")
Back to Journals » Clinical Ophthalmology » Volume 19
Differences in Ocular Biometry Between Short-Axial and Normal-Axial Eyes in the Elderly Japanese
Authors Tanaka T, Nishitsuka K , Obata H
Received 31 October 2024
Accepted for publication 10 January 2025
Published 20 January 2025 Volume 2025:19 Pages 187—197
DOI https://doi.org/10.2147/OPTH.S503988
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Takahiro Tanaka,* Koichi Nishitsuka,* Hiroto Obata*
Department of Ophthalmology, Saitama Medical Center, Saitama Medical University, Kawagoe-shi, Saitama, Japan
*These authors contributed equally to this work
Correspondence: Koichi Nishitsuka, Department of Ophthalmology, Saitama Medical Center, Saitama Medical University, 1981 Kamoda, Kawagoe-shi, Saitama, Japan, Tel +81-49-228-3682, Fax +81-49-225-5722, Email [email protected]
Purpose: Among patients with angle-closure glaucoma, it is common to have a short-axial eye, which also makes it difficult to select an appropriate intraocular lens. Previous studies have focused on the ocular biometry of the long-axial eye, whereas only a few reports have focused on the short-axial eye. This study aimed to clarify the characteristics of the short-axial eye on ocular biometry among the elderly Japanese.
Patients and Methods: This retrospective cross-sectional study included 142 patients who consulted at our hospital. The ocular axial length (AL), central corneal thickness (CCT), average anterior corneal radius of curvature (CR), white-to-white (WTW), anterior chamber depth (ACD), and lens thickness (LT) were measured using OA-2000. The short-axial and normal-axial groups (short-axial [SA] and normal-axial [NA] groups) included those with an AL less than 22.5 mm and ranging from 22.5– 26.5 mm, respectively. Comparisons between groups were analyzed using the Wilcoxon rank sum test. Spearman’s rank correlation coefficient tests and multiple regression analyses were performed for all parameters overall and per group.
Results: The parameters that were significantly different between the SA and NA groups were CR, WTW, and ACD (all P < 0.0001). In the SA group (42 patients), only ACD was significantly correlated with AL (r = 0.33, P = 0.031). On multiple regression analysis for the SA group, none of the parameters had a significant effect on AL (all P > 0.05).
Conclusion: In the SA group, ACD was the only factor that positively correlated with AL; it was significantly shallower than in the NA group. Thus, in the SA eye, it is clinically important to be aware of ACD.
Keywords: preoperative cataract patients, swept-source optical coherence tomography, ocular axial length, ocular parameters, angle-closure glaucoma
Introduction
Ocular axial length (AL) is one of the representative measurement items in ocular biometry. Recently, the OA-2000 (TOMEY Corporation, Nagoya, Japan) has been used to simultaneously measure various parameters including AL, central corneal thickness (CCT), average anterior corneal radius of curvature (CR), transverse corneal diameter/white-to-white (WTW), anterior chamber depth (ACD), and lens thickness (LT) with the swept-source optical coherence tomography (SS-OCT) method in a short time. We have previously reported changes in parameters due to increasing AL in elderly Japanese using the OA-2000.1 We found that, as AL increased, LT tended to be thinner and CR, WTW, and ACD increased, with no association with CCT.
AL is clinically related to myopia in the long-axial (LA) eye,2,3 as well as microphthalmos or nanophthalmos in the short-axial (SA) eye.4 The LA eye is associated with eye diseases, increasing the risk of retinal detachment, subretinal neovascularization, and glaucoma.2,3,5 The shallow ACD associated with AL is thought to be one reason for cases of angle-closure glaucoma seen in the SA eye.6–8 However, there have been no reports of a detailed analysis of AL and various parameters focused on the SA eye.
No previous study has reported an evidence-based definition of the SA eye. Hoffmann et al9 defined the SA eye as those with AL < 21.63 mm, which was the lowest 5% of all eyes. Meanwhile, other studies defining the SA eye as AL < 22 mm have reported that the accuracy of the intraocular lens (IOL) formula is lower in the SA eye.10–12 Only a few studies have reported on this topic, possibly due to the lack of a single definition and a clear rationale for evaluating the SA eye. This study aimed to investigate the characteristics of the SA eye by comprehensively measuring various parameters with OA-2000 among preoperative Japanese cataract patients, as well as examined the relationship between AL and various parameters.
