdy MA. Serum amyloid A, ferritin and carcinoembryonic antigen as biomarkers of severity in patients with COVID-19. Biomed Rep. 2022;16(2):13. doi:10.3892/br.2021.1496
44. Ahmed SK, Dabou EA, Abdelsamad S, et al. Monkeypox virus infection and myocarditis: a review of current evidence and possible pathogenesis. Narra J. 2023;3(1):e104. doi:10.52225/narra.v3i1.104
45. Panés J, Rimola J. Perianal fistulizing crohn’s disease: pathogenesis, diagnosis and therapy. Nat Rev Gastroenterol Hepatol. 2017;14(11):652–664. doi:10.1038/nrgastro.2017.104
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.