Material and Methods
Study Subjects
This was a retrospective cross-sectional review at our hospital. The subjects included 142 outpatients (142 eyes) from April 1, 2020 to March 31, 2023, who had their AL measured using the OA-2000 prior to cataract surgery. In this study, SA was defined by an AL of less than 22.5 mm; retrospectively, 42 eyes were classified under the SA group. Conversely, the normal-axial (NA) group included patients with an AL of 22.5 mm to less than 26.5 mm. A list of patients who met the criteria during the study period was compiled, and 100 eyes without missing values were randomly selected from the list. Therefore, eyes with an AL greater than 26.5 mm were excluded in advance. We show a flowchart of patient selection in Figure 1.
 |
Figure 1 Study flowchart of patient selection. |
Measurements
The ocular biometry parameters included AL, CCT, CR, WTW, ACD, and LT. Measurements were taken without mydriasis, completely automatic, and no manual correction was made; the analysis included only patients for whom all these parameters could be measured completely automatically. For each person, only one eye was included in the analysis. If both eyes could be measured, the longer eye was included in order to exclude morbidity due to the SA eye. Adoption was conditional on achieving a signal-to-noise ratio (SNR) > 2.1.13
Statistical Analyses
A nonparametric test (Wilcoxon rank sum test) was used to examine significant differences in the parameters between the SA and NA groups. Since we could not gather enough patients for the SA group, we conducted a post-hoc power analysis to confirm the adequacy of the sample size. Correlation analyses were performed using Spearman’s rank correlation coefficient test in a round-robin manner for the overall, SA and NA groups. To investigate the effect of each parameter on AL, multiple regression analyses were conducted overall and for each group using AL as the objective variable and each parameter, gender, and age as explanatory variables. Gender and age were included as explanatory variables because relationships have been observed between these two variables and AL.9,14–31
Statistical analyses were conducted using JMP Pro version 17 (SAS Institute Inc., Cary, NC, USA), with statistical significance set at p < 0.05. This research adhered to the principles of the Declaration of Helsinki and received approval from the Saitama Medical University Ethics Committee (approval number: sou2023-115). Consent was acquired through an opt-out format. The Ethics Committee at Saitama Medical University deemed informed consent unnecessary given the retrospective nature of the study. The study took measures to guarantee the confidentiality of personal information for each participant, ensuring that it remained secure and was not disclosed to third parties.
Results
Characteristics of the SA Group
Table 1 shows the average values of the parameters. The percentage of females in the SA group was 83.3% (35 out of 42 eyes). There was an association between having an SA eye and being female (Pearson’s chi-squared test: P = 0.0002).
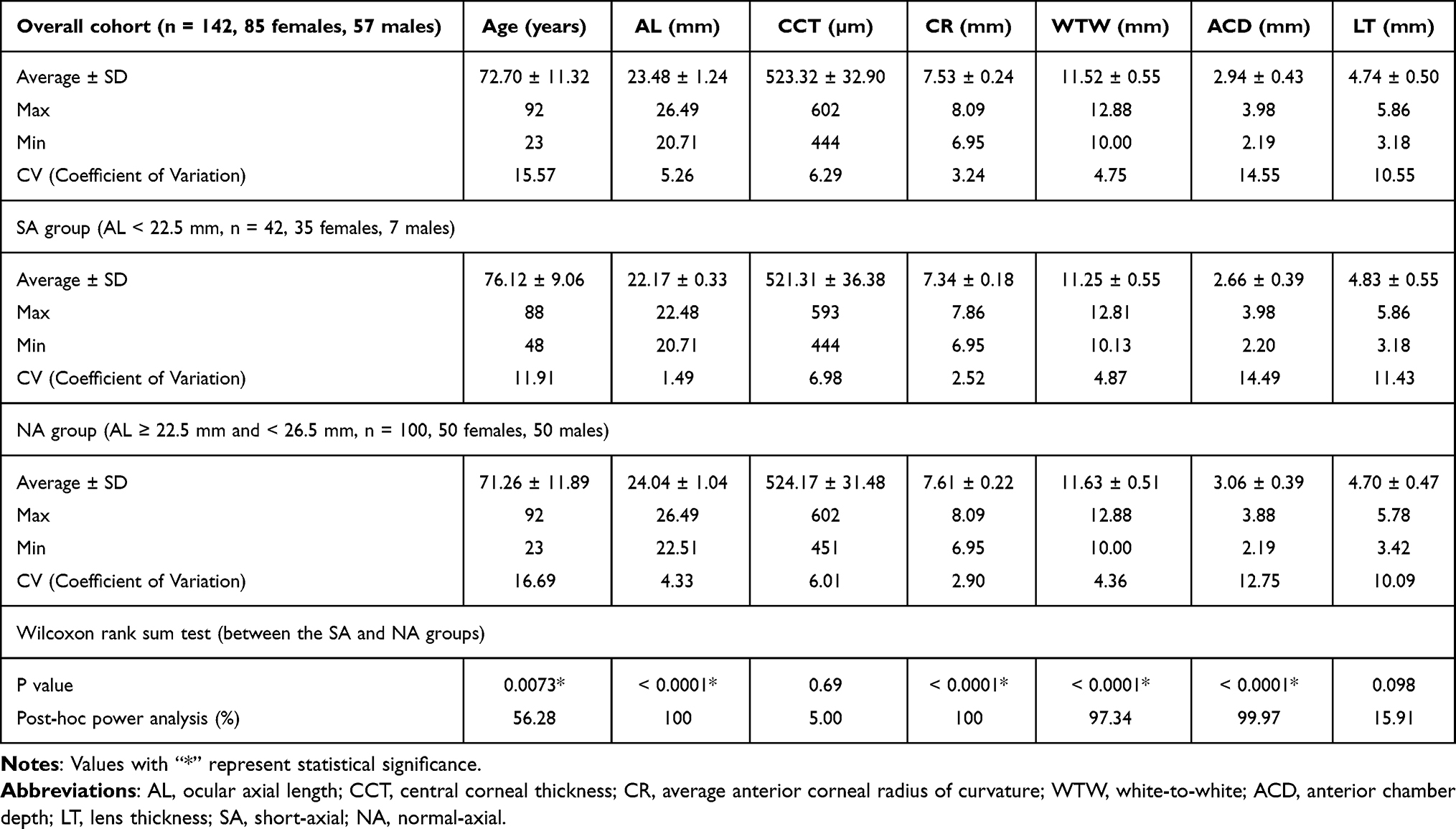 |
Table 1 Mean Values for Each Parameter and Comparison Between Two Groups |
Comparison of Parameters Between SA and NA Groups
Table 1 shows the results of the two-group comparisons for each parameter. Age (P = 0.0073), CR (P < 0.0001), WTW (P < 0.0001), and ACD (P < 0.0001) were significantly different between groups. CCT (P = 0.69) and LT (P = 0.098) were similar between both groups. However, in the post-hoc power analysis, we did not achieve sufficient power for age, CCT and LT.
Correlation Analyses in SA and NA Groups
Table 2 summarizes the results of correlation analyses by group. In the overall cohort, AL was significantly correlated with age (r = −0.26, P = 0.0018), CR (r = 0.53, P < 0.0001), WTW (r = 0.39, P < 0.0001), ACD (r = 0.63, P < 0.0001), and LT (r = −0.27, P = 0.0013), but not with CCT (P = 0.51). In the SA group, only ACD (r = 0.33, P = 0.031) was significantly correlated with AL. In the NA group, AL was significantly correlated with CR (r = 0.26, P = 0.0083), WTW (r = 0.26, P = 0.0091), ACD (r = 0.55, P < 0.0001), and LT (r = −0.27, P = 0.0057), but not with CCT (P = 0.38). The parameters that were correlated with the overall and NA groups were the same except for age.
 |
Table 2 Correlation Coefficients for Each Parameter by Group |
Multiple Regression Analyses
Table 3 shows the results of multiple regression analyses, with AL as the objective variable and each parameter, gender, and age as explanatory variables. Gender and age had no effect on AL in any of the multiple regression analyses (all P > 0.05). The overall multiple regression analysis showed that CCT and WTW did not affect AL (CCT, P = 0.68; WTW, P = 0.46). Multiple regression analysis of the SA group revealed that none of the parameters had any effect on AL (all P > 0.05) and that the regression equation was not valid (P = 0.90). Multiple regression analysis of the NA group revealed that only ACD affected AL (P < 0.0001). The adjusted coefficient of determination was higher for the overall cohort (adjusted R² = 0.51, P < 0.0001) compared to the NA group (adjusted R² = 0.32, P < 0.0001). Figure 2 represents the actual AL versus predicted AL plot derived from multiple regression analyses for each group. In Figure 2A, a linear relationship was observed between the actual AL and predicted AL values in the overall cohort. In contrast, Figure 2B showed no linear relationship for the SA group. In Figure 2C, the NA group showed a weaker linear relationship compared to the overall cohort.
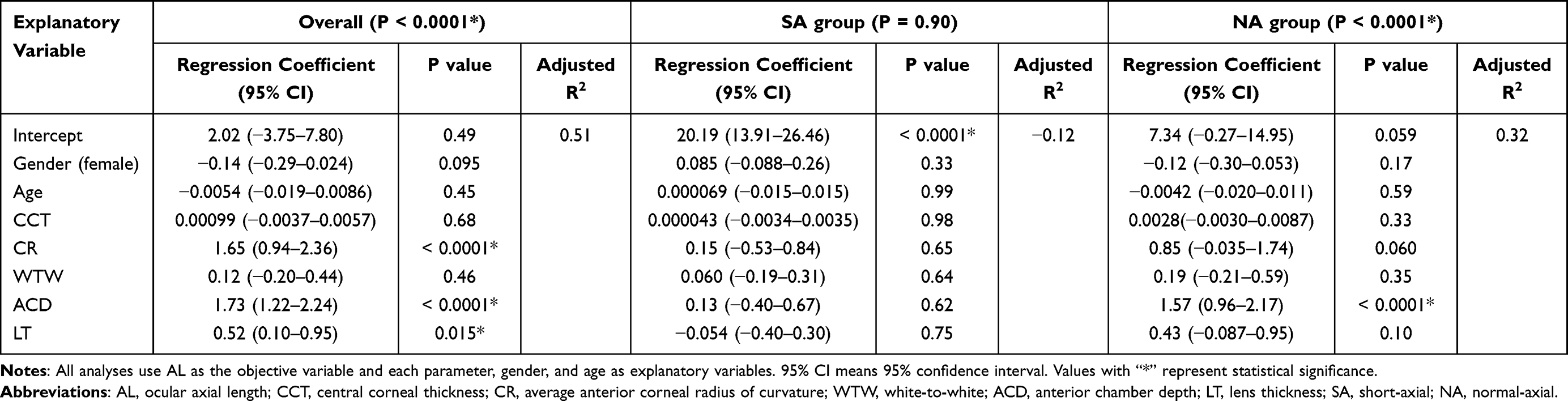 |
Table 3 Multiple Regression Analyses by Group |
 |
Figure 2 Plots of predicted AL versus actual AL using multiple regression analyses. Overall cohort (A), SA group (B), and NA group (C). The red line represents the regression line. The red zone shows its 95% confidential intervals. The blue line represents the mean value. |
Discussion
The novelty of this study lies in defining and characterizing the SA eye in the elderly Japanese. Hoffmann et al9 defined the SA eye as those with AL < 21.63 mm; only three cases met this criterion in the present study. However, when determining IOL power, the SA eye is often defined in those with AL < 22 mm,10–12 but only nine cases met this criterion in our study Figure 3. In addition, since Japanese are thought to have a higher prevalence of myopia and longer AL than Westerners,2,3 we considered it necessary to develop criteria specific to Japanese for the SA eye. Therefore, we defined the SA group as those with AL < 22.5 mm in this study. Meanwhile, domestic studies use AL > 26.5 mm as a cutoff for LA eye,32,33 but no reports have explained the rationales behind this. Nevertheless, we decided to define the NA group in this study as those with AL < 26.5 mm.
 |
Figure 3 Distribution of the overall AL. |
Notably, there were significantly more females in the SA group, which is consistent with previous reports claiming that males have longer ALs than females.9,14–25 Furthermore, the SA group was significantly older than the NA group. This finding may be associated with previous studies indicating that AL tends to decrease with age.16–18,21,23,29,31 Additionally, the present study revealed that those with the NA eye tend to undergo cataract surgery at a younger age compared to those with the SA eye. This finding suggests that longer ALs may contribute to the earlier onset of cataracts.29 However, it should be noted that the post-hoc power analysis regarding age had insufficient power.
In the SA group, only ACD showed a correlation with AL. Many positive correlations between AL and ACD have been reported in the past, although those previous studies did not explicitly focus on the SA eye.1,9,14–24,26–30,34,35 ACD was significantly different between the SA and NA groups in our study, indicating that the SA group had a significantly smaller ACD than the NA group. In contrast, Hoffmann et al9 found no significant correlation between AL and ACD in the SA eye. Therefore, ACD tends to become shallower as the AL becomes shorter, but this may be different if we used the same definition of SA as Hoffmann et al9 did. The significant positive correlation between AL and ACD in all groups suggests that these parameters are sensitive to each other.
Many may believe that angle-closure glaucoma occurs because the ACD is shallow in the SA eye. Indeed, the SA eye and shallow ACD are predictors of angle-closure glaucoma,6–8 but ACD does not directly cause this. Nongpiur et al36 reported that angle-closure eyes had significantly thicker LT (P = 0.01) and shallower ACD (P < 0.001) but with no significant difference in lens position (P = 0.34). Additionally, neither LT (odds ratio = 1.78) nor lens position (odds ratio = 1.94) were associated with the angle-closure eye on multivariate analysis. Instead, they found that the angle-closure eye has a thicker lens with a greater lens vault (LV, perpendicular distance from horizontal line joining the two scleral spurs to the anterior pole of the lens; odds ratio = 48.1). LV was found to be a new parameter associated with the angle-closure eye. Similarly, the Singapore Chinese Eye Study25 reported that LV was responsible for the decline in ACD. Thus, to elucidate the mechanism of the angle-closure glaucoma, it may be necessary to consider LV. However, since OA-2000 cannot measure LV, it must be measured separately using an anterior OCT or a similar tool.
CCT had no significant correlation with AL in all correlation analyses, which is in line with the findings of other previous studies.1,24,26,37–39 Other studies have reported significant positive correlations between AL and CCT, but the correlation coefficient was low.27–30,40,41 Nevertheless, none of those previous studies focused on the SA eye specifically. There was also no statistically significant difference between the SA and NA groups in our study. This suggests that CCT may not be significantly affected by AL. However, it is important to note that we did not have sufficient power in the post-hoc power analysis.
Both CR and WTW had significant positive correlations with AL in the correlation analyses overall and for the NA group. Previous reports have identified weak positive correlations between AL and CR1,17,28,34,40 and between AL and WTW,1,9,16,18,20,22,23,26,28–30 but none of these focused on the SA eye. In the present study, the SA group had significantly smaller CR and WTW than the NA group. Furthermore, due to the significant positive correlation between CR and WTW (r = 0.47) in the overall cohort, it is generally assumed that WTW shrinks as CR shrinks and the corneal shape becomes steeper.29,34 Conversely, in the SA group, neither CR nor WTW were correlated with AL. In line with this, Hoffmann et al9 also reported that there was no correlation between AL and WTW in the SA eye. Meanwhile, Wei et al42 reported positive or negative correlations between AL and WTW depending on the value of AL (AL < 22 mm; r = −0.228, AL 22–24.5 mm; r = 0.323; AL 24.5–26 mm; r = −0.055). Thus, the results may not be consistent because of the different ranges of ALs used in each study.
There are many reports of LT thinning as AL elongates,1,14,15,20,23,28,30 but these studies were not focused on the SA eye. In our study, there was a slight significant negative correlation between AL and LT in the overall and NA group but no correlation in the SA group. This indicates that LT thickens as AL shortens in the NA group, but there is a limit beyond a certain point that prevents thickening of the lens. This is further supported by the fact that there was no statistically significant difference between LT in the SA and NA groups. However, it is crucial to acknowledge that the post-hoc power analysis did not yield sufficient power. Meng et al43 reported that LT tended to decrease with increasing AL in normal eyes (r = −0.166, P < 0.001), but it conversely increased in short eyes (r = 0.076, P = 0.004), indicating that there is a point at which the trend of lens thickness changes between the SA and NA eyes.
Since no high correlation coefficients were observed in the correlation analyses (Table 2), we conducted multiple regression analyses without excluding any variables. On overall multiple regression analysis, CR, ACD, and LT were identified as significant coefficients for predicting AL. Other reports have conducted a multiple regression analysis26 or multivariate analyses27,28 with AL as the objective variable, but the parameters overlapping with this study were different. Compared to our previous report1 (adjusted R2 = 0.34), the present study had a higher adjusted coefficient of determination (adjusted R2 = 0.51). Although gender and age were included as explanatory variables in the model, excluding them did not substantially change the adjusted coefficient of determination (adjusted R2 = 0.50). The longer the AL, the more difficult it was to predict the AL using the parameters. The shape of LA eyes could differ greatly from that of NA eyes. The lack of AL prediction and linear relationship Figure 2B in the SA group might suggest certain properties that make it unique. In addition, the weak linearity observed in the NA group Figure 2C, which improved in the overall cohort Figure 2A, could suggest the need to interpret AL in the context of both the NA and SA groups collectively.
These results have several clinical implications. For instance, some factors should be considered during cataract surgeries in the SA eye. As the AL shortens, the WTW and ACD, respectively, become smaller and shallower, thus narrowing the anterior chamber space. The increased proximity of critical structures, such as the corneal endothelium and iris, demands heightened intra-operative precision. Thus, extra care should be made to handle surgical instruments meticulously, avoiding any contact or damage to these delicate structures during insertion and manipulation within the anterior chamber. Highlighting these anatomical and surgical considerations is crucial for improving outcomes in patients with the SA eye. Additionally, studies of the SA eye may help determine the IOL power. The IOL formulas for predicting postoperative cataract refraction vary based on AL.10,11,44 Although a meta-analysis of IOL formulas was conducted in recent years, it was difficult to select statistically superior IOL formulas for the SA eye.45 However, a meta-analysis by Luo et al12 suggests that a new generation of IOL formulas based on artificial intelligence or ray-tracking principles are more accurate in the SA eye. Although artificial intelligence is largely a black box, considering in various factors in the SA eye that have been poorly studied may help accurately predict postoperative refraction. Hence, as in the present study, comparing with the NA eye or considering the SA eye within the context of the NA eye as a whole could be useful for selecting the optimal power of intraocular lenses.
This study has some limitations that must be discussed. First, this study used objective results derived from a single machine, and did not account for physical measurements (eg, height, weight, and refractive power) and other demographic data (eg, educational background, social environment, and reading frequency) as in previous studies.17,31,46 In addition, our hospital has a large number of difficult cataract cases, and thus selection bias could have been present in the cases collected. In particular, there were fewer cases of SA eye compared to LA eye, and it took a long time to collect cases. In addition, post-hoc power analyses revealed that the power for age, CCT, and LT was inadequate. This indicates the necessity of collecting larger sample sizes in future studies. Another limitation is that we selected AL cutoffs for the SA and NA groups without strong evidence; differences in the definition of the SA may have affected the results. Hoffmann et al9 included cases of the SA eye in their study, but this cannot be simply compared due to possible racial variations in the range of the SA eye. Future research to define the range of the SA eye in Japanese will be necessary to validate our findings.
Conclusion
On multiple regression analysis among patients with SA eye, no parameters were associated with AL. However, ACD was the only factor associated with AL in the SA group correlations and a two-group comparison with the NA group. Therefore, it is clinically important to determine ACD in the SA eye.
Abbreviations
AL, ocular axial length; CCT, central corneal thickness; CR, average anterior corneal radius of curvature; WTW, white-to-white; ACD, anterior chamber depth; LT, lens thickness; SS-OCT, swept-source optical coherence tomography; SA, short-axial; NA, normal-axial; IOL, intraocular lens.
Data Sharing Statement
The datasets underpinning the conclusions of the present study can be obtained by contacting the corresponding author through a reasonable request.
Ethical Approval and Informed Consent
Consent was acquired through an opt-out format. The Ethics Committee at Saitama Medical University deemed informed consent unnecessary given the retrospective nature of the study. The study took measures to guarantee the confidentiality of personal information for each participant, ensuring that it remained secure and was not disclosed to third parties.
Consent for Publication
As this research did not include any identifiable patient information, consent for publication was not necessary.
Acknowledgments
We are grateful to Mrs. Ayako Marubayashi, a certified orthoptist at the Saitama Medical Center, for her research assistance. We extend our gratitude to enago (Crimson Interactive Japan Co., Ltd., Chiyoda-ku, Tokyo, Japan) for their professional proofreading services.
Author Contributions
All authors have played a substantial role in the development of the reported work, contributing to aspects such as conception, study design, execution, data acquisition, analysis, and interpretation. They have actively participated in drafting, revising, or critically reviewing the article and have provided final approval for the version to be published. The authors have collectively decided on the journal to which the article is submitted and have committed to being accountable for all facets of the work.
Funding
The authors received no specific funding for this work.
Disclosure
Prof. Koichi Nishitsuka has received personal fees from Santen Medical, Senju Medical, Otsuka Medical, Kowa Medical, Alcon, HOYA medical, and Chugai Medical, unrelated to the work submitted. The authors declare no other competing interests in this work.
References
1. Tanaka T, Nishitsuka K, Obata H. Correlation of ocular biometry with axial length in elderly Japanese. Clin Ophthalmol. 2024;18:351–360. doi:10.2147/OPTH.S446031
2. Meng W, Butterworth J, Malecaze F, Calvas P. Axial length of myopia: a review of current research. Ophthalmologica. 2011;225:127–134. doi:10.1159/000317072
3. Young TL, Metlapally R, Shay AE. Complex trait genetics of refractive error. Arch Ophthalmol. 2007;125:38–48. doi:10.1001/archopht.125.1.38
4. Yang N, Zhao -L-L, Liu J, Ma -L-L, Zhao J-S. Nanophthalmos: an update on the biological parameters and fundus abnormalities. J Ophthalmol. 2021;2021:1–6.
5. Grossniklaus HE, Green WR. Pathologic findings in pathologic myopia. Retina. 1992;12(2):127–133. doi:10.1097/00006982-199212020-00009
6. Salmon JF. Predisposing factors for chronic angle-closure glaucoma. Prog Retin Eye Res. 1999;18:121–132. doi:10.1016/S1350-9462(98)00007-X
7. George R, Paul PG, Baskaran M. Ocular biometry in occludable angles and angle closure glaucoma: a population based survey. Br J Ophthalmol. 2003;87:399–402. doi:10.1136/bjo.87.4.399
8. Sawaguchi S, Sakai H, Iwase A, et al. Prevalence of primary angle closure and primary angle-closure glaucoma in a southwestern rural population of Japan. Ophthalmology. 2012;119:1134–1142. doi:10.1016/j.ophtha.2011.12.038
9. Hoffmann PC, Hütz WW. Analysis of biometry and prevalence data for corneal astigmatism in 23 239 eyes. J Cataract Refr Surg. 2010;36:1479–1485. doi:10.1016/j.jcrs.2010.02.025
10. Hoffer KJ. Clinical results using the Holladay 2 intraocular lens power formula. J Cataract Refr Surg. 2000;26:1233–1237. doi:10.1016/S0886-3350(00)00376-X
11. Kane JX, Van Heerden A, Atik A, Petsoglou C. Intraocular lens power formula accuracy: comparison of 7 formulas. J Cataract Refr Surg. 2016;42:1490–1500. doi:10.1016/j.jcrs.2016.07.021
12. Luo Y, Li H, Gao L, et al. Comparing the accuracy of new intraocular lens power calculation formulae in short eyes after cataract surgery: a systematic review and meta-analysis. Int Ophthalmol. 2022;42:1939–1956. doi:10.1007/s10792-021-02191-4
13. Olsen T, Thorwest M. Calibration of axial length measurements with the Zeiss IOLMaster. J Cataract Refr Surg. 2005;31:1345–1350. doi:10.1016/j.jcrs.2004.12.066
14. Osuobeni EP. Ocular components values and their intercorrelations in Saudi Arabians. Ophthal Physl Opt. 1999;19:489–497. doi:10.1046/j.1475-1313.1999.00453.x
15. Jivrajka R, Shammas MC, Boenzi T, Swearingen M, Shammas JH. Variability of axial length, anterior chamber depth, and lens thickness in the cataractous eye. J Cataract Refr Surg. 2008;34:289–294. doi:10.1016/j.jcrs.2007.10.015
16. Fotedar R, Wang JJ, Burlutsky G, et al. Distribution of axial length and ocular biometry measured using partial coherence laser interferometry (IOL Master) in an older white population. Ophthalmology. 2010;117:417–423. doi:10.1016/j.ophtha.2009.07.028
17. Pan C-W, Wong T-Y, Chang L, et al. Ocular biometry in an urban Indian population: the Singapore Indian eye study (SINDI). Invest Ophthalmol Vis Sci. 2011;52:6636. doi:10.1167/iovs.10-7148
18. Cui Y, Meng Q, Guo H, et al. Biometry and corneal astigmatism in cataract surgery candidates from Southern China. J Cataract Refr Surg. 2014;40:1661–1669. doi:10.1016/j.jcrs.2014.01.039
19. Chen H, Lin H, Lin Z, Chen J, Chen W. Distribution of axial length, anterior chamber depth, and corneal curvature in an aged population in South China. BMC Ophthalmol. 2016;16:47. doi:10.1186/s12886-016-0221-5
20. Ferreira TB, Hoffer KJ, Ribeiro F, Ribeiro P, O’neill JG. Ocular biometric measurements in cataract surgery candidates in Portugal. PLoS One. 2017;
21. Huang Q, Huang Y, Luo Q, Fan W. Ocular biometric characteristics of cataract patients in western China. BMC Ophthalmology. 2018;18(1):99. doi:10.1186/s12886-018-0770-x
22. Natung T, Shullai W, Nongrum B, Thangkhiew L, Baruah P, Phiamphu ML. Ocular biometry characteristics and corneal astigmatisms in cataract surgery candidates at a tertiary care center in North-East India. Indian J Ophthalmol. 2019;67:1417. doi:10.4103/ijo.IJO_1353_18
23. Lei Q, Tu H, Feng X, Ortega-Usobiaga J, Cao D, Wang Y. Distribution of ocular biometric parameters and optimal model of anterior chamber depth regression in 28,709 adult cataract patients in China using swept‐source optical biometry. BMC Ophthalmol. 2021;21:178. doi:10.1186/s12886-021-01932-4
24. Chen M-J, Liu Y-T, Tsai -C-C, Chen Y-C, Chou C-K, Lee S-M. Relationship between central corneal thickness, refractive error, corneal curvature, anterior chamber depth and axial length. J Chin Med Assoc. 2009;72:133–137. doi:10.1016/S1726-4901(09)70038-3
25. Sng CC, Foo -L-L, Cheng C-Y, et al. Determinants of anterior chamber depth: the Singapore Chinese eye study. Ophthalmology. 2012;119:1143–1150. doi:10.1016/j.ophtha.2012.01.011
26. Park SH, Park KH, Kim JM, Choi CY. Relation between axial length and ocular parameters. Ophthalmologica. 2010;224:188–193. doi:10.1159/000252982
27. Nangia V, Jonas JB, Sinha A, Matin A, Kulkarni M, Panda-Jonas S. Ocular axial length and its associations in an adult population of central rural India: the Central India eye and medical study. Ophthalmology. 2010;117:1360–1366. doi:10.1016/j.ophtha.2009.11.040
28. Yin G, Wang YX, Zheng ZY, Yang H, Xu L, Jonas JB. Ocular axial length and its associations in Chinese: the Beijing eye study. PLoS One. 2012;7:e43172. doi:10.1371/journal.pone.0043172
29. Miao A, Tang Y, Zhu X, Qian D, Zheng T, Lu Y. Associations between anterior segment biometry and high axial myopia in 3438 cataractous eyes in the Chinese population. BMC Ophthalmol. 2022;22:71. doi:10.1186/s12886-022-02300-6
30. Kim S, Oh R, Kim MK, Yoon CH. SS-OCT–based ocular biometry in an adult Korean population with cataract. J Cataract Refr Surg. 2023;49:453–459. doi:10.1097/j.jcrs.0000000000001135
31. Lim LS, Saw S-M, Jeganathan VS, et al. Distribution and determinants of ocular biometric parameters in an Asian population: the Singapore Malay eye study. Invest Ophthalmol Vis Sci. 2010;51:103. doi:10.1167/iovs.09-3553
32. Ohno-Matsui K, Jonas JB, Spaide RF. Macular bruch membrane holes in choroidal neovascularization–related myopic macular atrophy by swept-source optical coherence tomography. Am J Ophthalmol. 2016;162:133–139.e1. doi:10.1016/j.ajo.2015.11.014
33. Ueda E, Yasuda M, Fujiwara K, et al. Trends in the prevalence of myopia and myopic maculopathy in a Japanese population: the Hisayama study. Invest Ophthalmol Vis Sci. 2019;60:2781. doi:10.1167/iovs.19-26580
34. Carney LG, Mainstone JC, Henderson BA. Corneal topography and myopia. A cross-sectional study. Invest Ophthalmol Vis Sci Feb. 1997;38:311–320.
35. Fernández‐vigo JI, Fernández‐vigo JÁ, Macarro‐merino A, Fernández‐pérez C, Martínez‐de‐la‐casa JM, García Feijoó J. Determinants of anterior chamber depth in a large Caucasian population and agreement between intra‐ocular lens Master and Pentacam measurements of this variable. Acta Ophthalmol. 2016;94:150–155. doi:10.1111/aos.12824
36. Nongpiur ME, He M, Amerasinghe N, et al. Lens vault, thickness, and position in Chinese subjects with angle closure. Ophthalmology. 2011;118(3):474–479. doi:10.1016/j.ophtha.2010.07.025
37. Tong L, Saw S-M, Siak J-K, Gazzard G, Tan D. Corneal thickness determination and correlates in Singaporean schoolchildren. Invest Ophthalmol Vis Sci. 2004;45:4004. doi:10.1167/iovs.04-0121
38. Shimmyo M, Orloff PN. Corneal thickness and axial length. Am J Ophthalmol. 2005;139:553–554. doi:10.1016/j.ajo.2004.08.061
39. Oliveira C, Tello C, Liebmann J, Ritch R. Central corneal thickness is not related to anterior scleral thickness or axial length. J Glaucoma. 2006;15:190–194. doi:10.1097/01.ijg.0000212220.42675.c5
40. Krishnan VM, Jayalatha V, Vijayakumar C. Correlation of central corneal thickness and keratometry with refraction and axial length: a prospective analytical study. Cureus. 2019;11:e3917. doi:10.7759/cureus.3917
41. Hashmani N, Hashmani S, Murad A, Asghar N, Islam M. Effect of demographic variables on the regional corneal pachymetry. Asia Pac J Ophthalmol (Phila). 2019;8(4):324–329. doi:10.1097/APO.0000000000000252
42. Wei L, He W, Meng J, Qian D, Lu Y, Zhu X. Evaluation of the white-to-white distance in 39,986 Chinese Cataractous eyes. Invest Ophthalmol Vis Sci. 2021;62:7. doi:10.1167/iovs.62.1.7
43. Meng J, Wei L, He W, Qi J, Lu Y, Zhu X. Lens thickness and associated ocular biometric factors among cataract patients in Shanghai. Eye Vis. 2021;8:22.
44. Aristodemou P, Knox Cartwright NE, Sparrow JM, Johnston RL. Formula choice: Hoffer Q, Holladay 1, or SRK/T and refractive outcomes in 8108 eyes after cataract surgery with biometry by partial coherence interferometry. J Cataract Refr Surg. 2011;37:63–71. doi:10.1016/j.jcrs.2010.07.032
45. Shrivastava AK, Nayak S, Mahobia A, Anto M, Pandey P. Accuracy of intraocular lens power calculation formulae in short eyes: a systematic review and meta-analysis. Indian J Ophthalmol. 2022;70:740–748. doi:10.4103/ijo.IJO_934_21
46. Namba H, Sugano A, Murakami T, et al. Ten-year longitudinal investigation of astigmatism: the Yamagata Study (Funagata). PLoS One. 2022;17:e0261324. doi:10.1371/journal.pone.0261324
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.